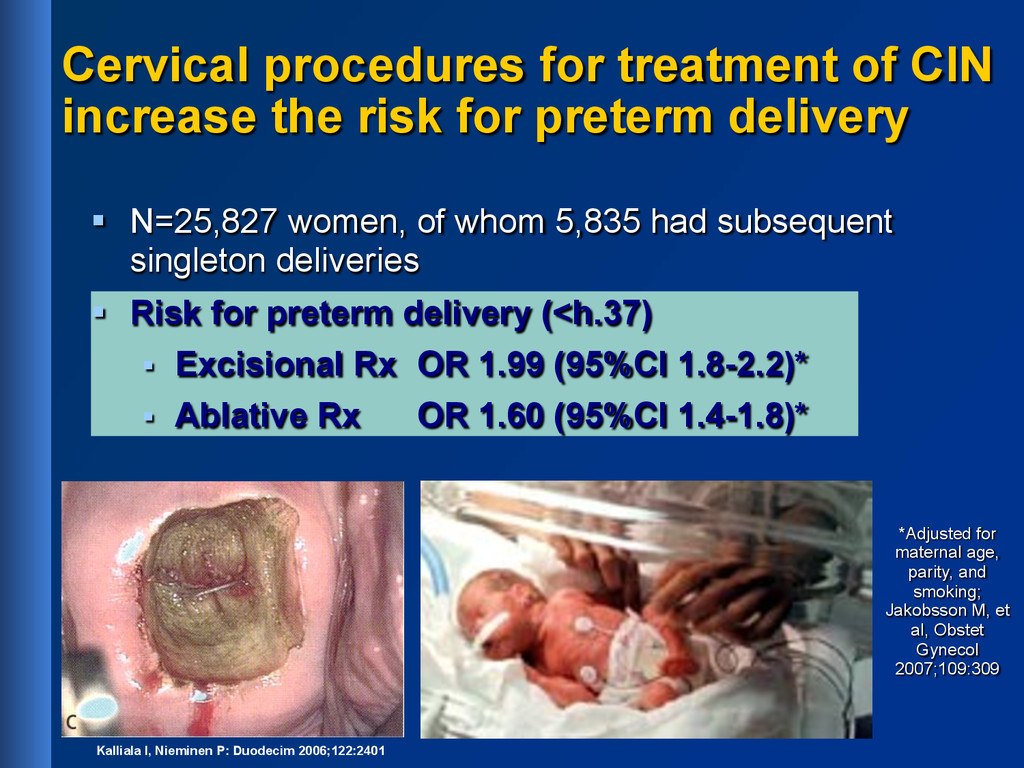
preterm delivery § N=25,827 women, of whom 5,835 had subsequent singleton deliveries § Risk for preterm delivery (<h.37) § Excisional Rx OR 1.99 (95%CI 1.8-2.2)* § Ablative Rx OR 1.60 (95%CI 1.4-1.8)* *Adjusted for maternal age, parity, and smoking; Jakobsson M, et al, Obstet Gynecol 2007;109:309 Kalliala I, Nieminen P: Duodecim 2006;122:2401
§ High risk HPV types § Strong data from ATHENA trial (N=47,000) 1 § Negative predictive value (NPV) 99,7 % 2 1 Wright TC, et al. Primary Cervical Cancer Screening with Human Papillomavirus: End of Study Results from the ATHENA study using HPV as the First-line Screening Test. Gynecol Oncol 2014 12Castle PE et al. Lancet Oncol 2011; 12(9): 880-906
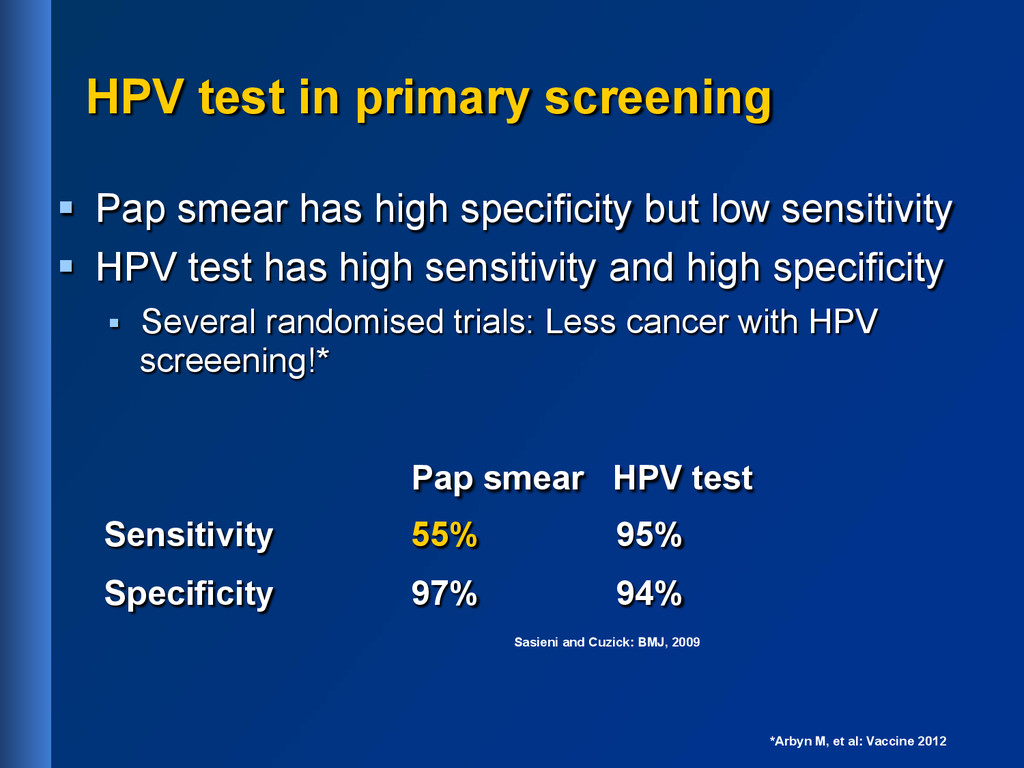
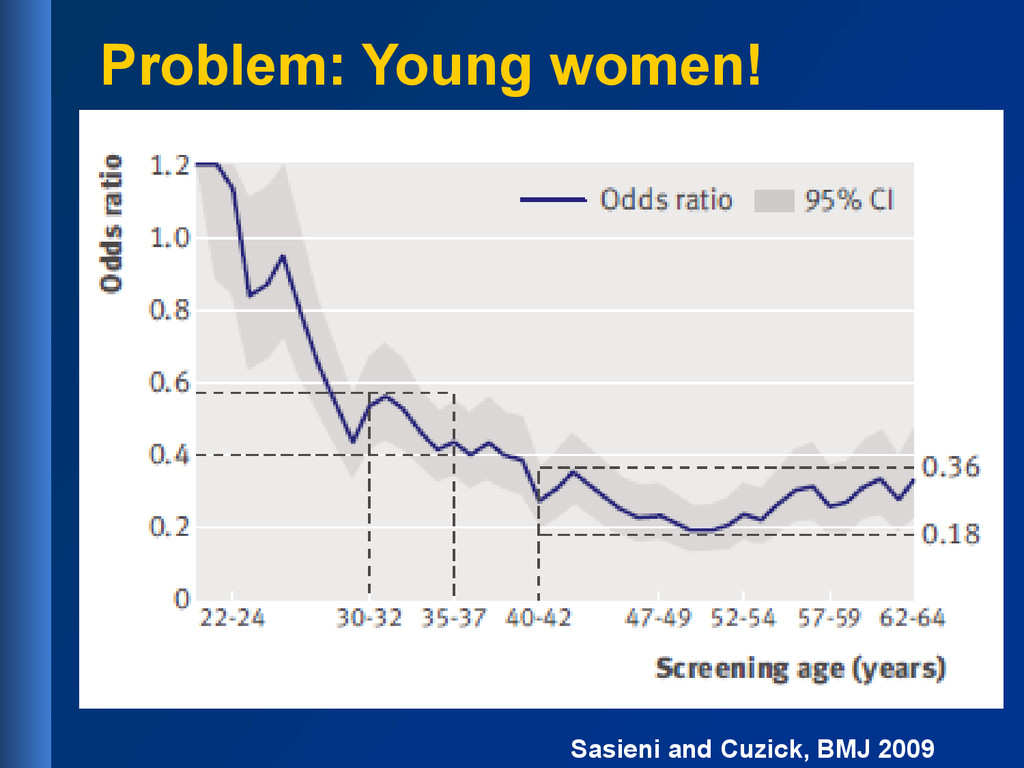
