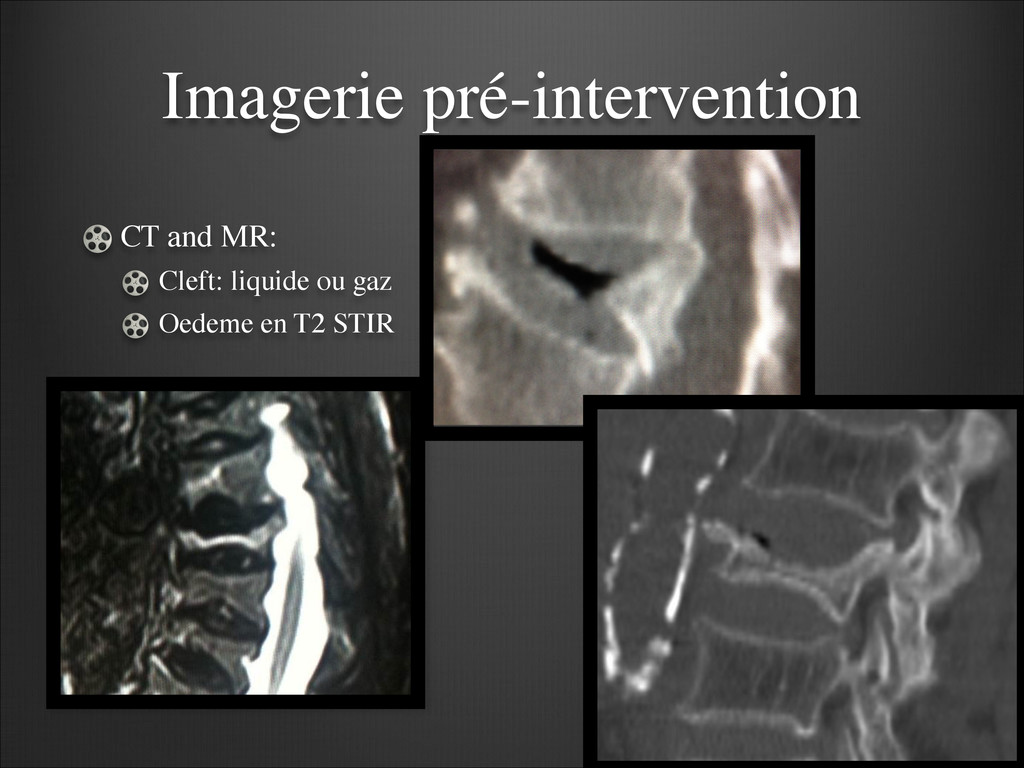
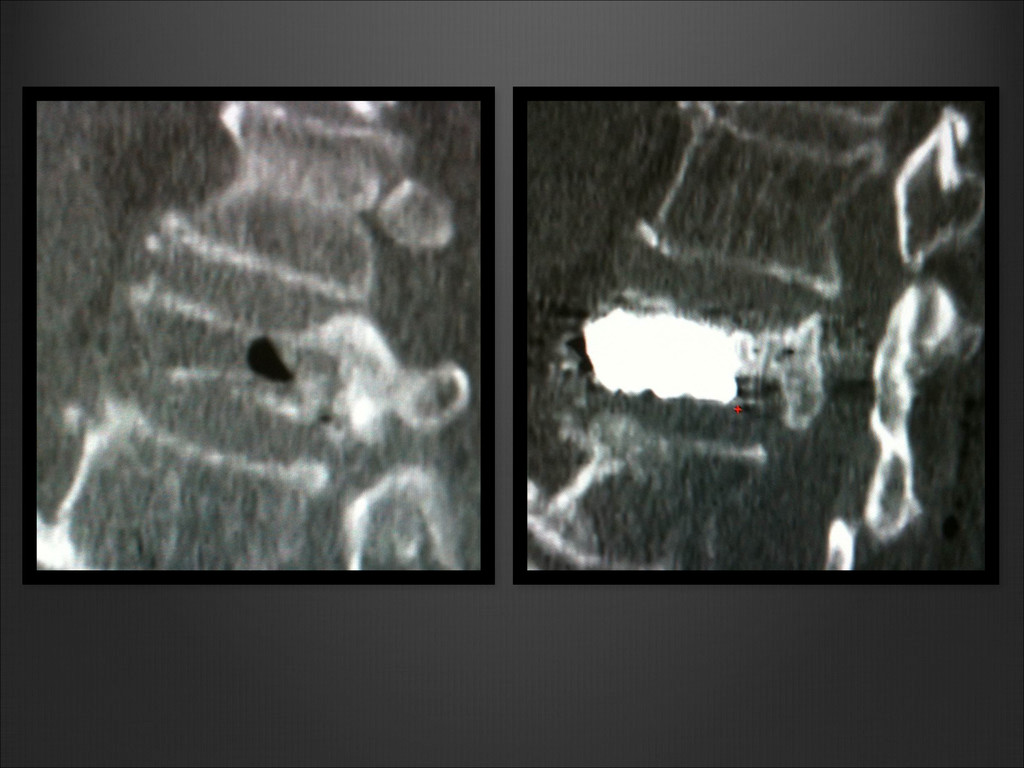
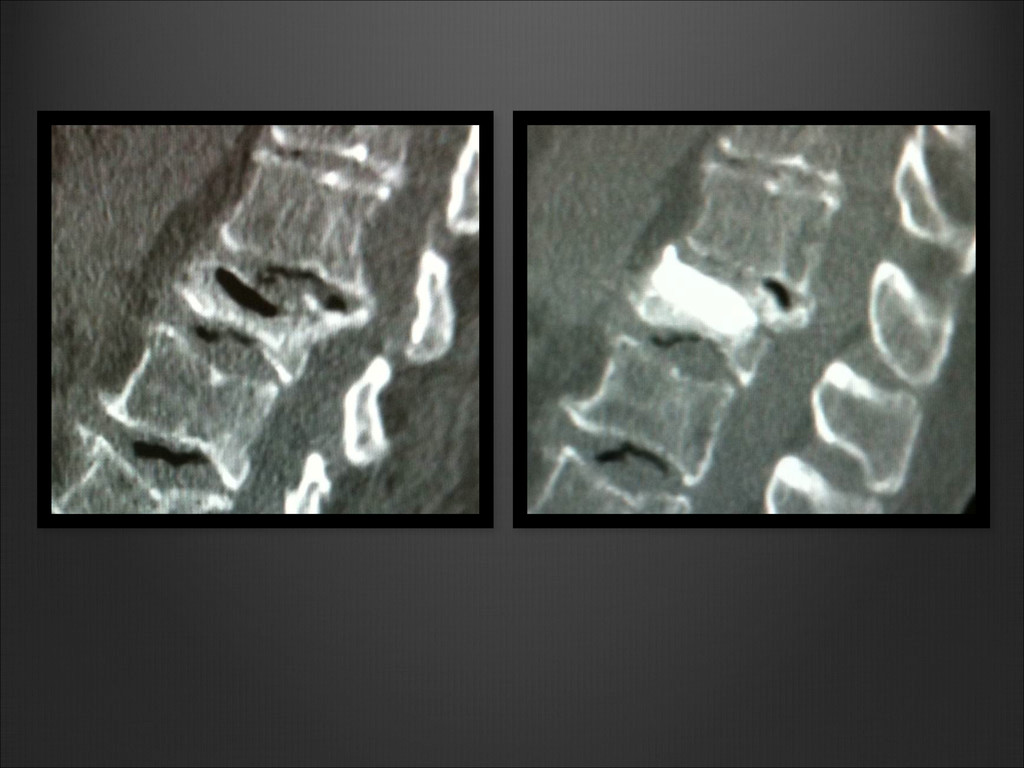
Le clivage gazeux ou liquide: considéré comme pathognomonique d’une necrose avasculaire du corps vertebral ? Ou plutôt trait de fracture non consolidé ?(Kummell’s disease) . La pression au sein de ce clivage est inférieure à la pression osseuse trabéculaire adjacente. (Theodorou DJ Radiology 2001) (Malghem J Radiology 1993) (Lane J AJNR 2002)
plus grande mobilité prédisposant à la pseudarthrose. Le clivage apparaît premièrement au niveau de la portion supérieure sous le plateau vertébral: vascularisation plus grêle, et détérioration architecturale plus importante. ! McKiernan F et al. Arthritis Rheum 2003;48:1414-9
