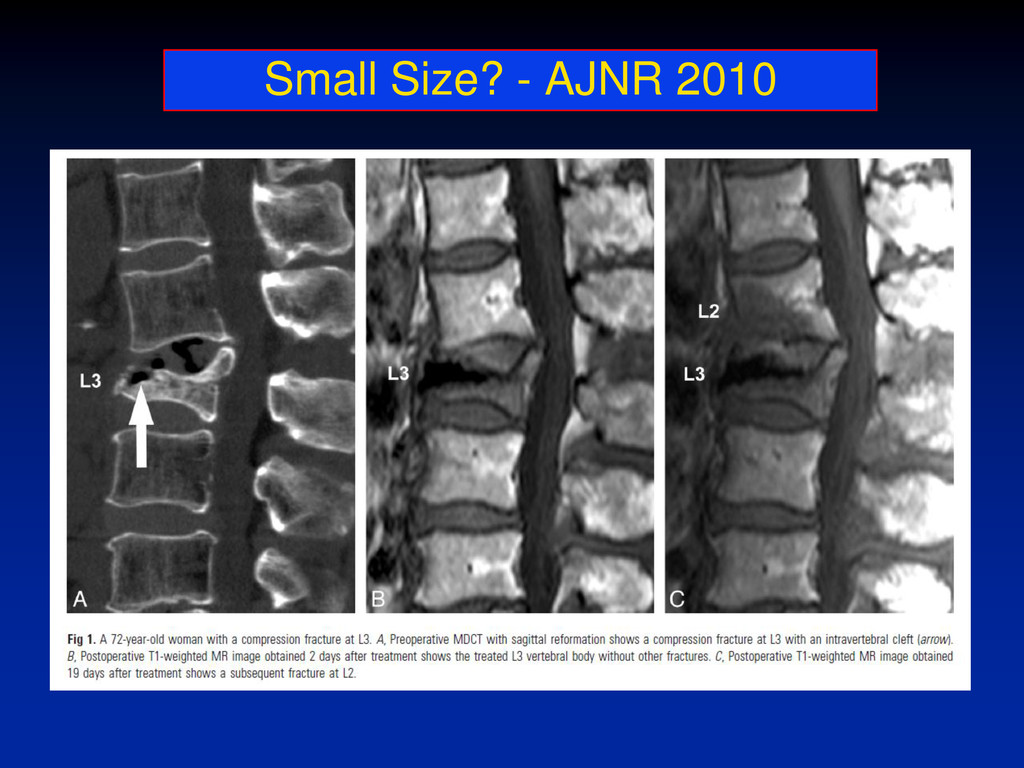
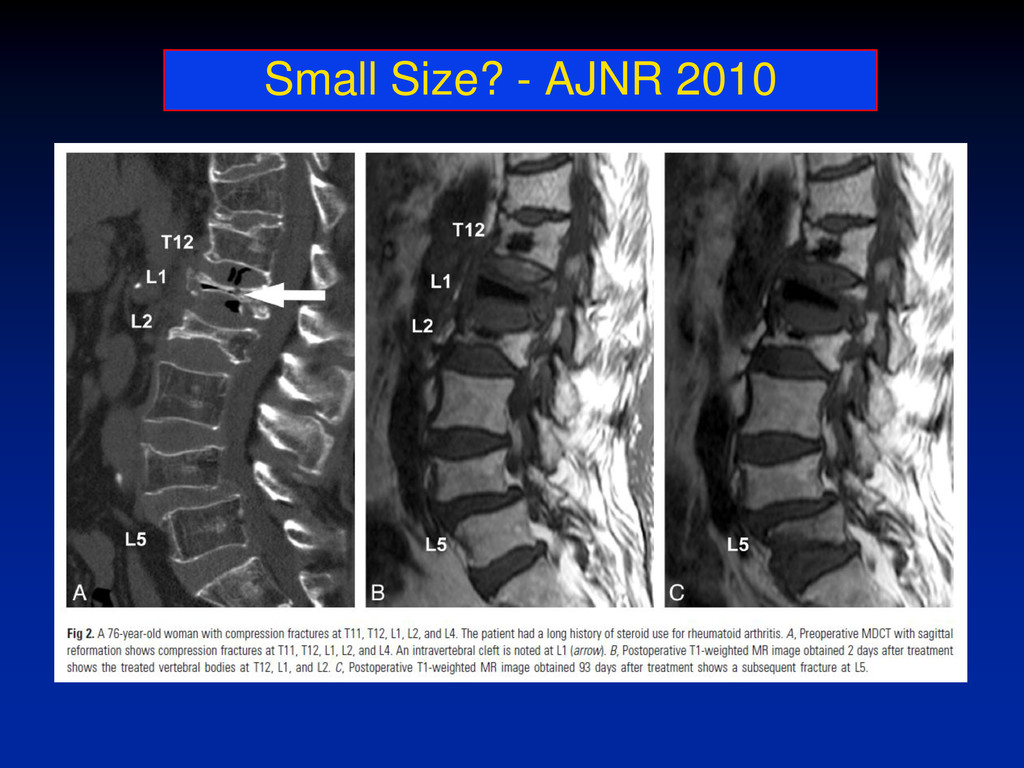
is the necessity of recent MRI for proper patient selection • We require evidence of marrow oedema on MRI before performing vertebroplasty • MRI also shows the actual number of recent fractures and detects fractures with no sign of vertebral collapse on initial radiographs but marrow oedema on MRI CVIR 2010
performed to confirm fracture activity and the number of vertebral bodies involved • Without a recent MRI or bone scan, one cannot confirm that the cause of pain was vertebral compression fracture
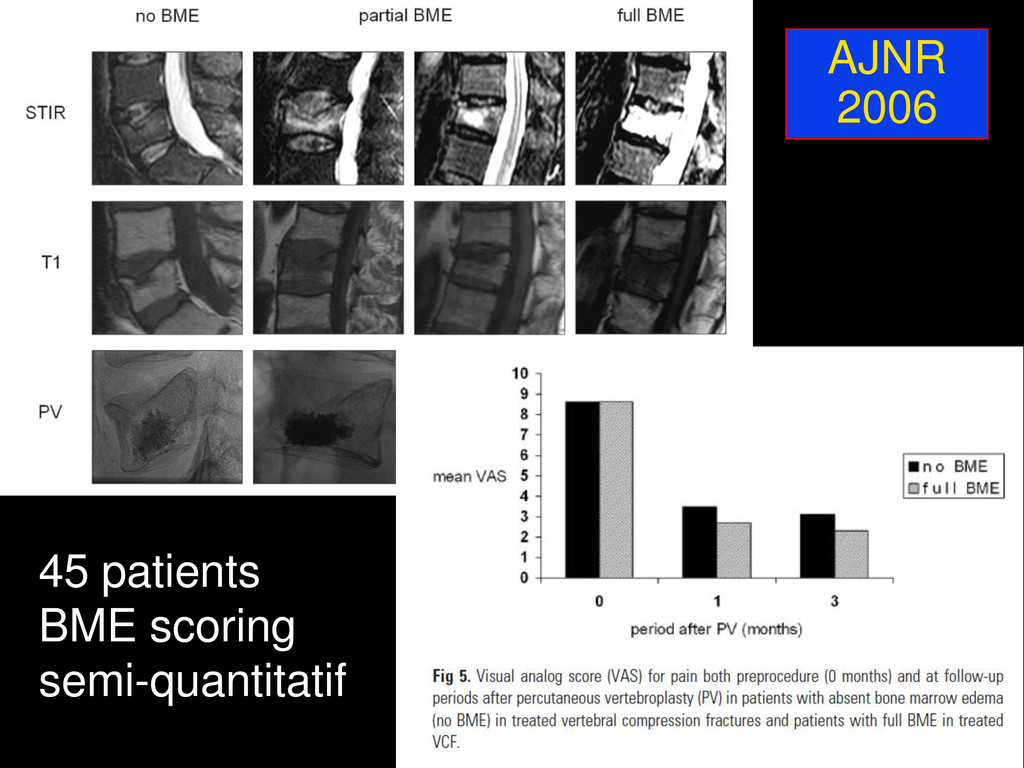
