• Decentralized to regional autonomies • Universal coverage • Free access • Very wide range of publicly covered services • Co-payment in pharmaceutical products • Services provided mainly in public facilities • Interterritorial Board to coordinate policies
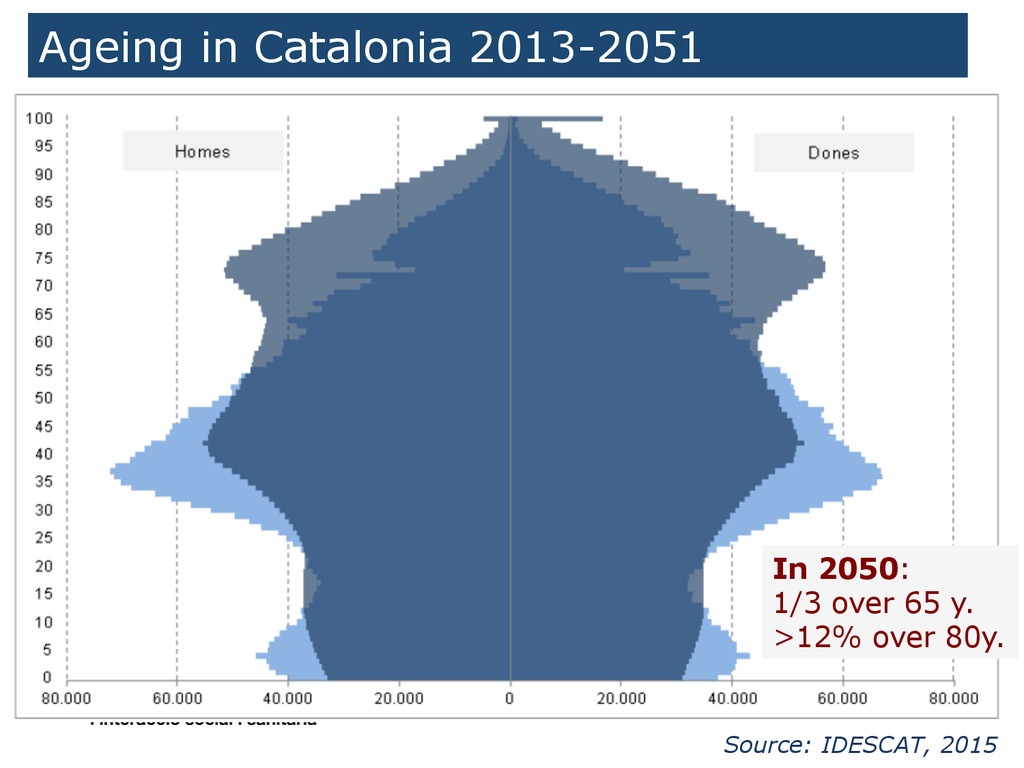
• Population: 7,611,711 inhabitants. 17% over 65 y. (expected 32% in 2050) • 1780 € expenditure per capita and 1150 € public expenditure per capita in 2012 • Life expectancy: 82.27 years • Gross Mortality rate (2010):8/1,000 inh. • Infant mortality (2010): 2.6 /1,000 live births • 369 Primary Health Centres (PHC) ranging from 20-45,000 inh) • 69 “acute hospitals” (no far from 50 Km. from every home) • 96 “long term care” centres (residential homes: long-stay, convalescence, pal.liative care) • 41 Mental Health Centres
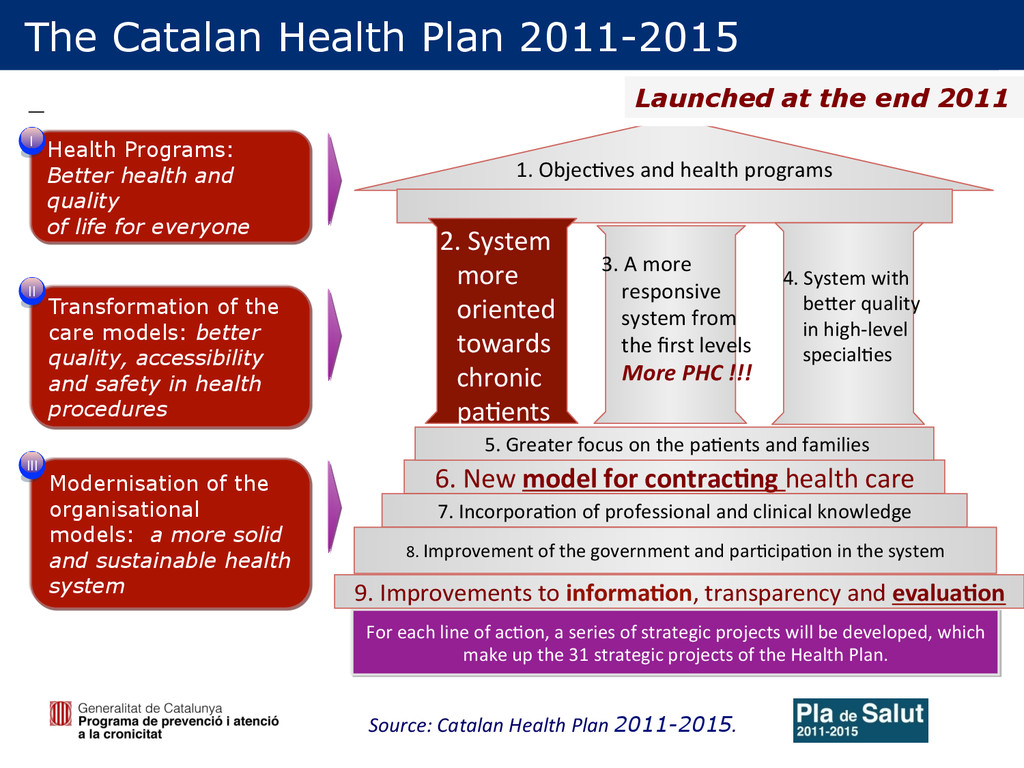
2011-2015 Health Programs: Better health and quality of life for everyone Transformation of the care models: better quality, accessibility and safety in health procedures Modernisation of the organisational models: a more solid and sustainable health system I II III For each line of ac.on, a series of strategic projects will be developed, which make up the 31 strategic projects of the Health Plan. 9. Improvements to informa(on, transparency and evalua(on 1. Objec.ves and health programs 7. Incorpora.on of professional and clinical knowledge 6. New model for contrac(ng health care 5. Greater focus on the pa.ents and families 8. Improvement of the government and par.cipa.on in the system 2. System more oriented towards chronic pa.ents 3. A more responsive system from the first levels More PHC !!! 4. System with beOer quality in high-‐level special.es Launched at the end 2011