de consolidation.(McKiernan F et al. J Bone Miner Res 2003;18:24–9) ! Ironiquement, ce clivage apparaîtrait comme étant un élément de réussite clinique de la vertèbroplastie facilitant la restauration anatomique durant la vertèbroplastie: c’est ce que nous allons voir…
de la vertebroplastie étude prospective de 50 patients Percutaneous vertebroplasty: does the presence of intravertebral cleft impact the effectiveness of the procedure? L Huwart, PY Marcy, P Foti, ME Amoretti, O Hauger, P Brunner, N Amoretti .RSNA 2012
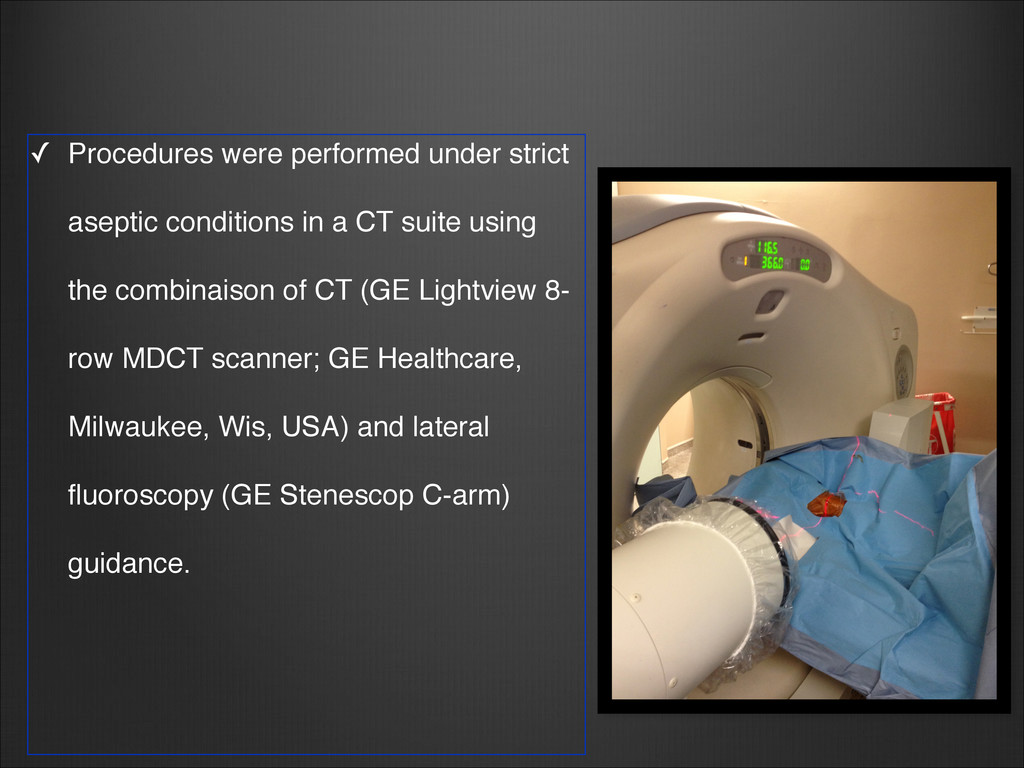
CT suite using the combinaison of CT (GE Lightview 8- row MDCT scanner; GE Healthcare, Milwaukee, Wis, USA) and lateral fluoroscopy (GE Stenescop C-arm) guidance.
