grant from Medtronic Spinal & Biologics Europe ! The sponsor was not involved in the panel process and preparation of the slides ! Panel members received honoraria from the sponsor for the rating activities and their participation in the panel meetings ! The study was coordinated by Ismar Healthcare, Lier, Belgium
of osteoporosis and can have a high impact on QoL1 • Common treatment options are non-surgical management (NSM), vertebroplasty (VP) and balloon kyphoplasty (BKP) • High-quality evidence to support treatment choice is limited and inconclusive • As a consequence, most guidelines are non very specific 1 J Bone Miner Res 2002;17:716-24.
of VCF at the patient-specific level, by combining evidence from clinical studies and expert opinion ! • To translate these criteria into clinically useful recommendations Aims
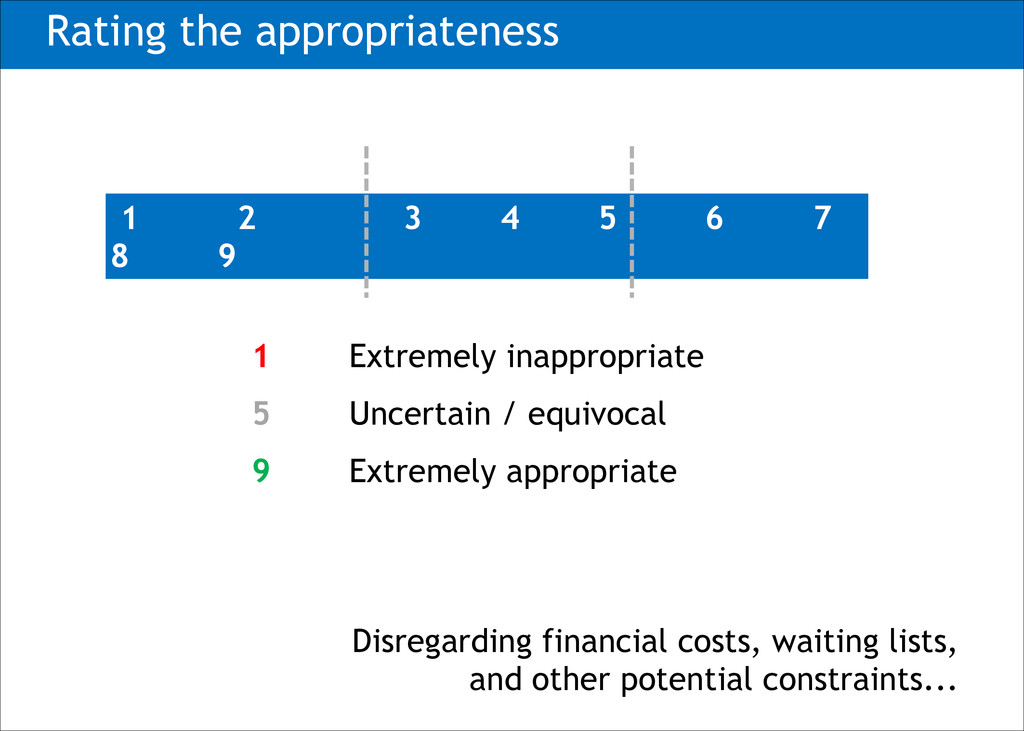
evidence ̶ Collective judgement of experts to assess the appropriateness of performing a procedure at the level of a patient’s symptoms, medical history and test results • A procedure is considered appropriate if its expected benefits outweigh its potential negative consequences by a sufficient margin that the procedure is worth doing RAND/UCLA Appropriateness Method1 1 Brook RH et al Int J Technol Assess Health Care 1986;2:53-63.