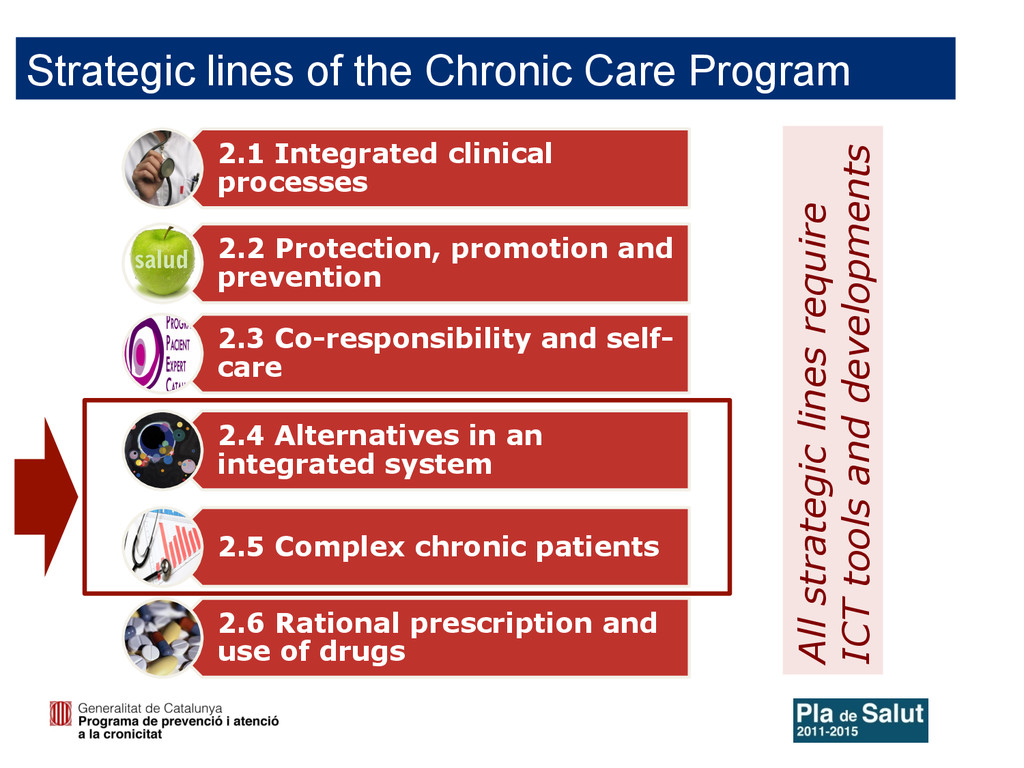
Co-responsibility and self- care 2.4 Alternatives in an integrated system 2.5 Complex chronic patients 2.6 Rational prescription and use of drugs Strategic lines of the Chronic Care Program All strategic lines require ICT tools and developments
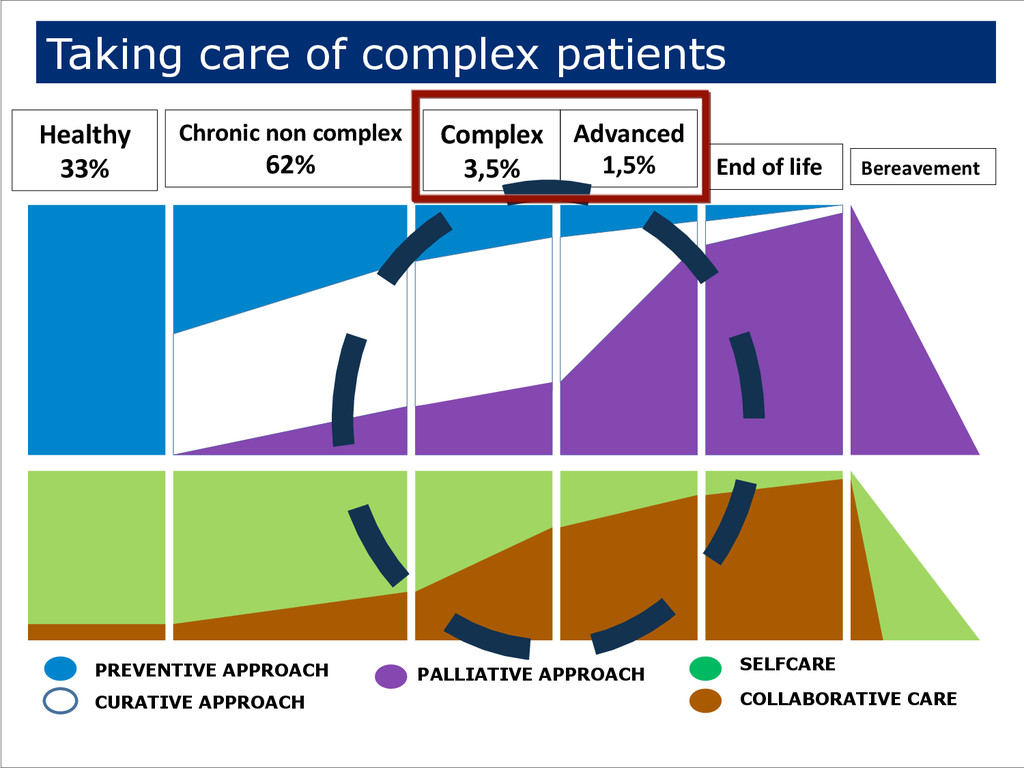
Complex 3,5% Advanced 1,5% End of life Bereavement PREVENTIVE APPROACH CURATIVE APPROACH PALLIATIVE APPROACH SELFCARE COLLABORATIVE CARE Taking care of complex patients
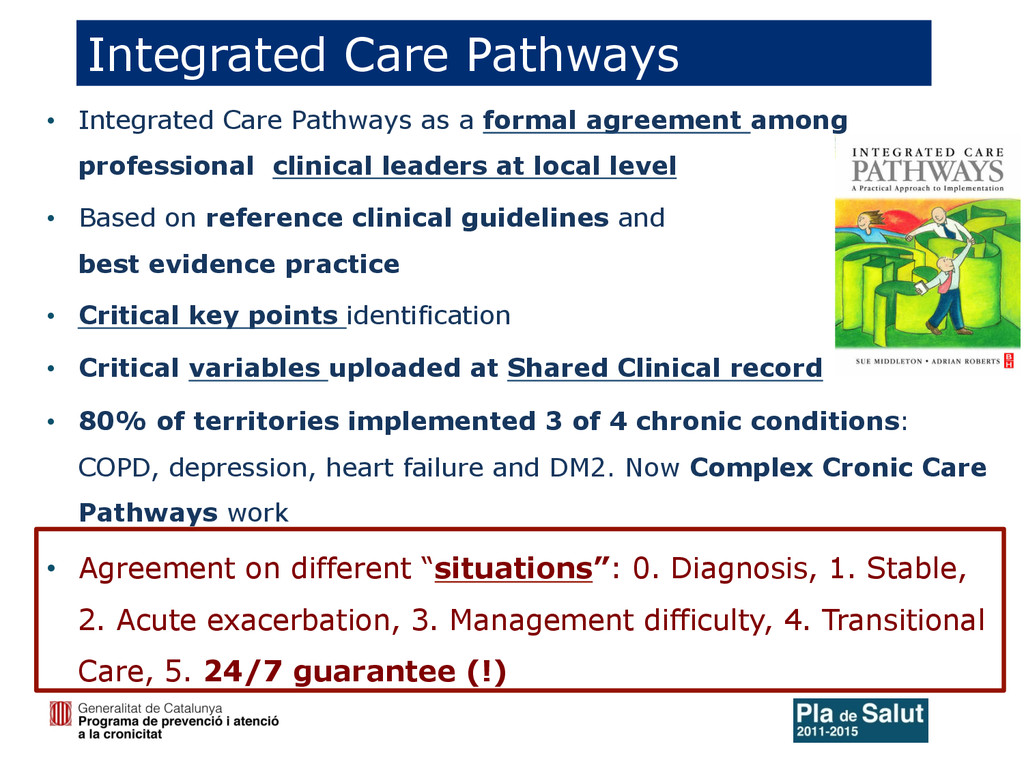
clinical leaders at local level • Based on reference clinical guidelines and best evidence practice • Critical key points identification • Critical variables uploaded at Shared Clinical record • 80% of territories implemented 3 of 4 chronic conditions: COPD, depression, heart failure and DM2. Now Complex Cronic Care Pathways work • Agreement on different “situations”: 0. Diagnosis, 1. Stable, 2. Acute exacerbation, 3. Management difficulty, 4. Transitional Care, 5. 24/7 guarantee (!) Integrated Care Pathways
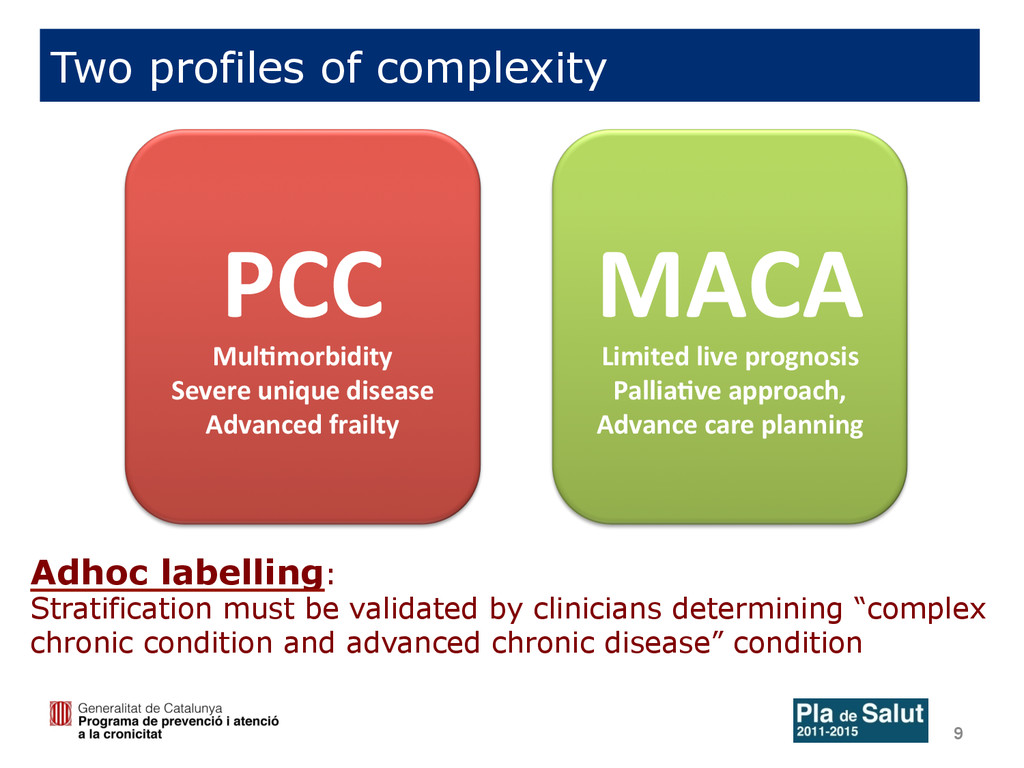
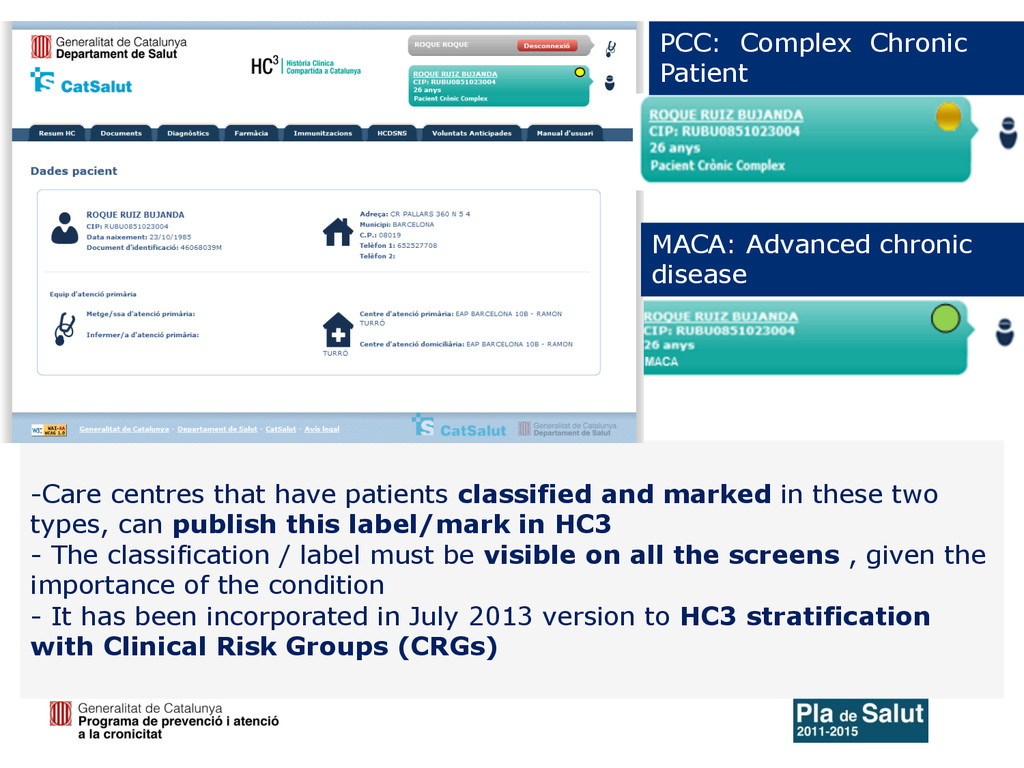
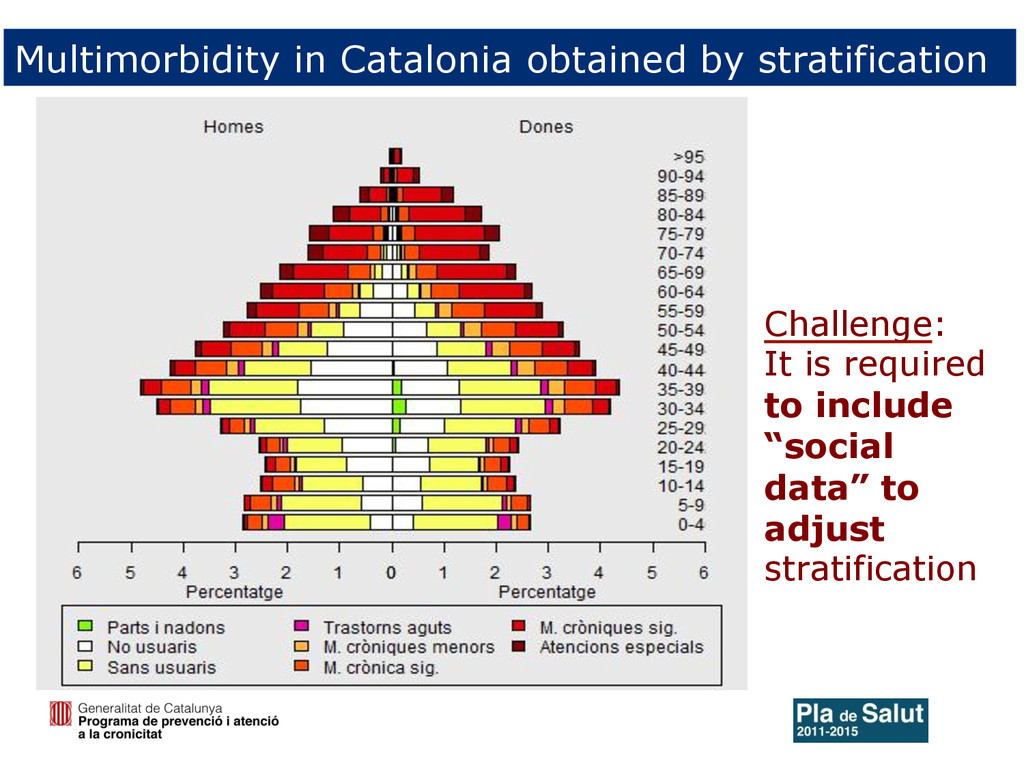
Advanced frailty MACA Limited live prognosis Pallia(ve approach, Advance care planning Two profiles of complexity Adhoc labelling: Stratification must be validated by clinicians determining “complex chronic condition and advanced chronic disease” condition
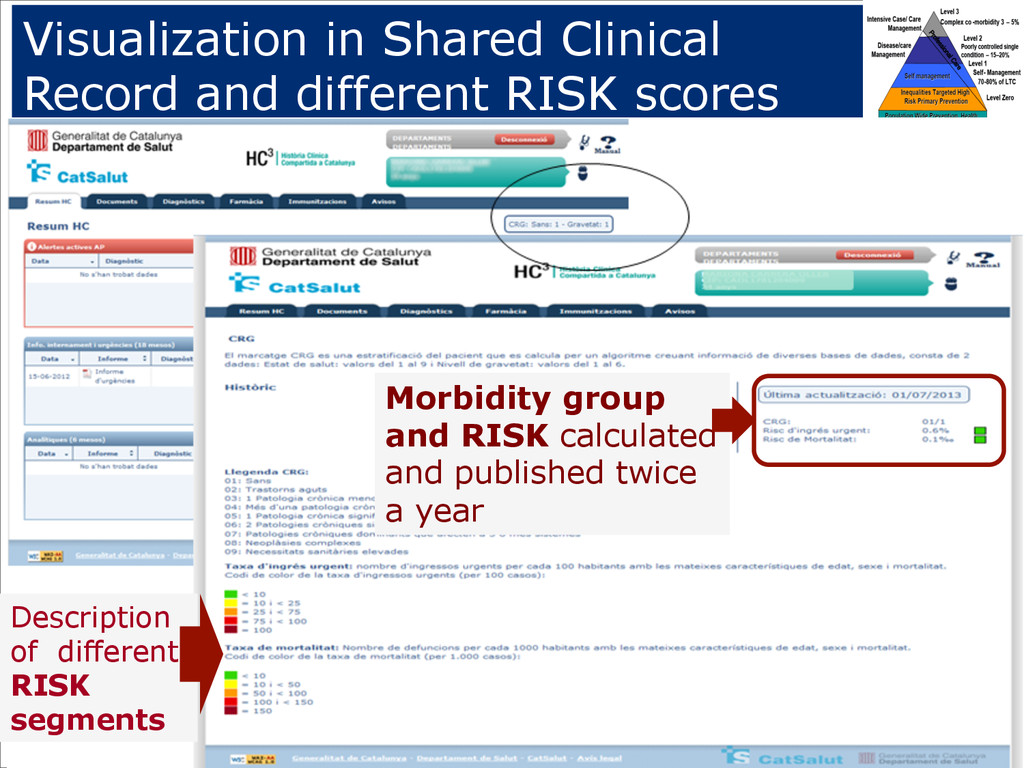