a 1, 1.5 or 3 Tesla MRI scanner • Bone edema in the VCF is defined as increased signal intensity at the STIR images and decreased signal intensity at the T1 weighted images • The shape and grade of every VCF is scored by two radiologists using the visual semiquantitative system according to Genant
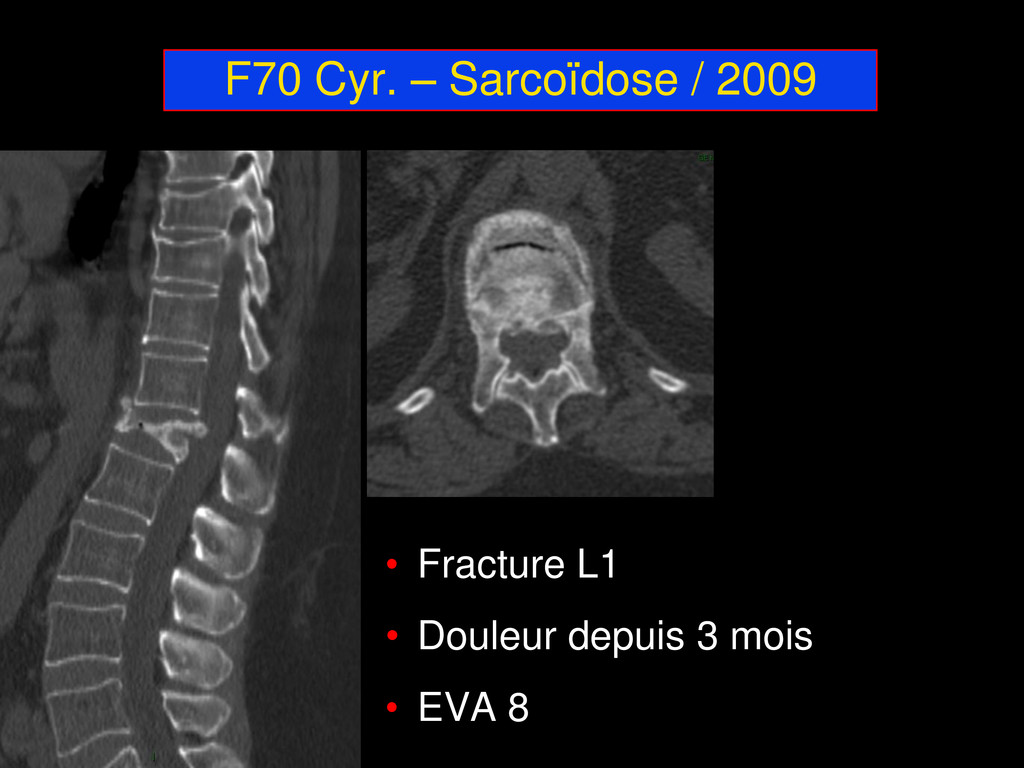
d’inclusion • Meilleure efficacité clinique de la VP si œdème étendu • Mais plusieurs séries concordantes avec efficacité VP malgré œdème absent • Fractures récentes vs anciennes?
treated with PV: Diagnostic Assessment and Clinical Significance SPINE 2011 Nieuwenhuijse, M.J. MD; van Rijswijk, C.S.P. MD, PhD; van Erkel, A.R. MD, PhD; Dijkstra, P.D.S. MD, PhD • Summary of Background Data. Patients with painful OVCFs with intravertebral clefts provide a unique and possibly superior indication for PVP. However, comparative studies are scarce and their results are conflicting. The extent of this difference attributable to interobserver variation in the identification of an intravertebral cleft is currently unknown. • Methods. 102 patients received PVP for 197 painful long- standing OVCFs and were prospectively followed using a pain-intensity numerical-rating scale for back pain, the SF-36 quality of life questionnaire and routine spinal radiographs. Three experienced examiners retrospectively examined all preoperative radiographs and MRI T1-weighted and STIR sequences and the direct postoperative CT-scans for the presence of an intravertebral cleft. Disagreements were re-examined and discussed for consensus.
