Entrepreneur in Residence (EiR) for AHIP’s Innovation Lab • Chairman of the Board of Netspective Communications, Publisher at Netspective Media and serial entrepreneur. • Angel investor, board member, in several digital health and Internet startups. • 25 years of software engineering and multi-site healthcare system deployment experience in Fortune 50 and public sector (Fed 100 winner). • 15 years of healthcare IT and medical devices experience (blog at http://healthcareguy.com) • 15 years of technology management experience (government, non-profit, commercial) Engineer, strategist, entrepreneur, investor, author, and journalist
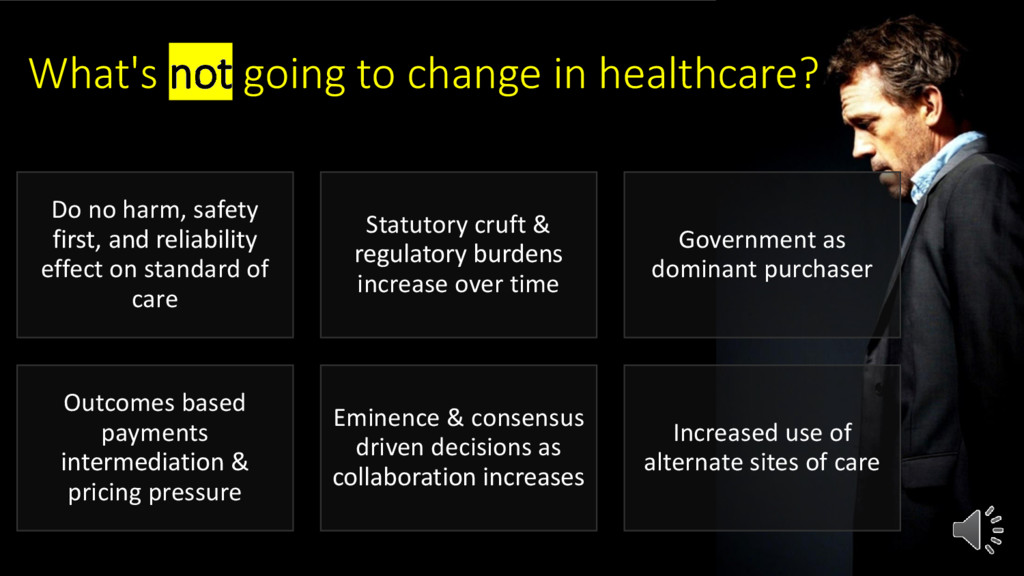
safety first, and reliability effect on standard of care Statutory cruft & regulatory burdens increase over time Government as dominant purchaser Outcomes based payments intermediation & pricing pressure Eminence & consensus driven decisions as collaboration increases Increased use of alternate sites of care
of healthcare” “we need to disrupt healthcare” “how would elimination of co-pays increase utilization?” “how can improving provider affinity increase member satisfaction?” “we need to buy more digital health tools” “how can we pay non-clinicians to handle more patient-facing tasks?”
consumer engagement Which one is driving demand for innovation versus responding to existing supply? Each member population requires different engagement techniques at various times. But is engagement with plan more important than intermediated engagement with provider? Picking the wrong channel creates confusion and reduces engagement. But, how important is all this compared to provider affinity associated with choices members make?