two types, can publish this label/mark in HC3 - The classification / label must be visible on all the screens , given the importance of the condition - It has been incorporated in July 2013 version to HC3 stratification with Clinical Risk Groups (CRGs) PCC: Complex Chronic Patient MACA: Advanced chronic disease
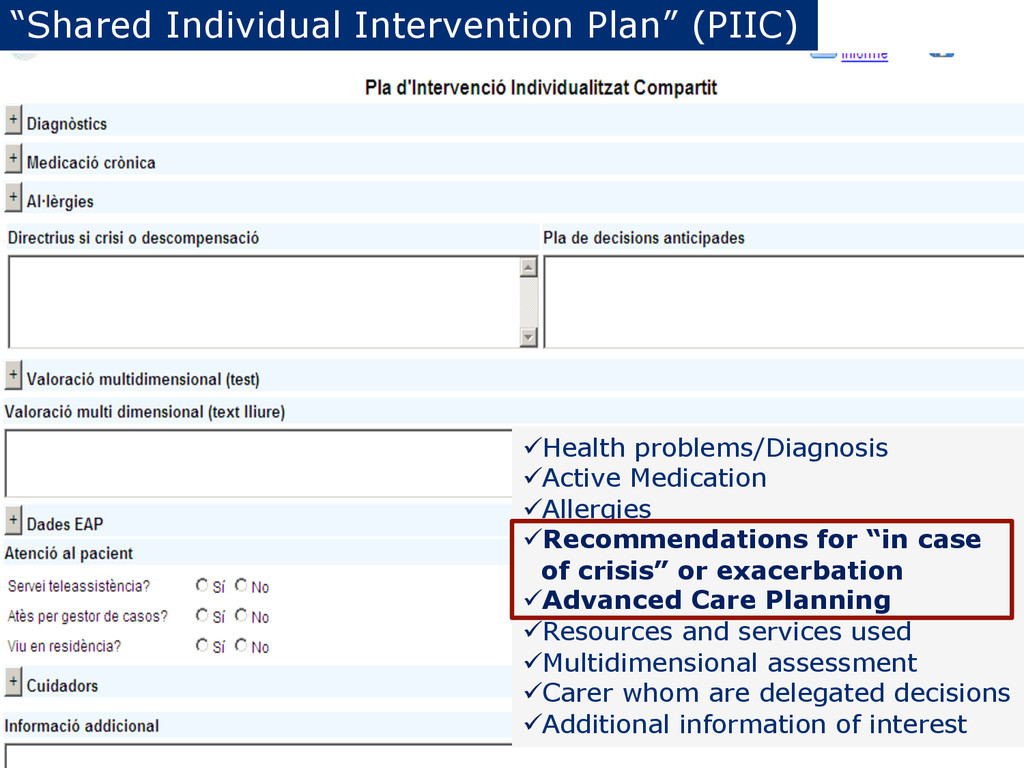
ü Recommendations for “in case of crisis” or exacerbation ü Advanced Care Planning ü Resources and services used ü Multidimensional assessment ü Carer whom are delegated decisions ü Additional information of interest
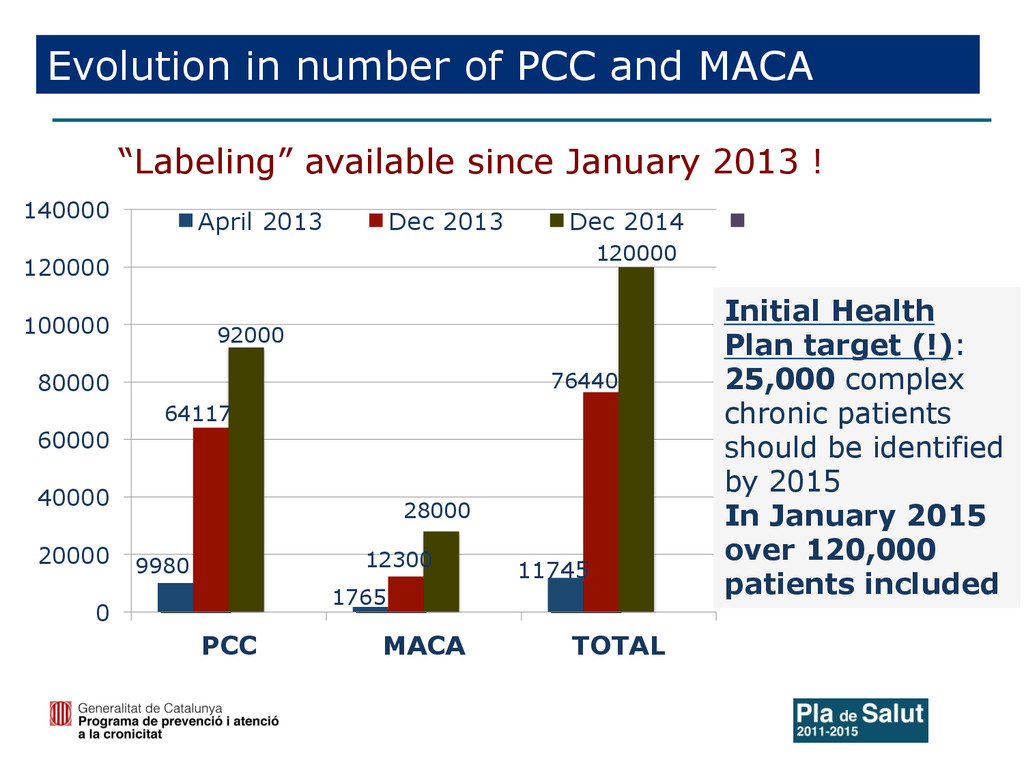
20000 40000 60000 80000 100000 120000 140000 PCC MACA TOTAL April 2013 Dec 2013 Dec 2014 Initial Health Plan target (!): 25,000 complex chronic patients should be identified by 2015 In January 2015 over 120,000 patients included Evolution in number of PCC and MACA “Labeling” available since January 2013 !
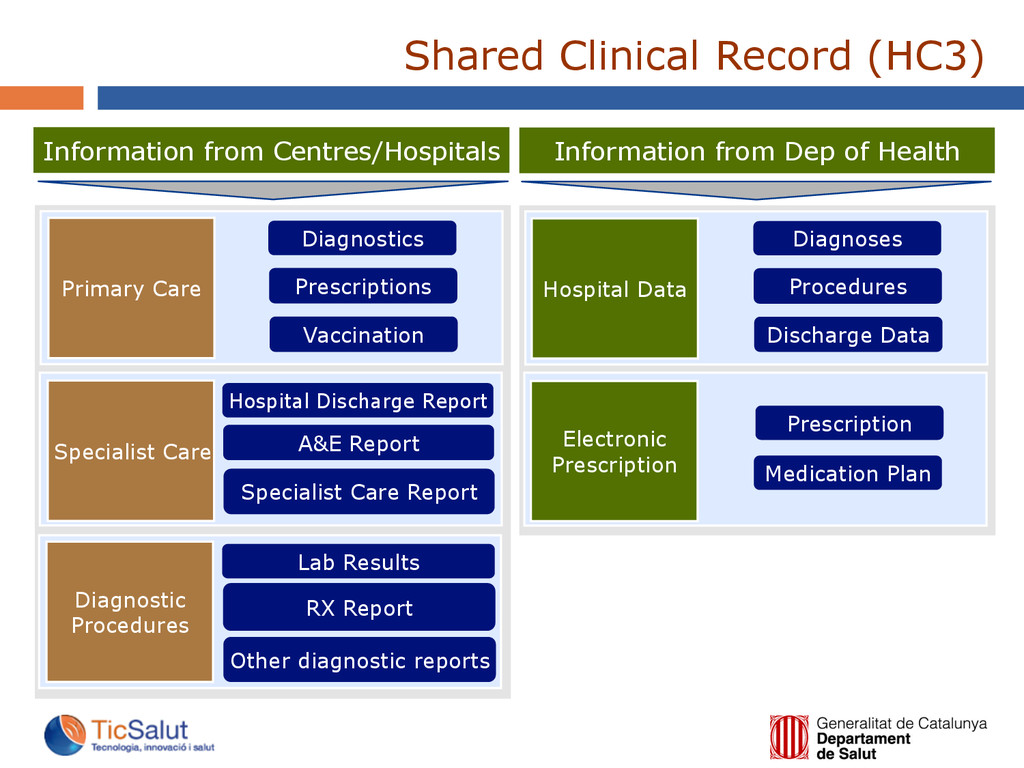
Prescriptions Vaccination Hospital Discharge Report A&E Report Specialist Care Report Lab Results RX Report Other diagnostic reports Hospital Data Information from Dep of Health Electronic Prescription Diagnoses Procedures Discharge Data Prescription Medication Plan Shared Clinical Record (HC3)
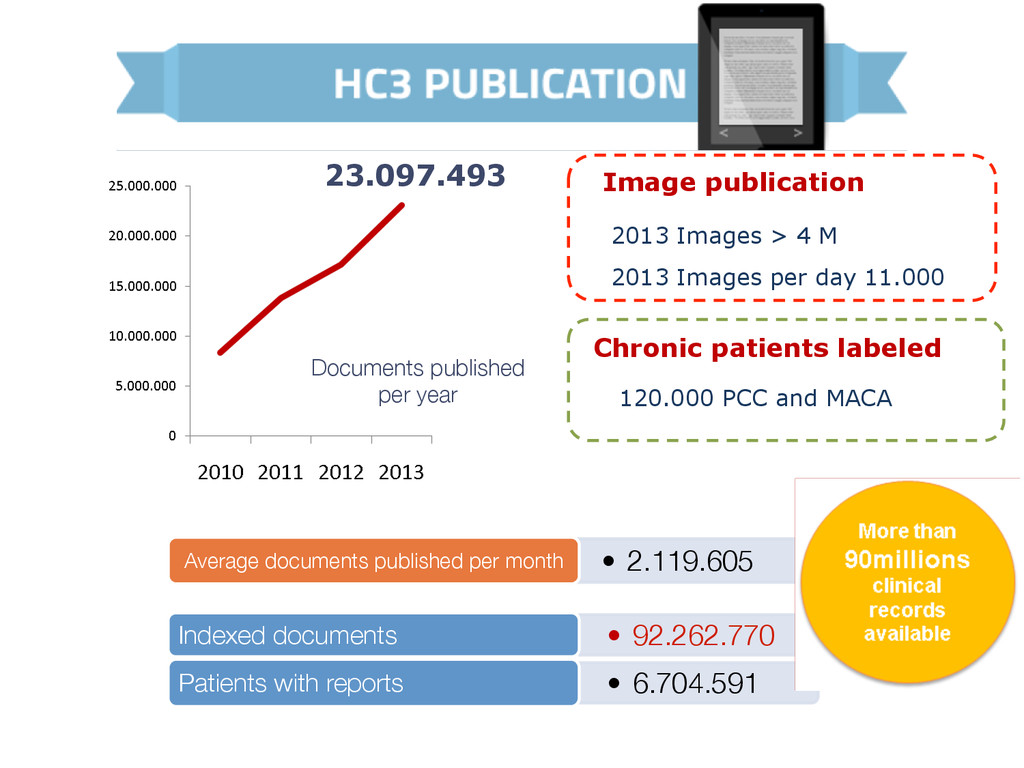
per month • 92.262.770 Indexed documents • 6.704.591 Patients with reports 2013 Images > 4 M 2013 Images per day 11.000 Image publication Chronic patients labeled 120.000 PCC and MACA
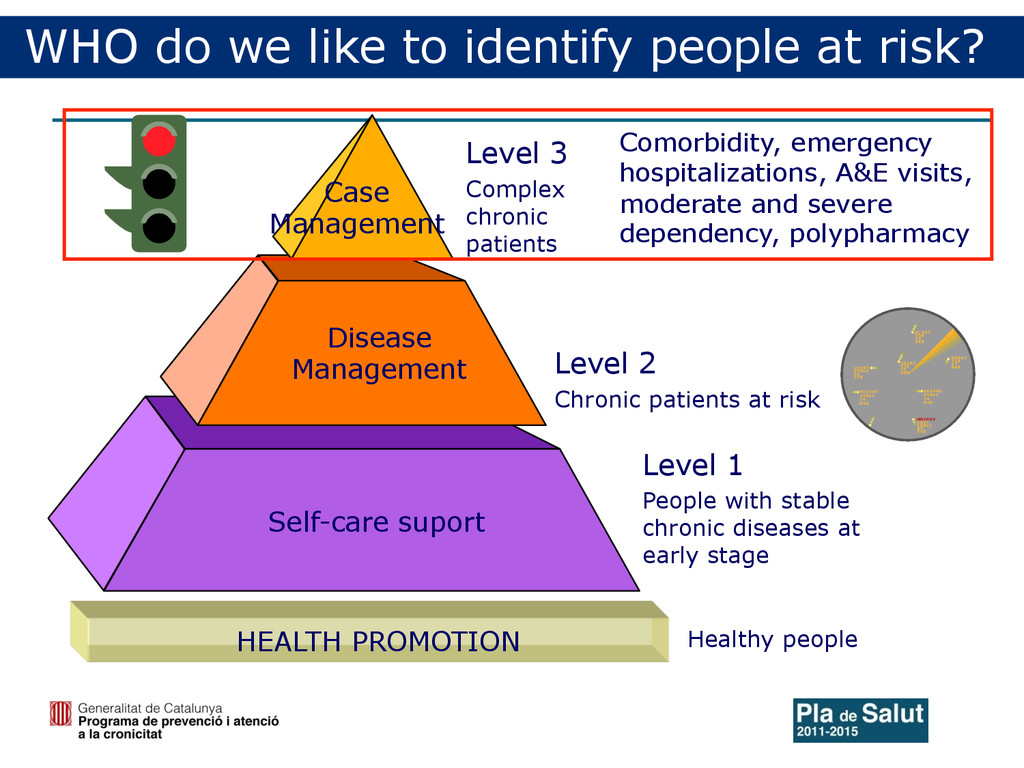
Self-care suport Level 1 People with stable chronic diseases at early stage Level 3 Complex chronic patients Comorbidity, emergency hospitalizations, A&E visits, moderate and severe dependency, polypharmacy HEALTH PROMOTION Healthy people WHO do we like to identify people at risk?