specificity but low sensitivity § HPV test has high sensitivity and high specificity § Several randomised trials: Less cancer with HPV screeening!* Pap smear HPV test Sensitivity 55% 95% Specificity 97% 94% Sasieni and Cuzick: BMJ, 2009 *Arbyn M, et al: Vaccine 2012
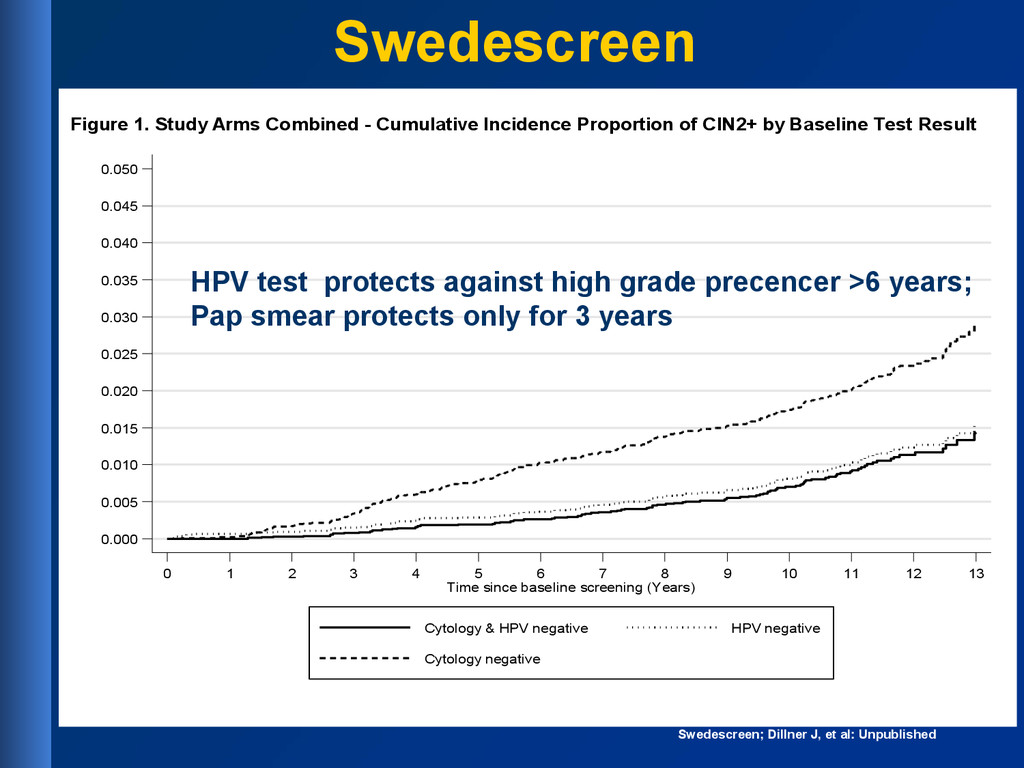
0.050 0 1 2 3 4 5 6 7 8 9 10 11 12 13 Time since baseline screening (Years) Cytology & HPV negative HPV negative Cytology negative Figure 1. Study Arms Combined - Cumulative Incidence Proportion of CIN2+ by Baseline Test Result Swedescreen; Dillner J, et al: Unpublished HPV test protects against high grade precencer >6 years; Pap smear protects only for 3 years Swedescreen
sensitive than cytology and protects longer § Costs of HPV tests are decreasing § HPV screening followed by cytology § Start with a sensitive test (HPV test) § Continue with a specific test (Pap smear) § Self-sampling increases participation rate § Organised screening program necessary § Opportunistic screening is not cost-effective
