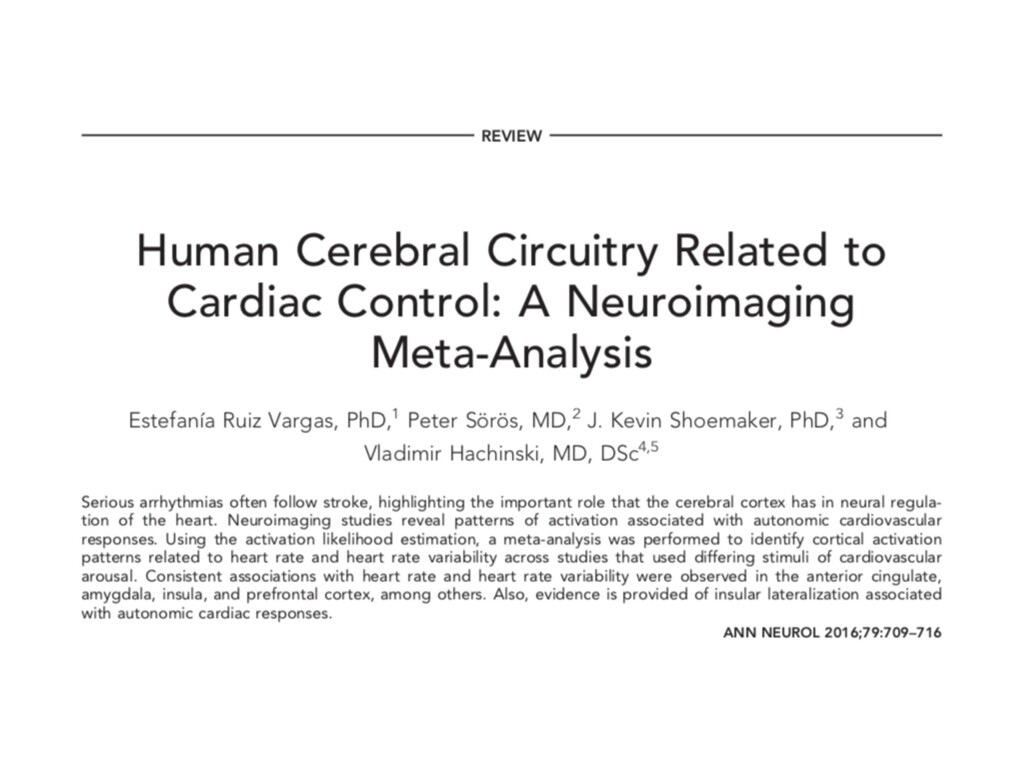
The brain controls the autonomic nervous system. Important areas are: the insula, the anterior cingulate cortex, medial prefrontal cortex, amygdala, and hypothalamus. This presentation will summarize:
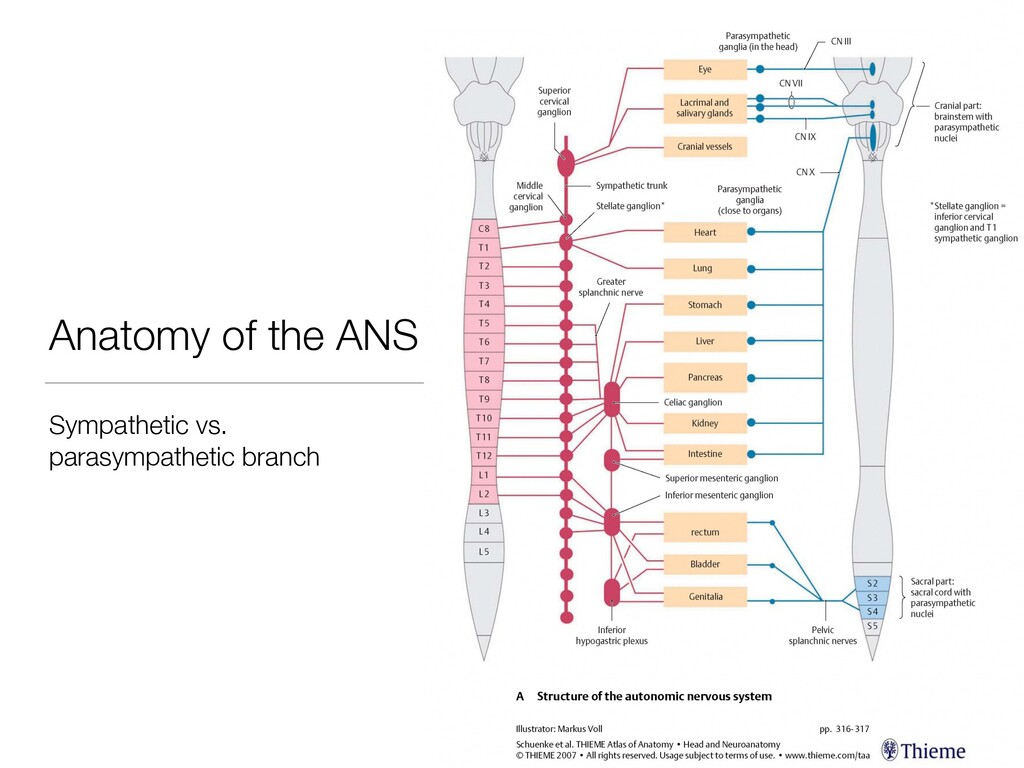