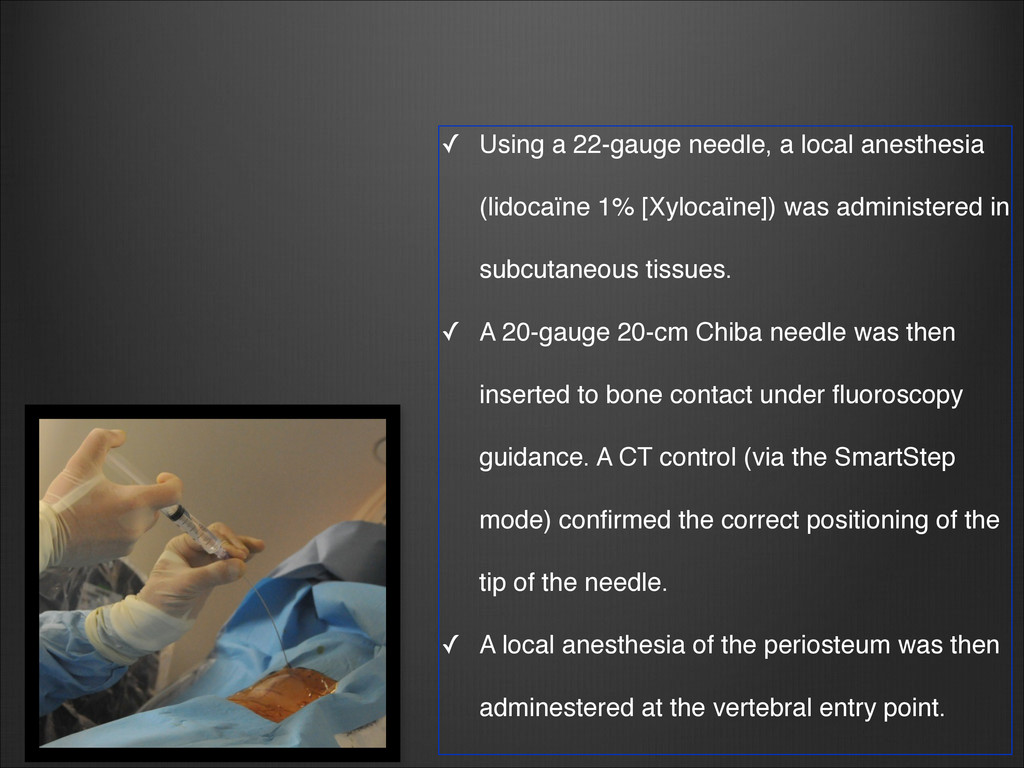
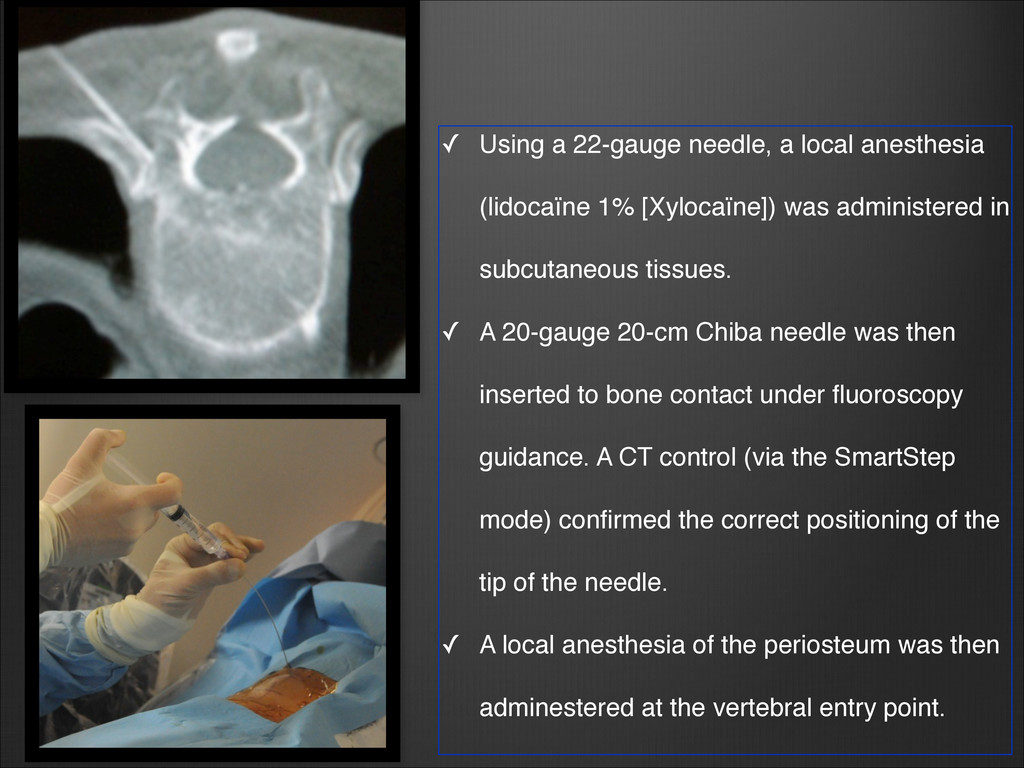
[Xylocaïne]) was administered in subcutaneous tissues. ✓ A 20-gauge 20-cm Chiba needle was then inserted to bone contact under fluoroscopy guidance. A CT control (via the SmartStep mode) confirmed the correct positioning of the tip of the needle. ✓ A local anesthesia of the periosteum was then adminestered at the vertebral entry point. !