spend 55 minutes thinking about the problem and 5 minutes thinking about solutions.” “Stay away from negative people. They have a problem for every solution.” Albert Einstein
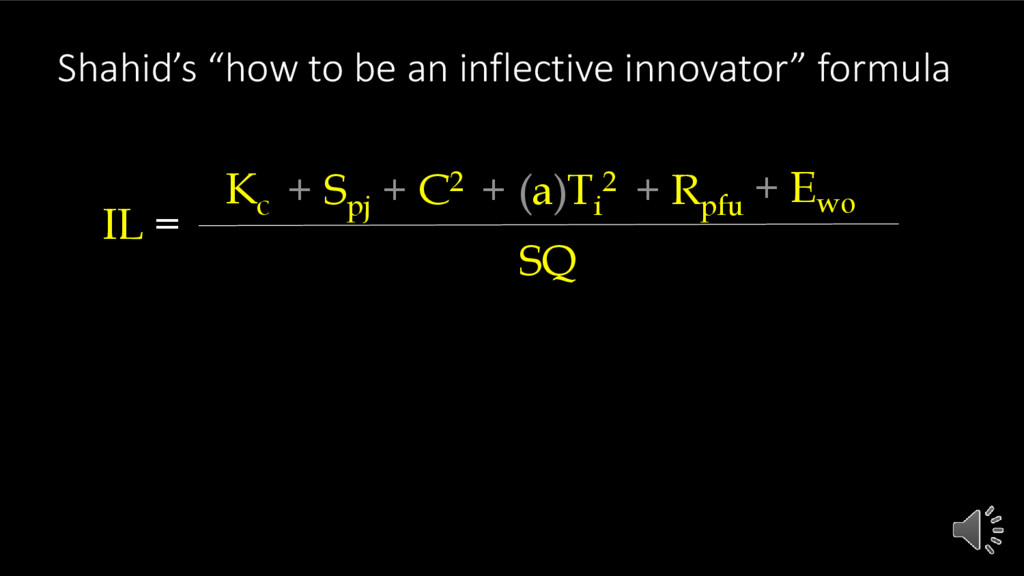
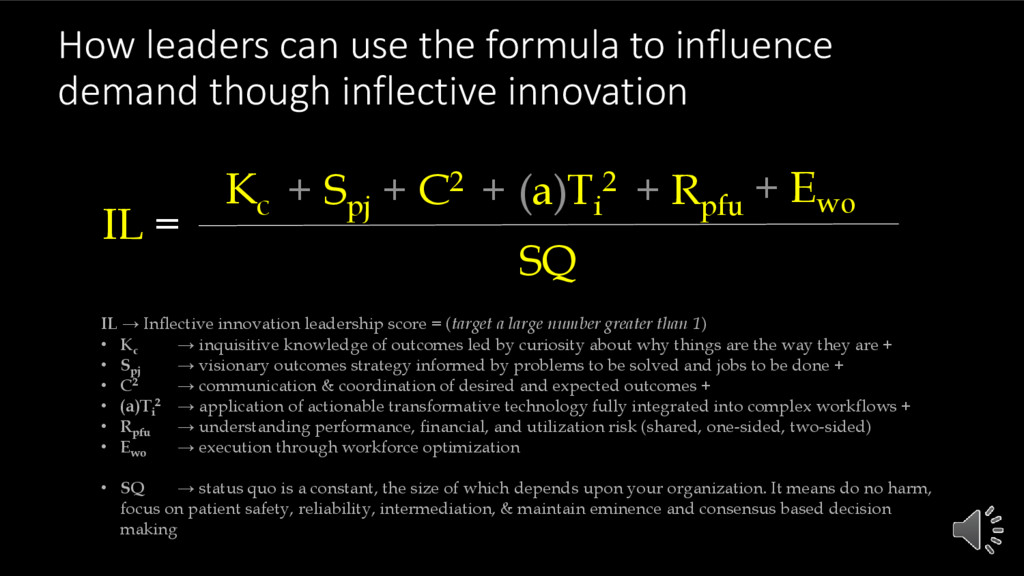
inflective innovation IL → Inflective innovation leadership score = (target a large number greater than 1) • Kc → inquisitive knowledge of outcomes led by curiosity about why things are the way they are + • Spj → visionary outcomes strategy informed by problems to be solved and jobs to be done + • C2 → communication & coordination of desired and expected outcomes + • (a)Ti 2 → application of actionable transformative technology fully integrated into complex workflows + • Rpfu → understanding performance, financial, and utilization risk (shared, one-sided, two-sided) • Ewo → execution through workforce optimization • SQ → status quo is a constant, the size of which depends upon your organization. It means do no harm, focus on patient safety, reliability, intermediation, & maintain eminence and consensus based decision making IL = SQ Kc + Spj + C2 + (a)Ti 2 + Rpfu + Ewo