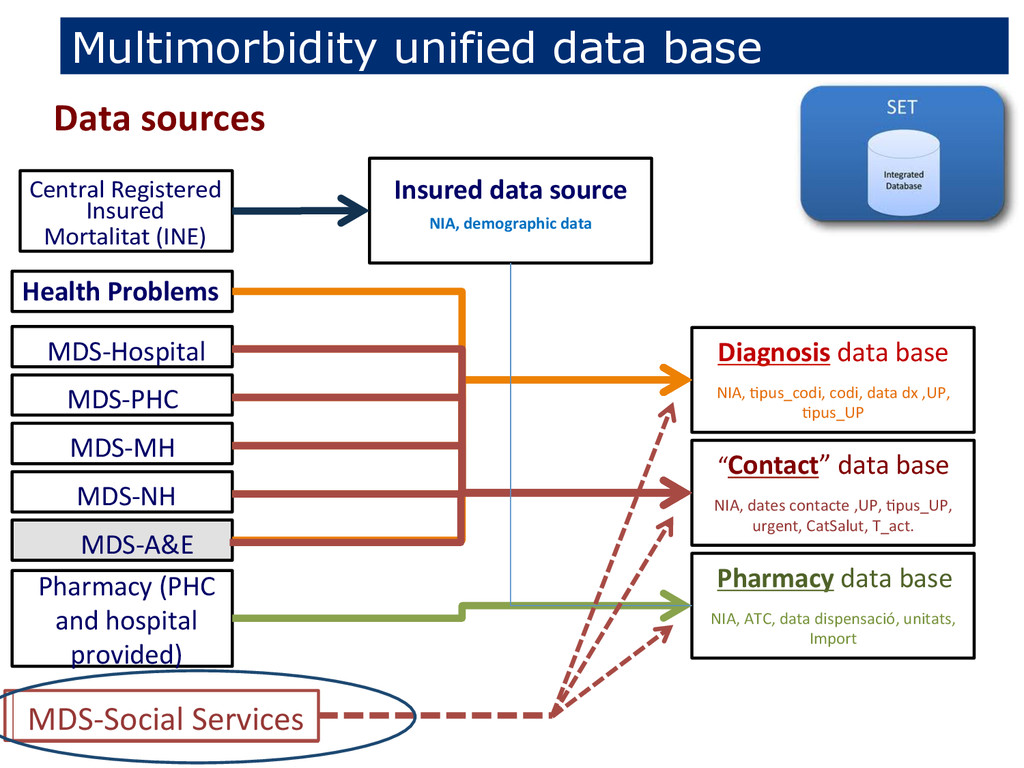
data Diagnosis data base NIA, .pus_codi, codi, data dx ,UP, .pus_UP “Contact” data base NIA, dates contacte ,UP, .pus_UP, urgent, CatSalut, T_act. MDS-‐Hospital MDS-‐PHC MDS-‐MH MDS-‐NH MDS-‐A&E Central Registered Insured Health Problems Pharmacy (PHC and hospital provided) Pharmacy data base NIA, ATC, data dispensació, unitats, Import Mortalitat (INE) Data sources MDS-‐Social Services
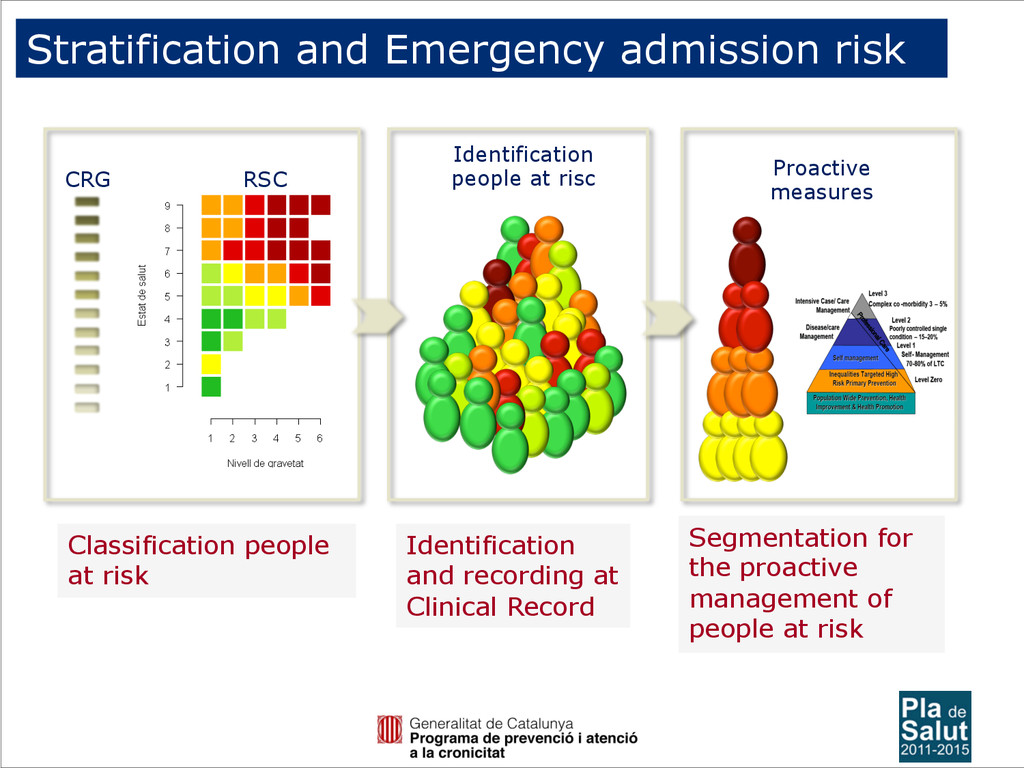
risc Proactive measures Classification people at risk Segmentation for the proactive management of people at risk Identification and recording at Clinical Record
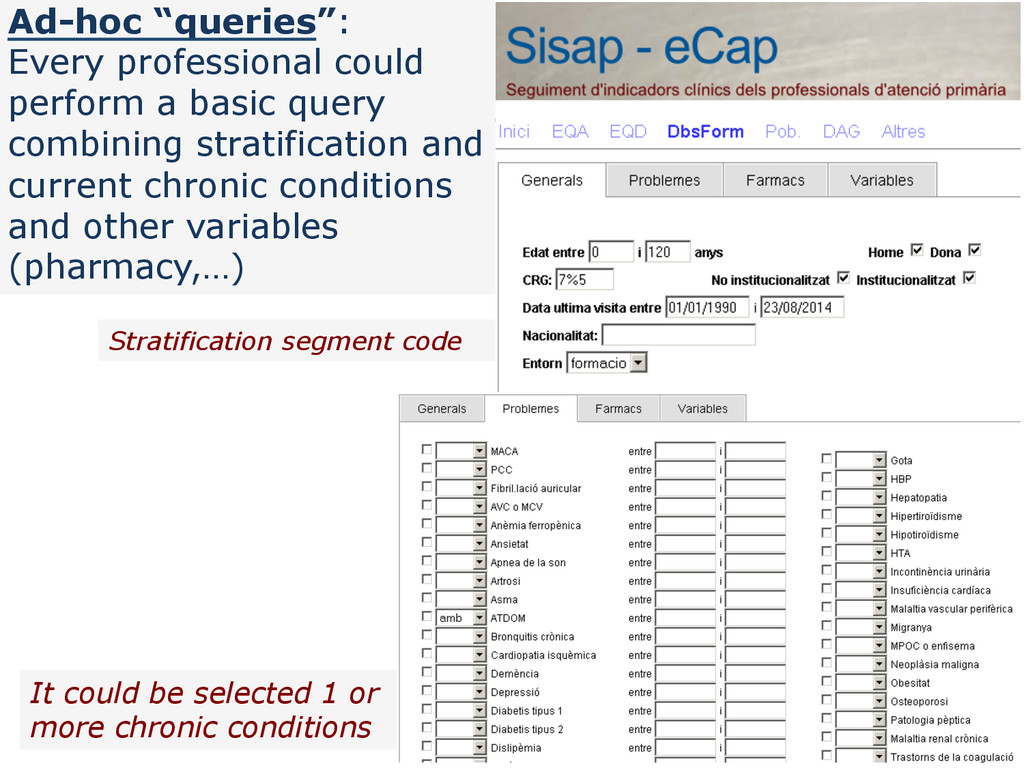
stratification and current chronic conditions and other variables (pharmacy,…) It could be selected 1 or more chronic conditions Stratification segment code
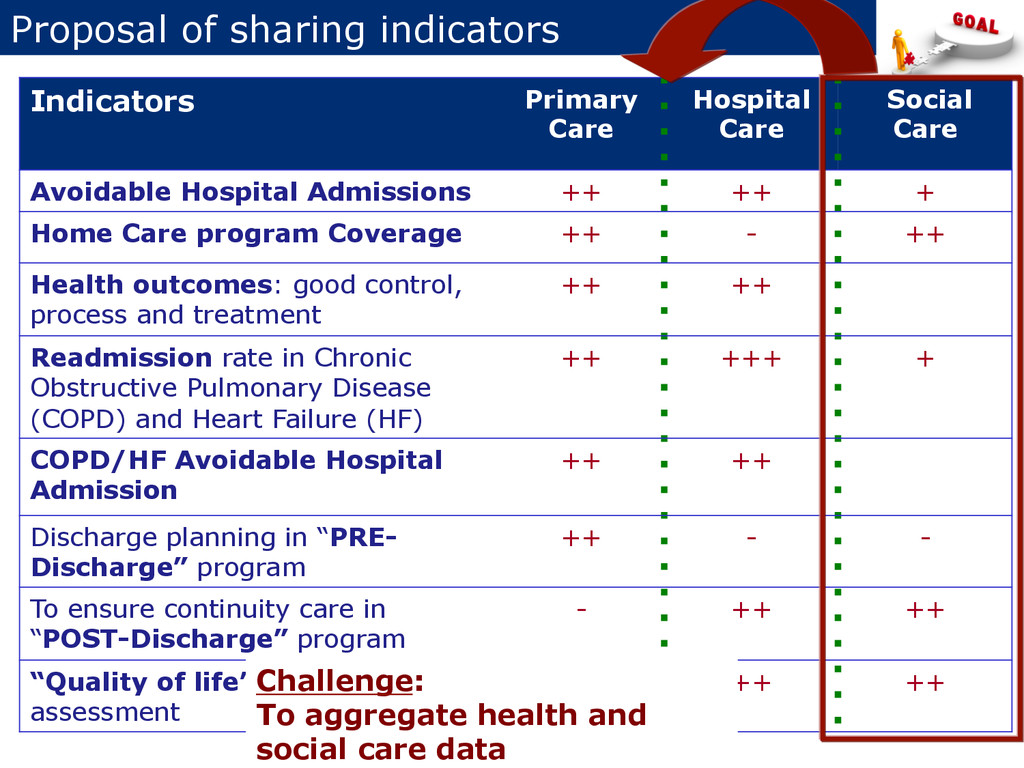
Care Avoidable Hospital Admissions ++ ++ + Home Care program Coverage ++ - ++ Health outcomes: good control, process and treatment ++ ++ Readmission rate in Chronic Obstructive Pulmonary Disease (COPD) and Heart Failure (HF) ++ +++ + COPD/HF Avoidable Hospital Admission ++ ++ Discharge planning in “PRE- Discharge” program ++ - - To ensure continuity care in “POST-Discharge” program - ++ ++ “Quality of life” (HRQoL) assessment ++ ++ ++ Challenge: To aggregate health and social care data
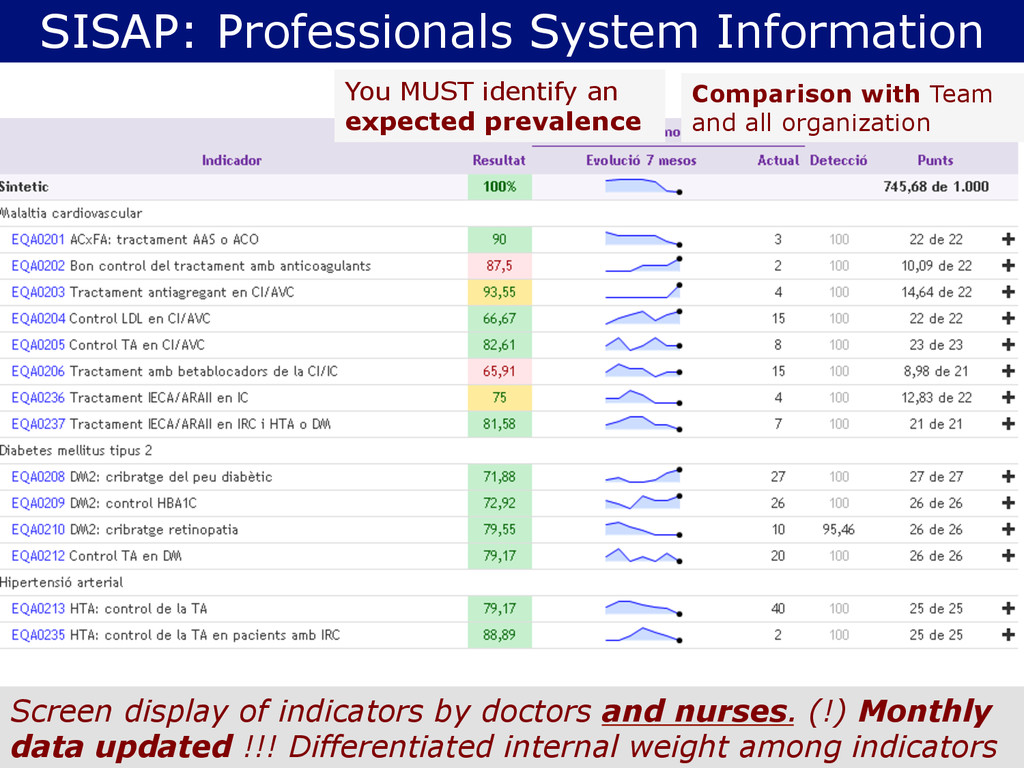
Comparison with Team and all organization Screen display of indicators by doctors and nurses. (!) Monthly data updated !!! Differentiated internal weight among indicators
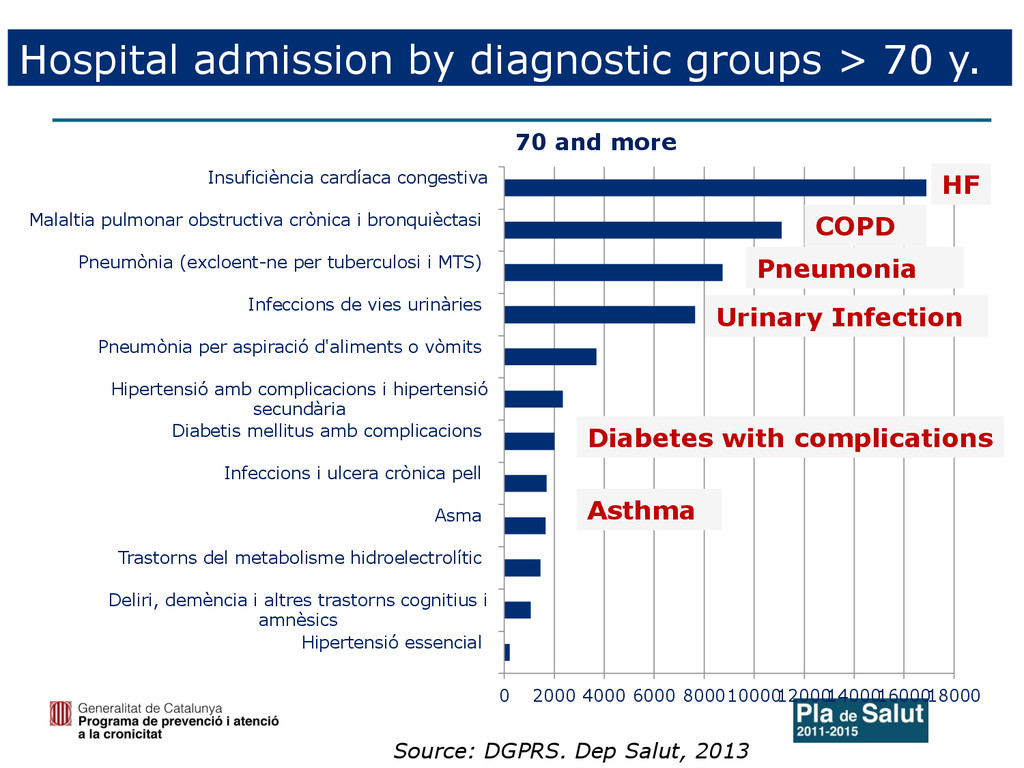
4000 6000 8000 10000 12000 14000 16000 18000 Hipertensió essencial Deliri, demència i altres trastorns cognitius i amnèsics Trastorns del metabolisme hidroelectrolític Asma Infeccions i ulcera crònica pell Diabetis mellitus amb complicacions Hipertensió amb complicacions i hipertensió secundària Pneumònia per aspiració d'aliments o vòmits Infeccions de vies urinàries Pneumònia (excloent-ne per tuberculosi i MTS) Malaltia pulmonar obstructiva crònica i bronquièctasi Insuficiència cardíaca congestiva 70 and more Pneumonia Source: DGPRS. Dep Salut, 2013 COPD HF Urinary Infection Asthma Diabetes with complications