[Xylocaïne]) was administered in subcutaneous tissues. ✓ A 20-gauge 20-cm Chiba needle was then inserted to bone contact under fluoroscopy guidance. A CT control (via the SmartStep mode) confirmed the correct positioning of the tip of the needle. ✓ A local anesthesia of the periosteum was then adminestered at the vertebral entry point. !
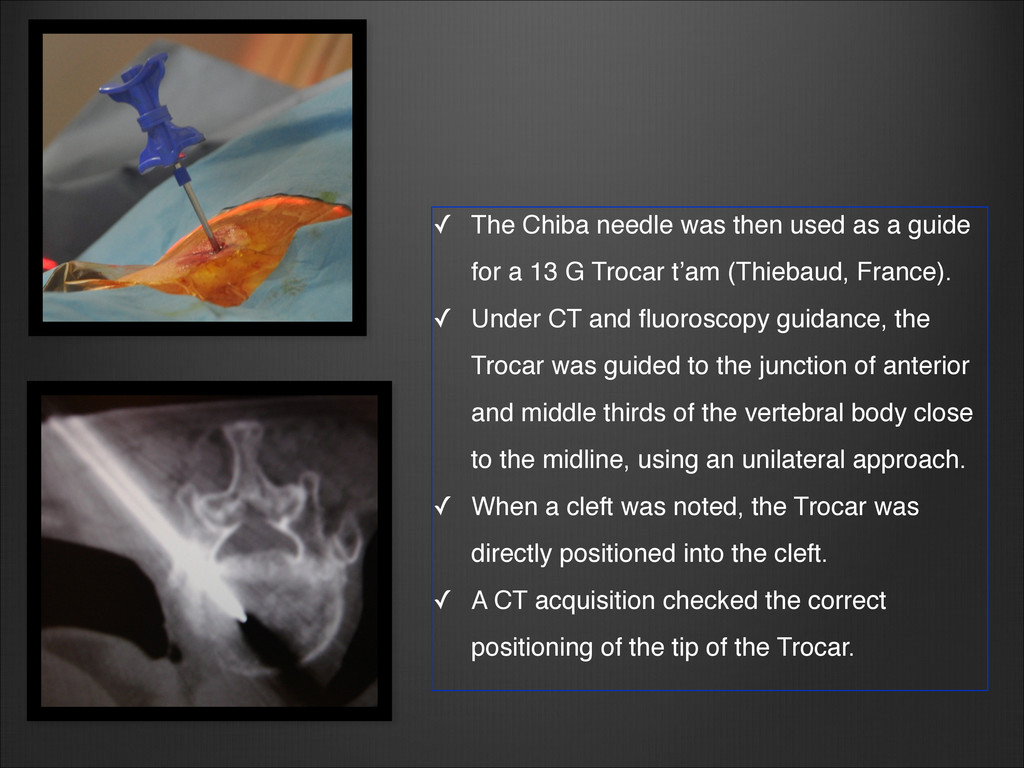
for a 13 G Trocar t’am (Thiebaud, France). ! ✓ Under CT and fluoroscopy guidance, the Trocar was guided to the junction of anterior and middle thirds of the vertebral body close to the midline, using an unilateral approach. ✓ When a cleft was noted, the Trocar was directly positioned into the cleft. ✓ A CT acquisition checked the correct positioning of the tip of the Trocar.
mixer with tungsten powder (4 g) to increase its radiopacity. ! ✓ Under CT and fluoroscopy guidance, cement was injected in its pasty phase by using 1-cc luer-lock syringes until adequate distribution was obtained. ✓ If adequate distribution was not possible through unilateral access, then the above process was repeated through the contra-lateral approach
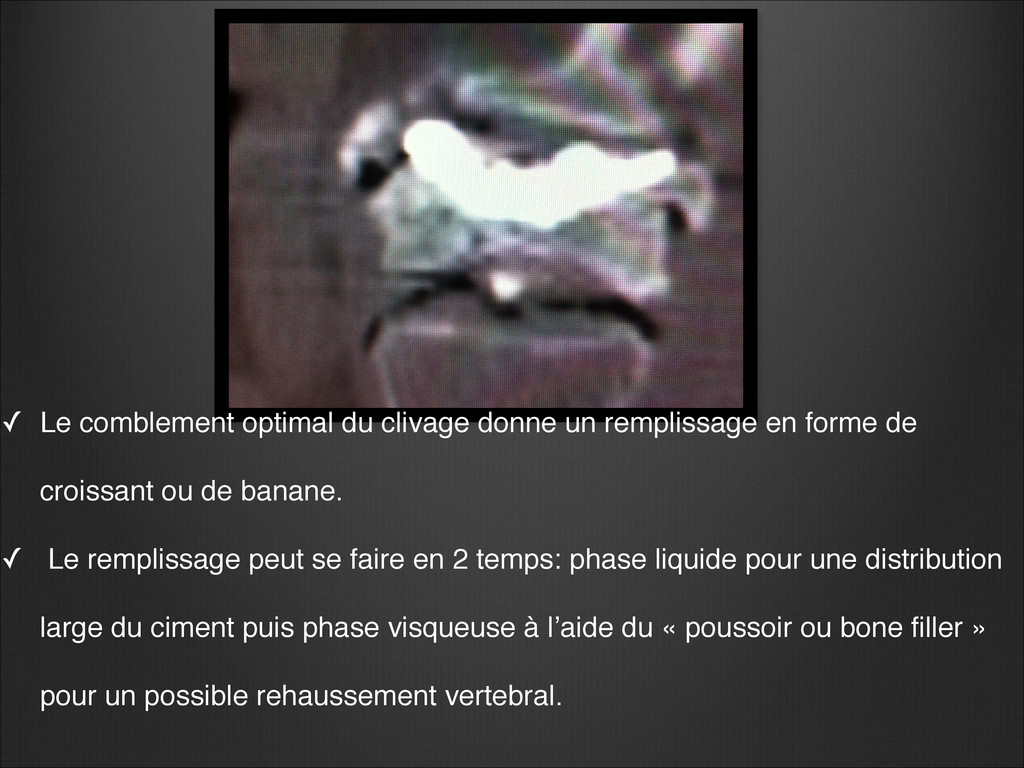
forme de croissant ou de banane. ✓ Le remplissage peut se faire en 2 temps: phase liquide pour une distribution large du ciment puis phase visqueuse à l’aide du « poussoir ou bone filler » pour un possible rehaussement vertebral.