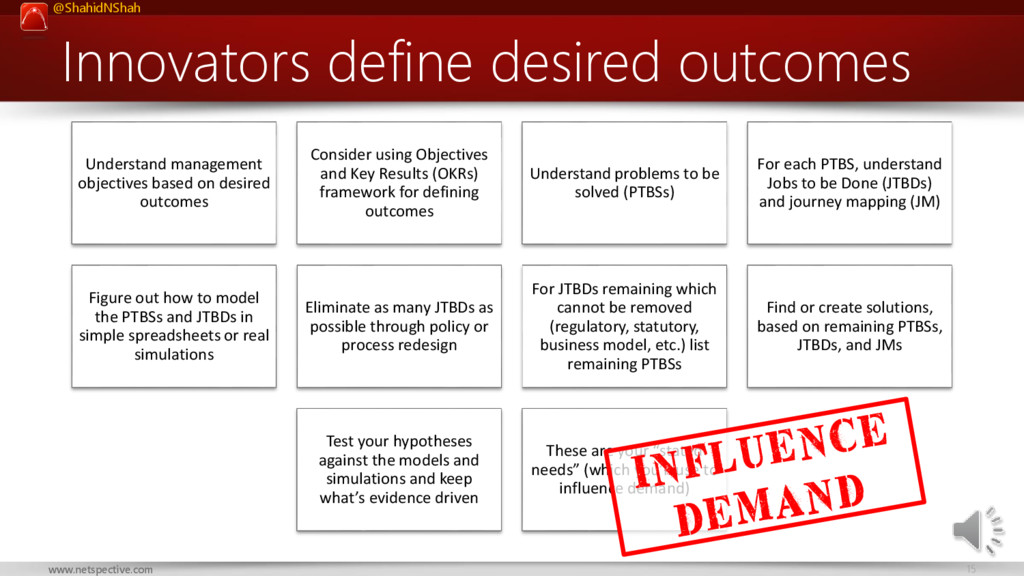
based on desired outcomes Consider using Objectives and Key Results (OKRs) framework for defining outcomes Understand problems to be solved (PTBSs) For each PTBS, understand Jobs to be Done (JTBDs) and journey mapping (JM) Figure out how to model the PTBSs and JTBDs in simple spreadsheets or real simulations Eliminate as many JTBDs as possible through policy or process redesign For JTBDs remaining which cannot be removed (regulatory, statutory, business model, etc.) list remaining PTBSs Find or create solutions, based on remaining PTBSs, JTBDs, and JMs Test your hypotheses against the models and simulations and keep what’s evidence driven These are your “stated needs” (which you’ll use to influence demand)
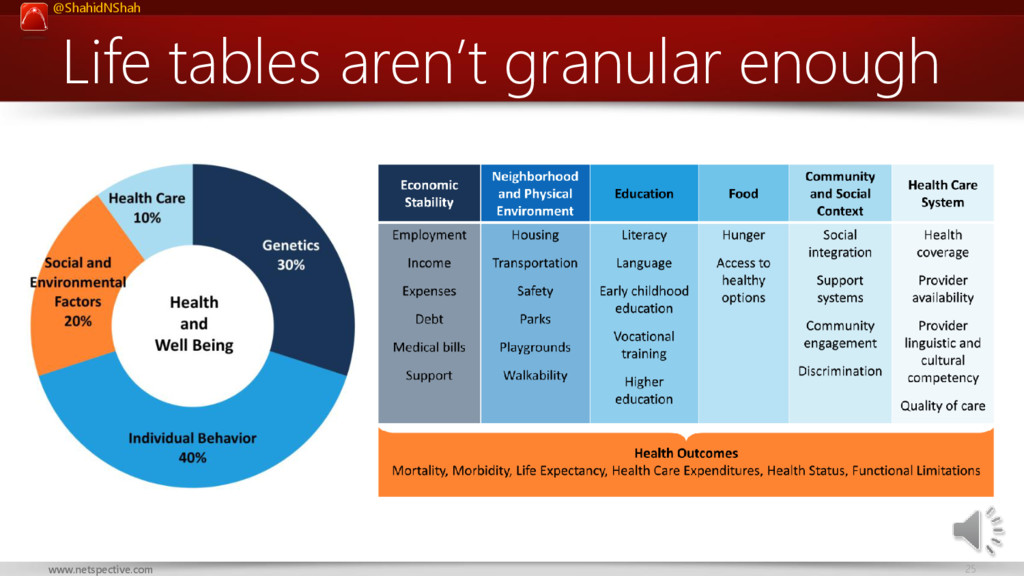