cleft was moderate on preoperative radiography (kappa:0.55-0.59) and substantial on preoperative MR-imaging (kappa:0.71-0.79) and postoperative CT-scanning (kappa:0.67-0.85). • Based on consensus, 42 (21.3%) clefts were detected. The associated sensitivity of preoperative radiography was low (31.7-48.8%), but the specificity was high (94.7-99.3%). The diagnostic performance of preoperative MRI T1-weighted and STIR sequences was excellent, with both high sensitivity (85.7- 88.1%) and high specificity (89.7-98.1%). Pain decrease and increase in quality of life obtained from PVP was ultimately comparable to patients without intravertebral clefts, but was obtained more gradually over the first postoperative year. An intravertebral cleft was a strong risk factor for the occurrence of cortical cement leakage (OR: 4.29, 95%CI: 1.51-12.2, p = 0.006). The Intravertebral Cleft in Painful Long-standing Osteoporotic Vertebral Compression Fractures treated with PV: Diagnostic Assessment and Clinical Significance SPINE 2011 Nieuwenhuijse, M.J. MD; van Rijswijk, C.S.P. MD, PhD; van Erkel, A.R. MD, PhD; Dijkstra, P.D.S. MD, PhD
of an intravertebral cleft and the identification of an intravertebral cleft is not always straightforward • For preoperative assessment, we recommend MRI with T1-weighted and STIR sequences • Regarding patient-reported outcome, patients with long-standing OVCFs with intravertebral clefts benefit from PVP, but, compared to patients with OVCFs without intravertebral clefts, the benefit obtained was not superior and may be delayed The Intravertebral Cleft in Painful Long-standing Osteoporotic Vertebral Compression Fractures treated with PV: Diagnostic Assessment and Clinical Significance SPINE 2011 Nieuwenhuijse, M.J. MD; van Rijswijk, C.S.P. MD, PhD; van Erkel, A.R. MD, PhD; Dijkstra, P.D.S. MD, PhD
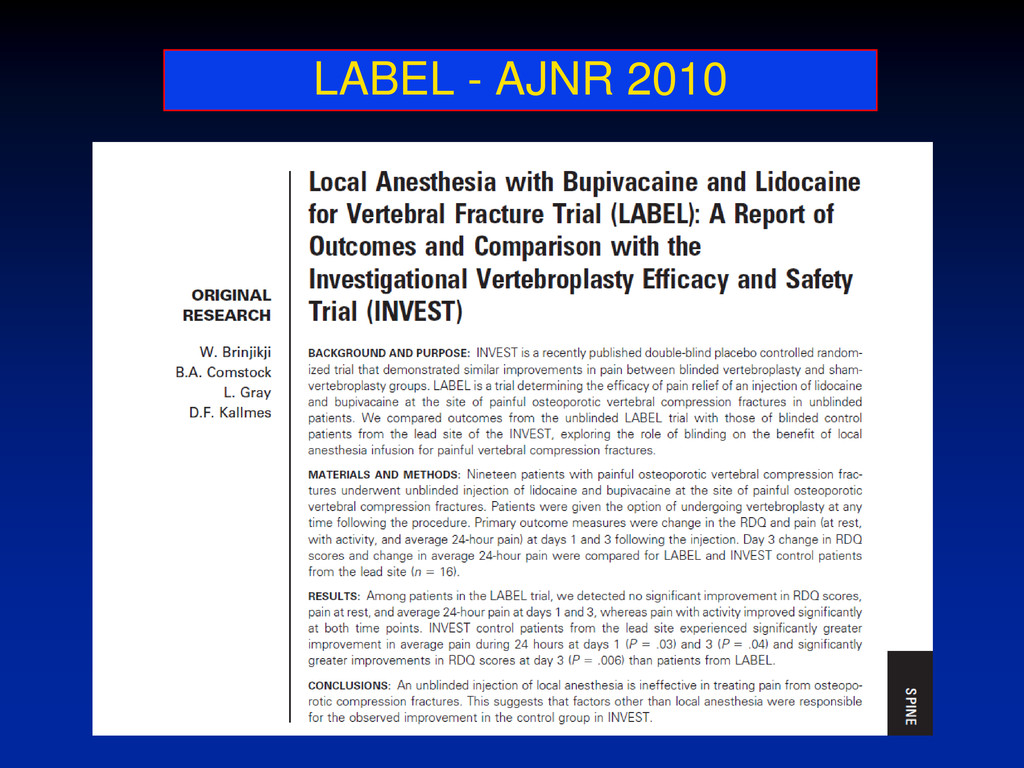
improvement in the majority but with no significant difference between the local anaesthetic and vertebroplasty groups. Potential explanations include placebo response or therapeutic response to the control procedure. • We investigated whether preliminary facet joint injection can identify those patients whose pain arises from paravertebral structures rather than the vertebral insufficiency fracture itself.
for treatment by vertebroplasty were first offered local anaesthetic and steroid facet joint injection (FJI) at the most painful level. Those who failed to respond were offered a vertebroplasty. RESULTS: 91 patients referred, 16 went straight to vertebroplasty. 61 of 75 were initially offered FJI. 21 were successful; two relapsed, had further FJIs with good results; 3 declined treatment; 5 had temporary benefit; 1 died from unrelated causes. Of 29 who failed to respond to FJIs, 24 underwent vertebroplasty and 23 had a successful outcome. • CONCLUSIONS: A third of patients technically suitable for vertebroplasty responded beneficially to FJI. In this group the pain mediator maybe one of instability and overload on the facet joints produced by adjacent wedge fracture. This protocol allows more selective and more successful vertebroplasty.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}