of the greatest ‘disease’ of our times- significant morbidity and mortality A significant workload in the ED (even greater in MTC) Basic measures instituted to ensure good outcome TEAM approach is paramount Central to all critical care specialties Early recognition of physiological parameters
documentation Failure to recognise injuries – importance of primary and secondary survey (if possible) Senior help not sought early Team Leader(coordinates the various personnel) - its absence Failure to gain overall control/insight Survival intrinsically linked to good basic initial management Getting vital information early- use AMPLE (Age, Mechanism, Past medical history, Last meal, Events around)
tourniquet A- all trauma patient HFO initially +C-spine immobilisation (triple immobilisation) (paediatric cases different) B- assess ventilation and oxygenation C- Establish- 2 large bore IV cannulae, EZ -IO if needed, Crossmatch , Baseline bloods, Analgesia, use of E-FAST if available D- GCS, Pupil response E- very important initially, beware of inducing hypothermia Early imaging once patient stable If unstable- damage control intervention
Pain- increases metabolic demands (oxygen requirements) Modified WHO ladder Consider IV analgesia early IV paracetamol as an adjunct with IV opiates (especially limb injuries) Effective pain management- leads to better outcome Consider nerve blocks (if applicable)
TXA (Tranexamic acid) early If bleeding- then give blood- Replace blood with blood Volume replacement- crystalloid – preferably Hartmann’s Consider pelvic binder Splint large bone fractures- reduces bleeding and pain Monitor U/O- Catheterise(urethral) unless evidence of urethral injury (retrograde urethrogram)
chances of hypothermia Concerns about subluxation of C-spine Larger occiput to body ratio- inadvertent C-spine hyper-extension Uncuffed tubes (reduce tracheal stenosis, strictures) Compensates well initially before haemodynamic collapse Plasticity of bone (if #- high impact trauma/ injury to deeper structures) Prepare team well early intervention of paediatricians
heavy machinery had crush injury to thorax Fit and Well- No PMHx/SurgHx No regular medications A- Patent, No C-spine injury B- Tachypneoic (RR-20/min), auscultation- vesicular breath sounds C- HR- 120, BP- 80/65 D- Alert, c/o pain in chest E- Some bruising to the chest, no other identified injuries present
chest wall trauma Associated with sternal fractures Non-specific ECG changes If ECG- Normal, Cardiac enzymes- Normal Can safely rule out diagnosis If suspected then needs Echo/ Myocardial perfusion scan Acutely needs cardiothoracic input Early ionotropic support following adequate fluid resusctiation
injury Fallen from a height of 20 feet Previously fit and well No PMHx/Surg Hx/No regular medications SAS- Extensive bruising in the right parietal region of scalp, no occult bleeding present, Open fracture of the left Tibia/fibula Trauma team – I+V Family on route
no issues B- On ventilator, 12/min C- BP- 200/160 HR- 55 D- Prior to I+V, GCS 5/15, was becoming combative, Pupil reactive but sluggish, Right pupil 4, Left pupil 5 E- Left lower limb in a temporary splint BM- 8, T- 36.5 Any immediate measures Management?
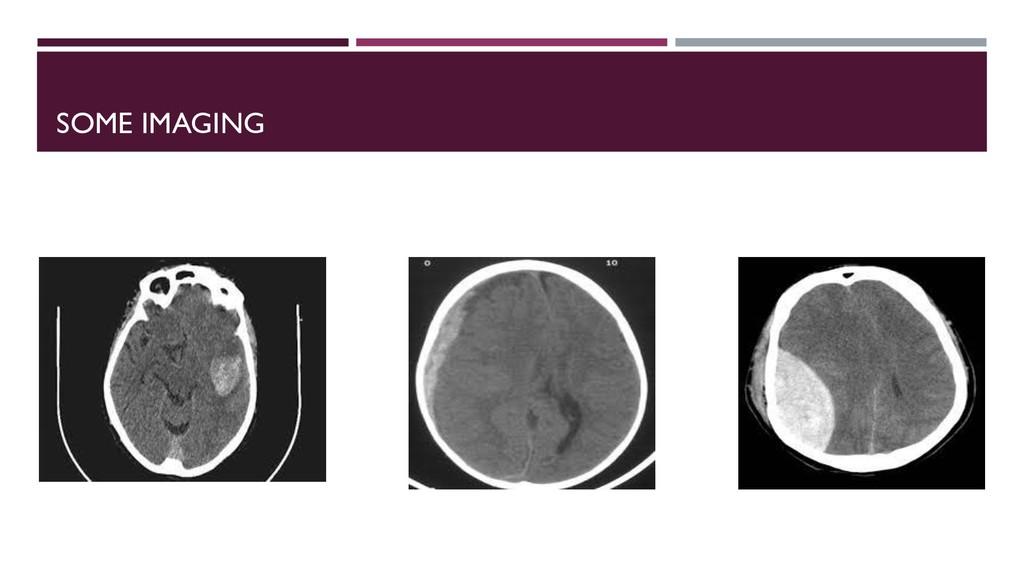
CSF and blood If any of the above volume rises then Brain has less space- will go through area of least resistance CPP = MAP-ICP CPP- Cerebral Perfusion Pressure MAP- Mean Arterial Pressure ICP- Intracranial Pressure SBP- Systolic Blood Pressure DBP- Diastolic Blood Pressure MAP= DBP+ 1/3(SBP-DBP) Cardiac output= Heart Rate x Stroke Volume CO = HR x SV Aim- Prevent Secondary Brain Injury
degree of suspicion of additional injuries- undertake trauma imaging Early normalisation of physiological markers Ask for help early Review and reassess Leadership in trauma management
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}