when she started having pain abdomen, continuous in nature, severe in intensity, radiating to back and thighs. No aggravating and relieving factors. Started having excessive P/V bleeding (No Clots) since morning soaking 4pads, associated with pain abdomen.
• No significant Surgical/Medical history. • No History of Blood transfusion. FAMILY HISTORY • No H/O similar complaints. PERSONAL HISTORY • Mixed diet. • Sleep and appetite normal. • Bladder/Bowel normal and regular.
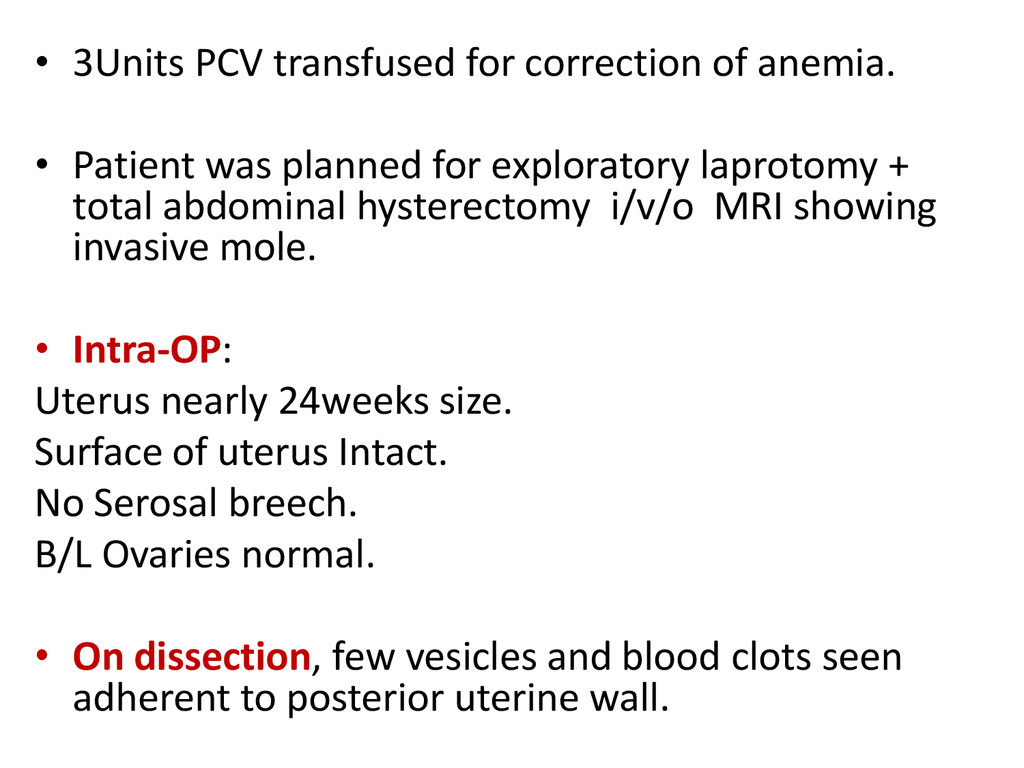
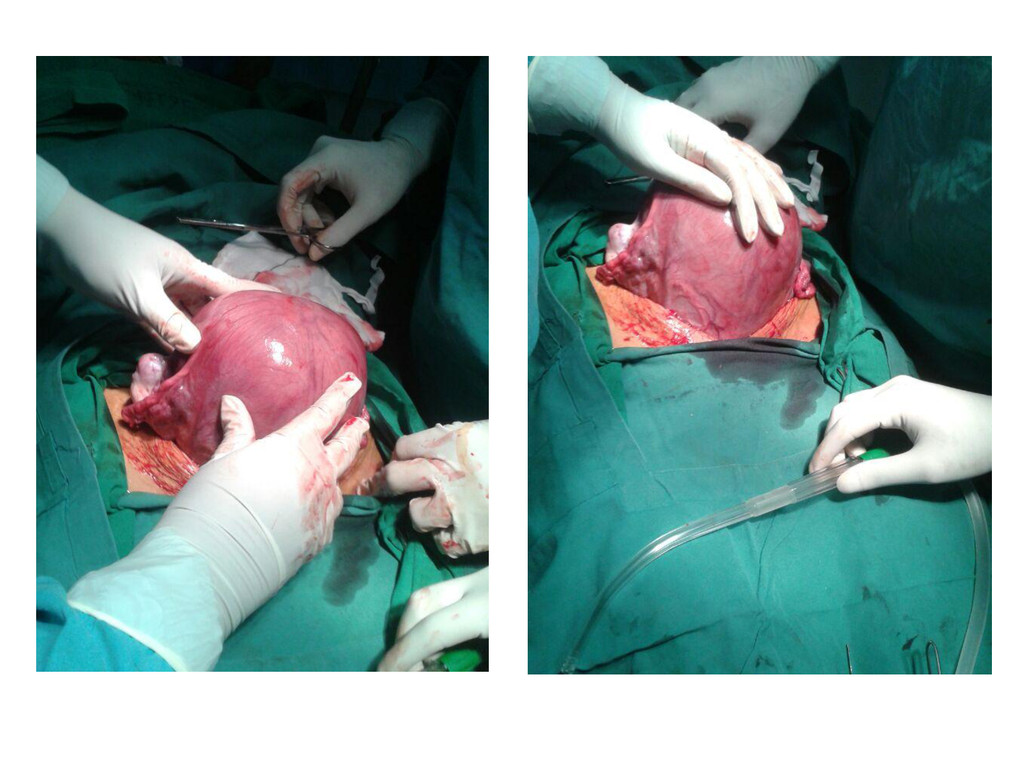
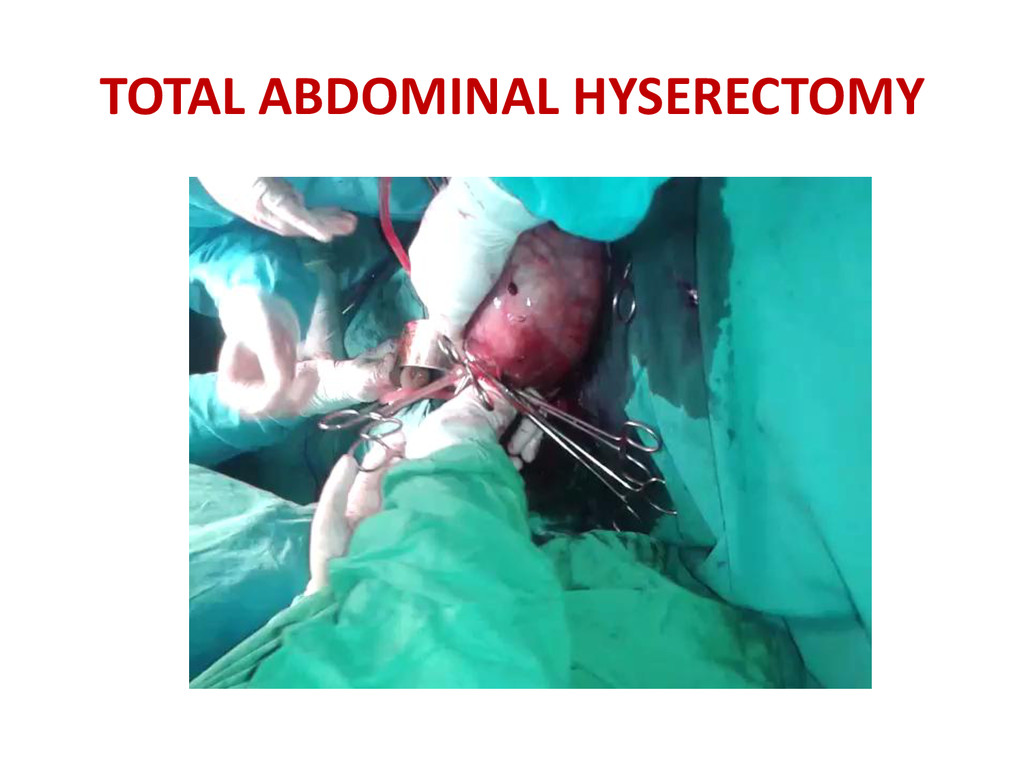