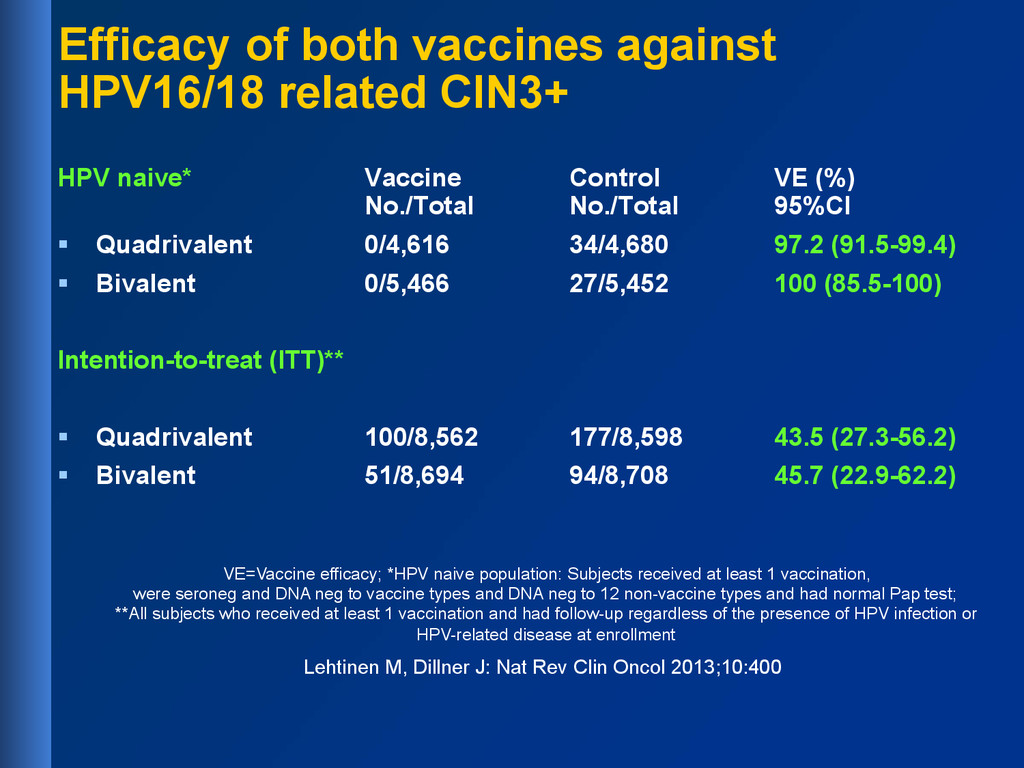
Vaccine Control VE (%) No./Total No./Total 95%CI § Quadrivalent 0/4,616 34/4,680 97.2 (91.5-99.4) § Bivalent 0/5,466 27/5,452 100 (85.5-100) Intention-to-treat (ITT)** § Quadrivalent 100/8,562 177/8,598 43.5 (27.3-56.2) § Bivalent 51/8,694 94/8,708 45.7 (22.9-62.2) VE=Vaccine efficacy; *HPV naive population: Subjects received at least 1 vaccination, were seroneg and DNA neg to vaccine types and DNA neg to 12 non-vaccine types and had normal Pap test; **All subjects who received at least 1 vaccination and had follow-up regardless of the presence of HPV infection or HPV-related disease at enrollment Lehtinen M, Dillner J: Nat Rev Clin Oncol 2013;10:400
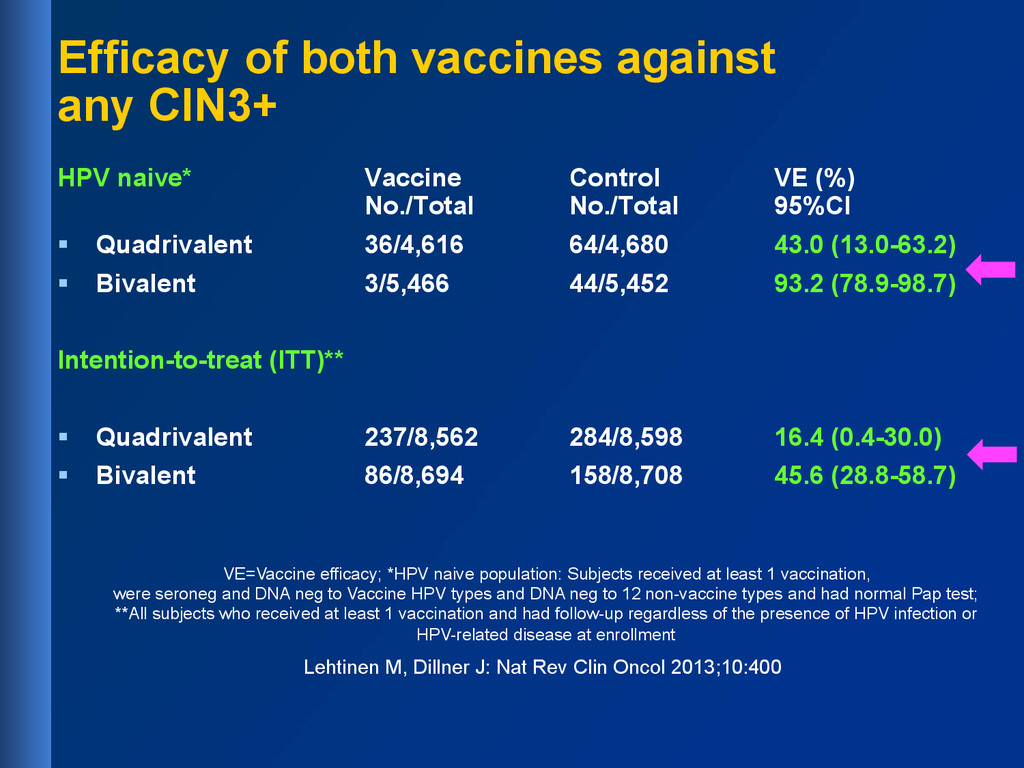