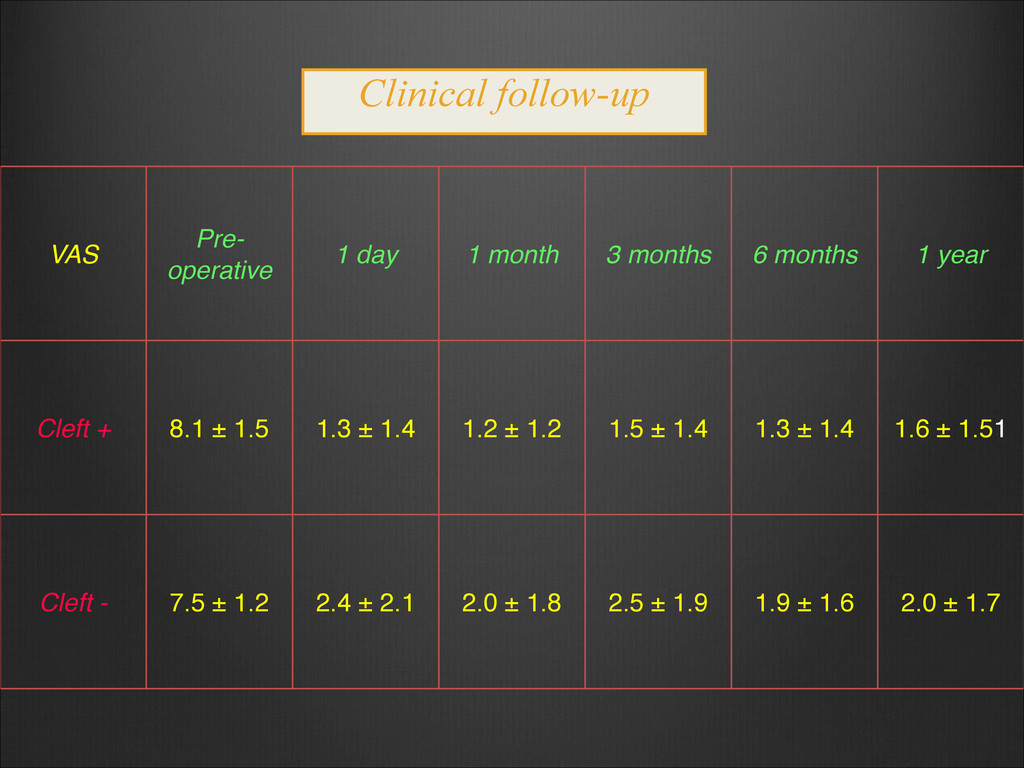
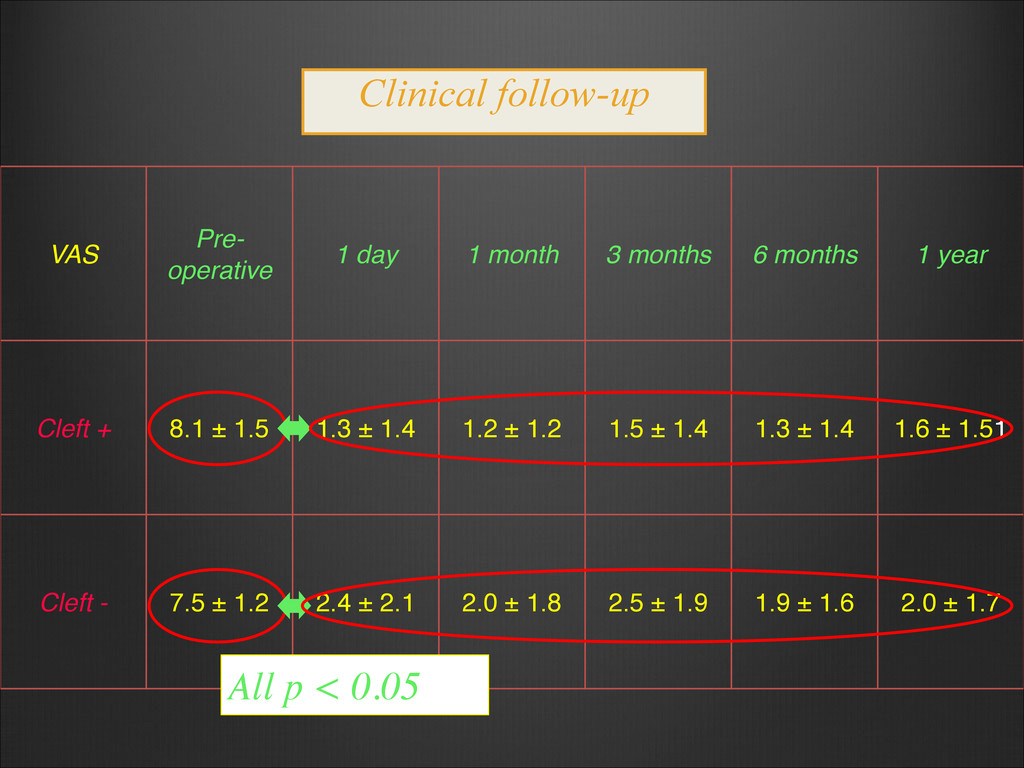
1 month, 3 months, 6 months and 1 year after the vertebroplasty: ➢ Visual Analog Score (VAS) score was measured at these 5 follow-up examinations. ➢ Pre- and post-operative scores were compared using the non- parametric Wilcoxon signed rank test for paired data. ✓ In case of new onset of back pain, MR and CT imaging were performed to detect adjacent new vertebral compression fractures.! ! !