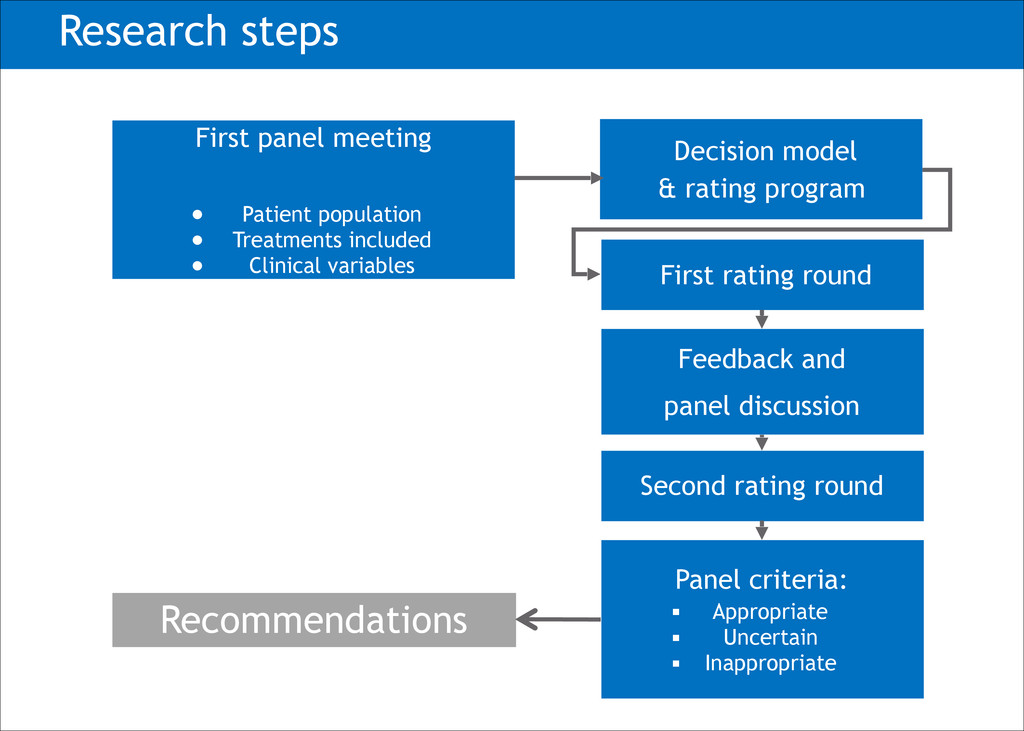
Panel criteria: ! ▪ Appropriate ▪ Uncertain ▪ Inappropriate First panel meeting ! • Patient population • Treatments included • Clinical variables Decision model & rating program Research steps Recommendations
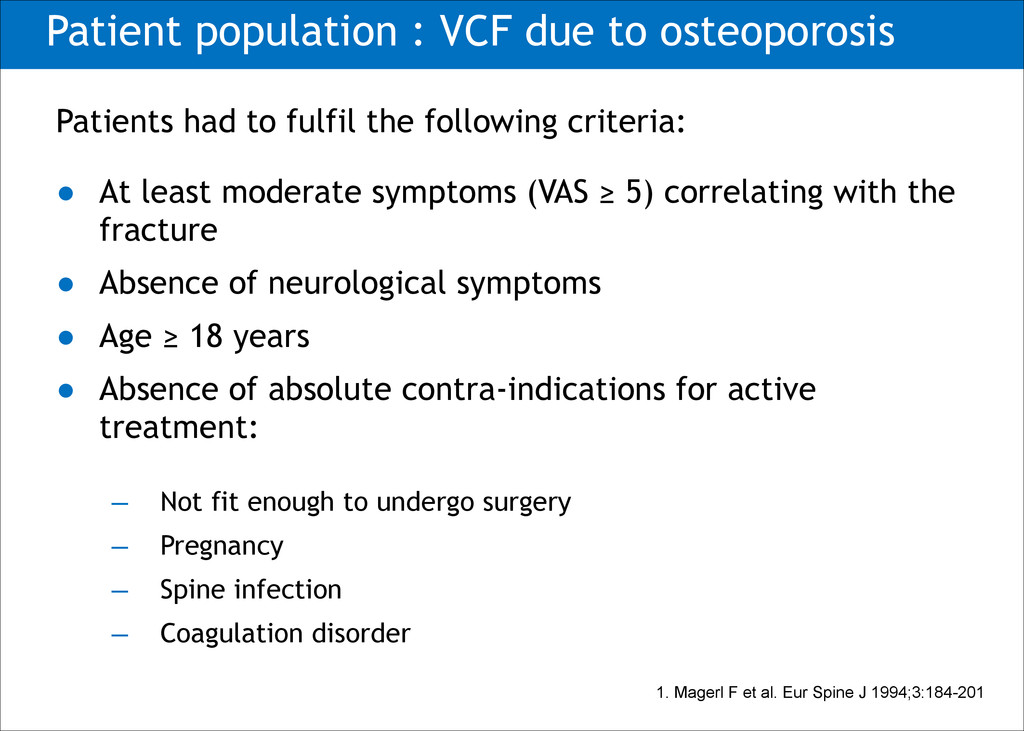
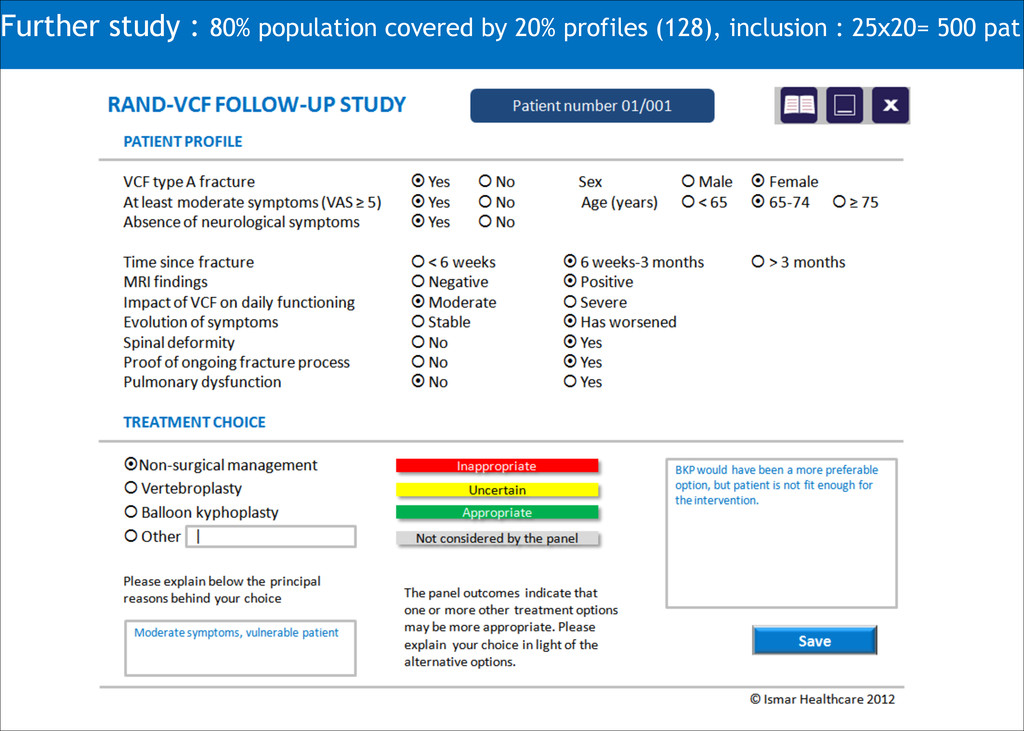
fulfil the following criteria: • At least moderate symptoms (VAS ≥ 5) correlating with the fracture • Absence of neurological symptoms • Age ≥ 18 years • Absence of absolute contra-indications for active treatment: ̶ Not fit enough to undergo surgery ̶ Pregnancy ̶ Spine infection ̶ Coagulation disorder 1. Magerl F et al. Eur Spine J 1994;3:184-201
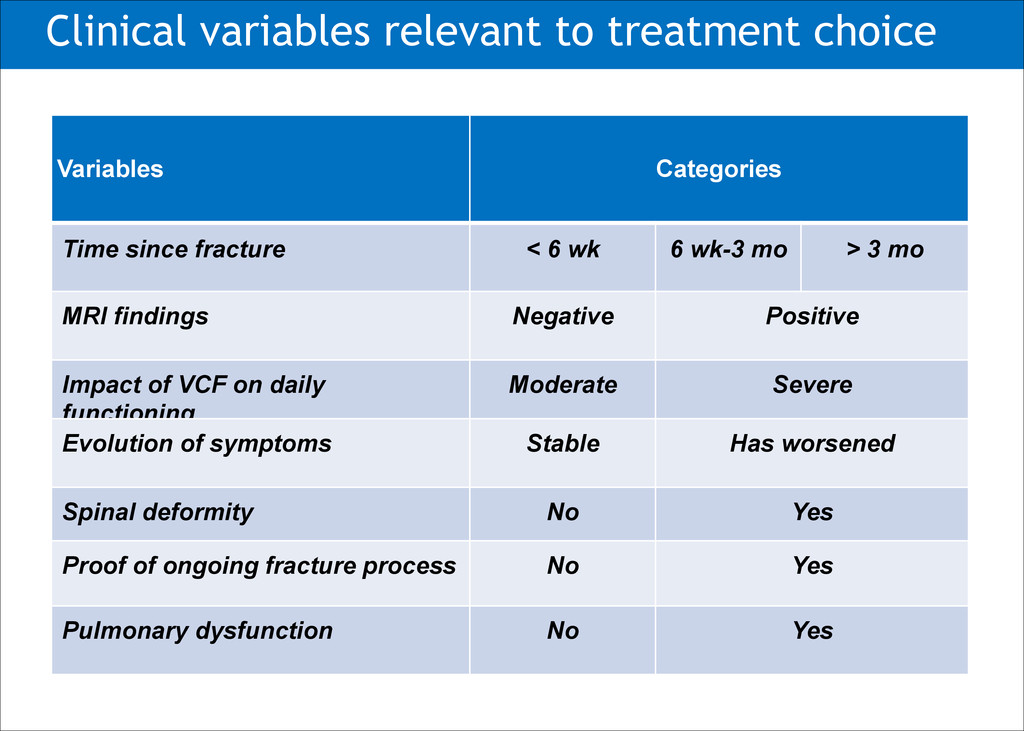
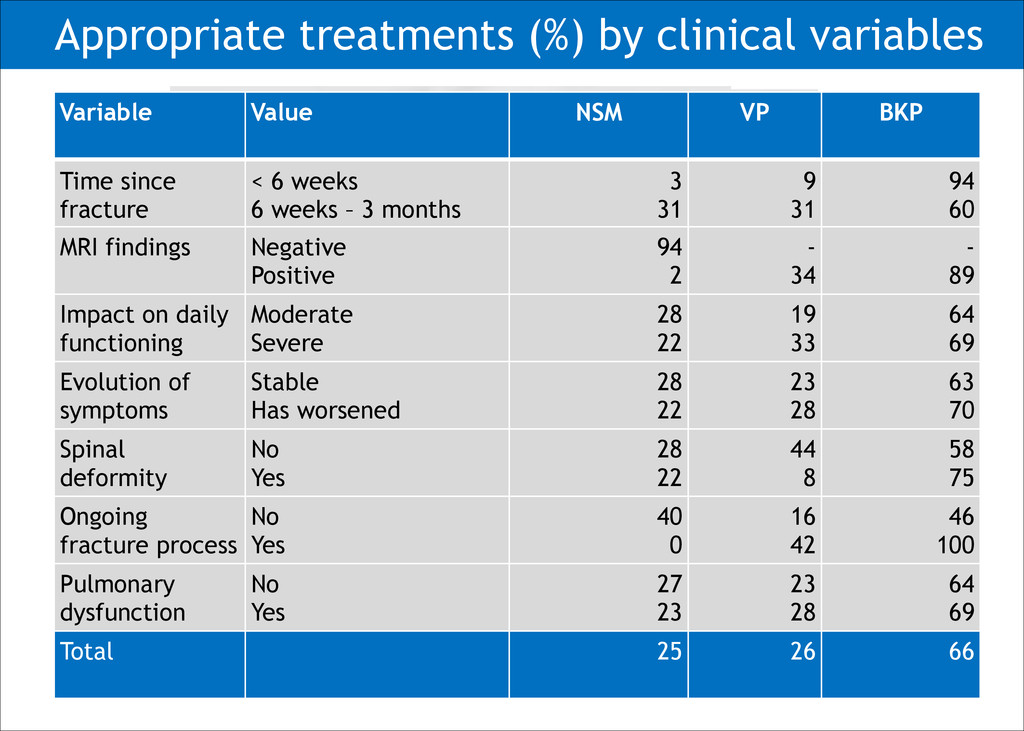
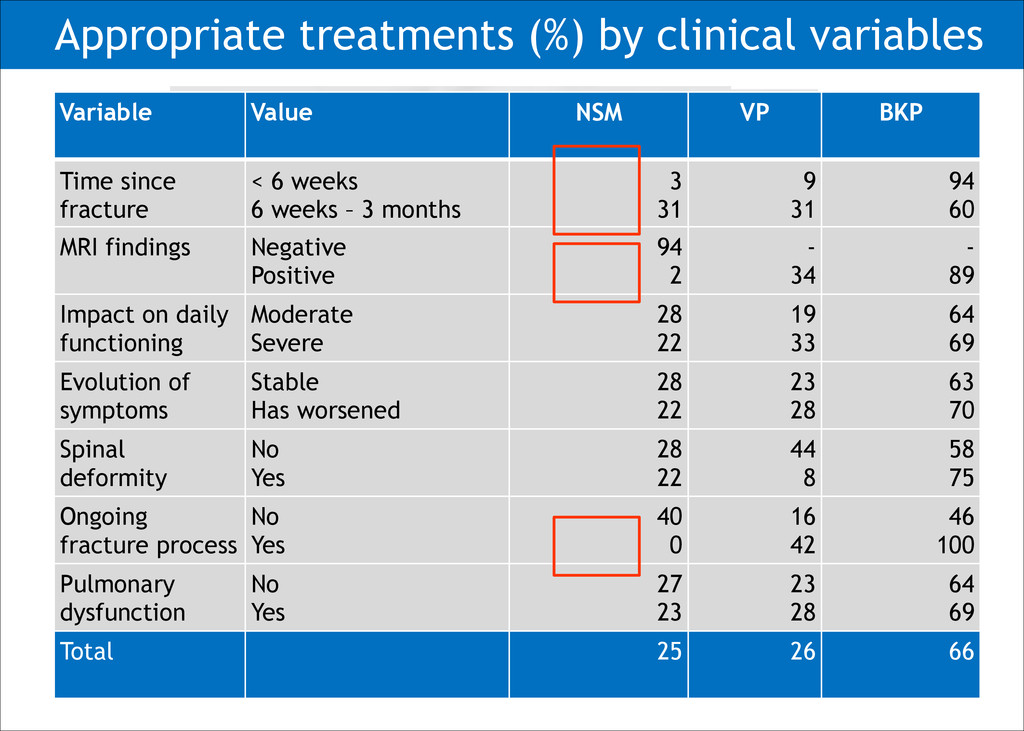
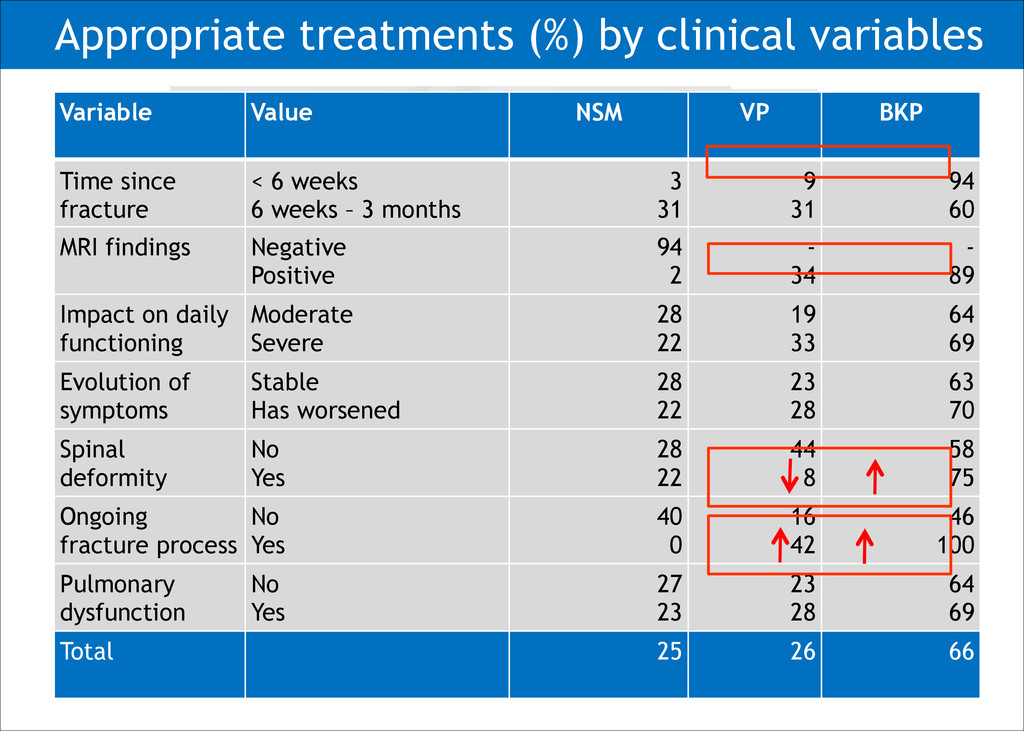
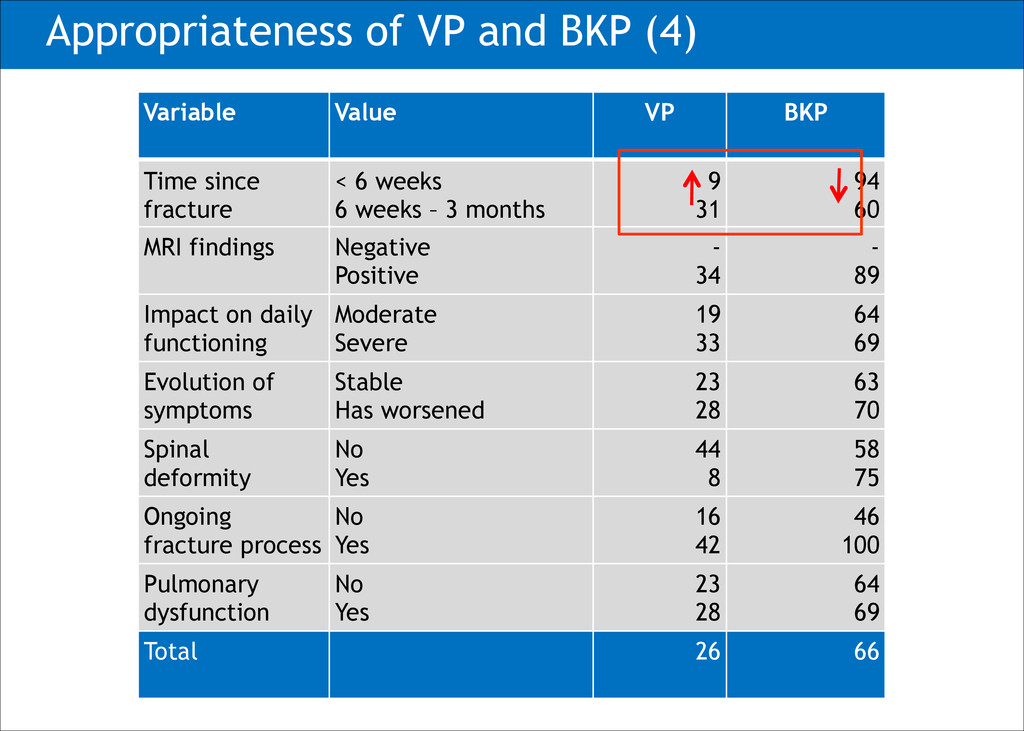
