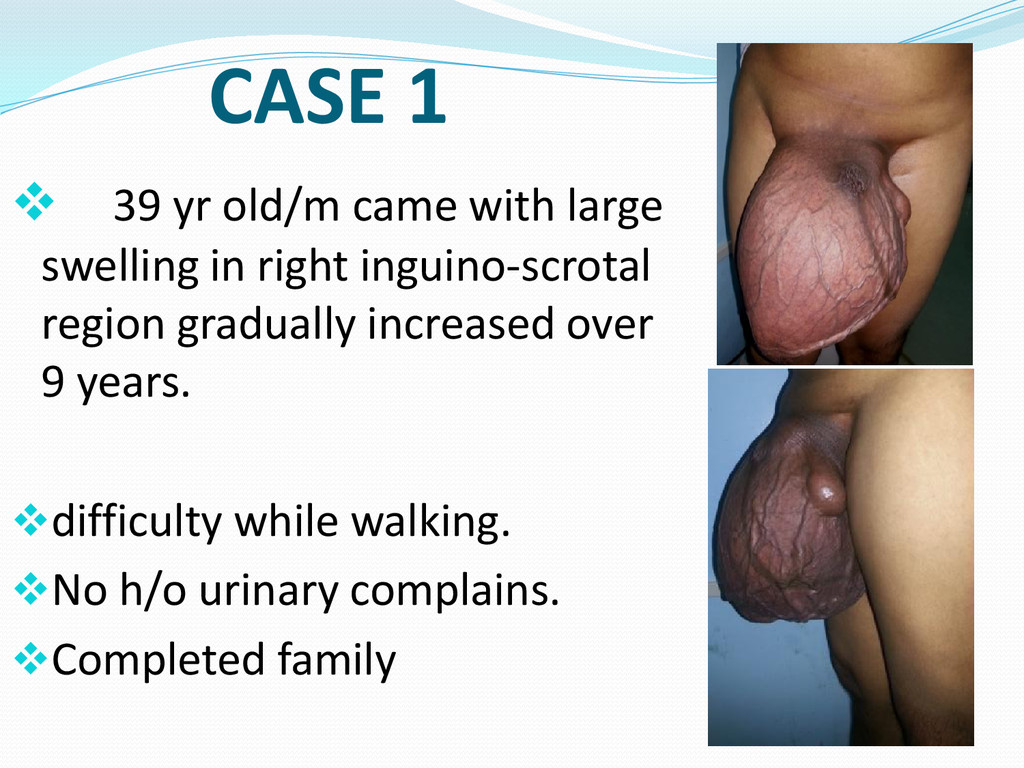
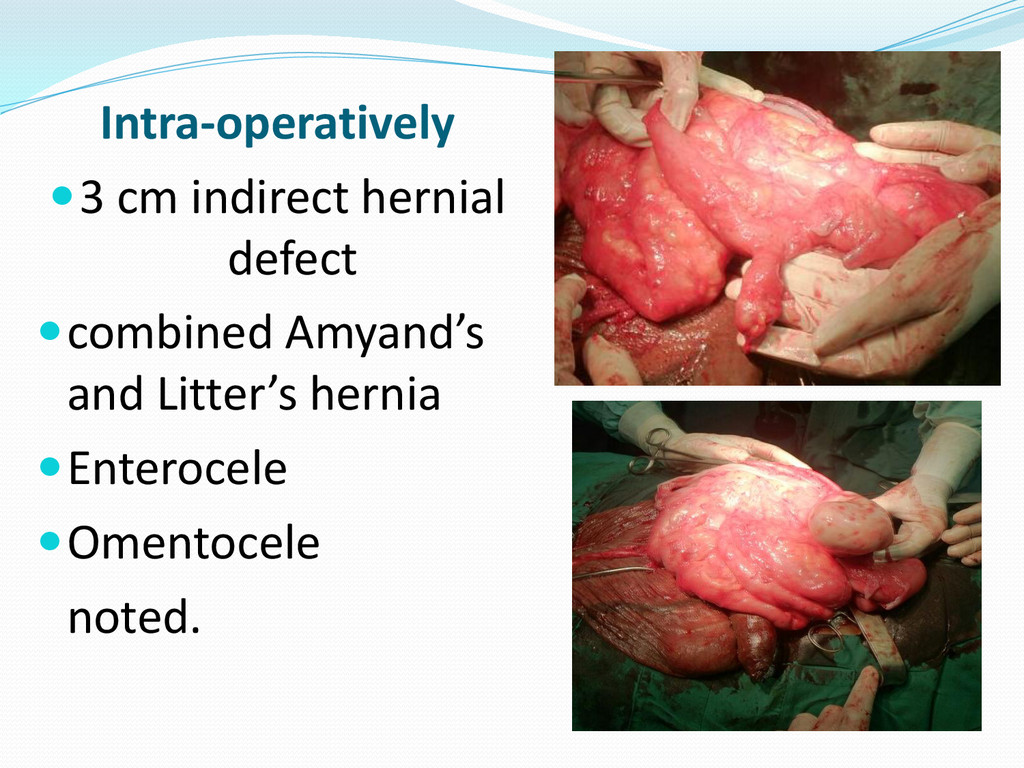
right inguinal region up to the knees with buried penis, dilated veins - soft, non reducible, non tender swelling, testis palpable at base, - peristalis at ascultation - suggesting enterocele and omentocele.