1. The anatomy and physiology of the ANS
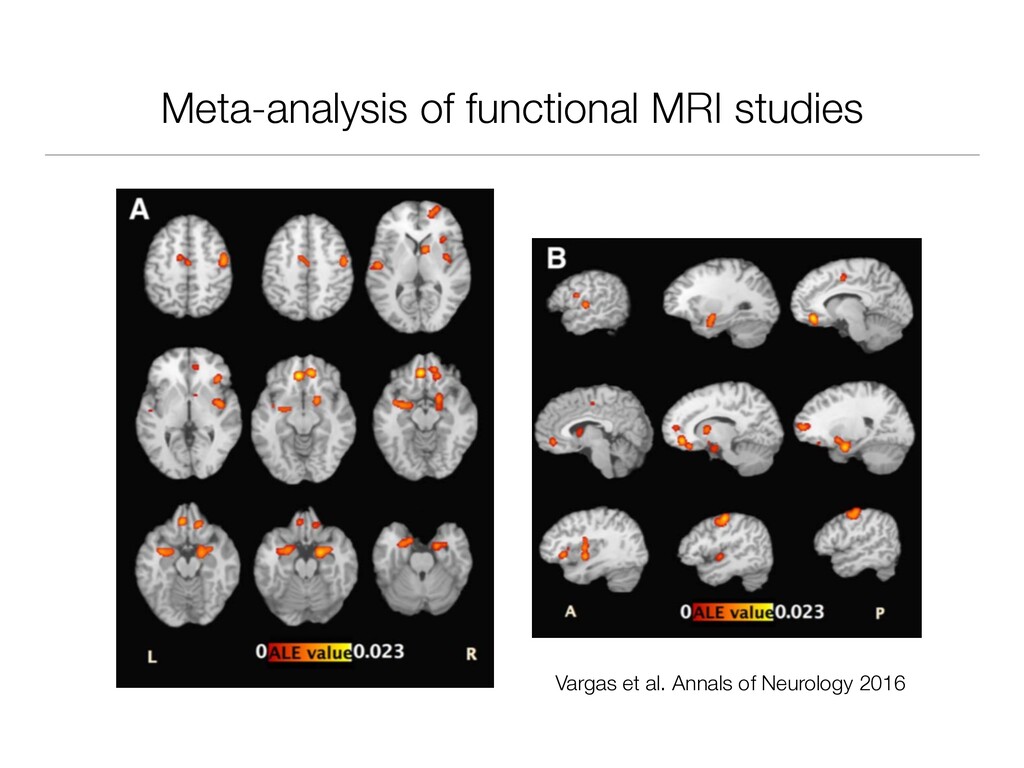
2. Central control of the ANS
3. Clinical relevance of autonomic dysregulation
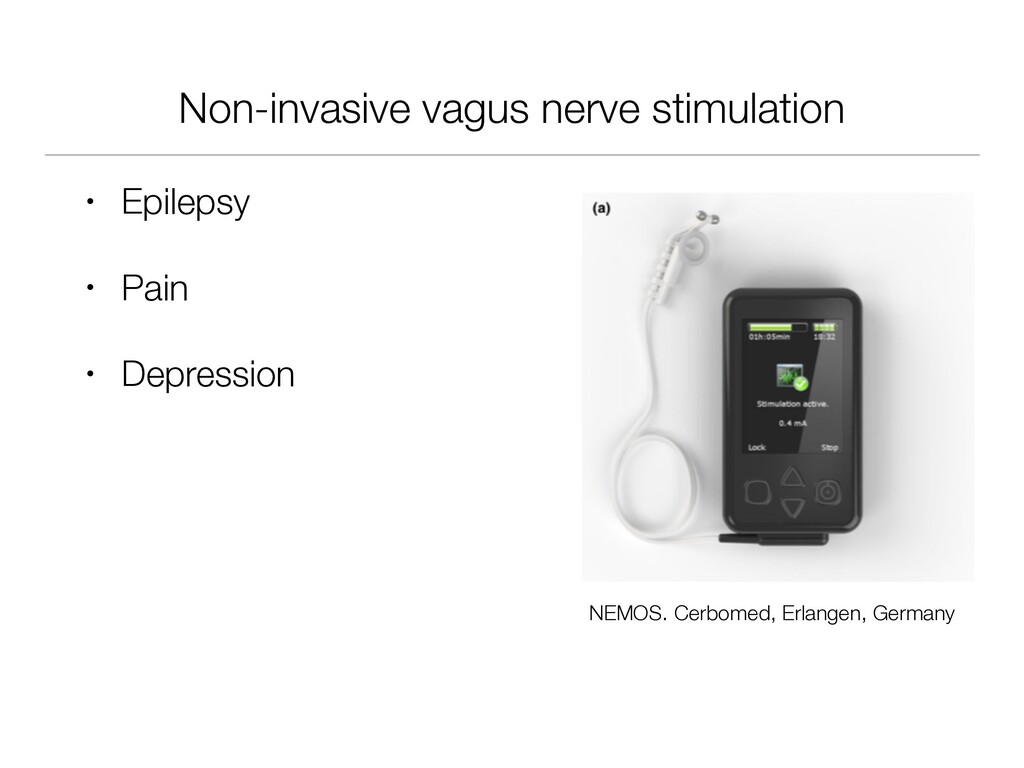
4. Modulation of ANS activity
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}