Control VE (%) No./Total No./Total 95%CI § Quadrivalent 36/4,616 64/4,680 43.0 (13.0-63.2) § Bivalent 3/5,466 44/5,452 93.2 (78.9-98.7) Intention-to-treat (ITT)** § Quadrivalent 237/8,562 284/8,598 16.4 (0.4-30.0) § Bivalent 86/8,694 158/8,708 45.6 (28.8-58.7) VE=Vaccine efficacy; *HPV naive population: Subjects received at least 1 vaccination, were seroneg and DNA neg to Vaccine HPV types and DNA neg to 12 non-vaccine types and had normal Pap test; **All subjects who received at least 1 vaccination and had follow-up regardless of the presence of HPV infection or HPV-related disease at enrollment Lehtinen M, Dillner J: Nat Rev Clin Oncol 2013;10:400
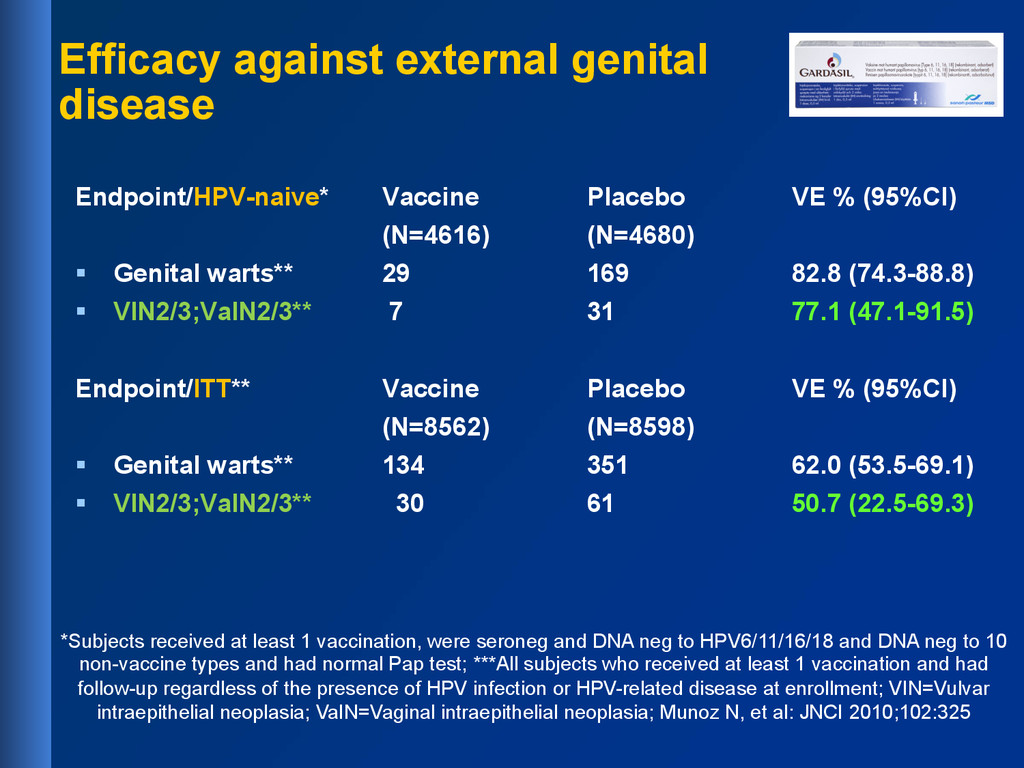
warts** 29 169 82.8 (74.3-88.8) § VIN2/3;VaIN2/3** 7 31 77.1 (47.1-91.5) Endpoint/ITT** Vaccine Placebo VE % (95%CI) (N=8562) (N=8598) § Genital warts** 134 351 62.0 (53.5-69.1) § VIN2/3;VaIN2/3** 30 61 50.7 (22.5-69.3) *Subjects received at least 1 vaccination, were seroneg and DNA neg to HPV6/11/16/18 and DNA neg