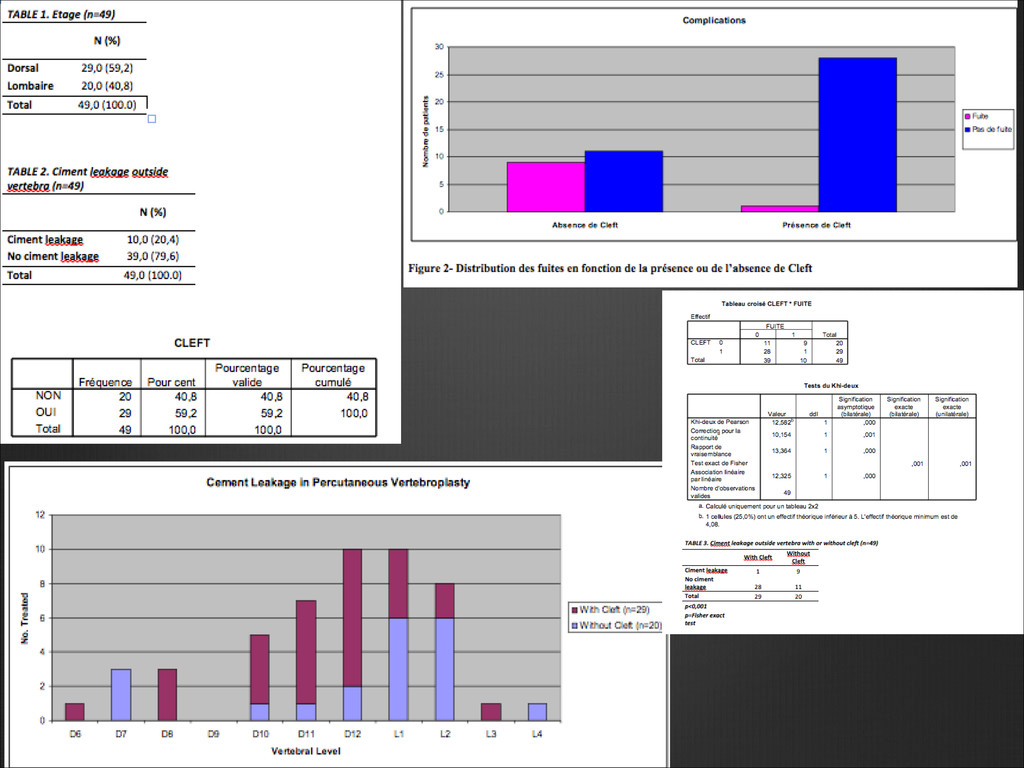
with 80% at the thoraco-lumbar junction (80%). ✓ Mean procedure time: 15 min (range, 10 - 20 min) ✓ Procedures were technically successful in all cases. ✓ Interventions were well tolerated by patients. ✓ Cement leakages into adjacent disks in 10/50 cases (20 %) ✓ Seven (14%) adjacent VCFs occured during the year of follow-up, and were successfully treated by vertebroplasty.
group with cleft compared to that without (p = 0.098, Wilcoxon test) ✓ Is there a significant difference of decrease in postoperative VAS scores between clefted and unclefted vertebrae?! ➢ YES, between preoperative VAS and 1-day, 1-month, 3-month and 6-month VAS scores (p < 0.05 in all cases). ➢ NO between preoperative VAS and 1-year VAS score (p = 0.148). The impact of cleft on VAS
(0.5%) in clefted fractures ➢ 9/30 (30%) in unclefted fractures Cement leakages Significantly fewer cement leakages in the group with cleft (p = 0.0006)
cement bridge by filling the cleft. ✓ CT- and fluoroscopy-guided PVP performed under local anesthesia only was a safe, rapid and effective method to achieve this objective. A perfect positioning of the Trocar into the cleft was made possible thanks to the precision of dual guidance. When a cleft represents a fracture nonunion Lane JI et al. AJNR 2002;23:1642-6
decrease in back pain in patients with clefted fractures. Therefore, these patients may constitute an excellent treatment indication for vertebroplasty in terms of outcome. ✓ Our results concur with the study by Lane et al. (AJNR 2002;23:1642-6) who showed a trend toward greater pain relief being achieved 6 and 12 months after the procedure in patients with clefts. ✓ But disagree with others who reported less benefit (Nieuwenhuijse MJ Spine J 2011;11:839-48; Ha KY et al. J Bone Joint Surg Br 2006;88:629-33) or no difference in patients with clefted vertebrae (Krauss M et al. Eur Radiol. 2006;16:1015-21; Wiggins MC et al. AJR 2007;188:634-40). Does the presence of a cleft impact on the effectiveness of PVP?
more frequent in vertebrae without cleft. ✓ This finding is in agreement with other studies: Hiwatashi A et al. AJR 2007;188:1089-93; Koh YH et al. Acta Radiol. 2007;48:315-20.! ✓ But disagrees with others: Tanigawa N et al. AJR 2009;193:442-5; Nieuwenhuijse MJ Spine J 2011;11:839-48. Is the cleft a risk factor for the occurrence of disk cement leakage?
