at the Department of Community Medicine, University College of Medical Sciences. It is being distributed under a CC – BY – NC (Attribution-Non-Commercial 3.0 Unported) License 2 Estimating Risk: RR, OR, Adjusted OR by Pranab Chatterjee is licensed under a Creative Commons Attribution-NonCommercial 3.0 Unported License.
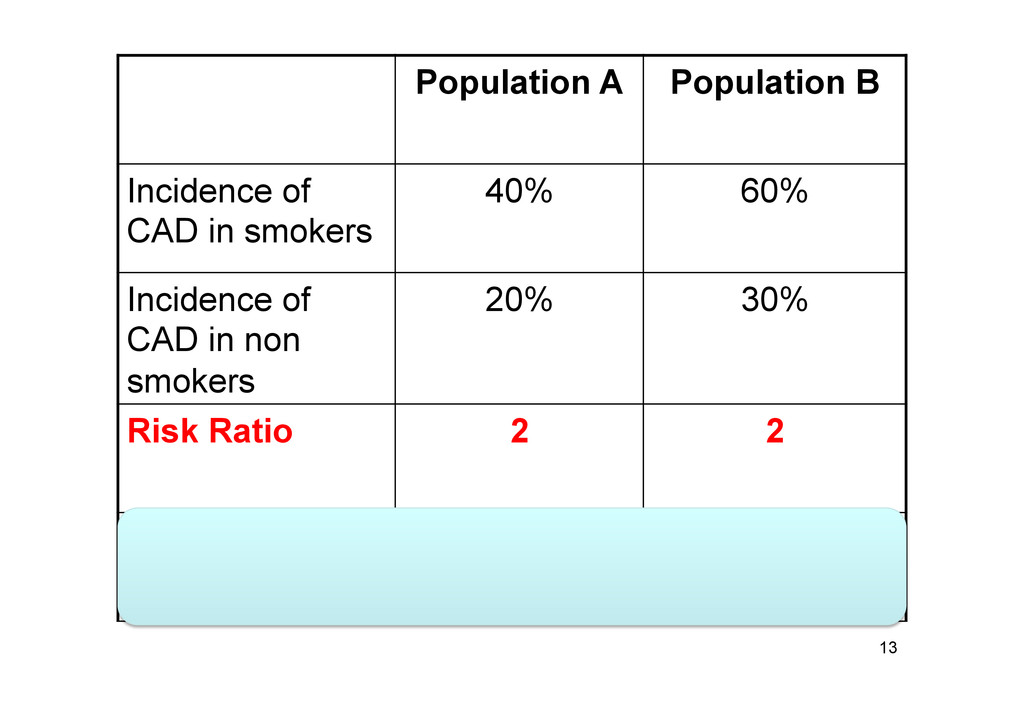
B: – Risk of developing disease: 10% • Difference in risk: what is the absolute excess risk present in Group B? – 10% - 5% = 5 percent points • Ratio: how many times larger is the risk in Group B? – 10%/5% = 2 11
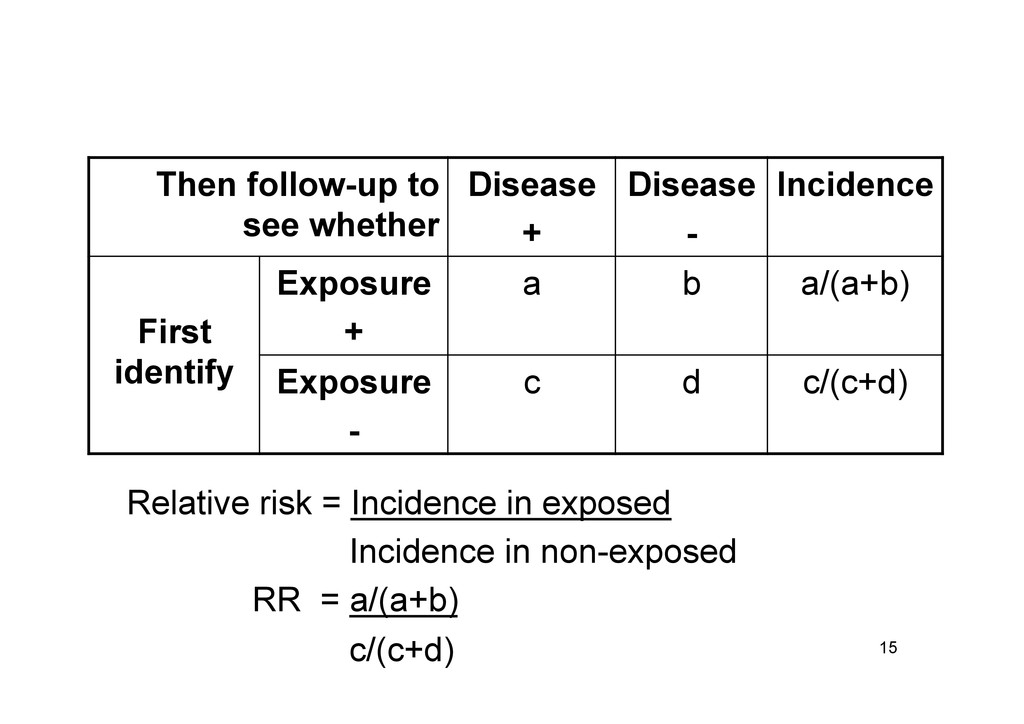
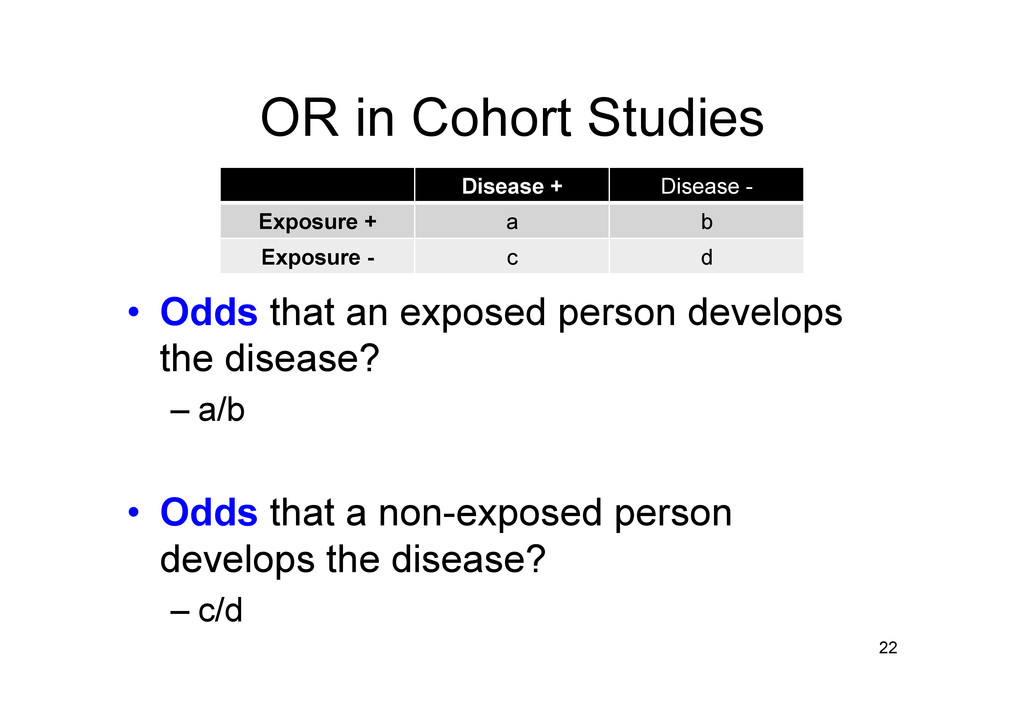
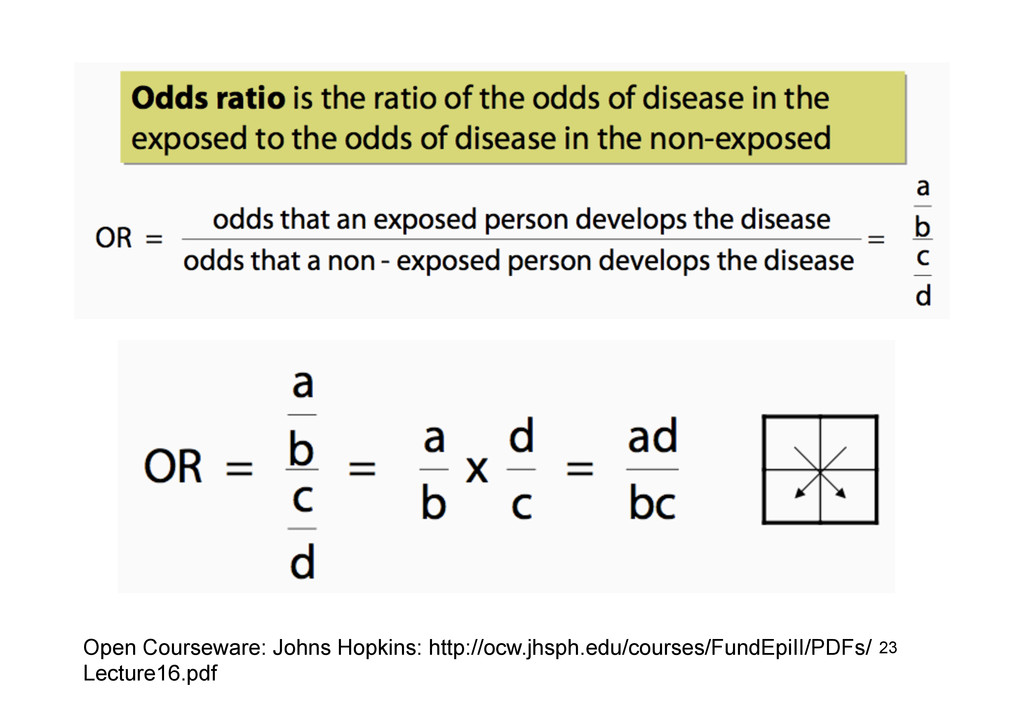
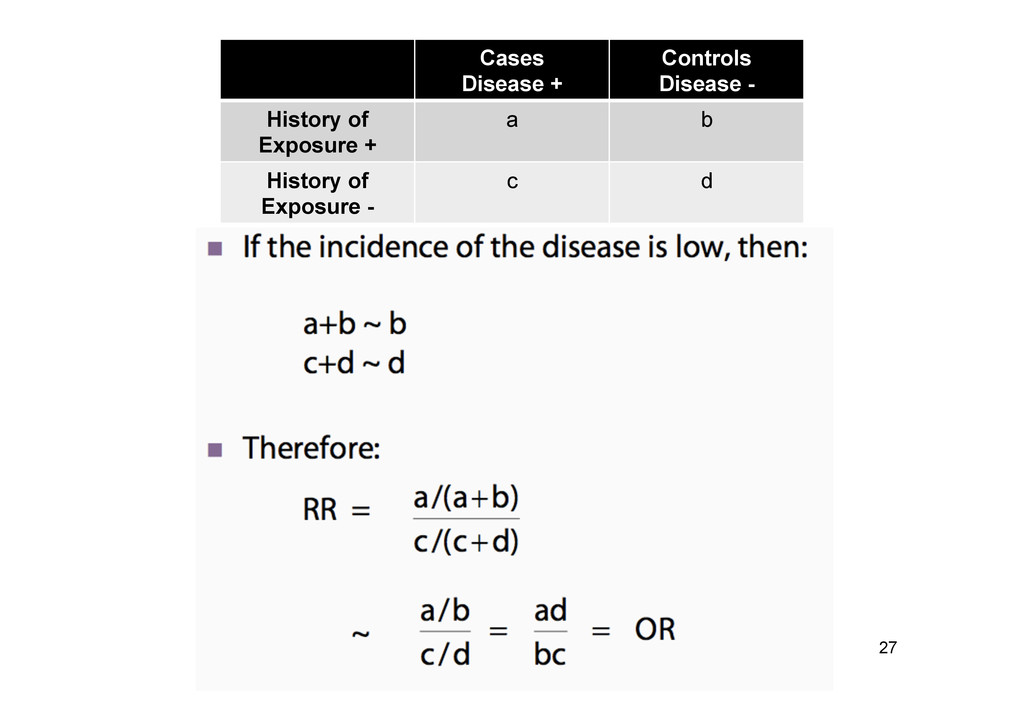
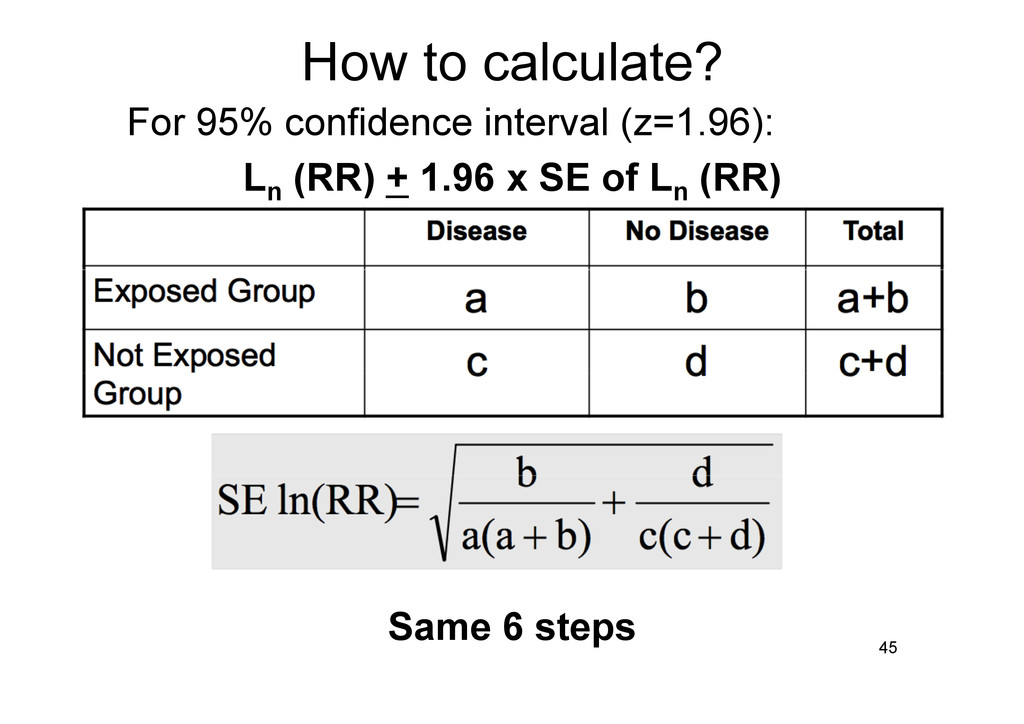