to 10 non-vaccine types and had normal Pap test; ***All subjects who received at least 1 vaccination and had follow-up regardless of the presence of HPV infection or HPV-related disease at enrollment; VIN=Vulvar intraepithelial neoplasia; VaIN=Vaginal intraepithelial neoplasia; Munoz N, et al: JNCI 2010;102:325 Efficacy against external genital disease
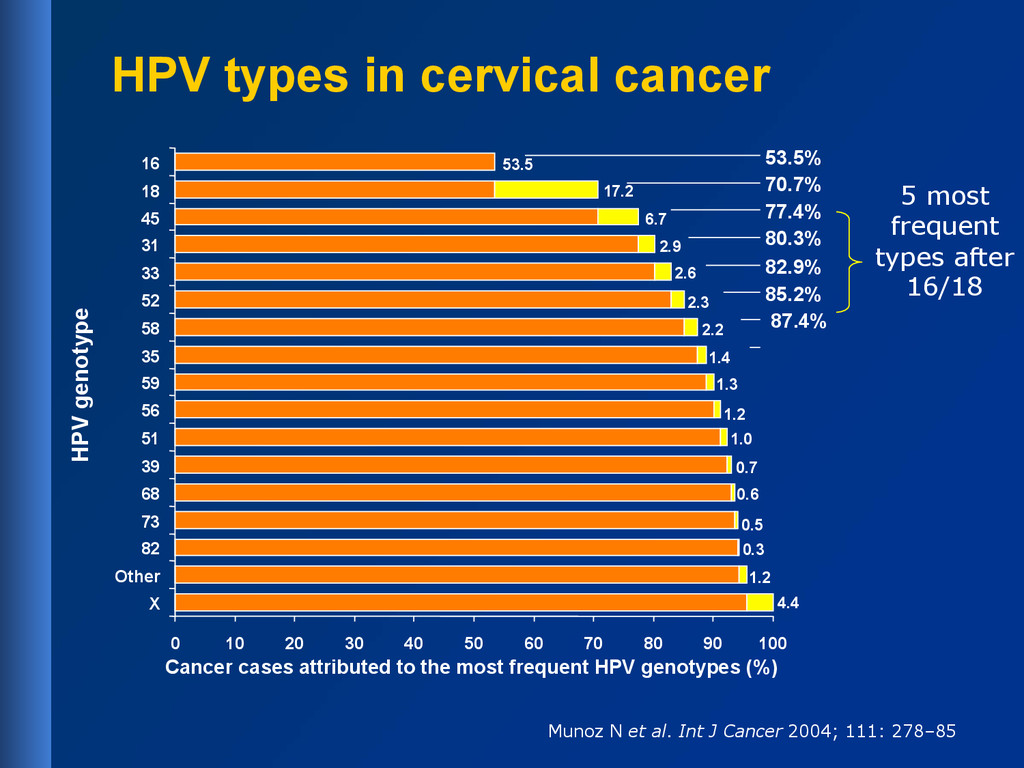
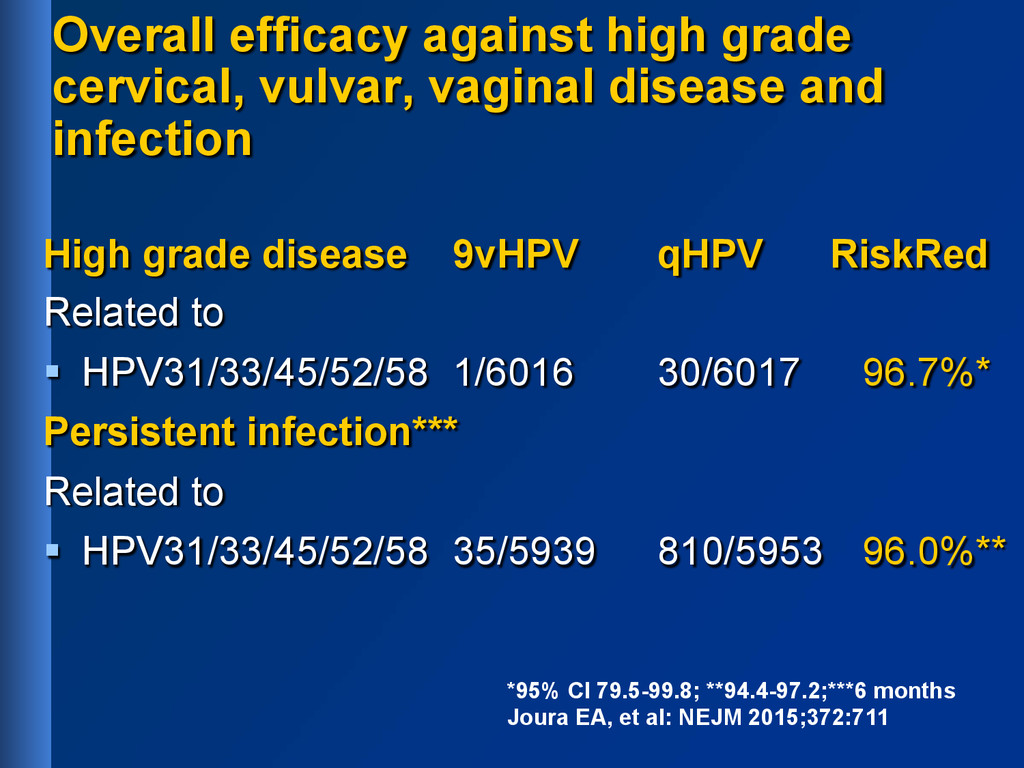
31, 33, 45, 52, 58 § Approximately 90% of cervical cancer cases worldwide could be prevented § FDA approval Dec 10, 2014 Joura EA, et al: Cancer Epidemiol Biomarkers Prev 2014;23:1997; Joura EA, et al: NEJM 2015;372:711
infection High grade disease 9vHPV qHPV RiskRed Related to § HPV31/33/45/52/58 1/6016 30/6017 96.7%* Persistent infection*** Related to § HPV31/33/45/52/58 35/5939 810/5953 96.0%** *95% CI 79.5-99.8; **94.4-97.2;***6 months Joura EA, et al: NEJM 2015;372:711