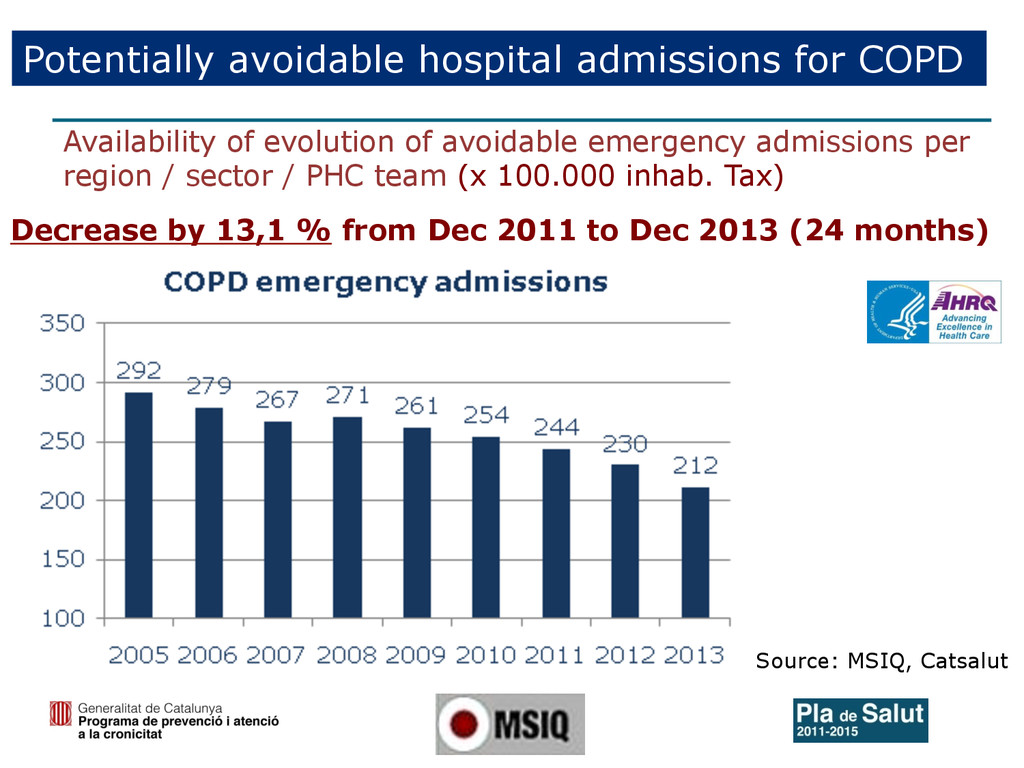
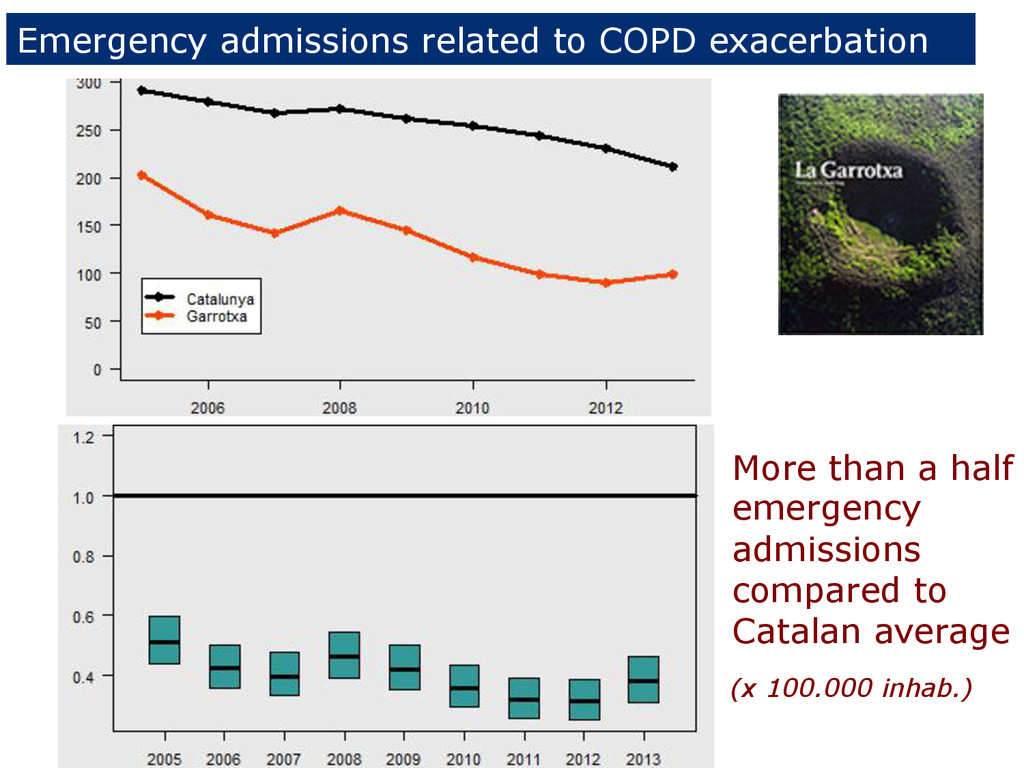
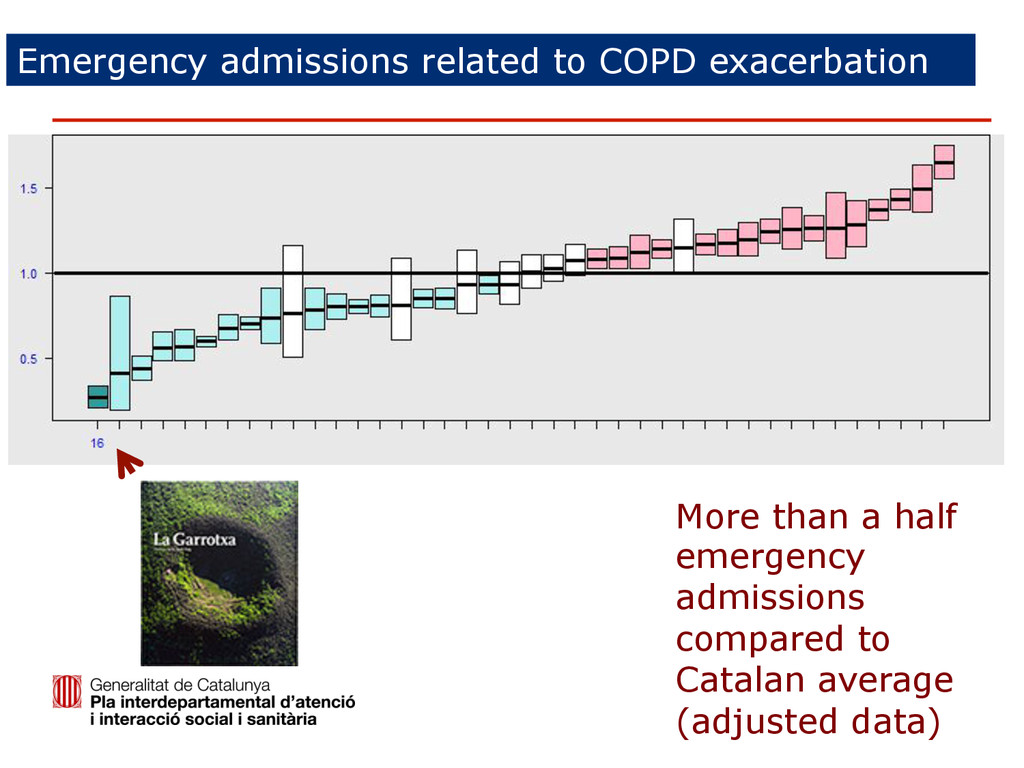
from Dec 2011 to Dec 2013 (24 months) Availability of evolution of avoidable emergency admissions per region / sector / PHC team (x 100.000 inhab. Tax) Source: MSIQ, Catsalut
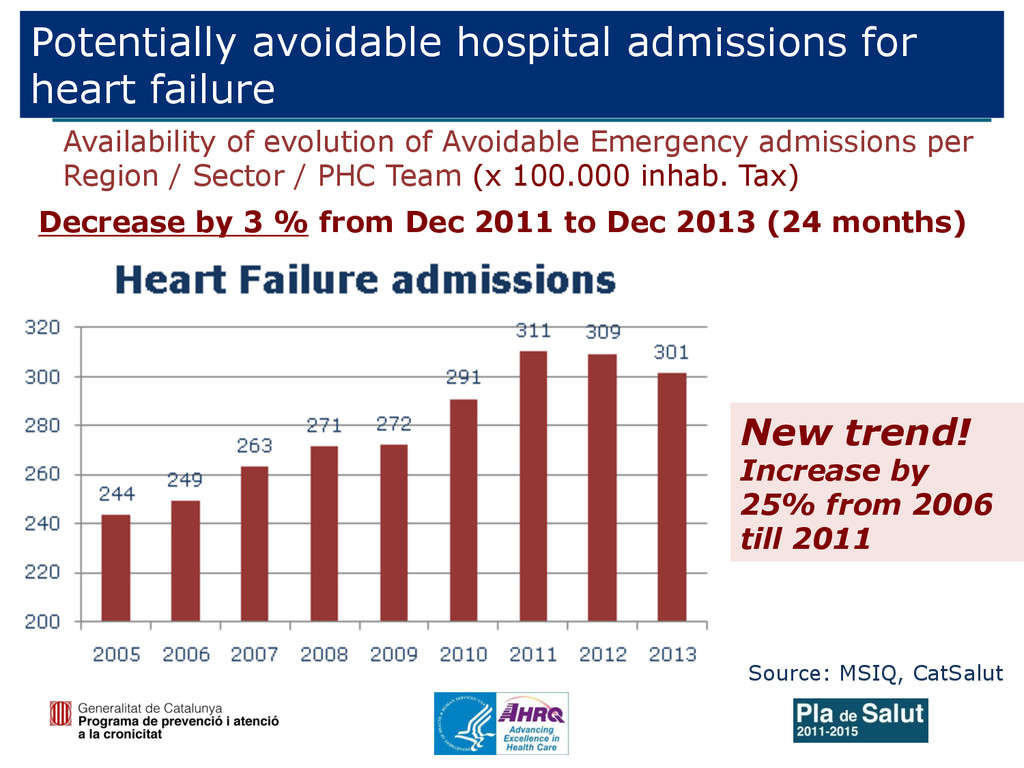
Decrease by 3 % from Dec 2011 to Dec 2013 (24 months) Availability of evolution of Avoidable Emergency admissions per Region / Sector / PHC Team (x 100.000 inhab. Tax) New trend! Increase by 25% from 2006 till 2011
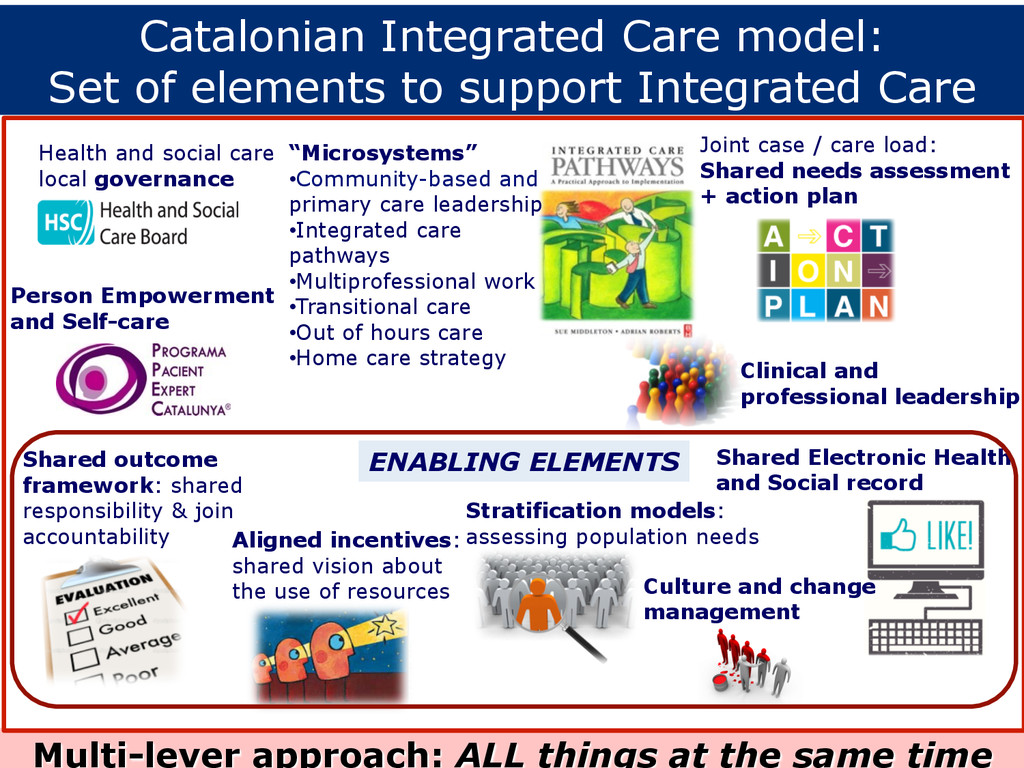
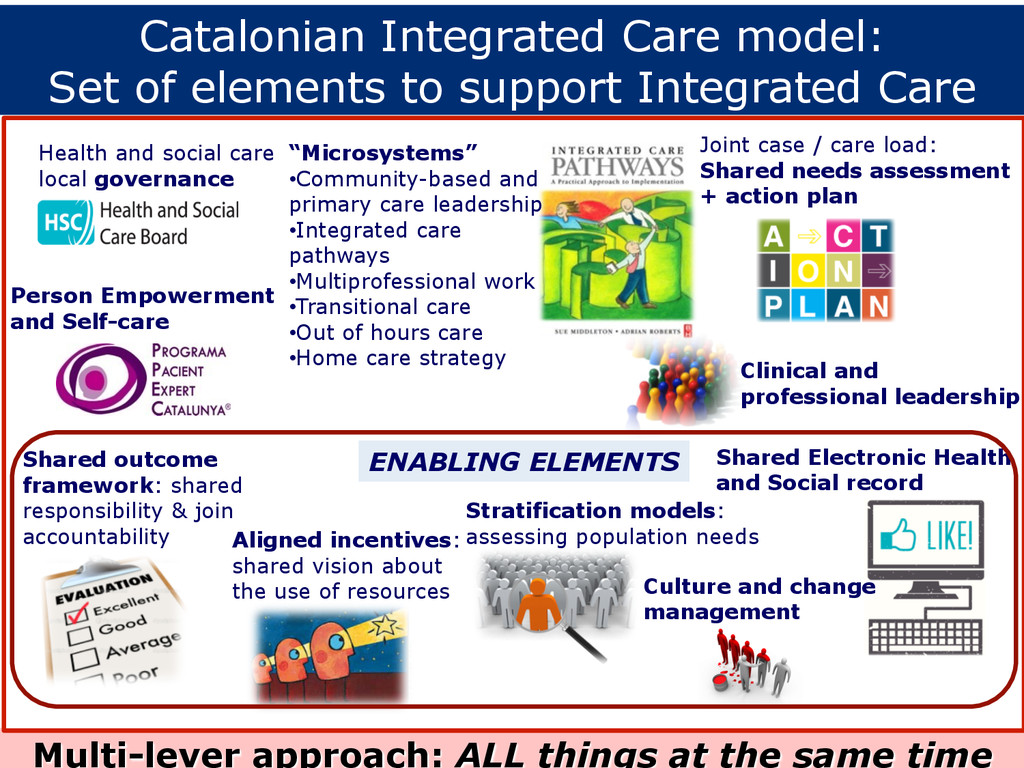
work • Transitional care • Out of hours care • Home care strategy Joint case / care load: Shared needs assessment + action plan Stratification models: assessing population needs Clinical and professional leadership Health and social care local governance Shared outcome framework: shared responsibility & join accountability Aligned incentives: shared vision about the use of resources Shared Electronic Health and Social record Person Empowerment and Self-care ENABLING ELEMENTS Multi-lever approach: ALL things at the same time Culture and change management Catalonian Integrated Care model: Set of elements to support Integrated Care
record • Identify the person with the CIP (Identification Number) as a common identifier. • Prior agreement on the coding and register of social problems. • Prepare the local social services information system for it to be ‘interoperable’ in a short-medium term and provide a minimum set of information and variables for a Shared Social and Clinical Record • Access to a minimum set of information and variables of common interest on social field for the Shared Clinical Record of Catalonia (HC3). 