Factors Physical Environment 30% 20% 40% 10% Access to Care Quality of Care Education Employment Income Family/Social Support Community Safety Air & Water Quality Housing & Transit Source: RWJF/UWPHI. Genetics Diet & Exercise Tobacco Use Alcohol & Drug Use Sexual Activity Sleep Inflective innovation outcomes drivers
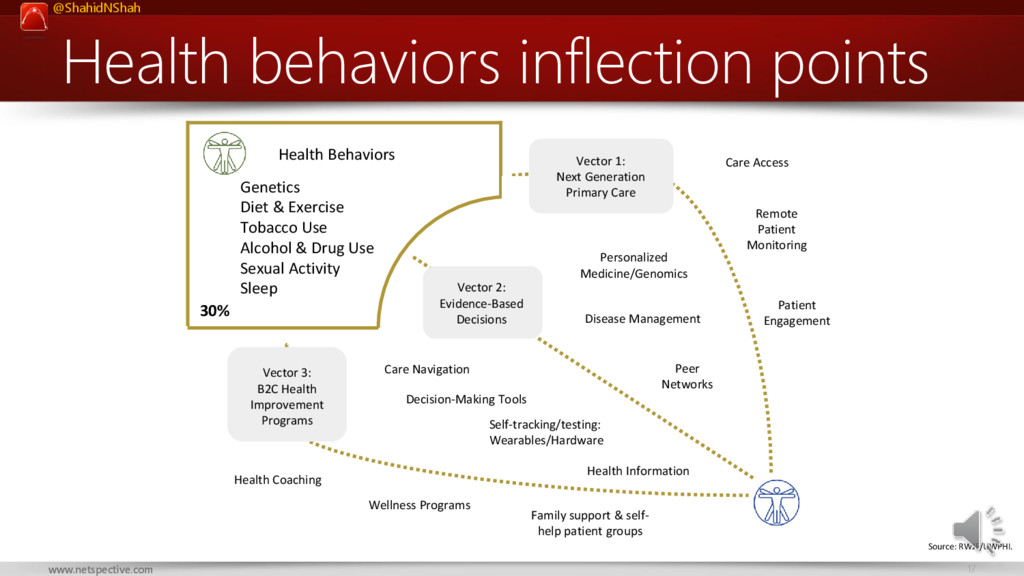
Health Improvement Programs Vector 1: Next Generation Primary Care Self-tracking/testing: Wearables/Hardware Personalized Medicine/Genomics Health Information Care Navigation Disease Management Peer Networks Health Coaching Decision-Making Tools Care Access Remote Patient Monitoring Patient Engagement Health Behaviors 30% Wellness Programs Source: RWJF/UWPHI. Genetics Diet & Exercise Tobacco Use Alcohol & Drug Use Sexual Activity Sleep Family support & self- help patient groups Health behaviors inflection points
Vector 2: Next Generation Primary Care Vector 3: Value-Based Care Vector 4: Operational Efficiency Vector 1: Disease-Specific Care Pathways Care Coordination Patient Engagement