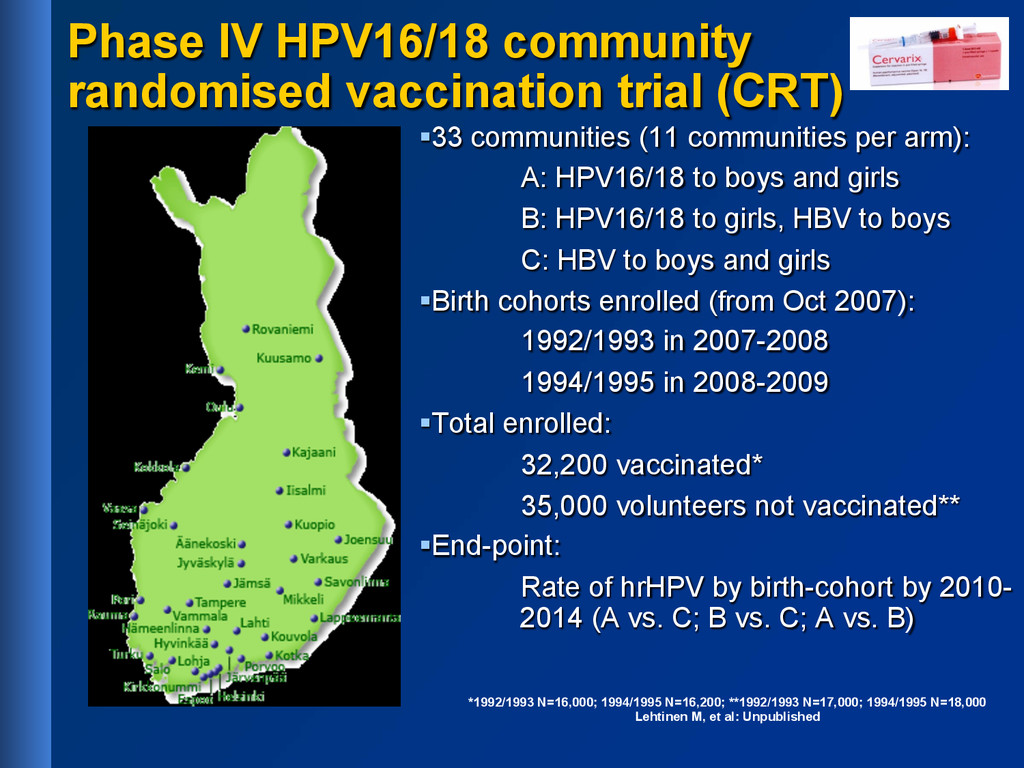
(11 communities per arm): A: HPV16/18 to boys and girls B: HPV16/18 to girls, HBV to boys C: HBV to boys and girls § Birth cohorts enrolled (from Oct 2007): 1992/1993 in 2007-2008 1994/1995 in 2008-2009 § Total enrolled: 32,200 vaccinated* 35,000 volunteers not vaccinated** § End-point: Rate of hrHPV by birth-cohort by 2010- 2014 (A vs. C; B vs. C; A vs. B) *1992/1993 N=16,000; 1994/1995 N=16,200; **1992/1993 N=17,000; 1994/1995 N=18,000 Lehtinen M, et al: Unpublished
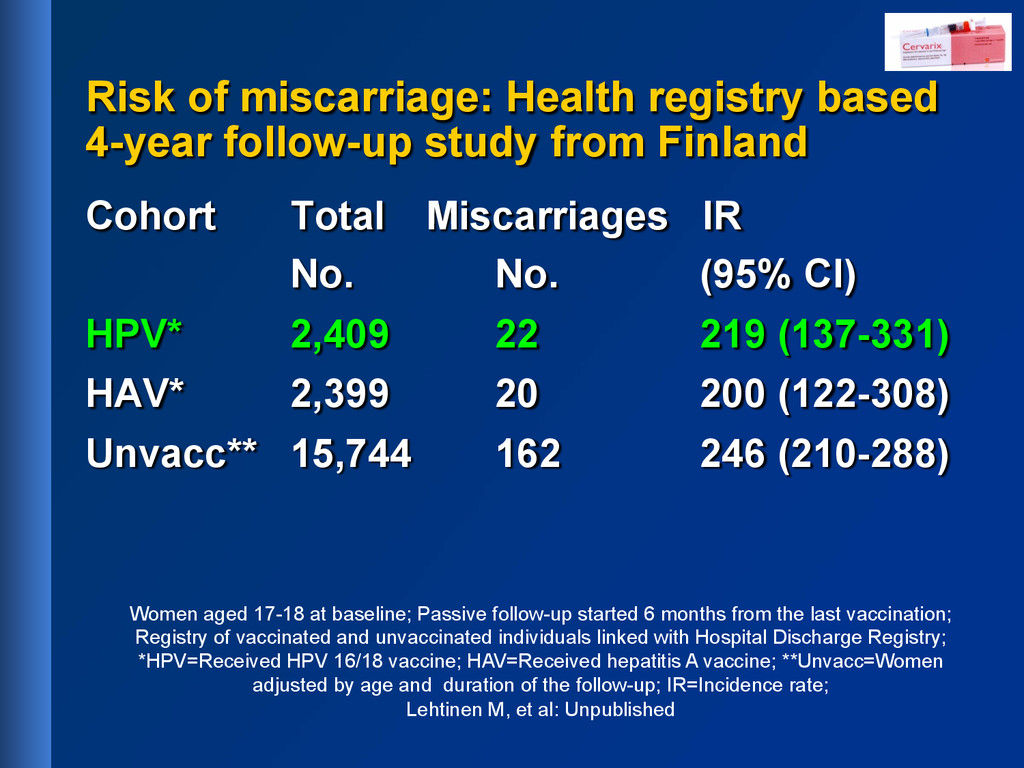
Finland Cohort Total Miscarriages IR No. No. (95% CI) HPV* 2,409 22 219 (137-331) HAV* 2,399 20 200 (122-308) Unvacc** 15,744 162 246 (210-288) Women aged 17-18 at baseline; Passive follow-up started 6 months from the last vaccination; Registry of vaccinated and unvaccinated individuals linked with Hospital Discharge