Disease - History of Exposure + a b History of Exposure - c d Open Courseware: Johns Hopkins: http://ocw.jhsph.edu/courses/FundEpiII/PDFs/ Lecture16.pdf
x (Lung CA – Smoking -) (Lung CA+ Smoking -) x (Lung CA – Smoking +) Cases (Lung CA) Disease + Controls (Lung CA) Disease - Exposure (Smoking) + a b Exposure (Smoking) - c d
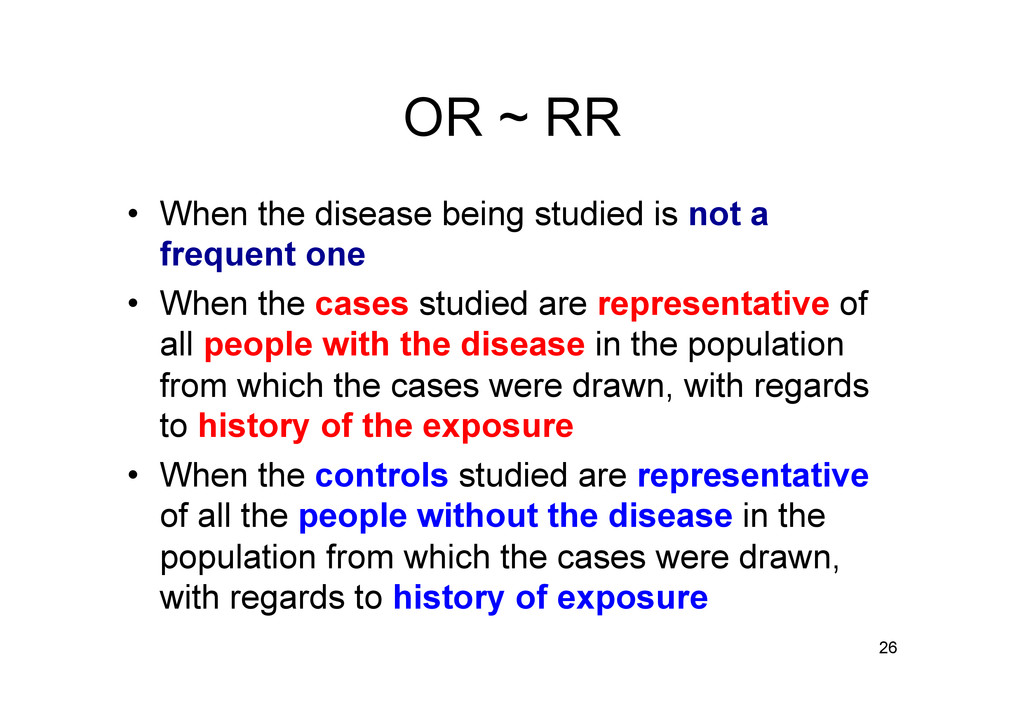
not a frequent one • When the cases studied are representative of all people with the disease in the population from which the cases were drawn, with regards to history of the exposure • When the controls studied are representative of all the people without the disease in the population from which the cases were drawn, with regards to history of exposure 26
Disease prevalence <10% • May not always hold true! 28 Cornfield J. A method of estimating comparative rates from clinical data. J Natl Cancer Inst 1951;11:1269–75.