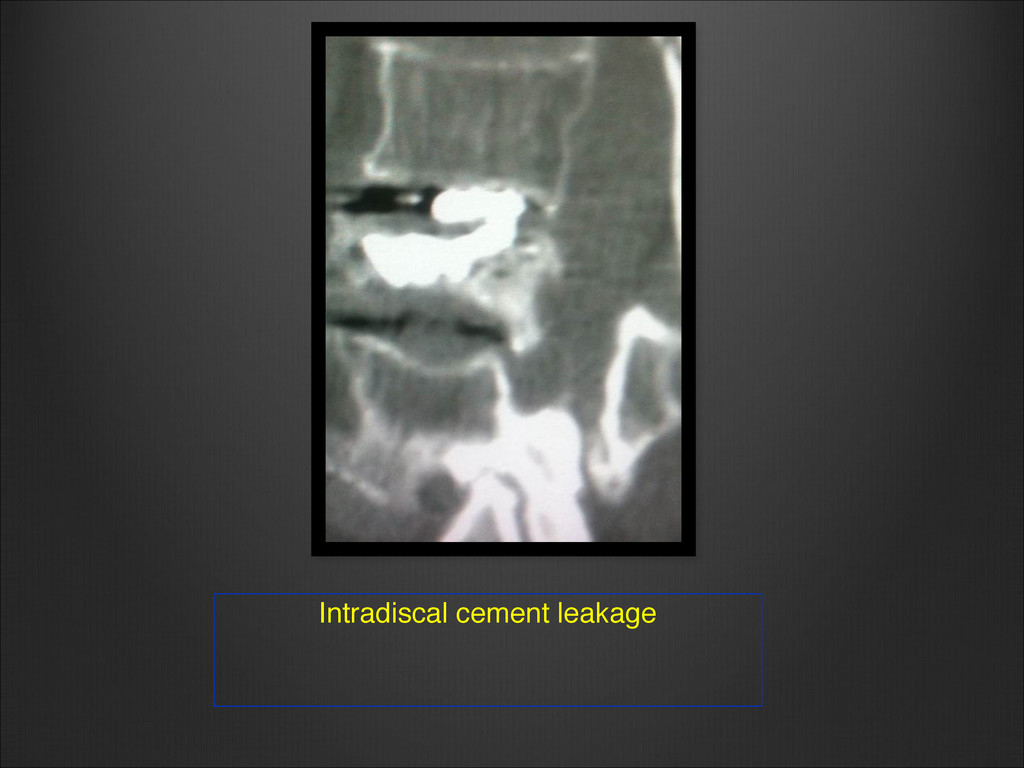
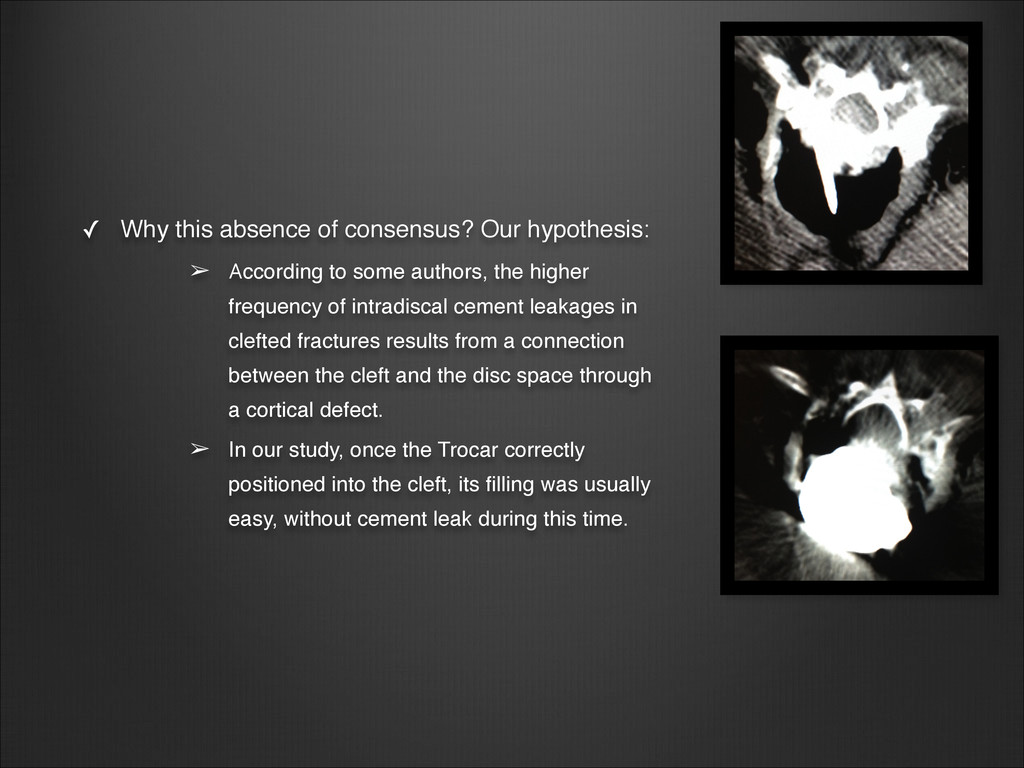
to some authors, the higher frequency of intradiscal cement leakages in clefted fractures results from a connection between the cleft and the disc space through a cortical defect. ➢ In our study, once the Trocar correctly positioned into the cleft, its filling was usually easy, without cement leak during this time.