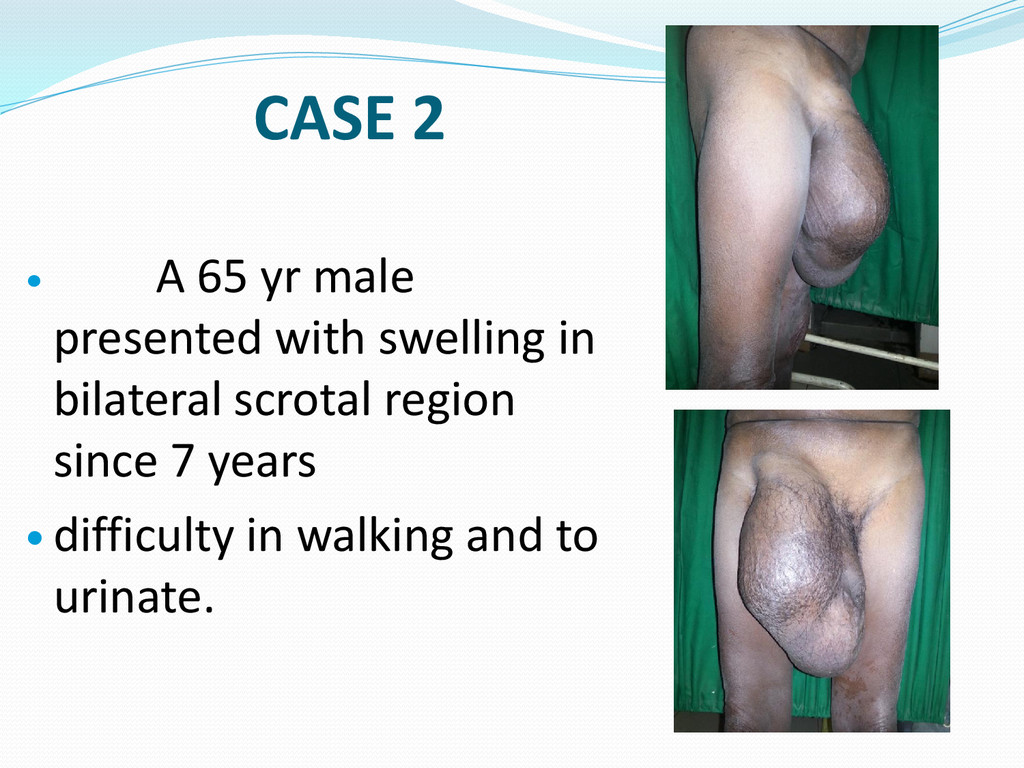
25X18X17cm from right inguino- scrotal region beyond mid thigh, partially reducible suggestive of enterocele and omentocele. Lt. scrotal region: swelling of size 12X10X10cm, cystic, fluctuant with transillumination.
repair of a giant inguinoscrotal hernia; Int J Surg Case Rep. 2011; 2(3): 32–35; PMCID: PMC3199728 2. E Tay, E Gray and M W Morgan; Repair of a massive inguinal hernia; J R Soc Med. 1999 November; 92(11): 586– 587. PMCID: PMC1297438 3. Mohammad Tahir, Faiz U. Ahmed, V. Seenu; Giant inguinoscrotal hernia: Case report and management principles; International Journal of Surgery Volume 6, Issue 6, December 2008, Pages 495–497.
hernias that extend below the midpoint of the inner thigh in the standing position. They present a new spectrum of problems for patients apart from the classical complications of inguinoscrotal hernia. Patients encounter difficulties in walking, sitting or simply lying down, and their mobility is dramatically restricted. Often develop gangrene and ulcers of the scrotal skin. May present with acute retention of urine due to voiding difficulties as the scrotum tightens around the penis. Also develop fatal tissue expansion of vascular pedicles.
repair is the necessity to avoid complications and morbidity of patient. Adequate pre-operative planning as well as intra-operative and postoperative monitoring is essential. Patient’s awareness towards this treatable condition and early diagnosis forms a vital aspect for the management of giant hernias. Thank You !!
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}