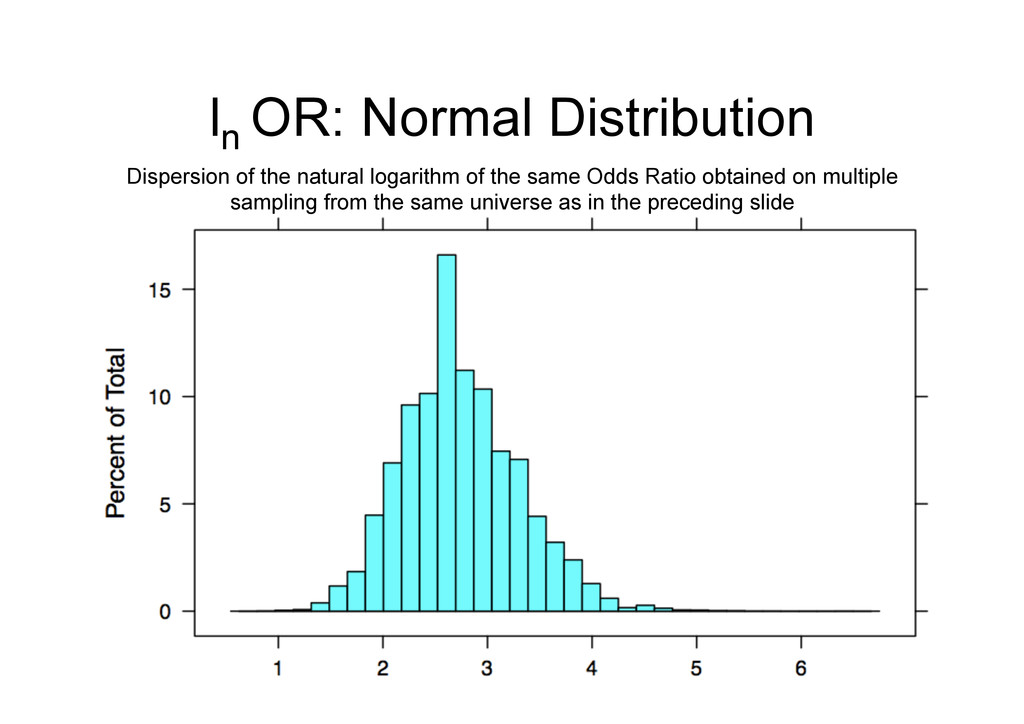
inherent in results derived from data that is in itself a randomly selected subset of a population? – 100 samples from same population: 95 times their CI contains the true mean value! 32
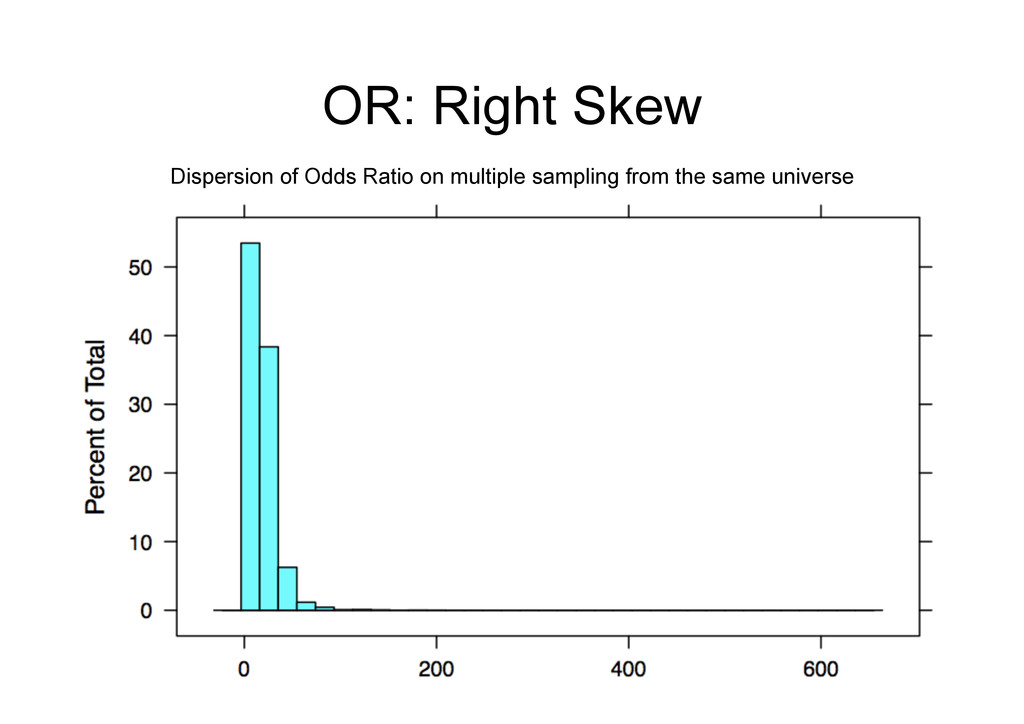
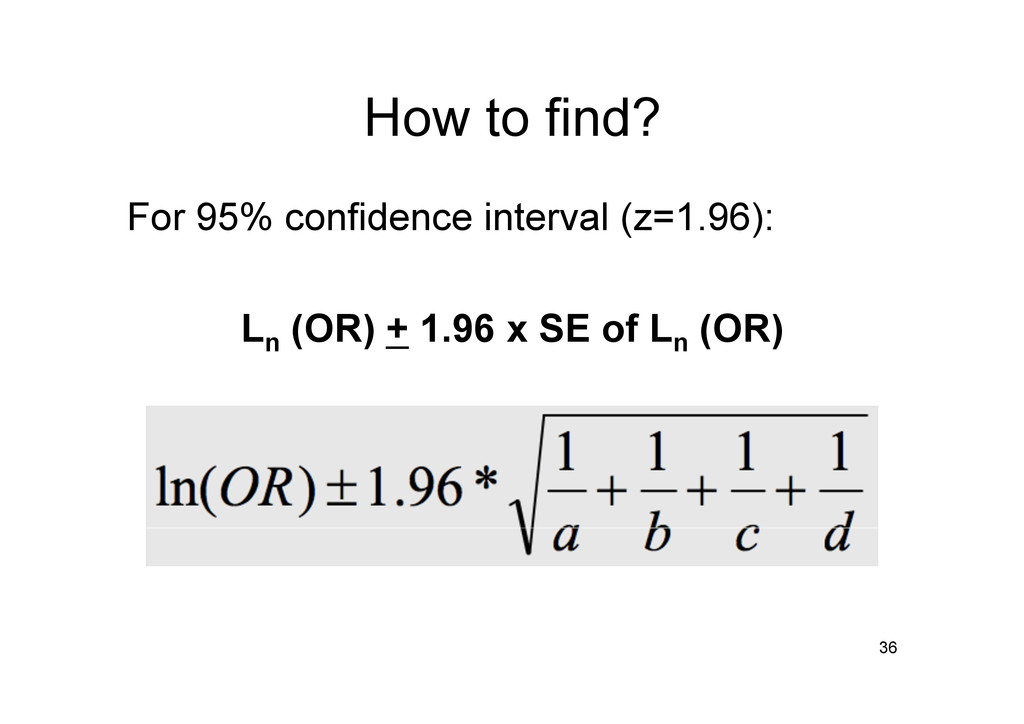
+ Confidence coefficient x standard error • However, for odds ratio, CI is calculated on the natural log scale. Then reversed on the exponential scale… WHY? 33
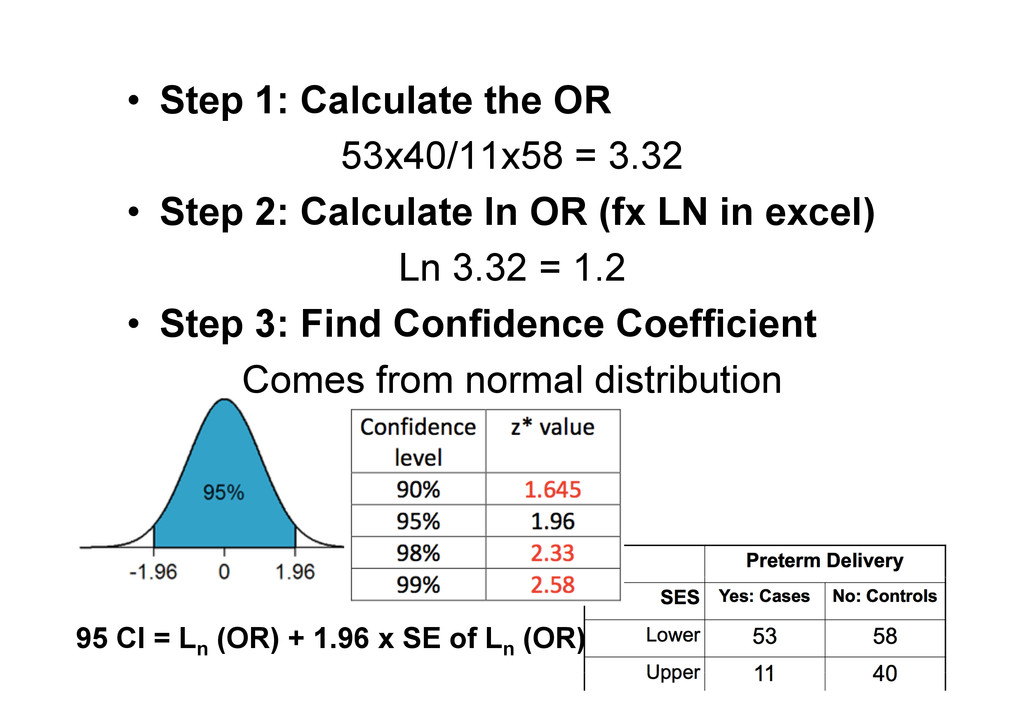
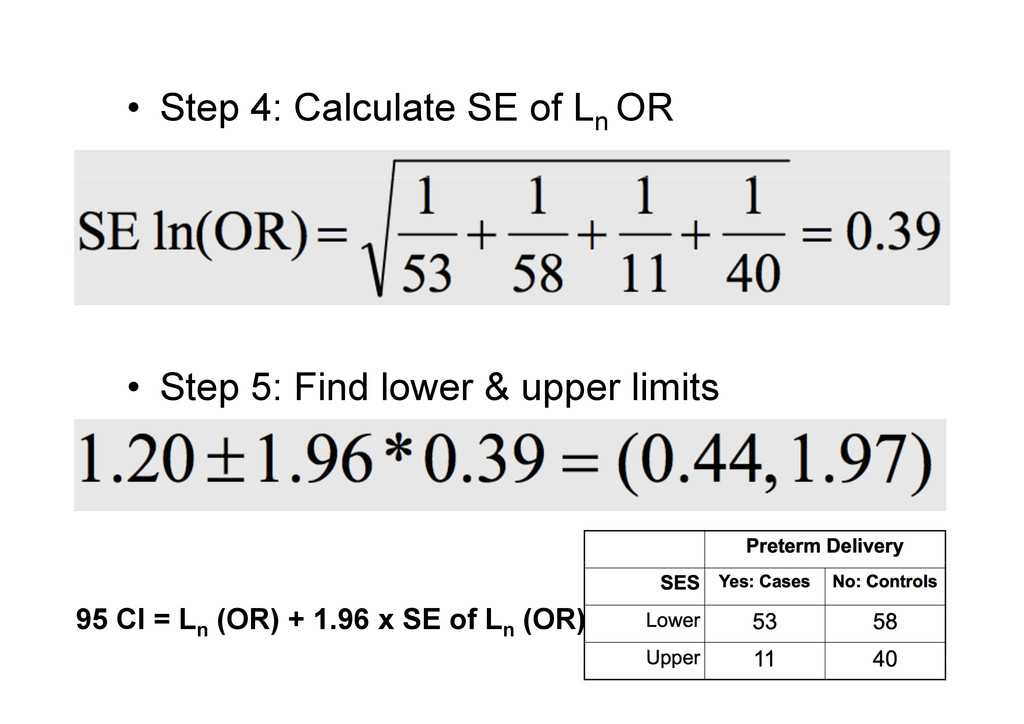
Step 2: Calculate ln OR (fx LN in excel) Ln 3.32 = 1.2 • Step 3: Find Confidence Coefficient Comes from normal distribution 38 95 CI = Ln (OR) + 1.96 x SE of Ln (OR)
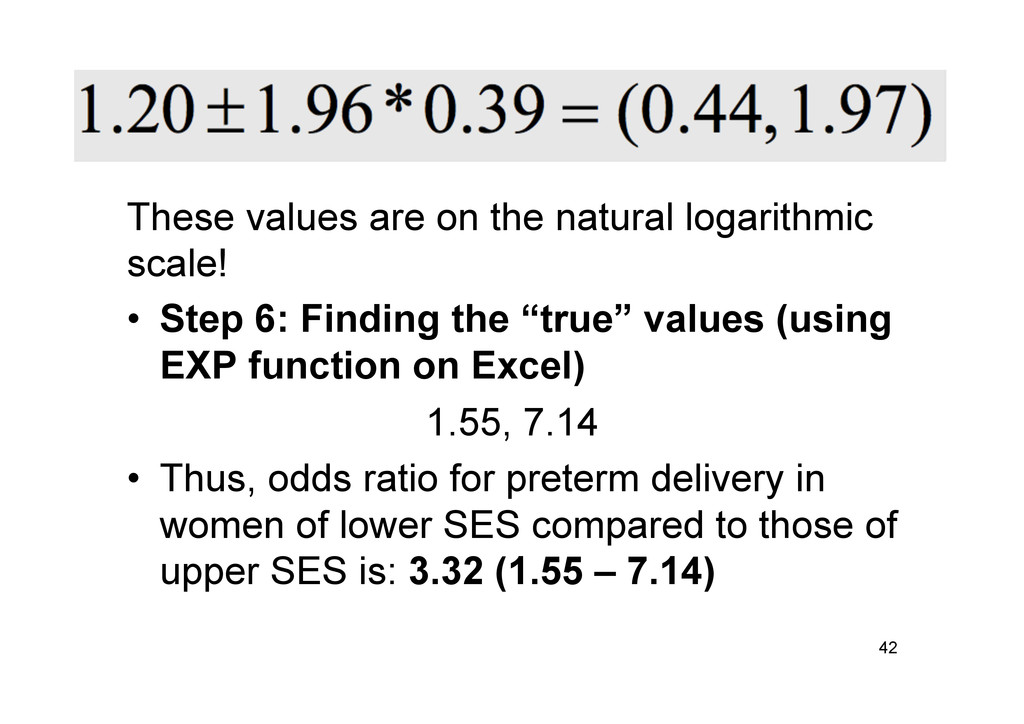