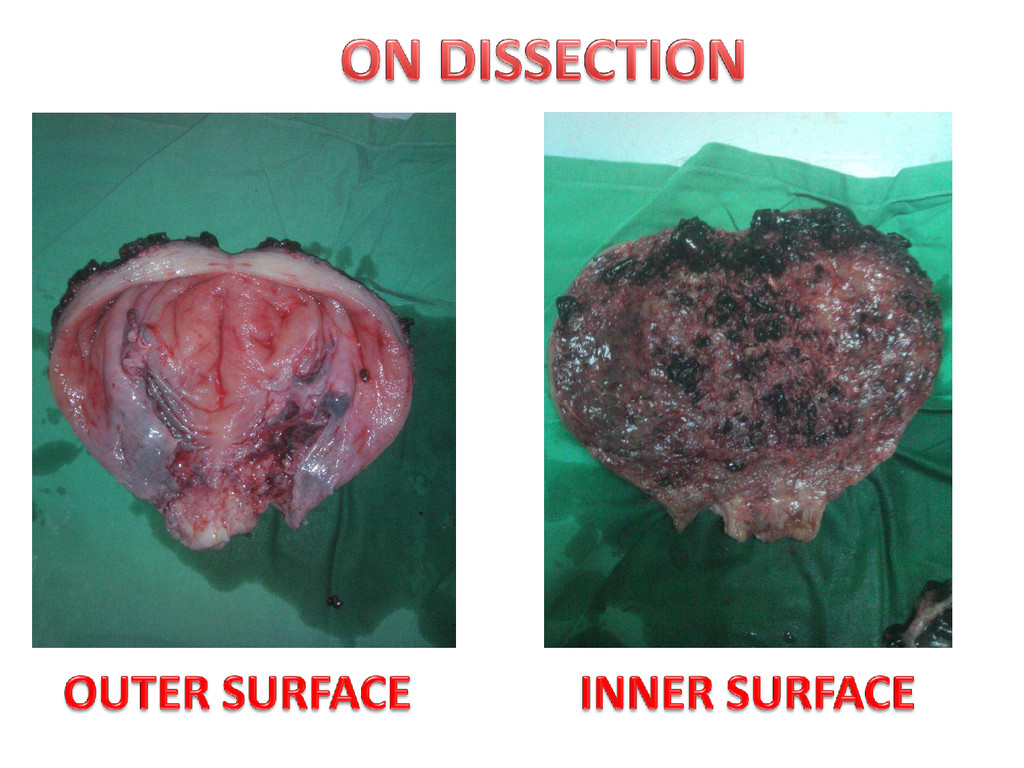
was planned for exploratory laprotomy + total abdominal hysterectomy i/v/o MRI showing invasive mole. • Intra-OP: Uterus nearly 24weeks size. Surface of uterus Intact. No Serosal breech. B/L Ovaries normal. • On dissection, few vesicles and blood clots seen adherent to posterior uterine wall.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
![DR ASMA KHAN[ RESIDENT] DR GOWRI SAI PRASAD[ASSOCIATE PROFFESOR] DR](https://files.speakerdeck.com/presentations/f7903040ecb901318ac32a5458301a54/slide_20.jpg){kind=link}