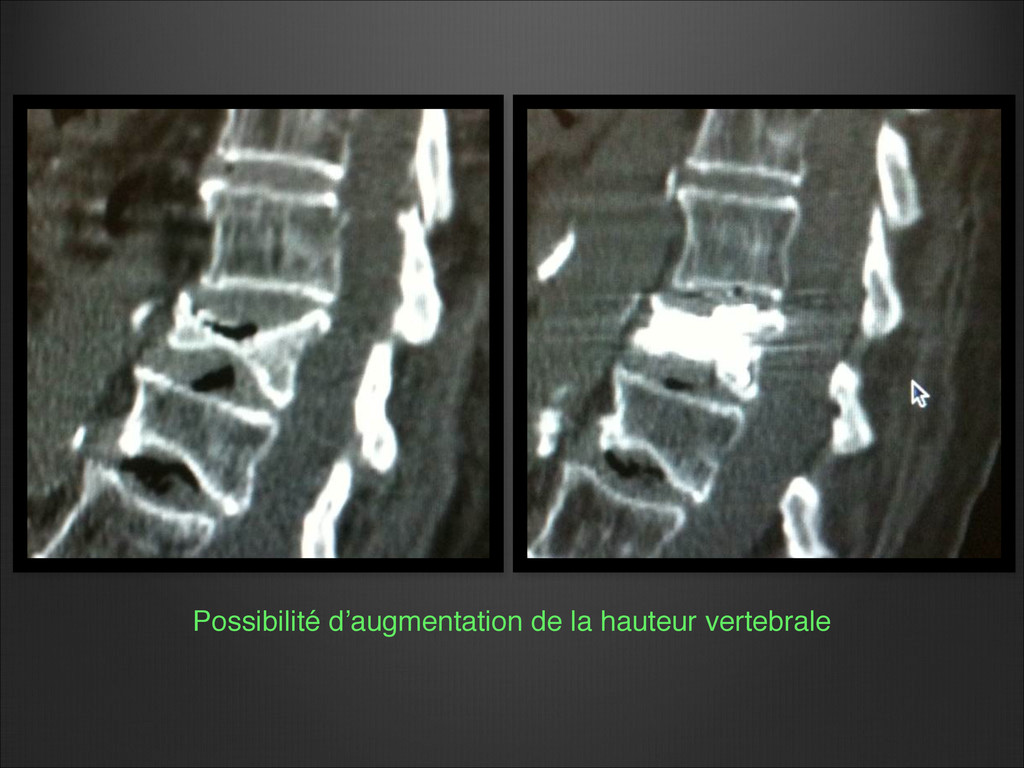
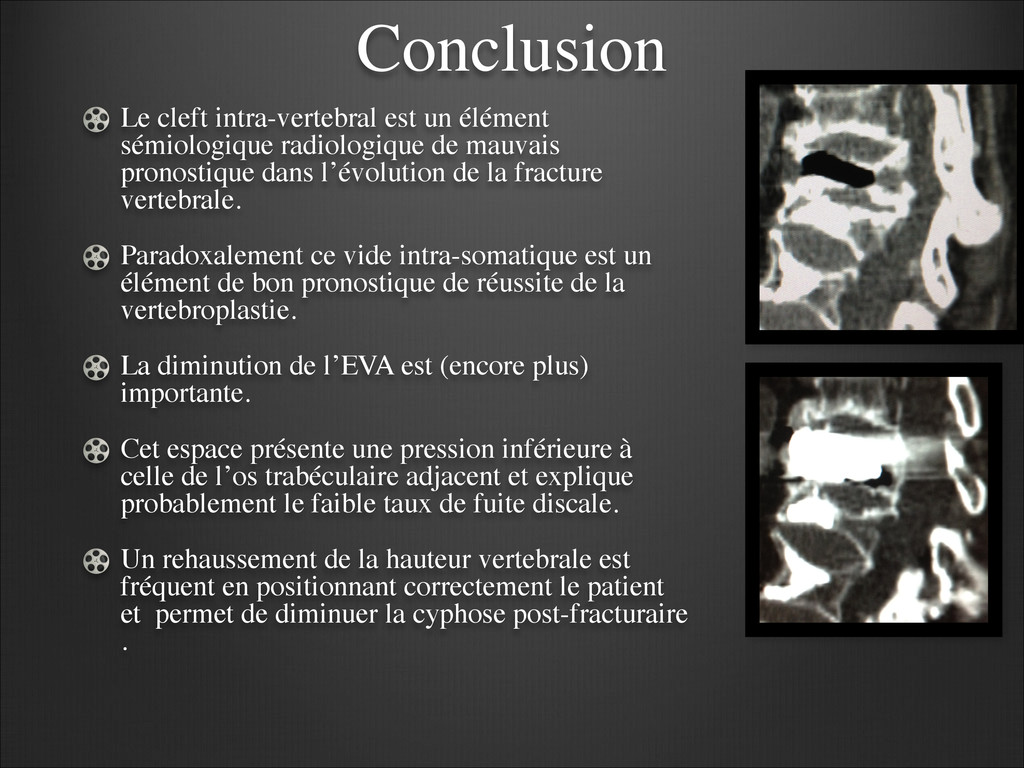
mauvais pronostique dans l’évolution de la fracture vertebrale. Paradoxalement ce vide intra-somatique est un élément de bon pronostique de réussite de la vertebroplastie. La diminution de l’EVA est (encore plus) importante. Cet espace présente une pression inférieure à celle de l’os trabéculaire adjacent et explique probablement le faible taux de fuite discale. Un rehaussement de la hauteur vertebrale est fréquent en positionnant correctement le patient et permet de diminuer la cyphose post-fracturaire .
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}