6: Finding the “true” values (using EXP function on Excel) 1.55, 7.14 • Thus, odds ratio for preterm delivery in women of lower SES compared to those of upper SES is: 3.32 (1.55 – 7.14) 42
Confidence coefficient x standard error • Also calculated on the natural logarithmic scale for the same reasons • Only difference: calculating the standard error 44
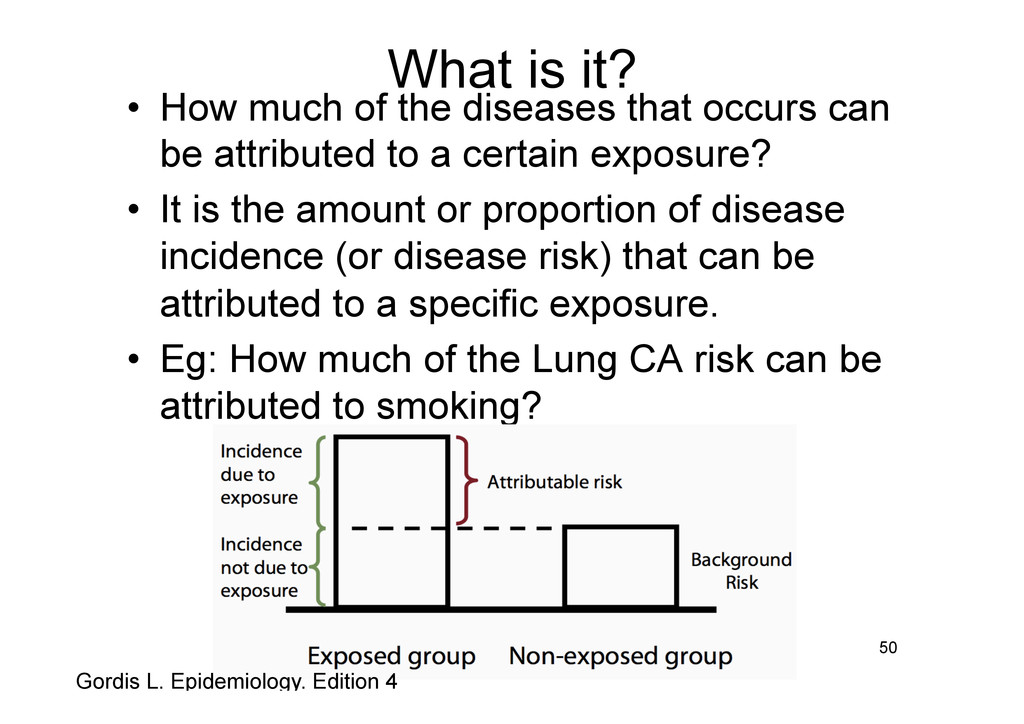
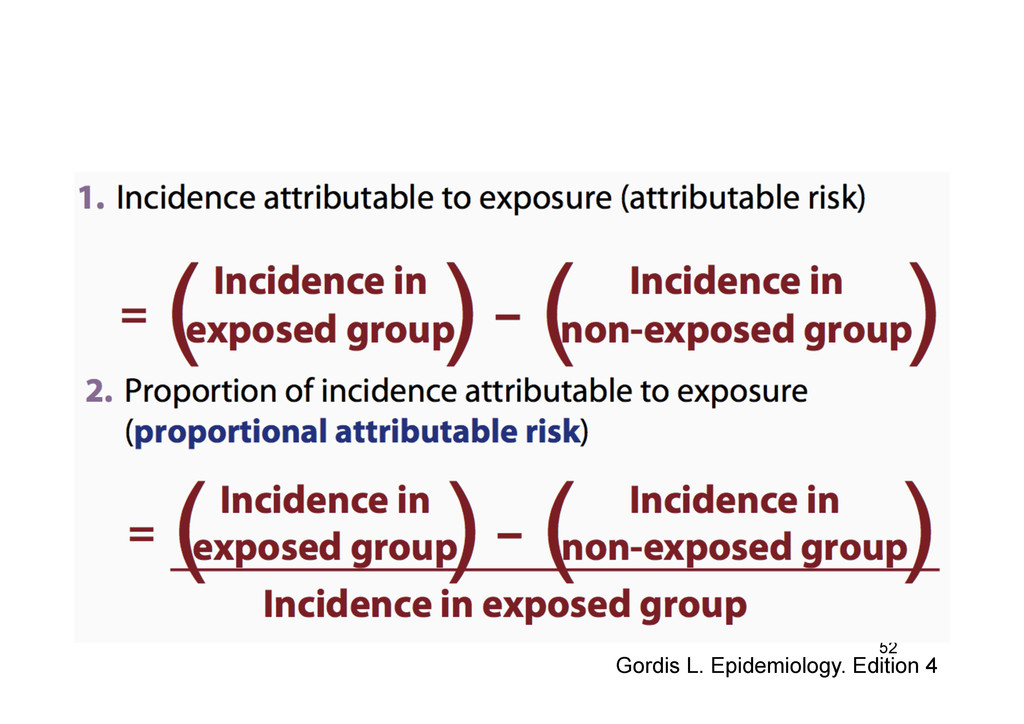
occurs can be attributed to a certain exposure? • It is the amount or proportion of disease incidence (or disease risk) that can be attributed to a specific exposure. • Eg: How much of the Lung CA risk can be attributed to smoking? 50 Gordis L. Epidemiology. Edition 4
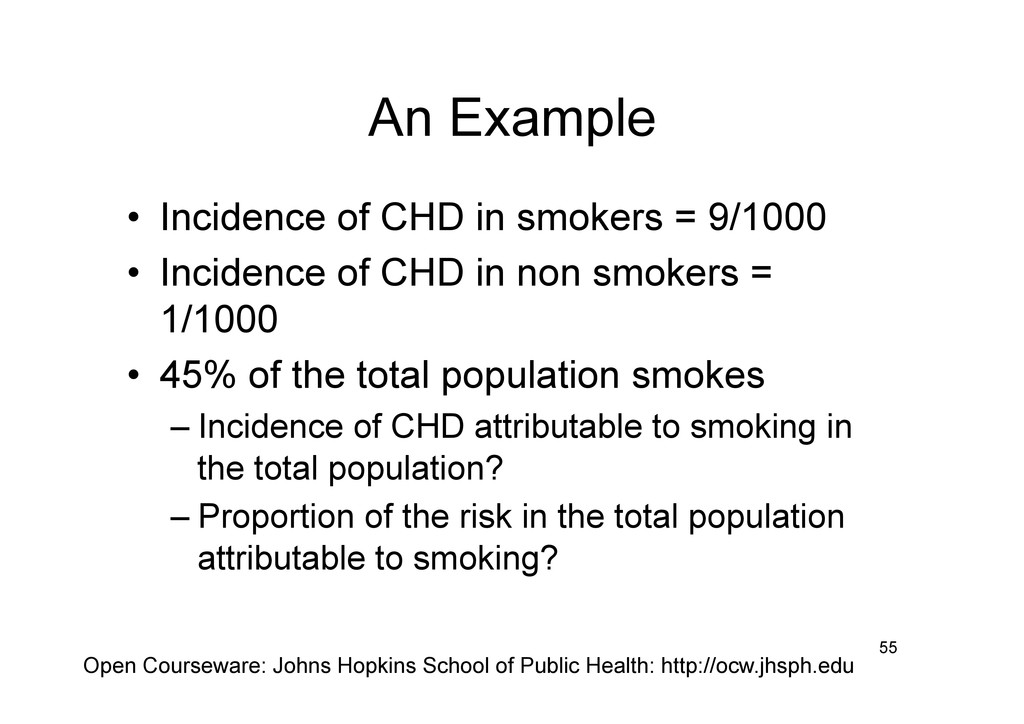
• Incidence of CHD in non smokers = 1/1000 • 45% of the total population smokes – Incidence of CHD attributable to smoking in the total population? – Proportion of the risk in the total population attributable to smoking? 55 Open Courseware: Johns Hopkins School of Public Health: http://ocw.jhsph.edu