Registry; *HPV=Received HPV 16/18 vaccine; HAV=Received hepatitis A vaccine; **Unvacc=Women adjusted by age and duration of the follow-up; IR=Incidence rate; Lehtinen M, et al: Unpublished
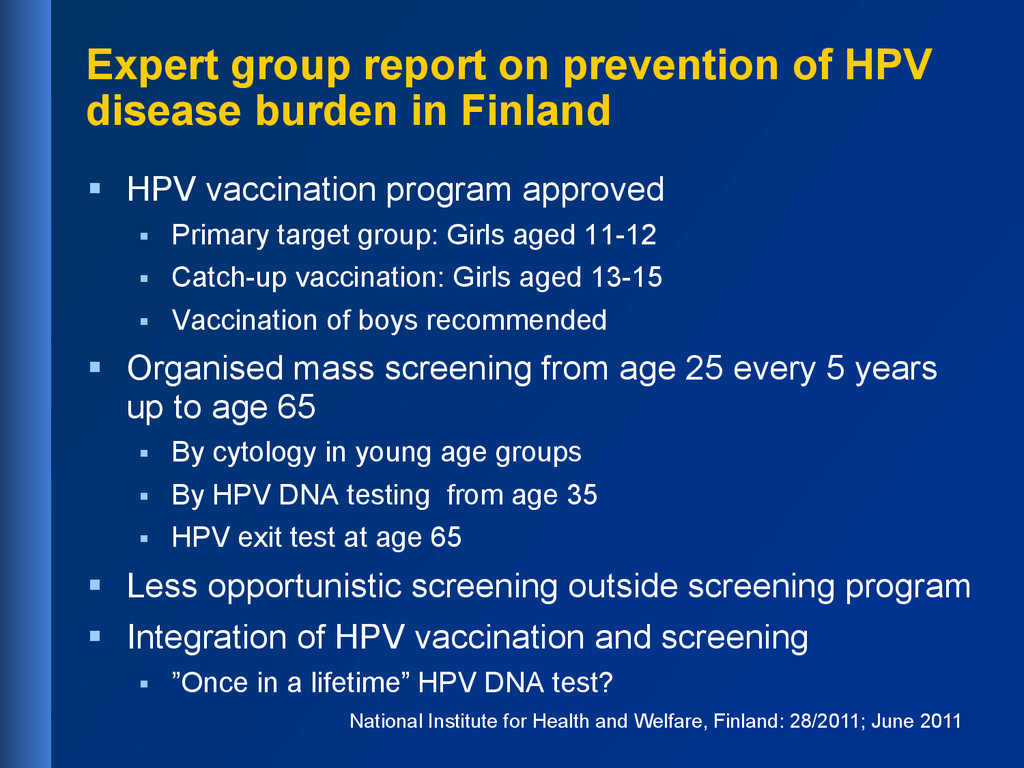
Finland § HPV vaccination program approved § Primary target group: Girls aged 11-12 § Catch-up vaccination: Girls aged 13-15 § Vaccination of boys recommended § Organised mass screening from age 25 every 5 years up to age 65 § By cytology in young age groups § By HPV DNA testing from age 35 § HPV exit test at age 65 § Less opportunistic screening outside screening program § Integration of HPV vaccination and screening § ”Once in a lifetime” HPV DNA test? National Institute for Health and Welfare, Finland: 28/2011; June 2011
screening and HPV vaccination are synergistic § Vaccine efficacy high in younger age groups § HPV screening effective in older age groups § HPV vaccination does not replace screening § Screening strategy will change