Big Data Personalized Medicine Medication Management Clinical Care 20% Access to Care Quality of Care Nanotechnology Source: RWJF/UWPHI. Knowledge Sharing Clinical care inflection points Practice Management, EMRs, Pharmacy Management Transparency Tech-enabled services Retail Clinics, DPC House Calls
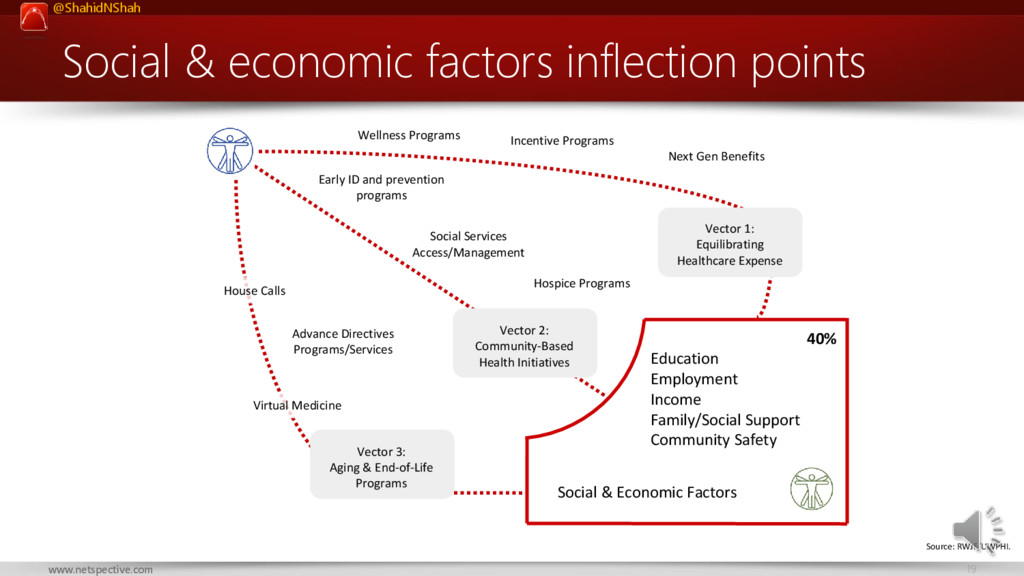
Services Access/Management Vector 1: Equilibrating Healthcare Expense Vector 2: Community-Based Health Initiatives Vector 3: Aging & End-of-Life Programs Social & Economic Factors 40% Education Employment Income Family/Social Support Community Safety House Calls Hospice Programs Virtual Medicine Incentive Programs Wellness Programs Source: RWJF/UWPHI. Early ID and prevention programs Social & economic factors inflection points
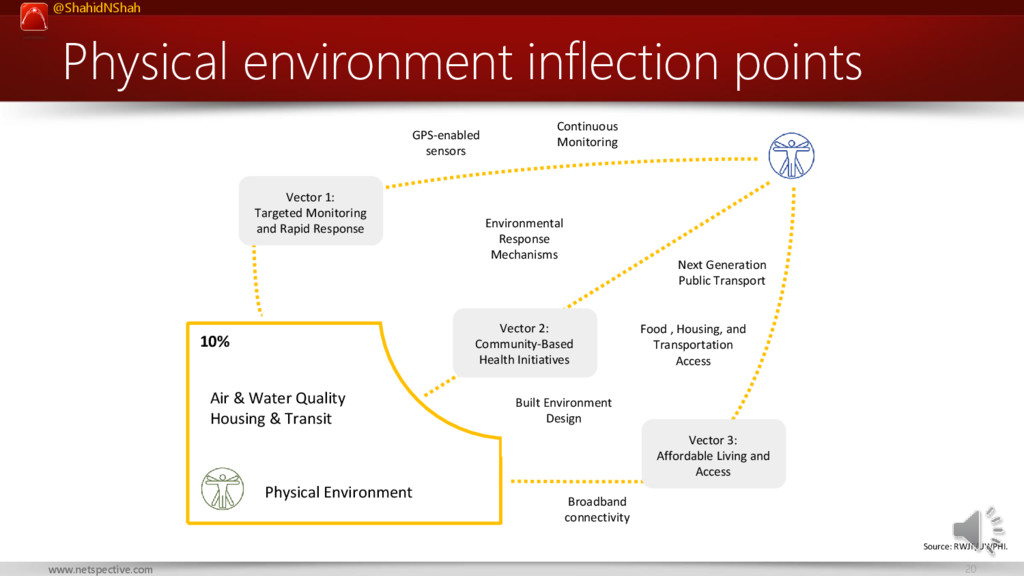
Water Quality Housing & Transit Vector 1: Targeted Monitoring and Rapid Response Vector 2: Community-Based Health Initiatives Vector 3: Affordable Living and Access Food , Housing, and