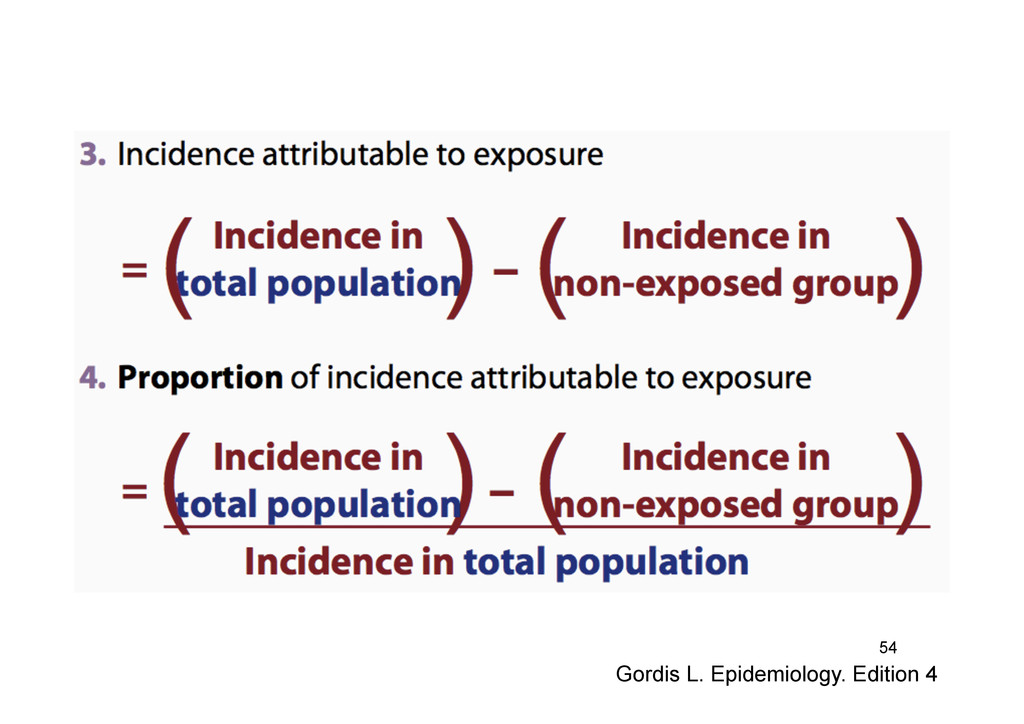
to exposure in total population (Incidence in total population – Incidence in non smokers) / Incidence in total population = (4.6 – 1) / 4.6 x 100 = 78.26% • Interpretation? 58
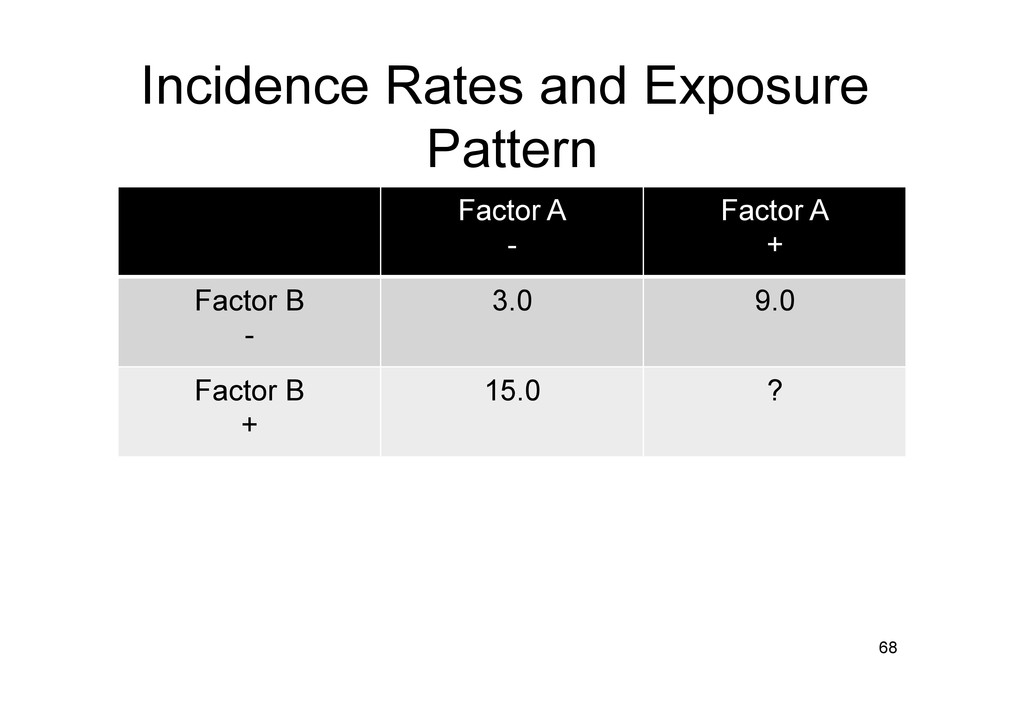
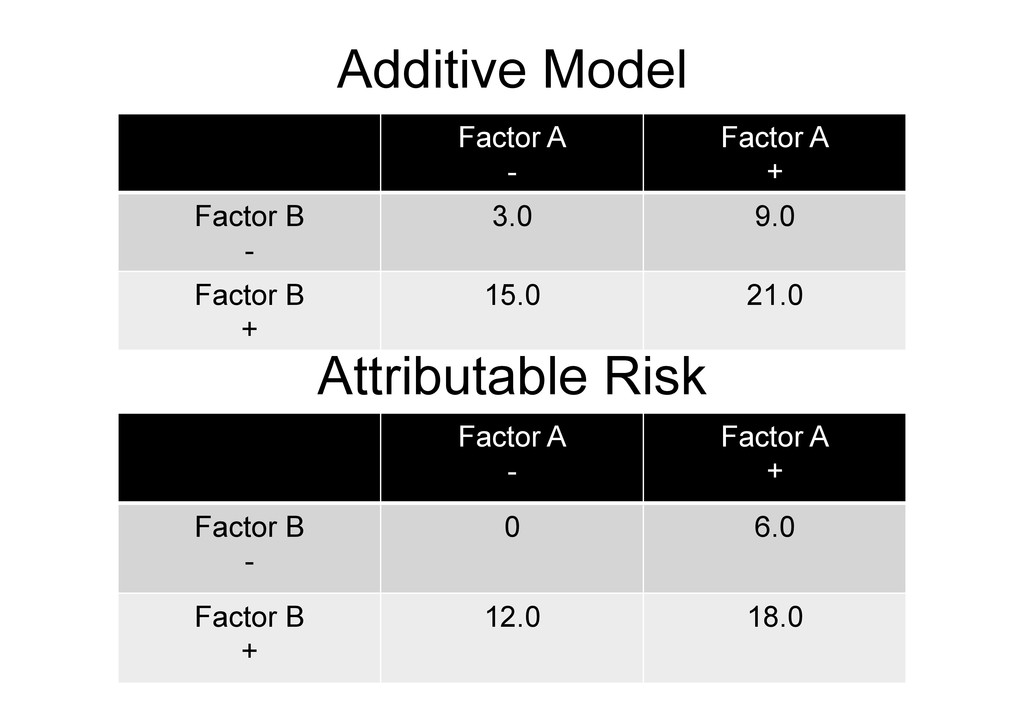
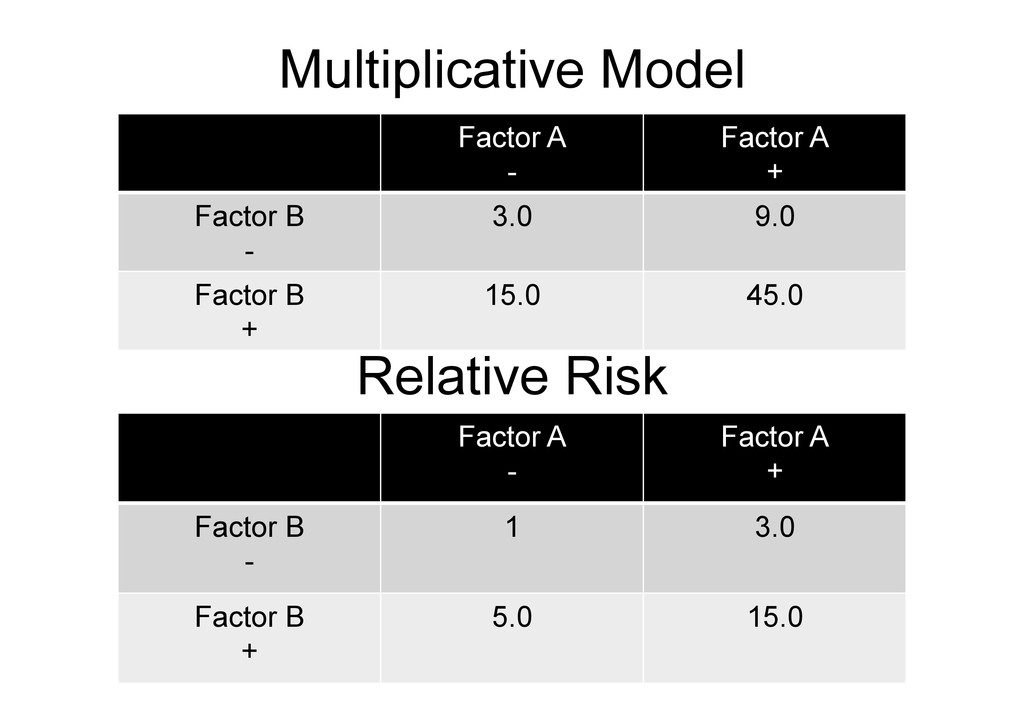
the presence of two or more risk factors differs from the incidence rate expected to result from their individual effects – Positive interaction or Synergism – Negative interaction or Antagonism 67
is present • Which one? – Biological plausibility – Statistical consideration – Model valid and replicable • Difficult to decide – maybe open to interpretation/criticism 71