1st stage: generation of a Social Intervention Plan incorporated to HC3. 2nd stage: Shared Individual Intervention Plan. • Communication systems to improve accessibility, messaging and virtual work between social and health areas. • Introduce social variables gradually to available health stratification. Challenges to construct and Integrated Health and Social Care record
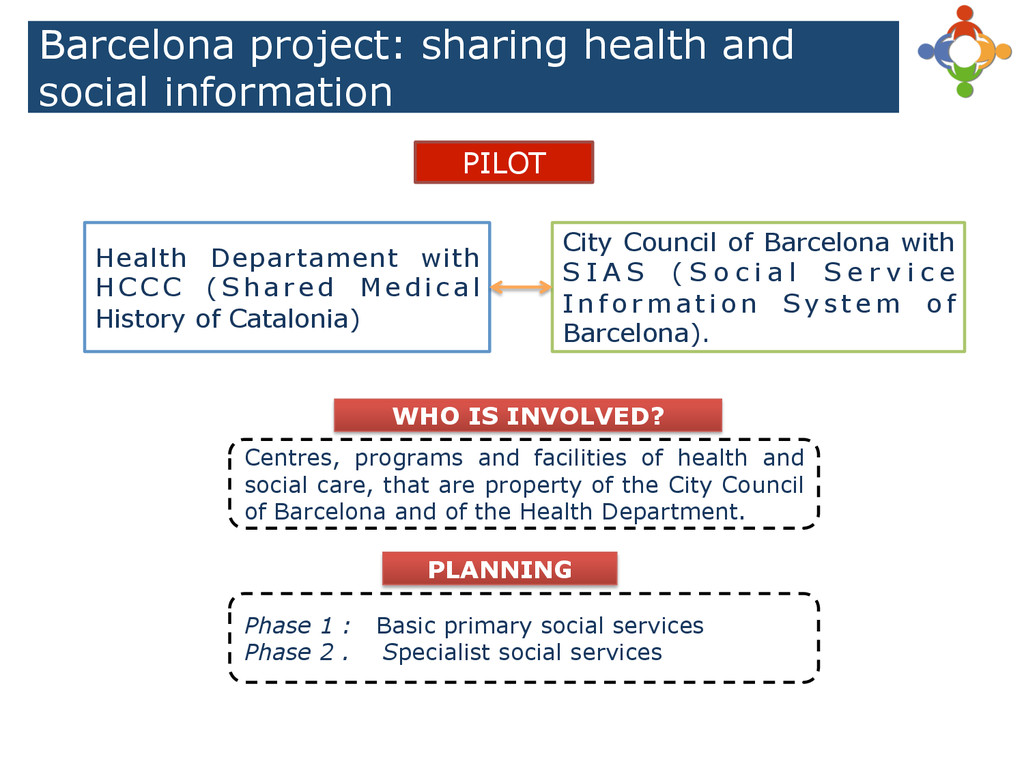
with H C C C ( S h a r e d M e d i c a l History of Catalonia) City Council of Barcelona with S I A S ( S o c i a l S e r v i c e I n f o r m a t i o n S y s t e m o f Barcelona). Centres, programs and facilities of health and social care, that are property of the City Council of Barcelona and of the Health Department. Phase 1 : Basic primary social services Phase 2 . Specialist social services WHO IS INVOLVED? PLANNING
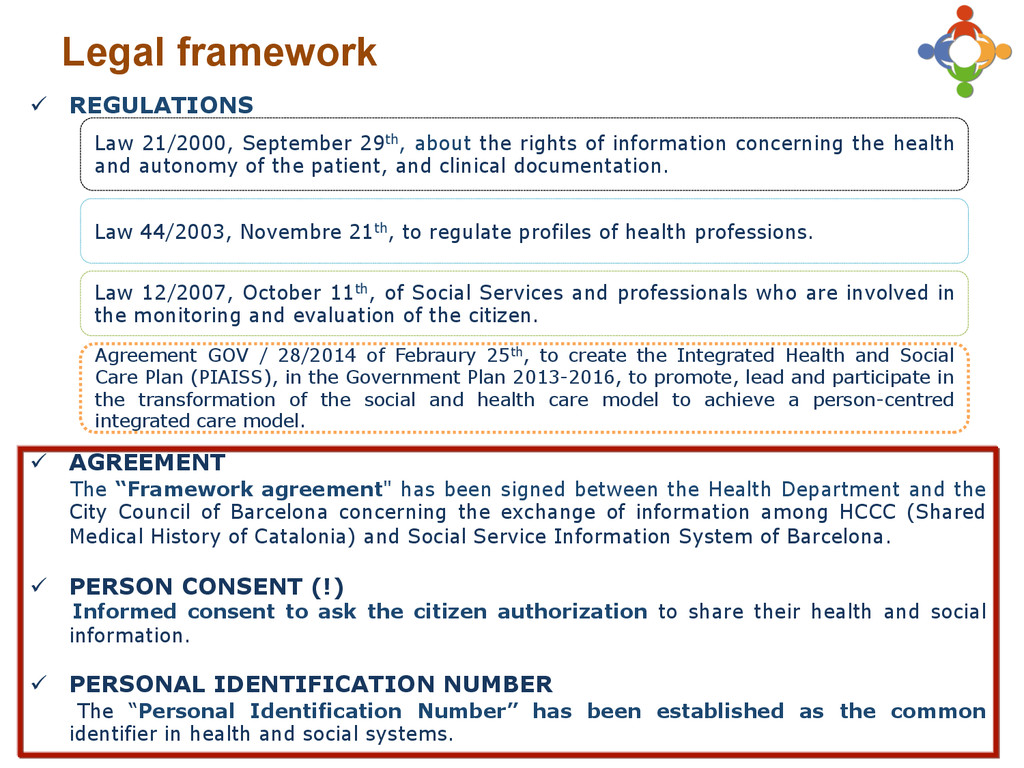
been signed between the Health Department and the City Council of Barcelona concerning the exchange of information among HCCC (Shared Medical History of Catalonia) and Social Service Information System of Barcelona. ü PERSON CONSENT (!) Informed consent to ask the citizen authorization to share their health and social information. ü PERSONAL IDENTIFICATION NUMBER The “Personal Identification Number” has been established as the common identifier in health and social systems. Law 12/2007, October 11th, of Social Services and professionals who are involved in the monitoring and evaluation of the citizen. Law 21/2000, September 29th, about the rights of information concerning the health and autonomy of the patient, and clinical documentation. Law 44/2003, Novembre 21th, to regulate profiles of health professions. Agreement GOV / 28/2014 of Febraury 25th, to create the Integrated Health and Social Care Plan (PIAISS), in the Government Plan 2013-2016, to promote, lead and participate in the transformation of the social and health care model to achieve a person-centred integrated care model.
