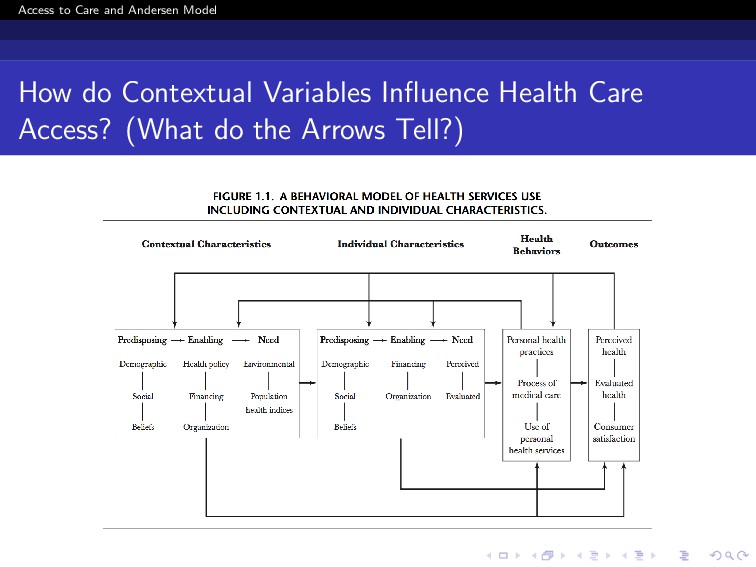
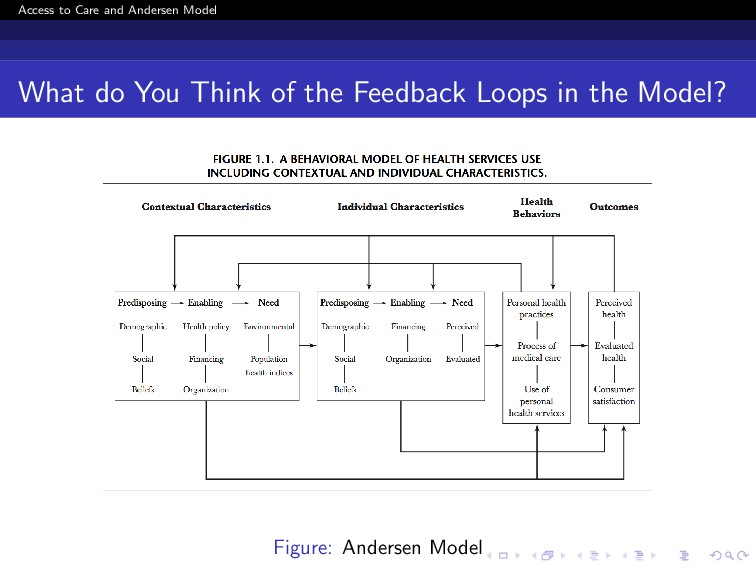
use of personal health services and Also, Everything that facilitates or impedes their use Link between health services systems and the populations they serve. Not Just visiting Health provider Getting Right services at the Right time to promote improved health outcomes
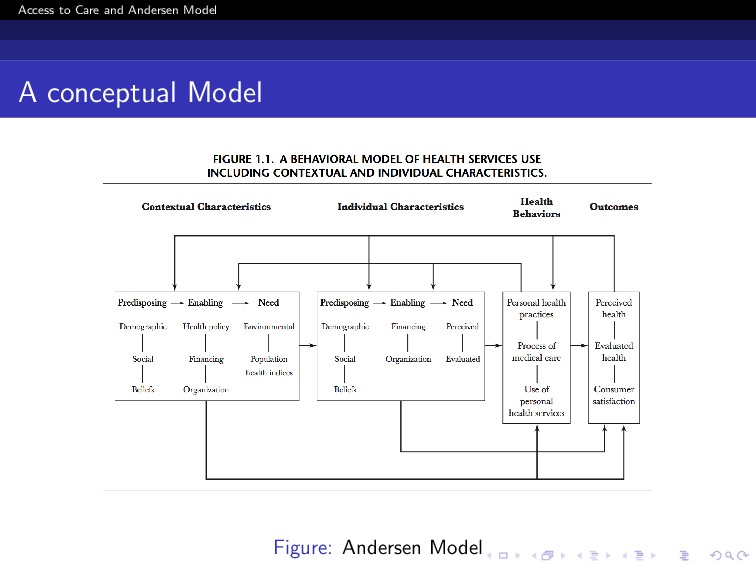
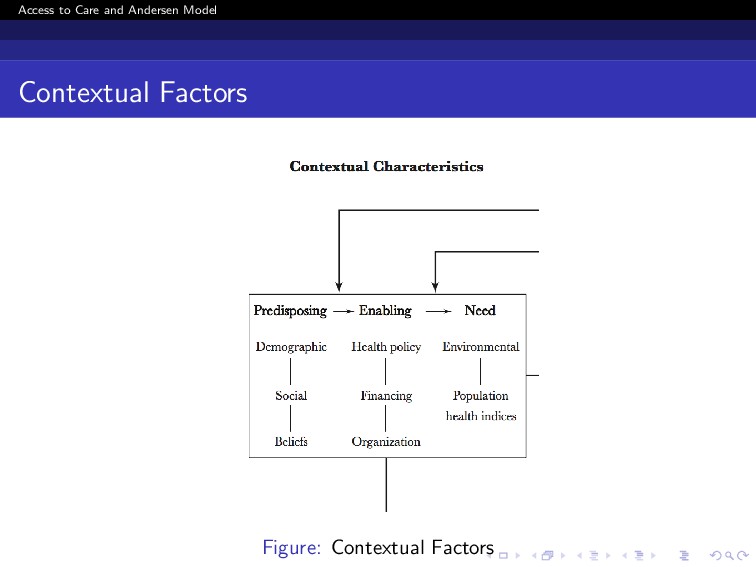
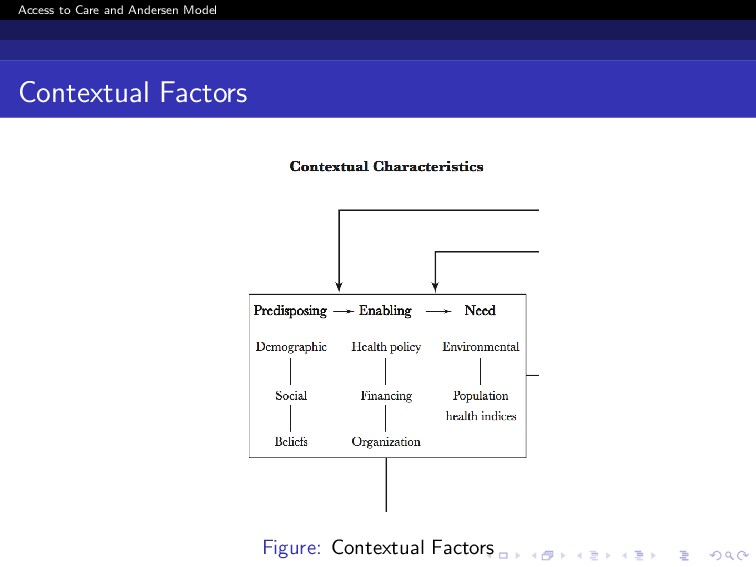
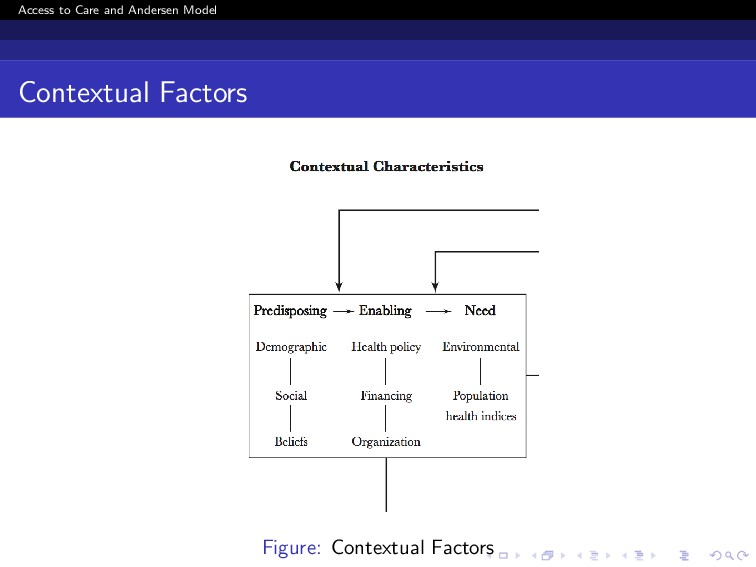
Major components of contextual characteristics are divided in the same way as individual characteristics Existing conditions that predispose are not directly responsible for use Enabling conditions make easy/difficult use of services Need == conditions that laypeople or health care providers recognize as requiring medical treatment Emphasizes contextual factors - importance of community, Structure and process of providing care Ultimate focus of the model remains on use of health services