fracture < 6 wk 6 wk-3 mo > 3 mo MRI findings Negative Positive Impact of VCF on daily functioning Moderate Severe Evolution of symptoms Stable Has worsened Spinal deformity No Yes Proof of ongoing fracture process No Yes Pulmonary dysfunction No Yes
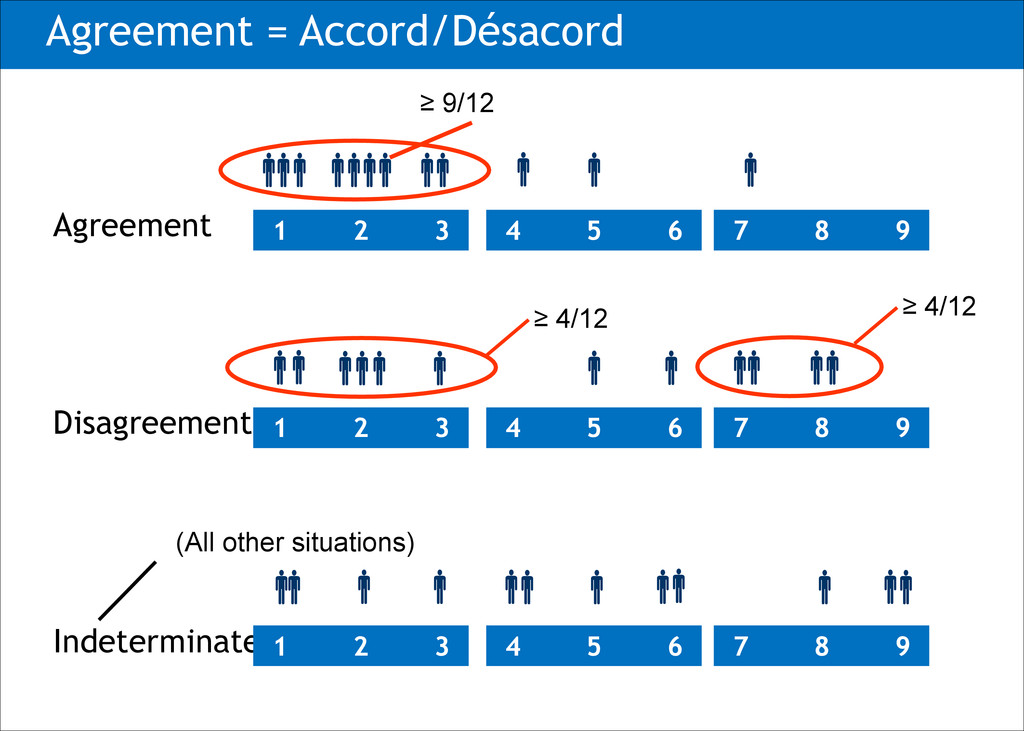
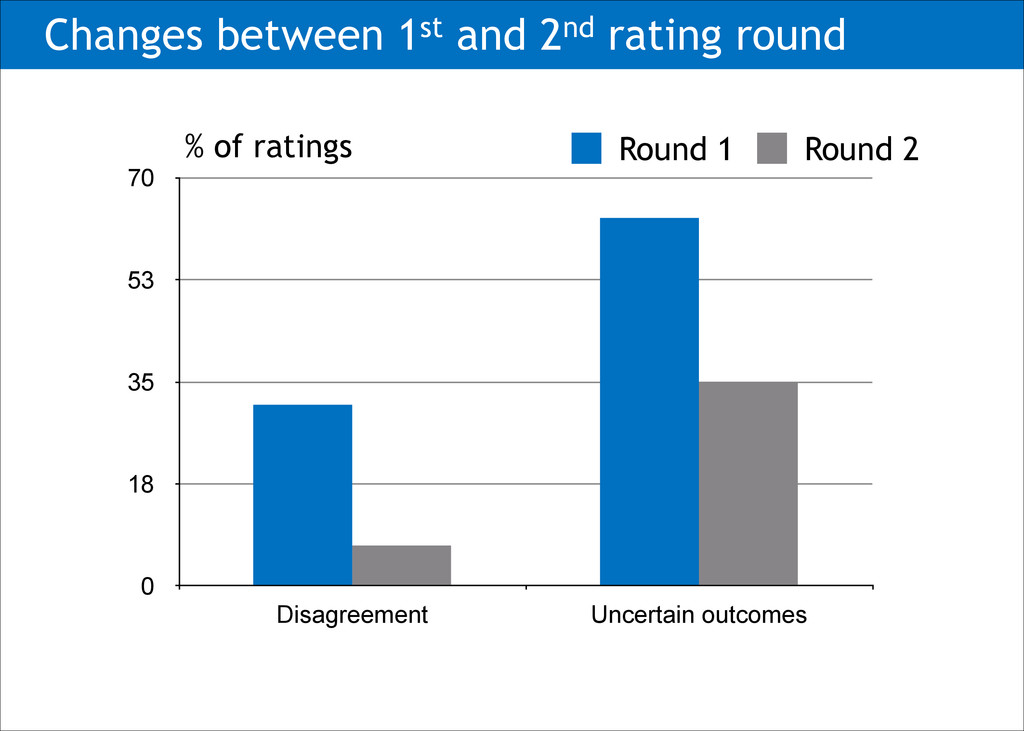
3 treatment options (NSM, VP, BKP) had to be rated • Substantial disagreement : 31% due to: ― Different ways of rating ― Different interpretation of definitions and cases ― Variations in opinion between specialties à Adaptation of rating structure, exclusion of unrealistic cases, refinement of instructions à Second rating round: 128 cases
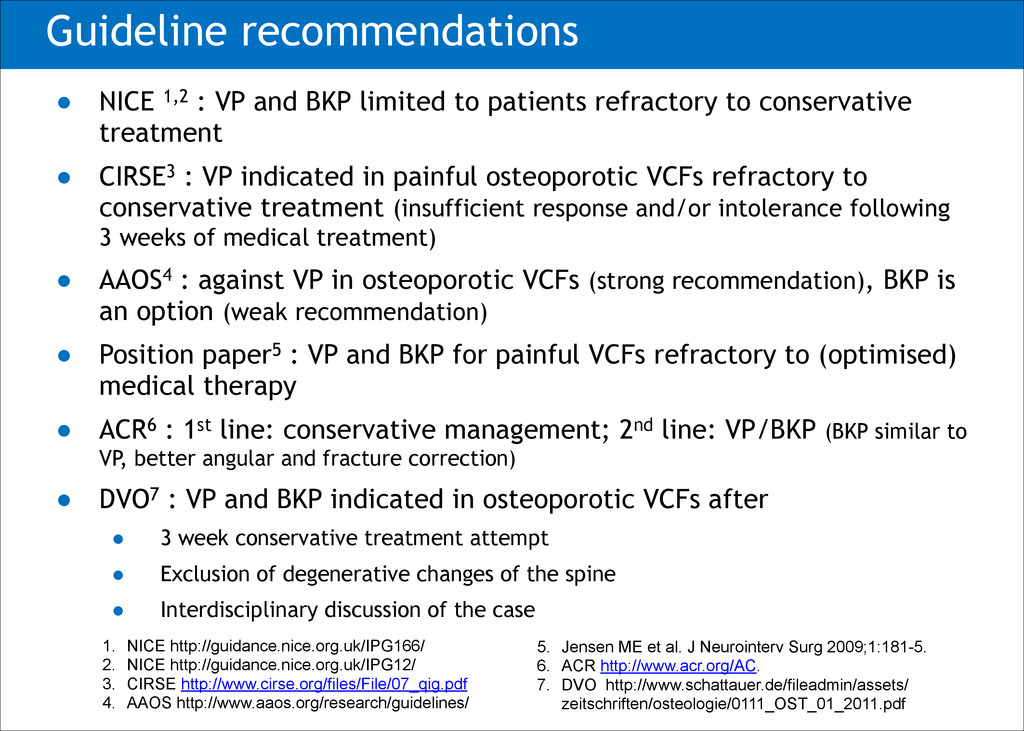
to patients refractory to conservative treatment • CIRSE3 : VP indicated in painful osteoporotic VCFs refractory to conservative treatment (insufficient response and/or intolerance following 3 weeks of medical treatment) • AAOS4 : against VP in osteoporotic