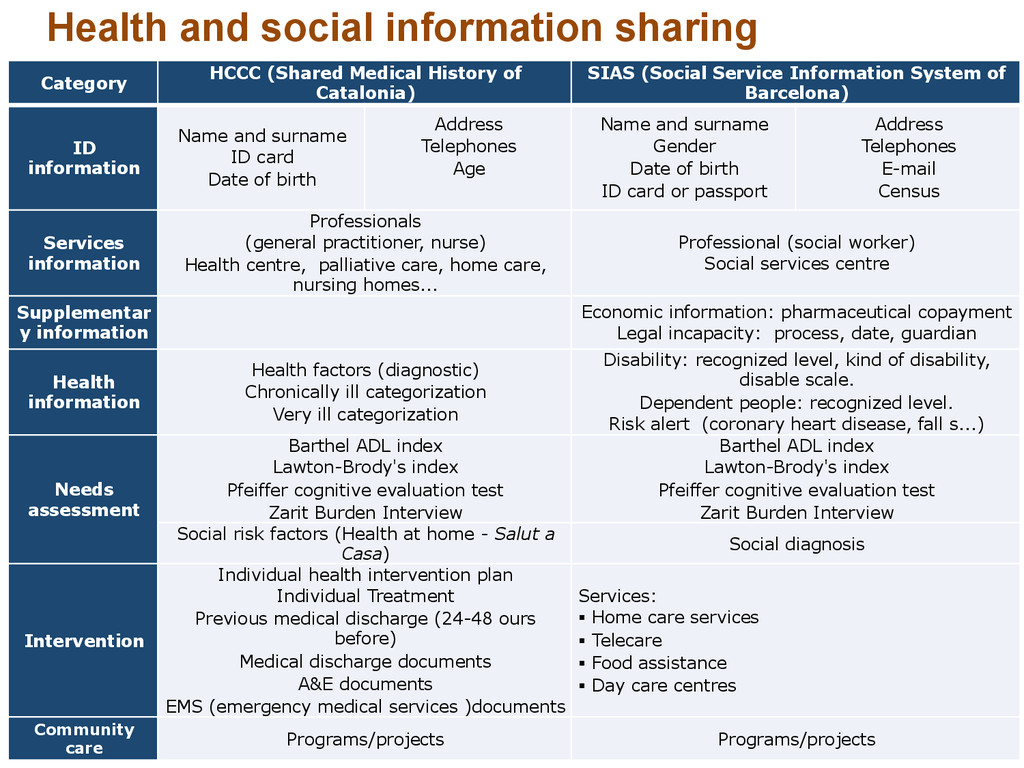
Medical History of Catalonia) SIAS (Social Service Information System of Barcelona) ID information Name and surname ID card Date of birth Address Telephones Age Name and surname Gender Date of birth ID card or passport Address Telephones E-mail Census Services information Professionals (general practitioner, nurse) Health centre, palliative care, home care, nursing homes... Professional (social worker) Social services centre Supplementar y information Economic information: pharmaceutical copayment Legal incapacity: process, date, guardian Health information Health factors (diagnostic) Chronically ill categorization Very ill categorization Disability: recognized level, kind of disability, disable scale. Dependent people: recognized level. Risk alert (coronary heart disease, fall s...) Needs assessment Barthel ADL index Lawton-Brody's index Pfeiffer cognitive evaluation test Zarit Burden Interview Barthel ADL index Lawton-Brody's index Pfeiffer cognitive evaluation test Zarit Burden Interview Social risk factors (Health at home - Salut a Casa) Social diagnosis Intervention Individual health intervention plan Individual Treatment Previous medical discharge (24-48 ours before) Medical discharge documents A&E documents EMS (emergency medical services )documents Services: § Home care services § Telecare § Food assistance § Day care centres Community care Programs/projects Programs/projects
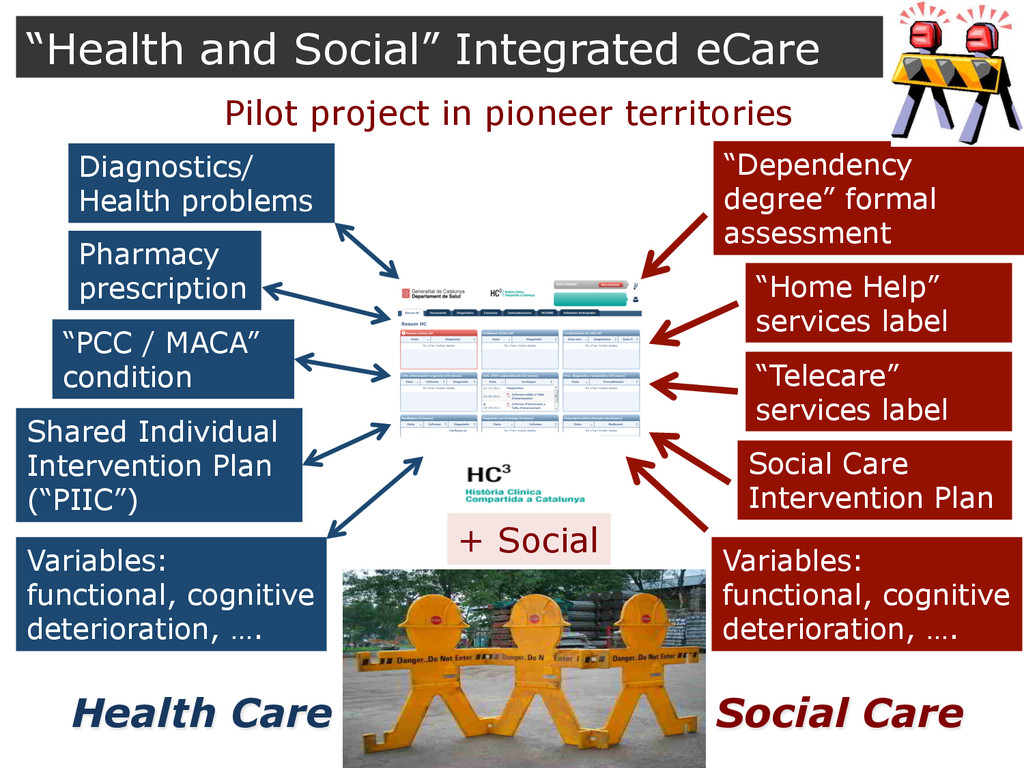
Health problems “Dependency degree” formal assessment “Home Help” services label “Telecare” services label Social Care Intervention Plan Pharmacy prescription Health Care Social Care + Social “Health and Social” Integrated eCare Pilot project in pioneer territories Variables: functional, cognitive deterioration, …. Variables: functional, cognitive deterioration, ….