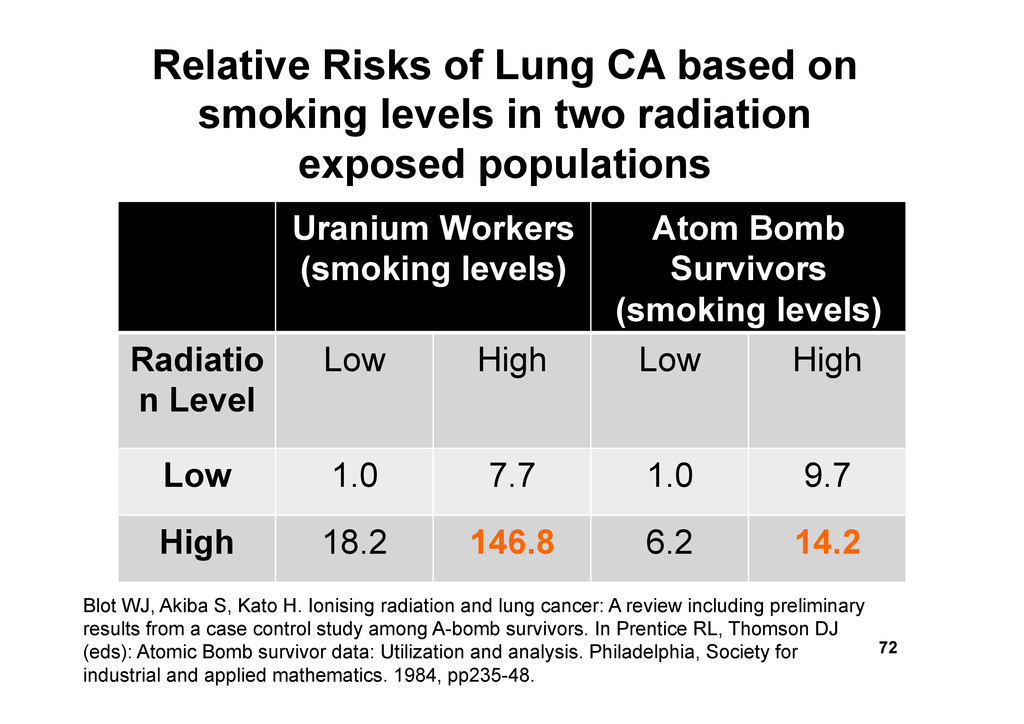
n Level Low High Low High Low 1.0 7.7 1.0 9.7 High 18.2 146.8 6.2 14.2 72 Relative Risks of Lung CA based on smoking levels in two radiation exposed populations Blot WJ, Akiba S, Kato H. Ionising radiation and lung cancer: A review including preliminary results from a case control study among A-bomb survivors. In Prentice RL, Thomson DJ (eds): Atomic Bomb survivor data: Utilization and analysis. Philadelphia, Society for industrial and applied mathematics. 1984, pp235-48.
– CI and SE – Coefficient of variance • Woolf’s method uses coefficient of variance 74 London School of Hygiene and Tropical Medicine: http://conflict.lshtm.ac.uk/page_45.htm
value, then the odds ratio becomes zero for that strata • And log (0) is undefined • Invalidates the stratification • However: – Easy to understand – Small number of strata – Large sample size in each strata 75