VCFs (strong recommendation), BKP is an option (weak recommendation) • Position paper5 : VP and BKP for painful VCFs refractory to (optimised) medical therapy • ACR6 : 1st line: conservative management; 2nd line: VP/BKP (BKP similar to VP, better angular and fracture correction) • DVO7 : VP and BKP indicated in osteoporotic VCFs after • 3 week conservative treatment attempt • Exclusion of degenerative changes of the spine • Interdisciplinary discussion of the case 1. NICE http://guidance.nice.org.uk/IPG166/ 2. NICE http://guidance.nice.org.uk/IPG12/ 3. CIRSE http://www.cirse.org/files/File/07_qig.pdf 4. AAOS http://www.aaos.org/research/guidelines/ ! 5. Jensen ME et al. J Neurointerv Surg 2009;1:181-5. 6. ACR http://www.acr.org/AC. 7. DVO_http://www.schattauer.de/fileadmin/assets/ zeitschriften/osteologie/0111_OST_01_2011.pdf
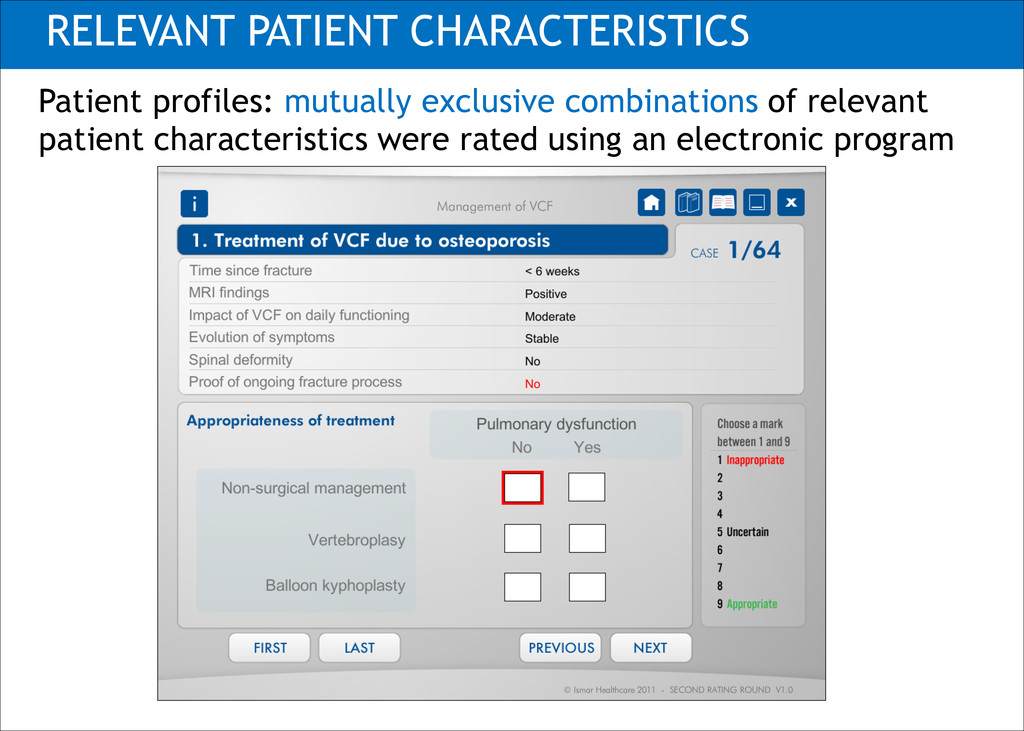
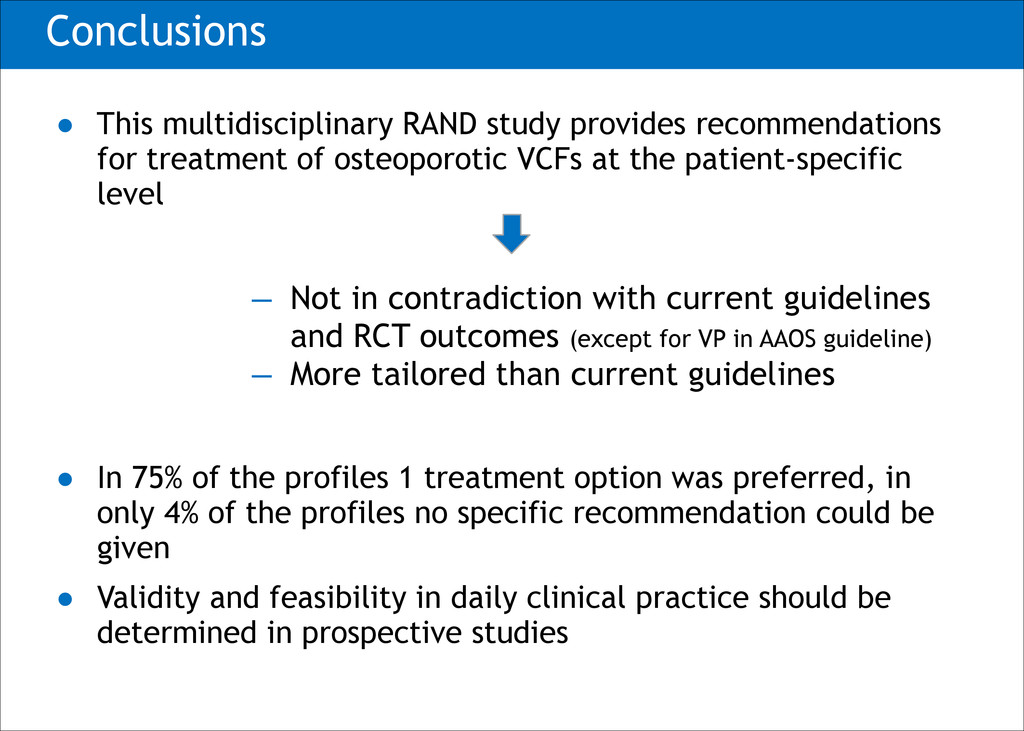
of osteoporotic VCFs at the patient-specific level ! ! ! ! ! • In 75% of the profiles 1 treatment option was preferred, in only 4% of the profiles no specific recommendation could be given • Validity and feasibility in daily clinical practice should be determined in prospective studies ̶ Not in contradiction with current guidelines and RCT outcomes (except for VP in AAOS guideline) ̶ More tailored than current guidelines
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}