§ Eero Pukkala § Mika Gissler § Ahti Anttila § Xavier Bosch § Harald zur Hausen § Lutz Gissmann § Maija Jakobsson, Annika Riska, Anna-Maija Tapper, Päivi Pakarinen, Leena Laitinen § Gary Dubin, Frank Struyf, Jenny Andersson, Attila Mihalyi § Heather Sings § HPV vaccination trial Investigators ad Co- investigators Matti Lehtinen Eero Pukkala Mika Gissler Harald zur Hausen Lutz Gissmann Matti Lehtinen Pekka Nieminen
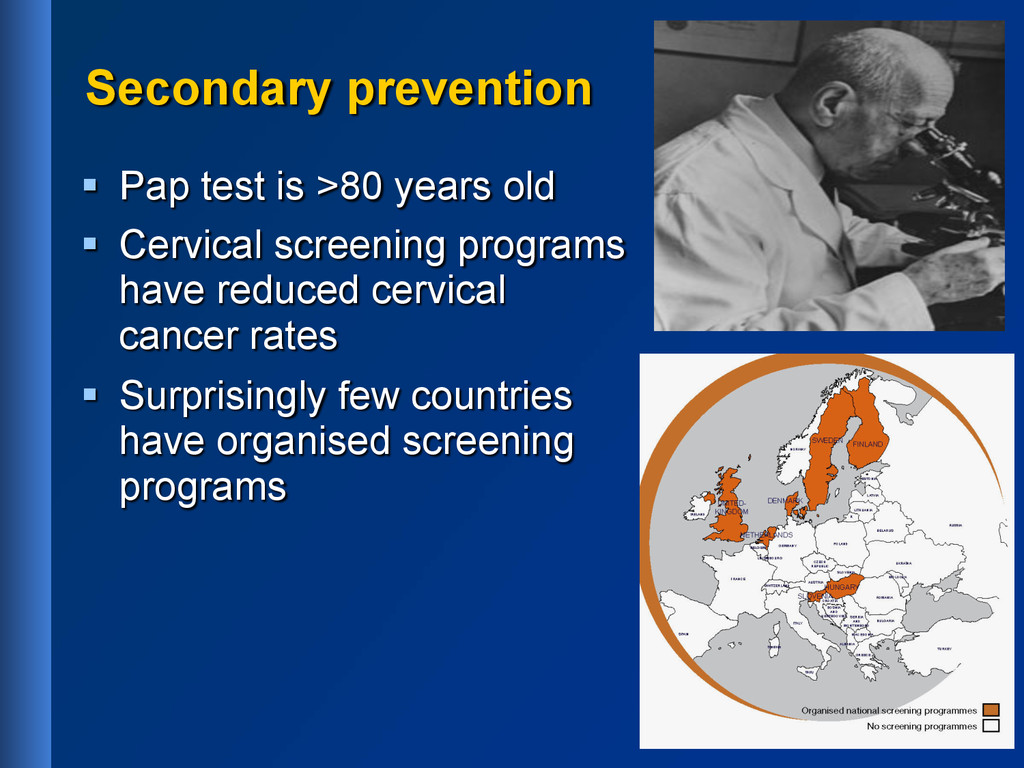
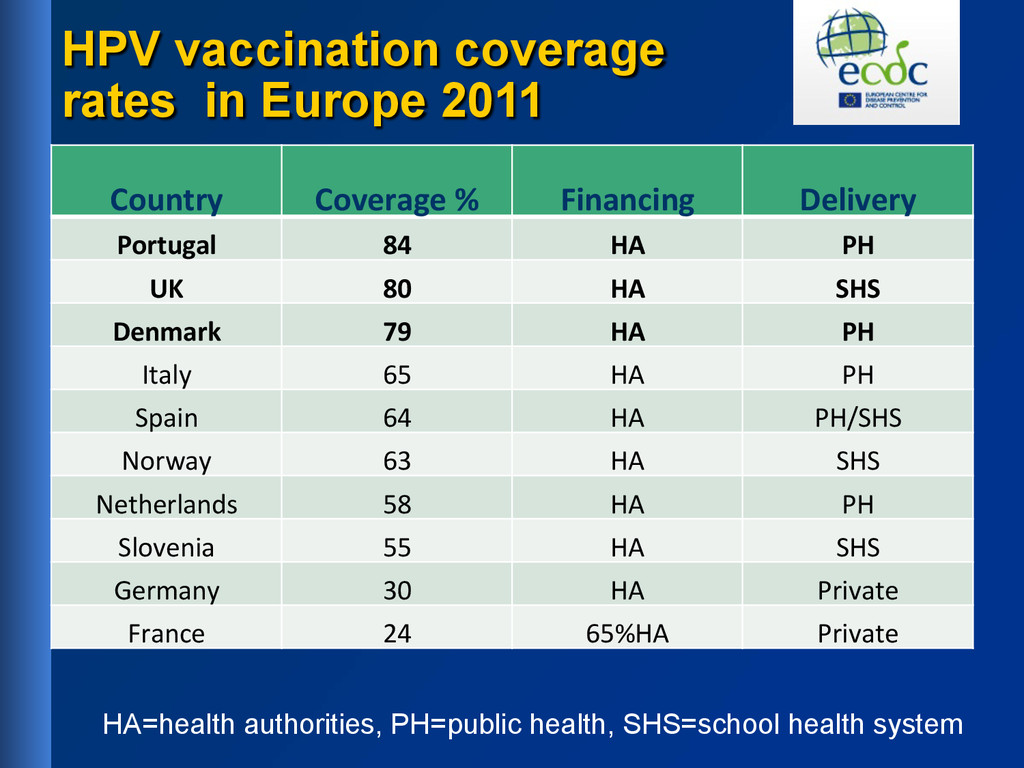
% Financing Delivery Portugal 84 HA PH UK 80 HA SHS Denmark 79 HA PH Italy 65 HA PH Spain 64 HA PH/SHS Norway 63 HA SHS Netherlands 58 HA PH Slovenia 55 HA SHS Germany 30 HA Private France 24 65%HA Private HA=health authorities, PH=public health, SHS=school health system
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}