Transportation Access Next Generation Public Transport Environmental Response Mechanisms Continuous Monitoring Source: RWJF/UWPHI. Built Environment Design Broadband connectivity Physical environment inflection points
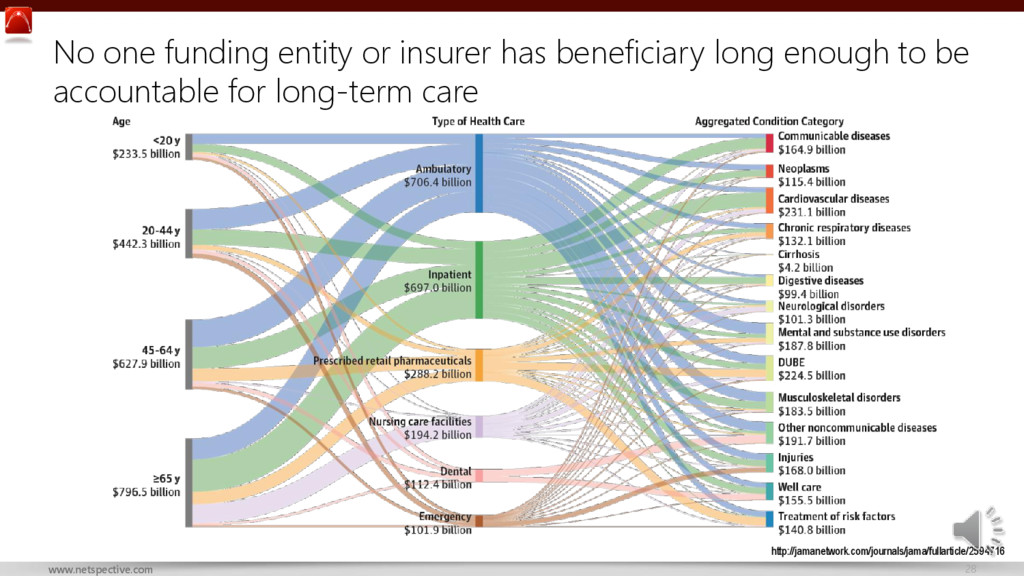
real costs for more modern life tables? How do we increase transparency of costs across the supply chain? How do we combat information asymmetry? How can we be accountable for long-term care when beneficiaries move freely between insurers? How do we take long term risks in a low interest rates environment which has reduced investment income?
strategic partners in their own well being? How do we encourage members to take more responsibility for care without increasing out of pocket expenses? How can we empower employers to engage more with their employees’ health? How do we empower providers without getting in the way of care? How do we increase collaboration across narrow networks and treat providers as partners not suppliers?