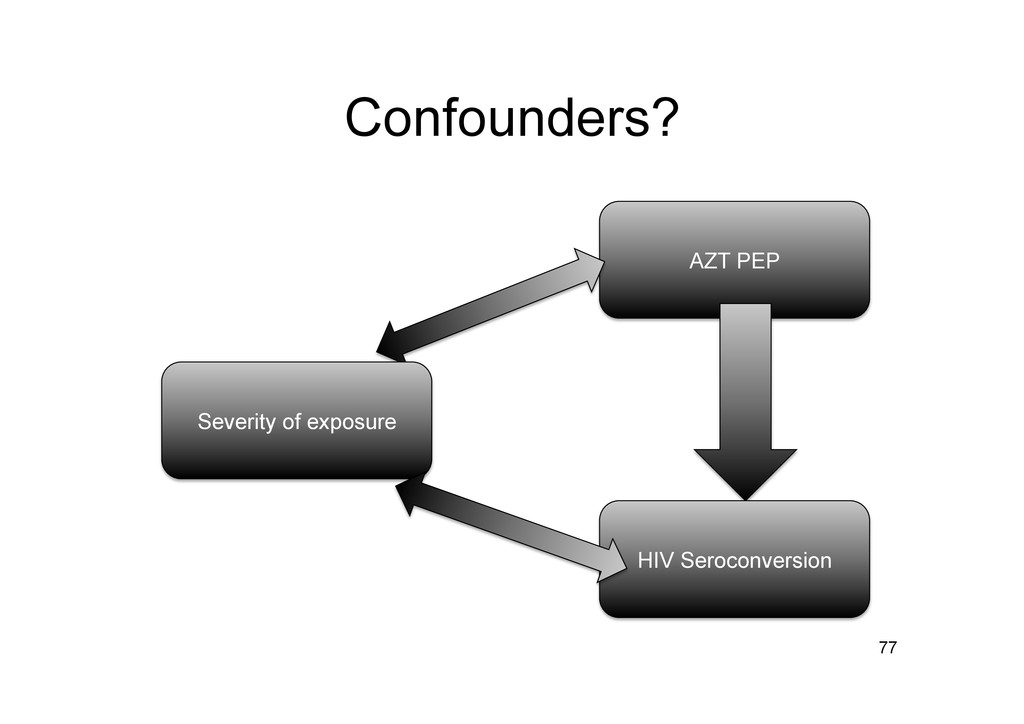
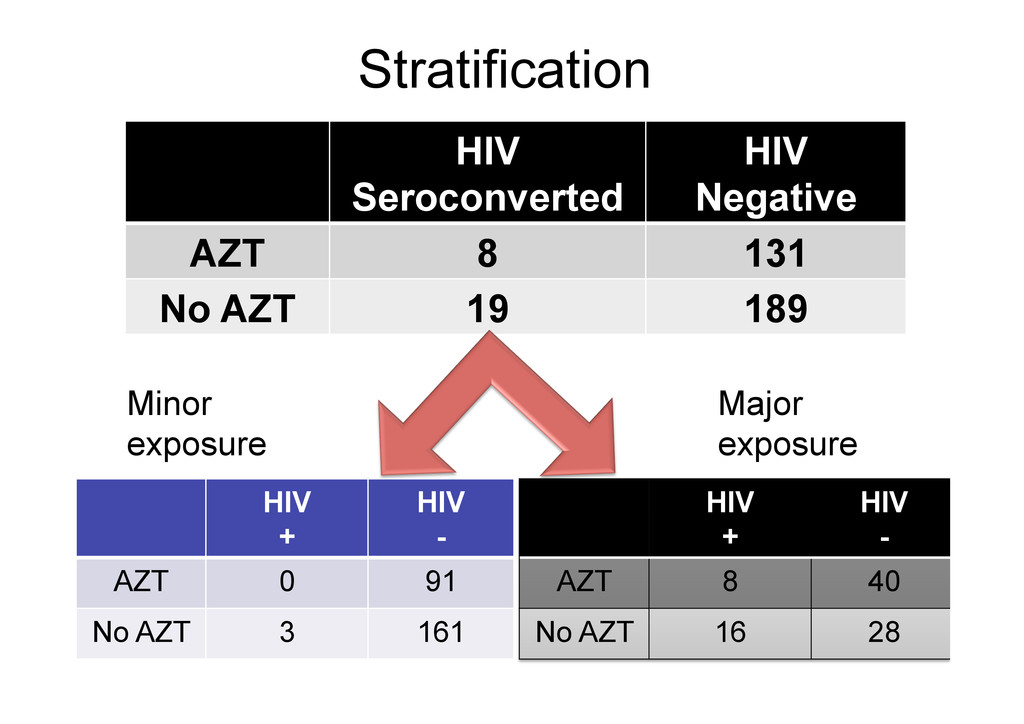
131 No AZT 19 189 76 Li, R. W., & Wong, J. B. (1997). Postexposure treatment of HIV. N Engl J Med, 337(7), 499-500; author reply 501. ORcrude =0.61 95% CI = 0.26 – 1.4
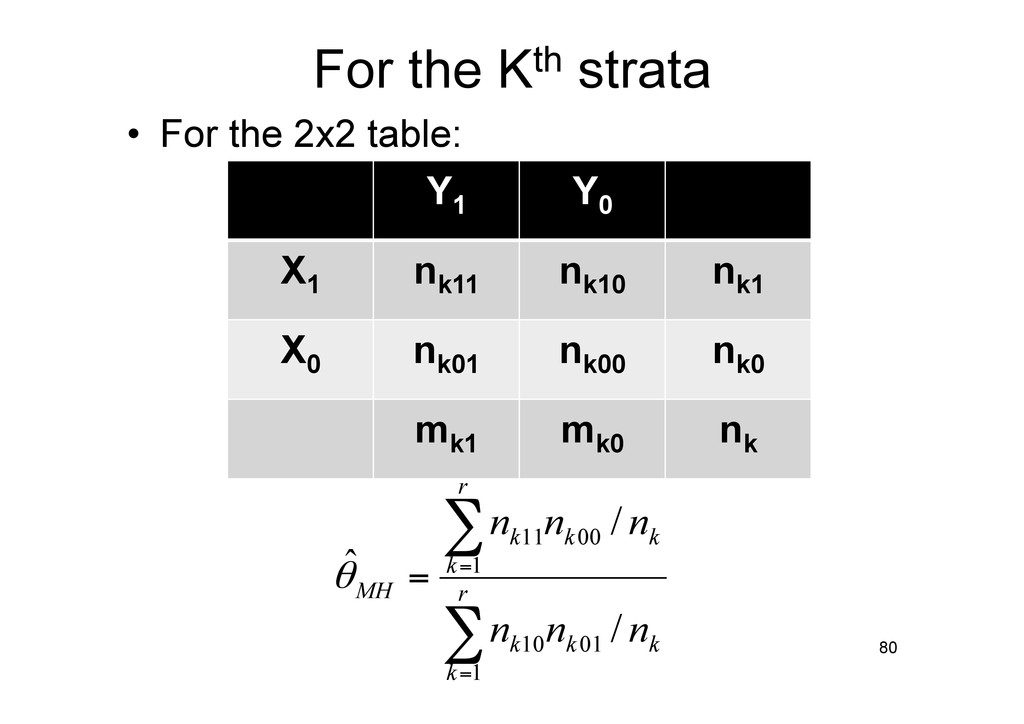
1959 • Weighted mean of the odds ratio of the individual strata. (hence “common”) 79 Mantel, N.; Haenszel, W. (1959), "Statistical aspects of the analysis of data from the retrospective analysis of disease", Journal of the National Cancer Institute 22 (4): 719–748, PMID 13655060
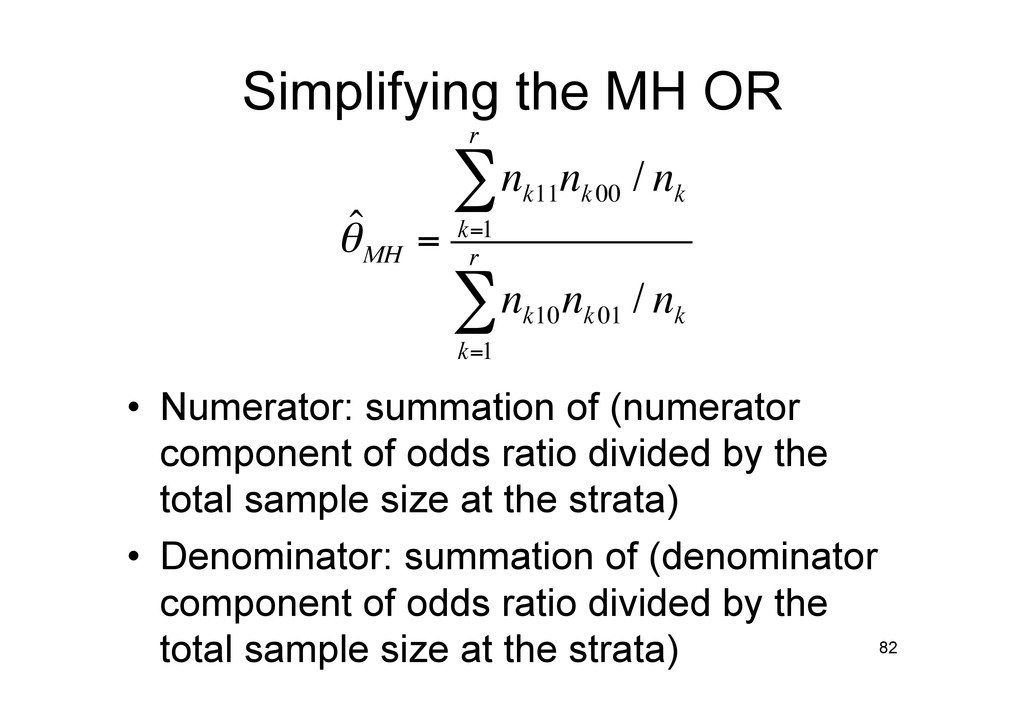
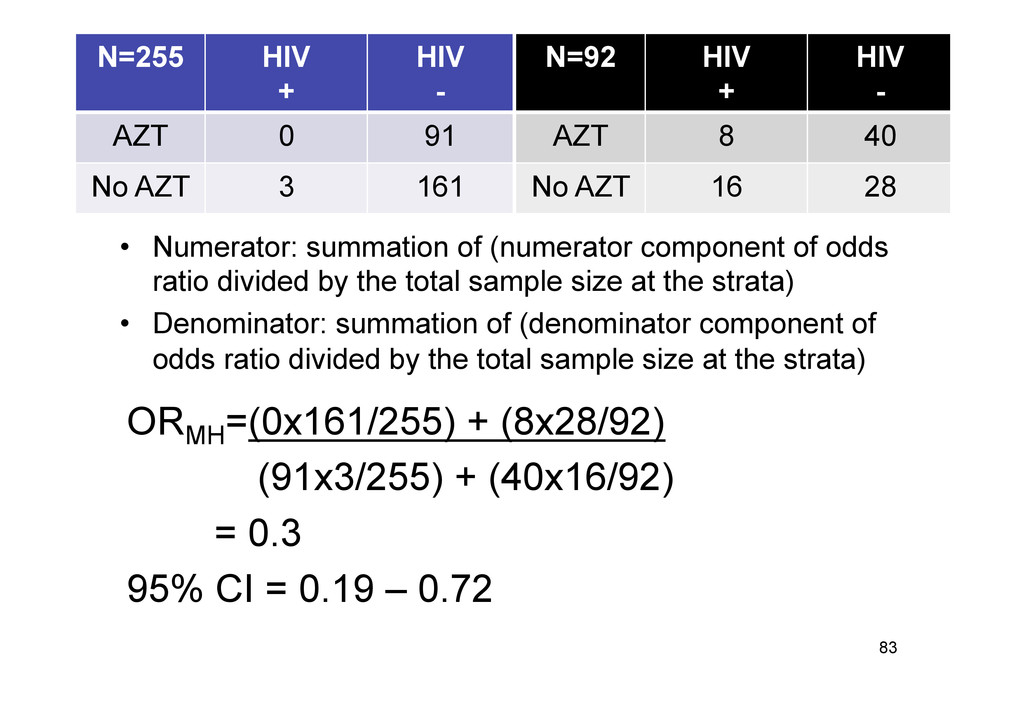
of odds ratio divided by the total sample size at the strata) • Denominator: summation of (denominator component of odds ratio divided by the total sample size at the strata) 82 ˆ θMH = n k11 n k00 / n k k=1 r ∑ n k10 n k01 / n k k=1 r ∑
CI = 0.19 – 0.72 83 N=255 HIV + HIV - AZT 0 91 No AZT 3 161 N=92 HIV + HIV - AZT 8 40 No AZT 16 28 • Numerator: summation of (numerator component of odds ratio divided by the total sample size at the strata) • Denominator: summation of (denominator component of odds ratio divided by the total sample size at the strata)
to “visualize” • Clinical use of OR limited • Misreporting of OR in published papers • OR: A Ratio of Ratios! • The RR = OR conundrum 86 Holcomb WL Jr, Chaiworapongsa T, Luke DA, Burgdorf KD. An odd measure of risk: use and misuse of the odds ratio. Obstet Gynecol 2001;98:685–8. Katz KA. The (relative) risks of using odds ratios. Arch Dermatol 2006;142: 761–4.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}