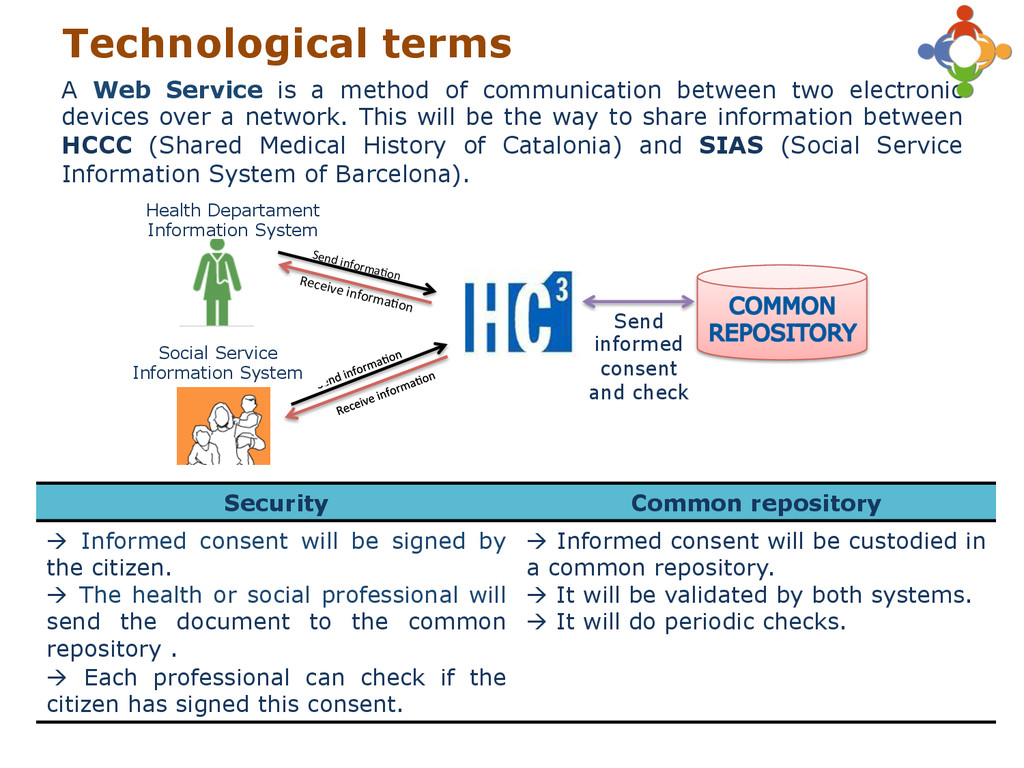
electronic devices over a network. This will be the way to share information between HCCC (Shared Medical History of Catalonia) and SIAS (Social Service Information System of Barcelona). Security Common repository à Informed consent will be signed by the citizen. à The health or social professional will send the document to the common repository . à Each professional can check if the citizen has signed this consent. à Informed consent will be custodied in a common repository. à It will be validated by both systems. à It will do periodic checks. Send informa.on Receive informa.on Send informed consent and check Technological terms Health Departament Information System Social Service Information System
AND SOCIAL NEEDS HIGH HEALTH AND SOCIAL COMPLEXITY 1 2 3 4 5 6 7 Complex health and social needs ? The need of incorporating Social Services in the definition of a JOINT Care Plan
1. To adapt a validated commercial solution: interRAI, SMAF,… 2. To construct a shared need assessment instrument based on professional consensus *It is required to facilitate collaborative environment between professionals working in different areas of health and social services
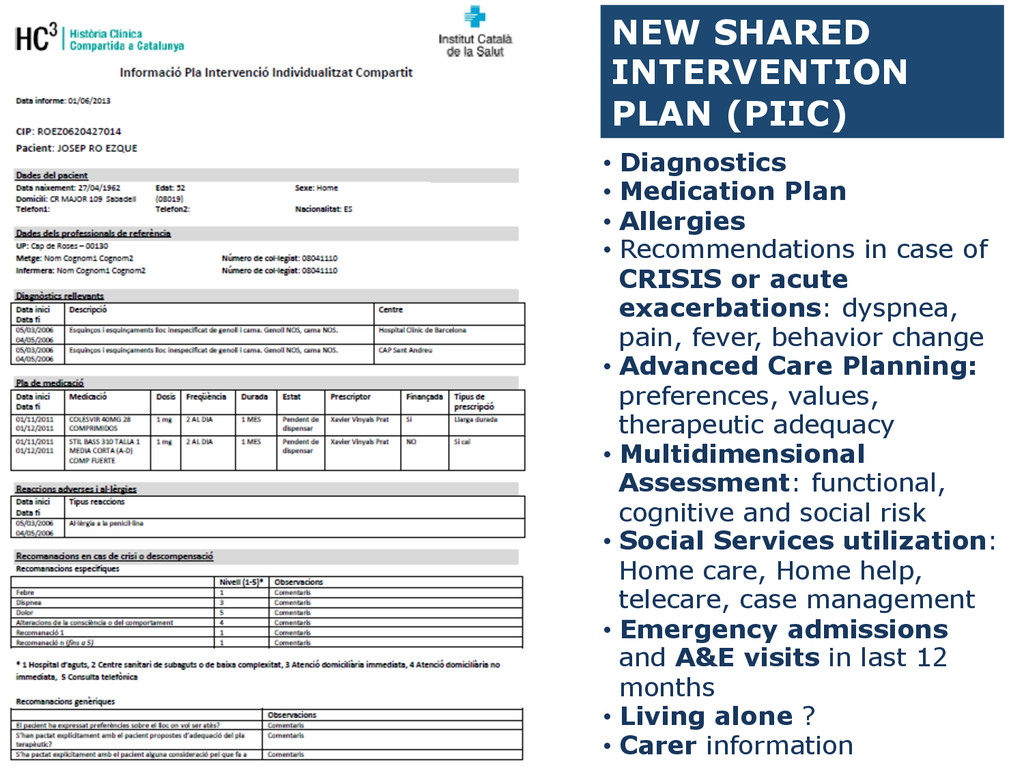
in case of CRISIS or acute exacerbations: dyspnea, pain, fever, behavior change • Advanced Care Planning: preferences, values, therapeutic adequacy • Multidimensional Assessment: functional, cognitive and social risk • Social Services utilization: Home care, Home help, telecare, case management • Emergency admissions and A&E visits in last 12 months • Living alone ? • Carer information
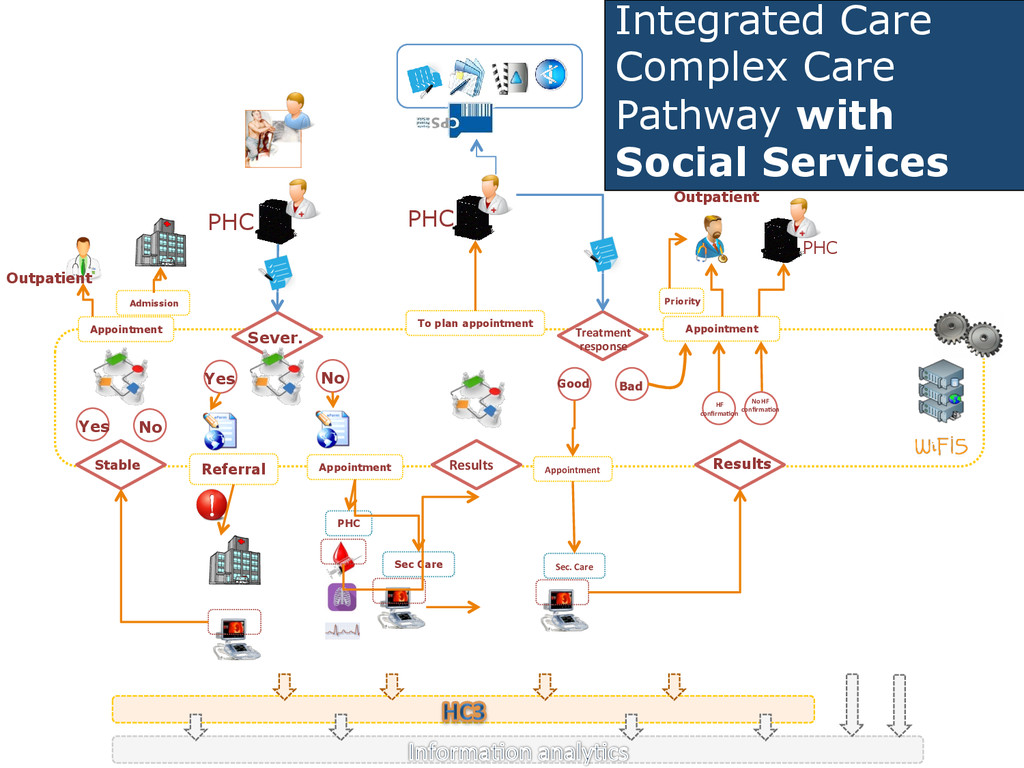
Referral Appointment Results PHC Sec Care PHC To plan appointment Treatment response Sec. Care Good Appointment Bad Results HF confirma(on Appointment Outpatient No HF confirma(on Priority PHC Yes No Stable Yes No Appointment Outpatient Admission
work • Transitional care • Out of hours care • Home care strategy Joint case / care load: Shared needs assessment + action plan Stratification models: assessing population needs Clinical and professional leadership Health and social care local governance Shared outcome framework: shared responsibility & join accountability Aligned incentives: shared vision about the use of resources Shared Electronic Health and Social record Person Empowerment and Self-care ENABLING ELEMENTS Multi-lever approach: ALL things at the same time Culture and change management Catalonian Integrated Care model: Set of elements to support Integrated Care
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}