gender, and marital status composition of a community) Question: How will a Society of Primarily older persons differ in utilisation from a society where majority are younger parents and children? Social characteristics (how supportive or unsupportive are the communities where people live and work) Question: How and Why might this affect health and access to health services? Relevant measures (educational level, ethnic composition, crime rate, employment) Underlying Values and Beliefs
are authoritative decisions Can be public policies made in the legislative/executive/or judicial branch of government (MoH/DHB) Can be Private Provider Based (GPs, Clinic Policies) All levels from local to national
Resources available to pay for health services Per capita community income and wealth (Deciles) Incentives to purchase or provide services Price of medical care and other goods and services, and method of compensating providers
and distribution of health services facilities and personnel Supply of services in the community Ratios of physicians and hospital beds to population Waiting Time Quality Control Outreach Services
need Health-related measures of the physical environment Housing, Water, Air, Others?? Injury and Death Rates (Motor Vehicle Accidents, Farming Accidents) Population Health Indices (infant mortality, birth rates, prevalence, disease-specific mortality)
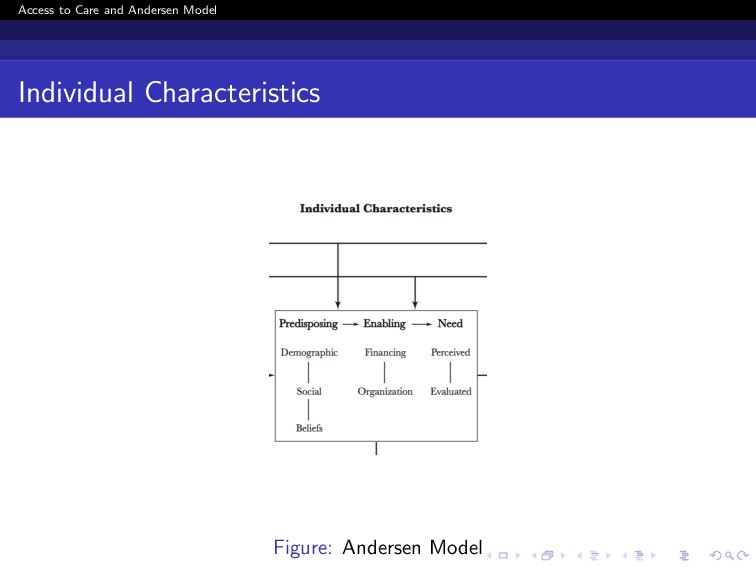
(Age, Gender, Other Biological imperatives) Social factors (education, occupation, immigration, and ethnicity) Health beliefs (attitudes, values, and knowledge)
and wealth Effective price of health care to the patient Think: Regular Care, Care of Children, and Dental Care Whether or not the individual has a regular source of care What kind of Care (private doctor, community clinic, emergency room) Transportation, waiting time for care
people view their own general health and functional state How they experience and emotionally respond to signs and symptoms Discuss: To What Extent These Determine People‘s Access?
Nurses judgment Objective measurement about a patients physical status and need for medical care Biological Perspective and Others Professional Expertise Also social and professional (How??)
Key Difference between Perceived and Evaluated Need? What do You think? Perceived Need = Care Seeking Process, Adherence, Compliance Evaluated Need = Actual Treatment Received and Outcomes
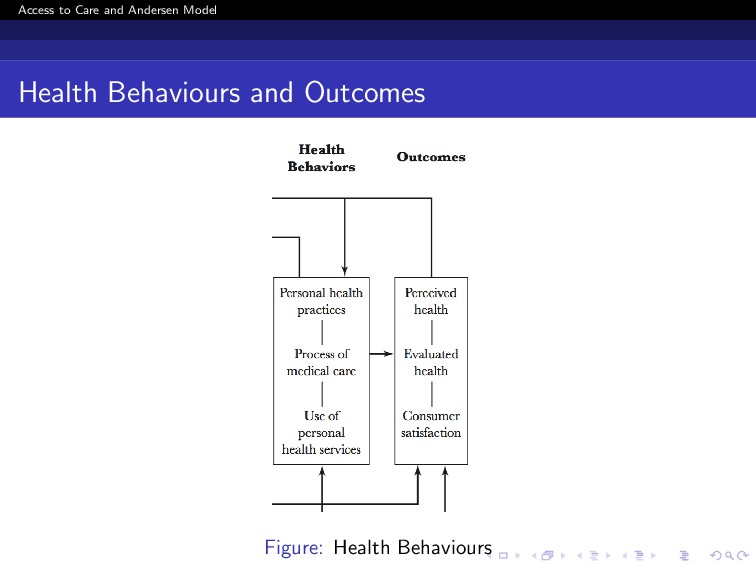
Individual Health behaviours that influence health status (diet, exercise, smoking, addiction, self-care) Behaviour of health providers interacting with patients (patient counselling, test ordering, prescribing patterns, and quality of provider-patient communication) Are the Physicians/Nurses doing their bit? (Where Evidence Based Health and Guidelines Come into play)
Kind of Service Utilisation? What kind of service utilisation do you think will be explained by Need and Demographic Factors? What kind of service utilisation do you think will be explained by Social and Enabling Factors? What Factors Do You Think will explain Ambulatory Care Seeking or OPD attendance?
Perceived health status. Indicates extent to which a person can live a functional, comfortable, and pain-free life Measures include reports of general perceived health status, activities of daily living
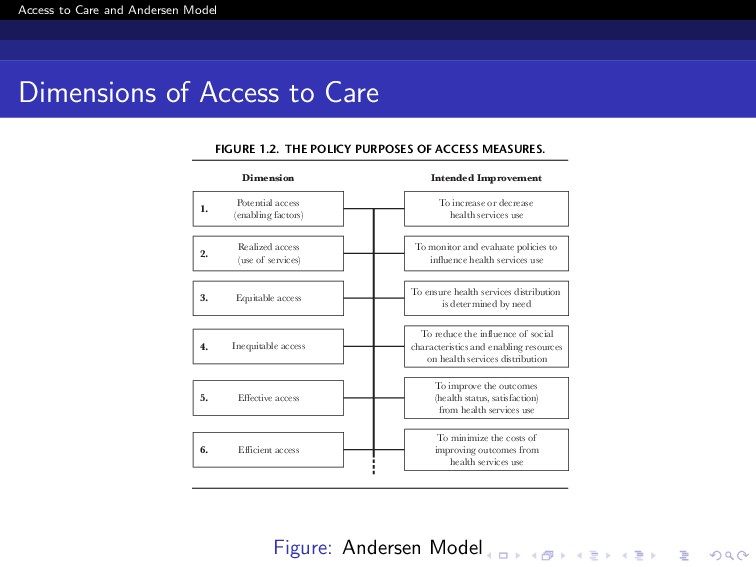
Care tion shifted in the 1970s to concern for health care cost containment and creation of mechanisms to limit access to health care. Examples of policies designed to limit access are coinsurance, deductibles, utilization review, and the genesis of managed Improving Access to Care in America 11 Dimension Intended Improvement To minimize the costs of improving outcomes from health services use Efficient access 6. To improve the outcomes (health status, satisfaction) from health services use Effective access 5. To reduce the influence of social characteristics and enabling resources on health services distribution Inequitable access 4. Equitable access To ensure health services distribution is determined by need 3. Realized access (use of services) To monitor and evaluate policies to influence health services use 2. Potential access (enabling factors) To increase or decrease health services use 1. FIGURE 1.2. THE POLICY PURPOSES OF ACCESS MEASURES. Andersen.c01 12/5/06 2:33 PM Page 11 Figure: Andersen Model
Access is defined according to which determinants of realized access are dominant in predicting utilization. Equitable access occurs when demographic variables (age and gender), and need variables account for utilisation Inequitable Access occurs when social characteristics and enabling resources such as ethnicity or income determine who gets medical care.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}