behavioral economics to increase affinity with care providers? How do we define performance outcomes in value driven care contracts? How do we manage pharmacy costs without global negotiated rates? How do we catch fraud, waste, and abuse in real-time vs. retrospectively? How do we get more participants in the health ecosystem to take on more risk?
not incentivized to change long term behaviors (new incoming administration indicates decentralization from Federal to State, potentially impacting incentives)
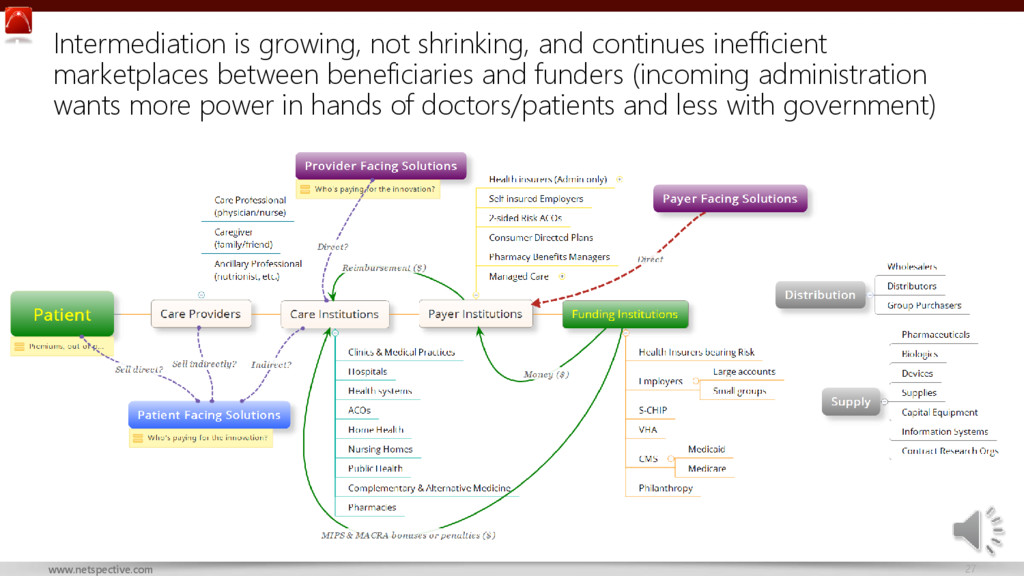
shrinking, and continues inefficient marketplaces between beneficiaries and funders (incoming administration wants more power in hands of doctors/patients and less with government)
about That the repeal of the Affordable Care Act (ACA) will be disruptive Why it’s hard to deliver Adapting to the ACA’s healthcare reform agenda (which is not likely to change) while continuing to focus on internal priorities of demand generation and cost containment
talk about ACA repeal or replacement is going to affect new patients entrants into the insurance market Why it’s hard to deliver Attracting the right kinds of ‘profitable’ patients in a rapidly changing and complex market will be difficult; when cost is more transparent and easier to compare, smarter buyers will force changes faster than payers can accommodate
about Aging populations and demographic changes are expanding the insurance market Why it’s hard to deliver It’s unclear where money for the new entrants in the market will come from so new products need to be created more rapidly and with more market data than ever before
talk about Cost containment is necessary Why it’s hard to deliver • Removing manual processes in favor of automation requires migration to cloud, focusing on integration, and providing more self-service applications • telemedicine, analytics, increased regulations, simplifying claims processing are all causing priority conflicts
talk about Increased provider communications and engagement is necessary Why it’s hard to deliver How to connect with providers that have more complex relationships with their health systems and are seeking alternative care models requires next generation thinking and technologies
to talk about • Need to participate in alternative and often value- based care models • Need to be more patient centric Why it’s hard to deliver • Most technology and processes are built around fee for service (FFS) delivery, providers are incented for various kinds of FFS and new ‘accountable tech’ is required for models such as ACOs • Patient-centricity is not easy to define or execute
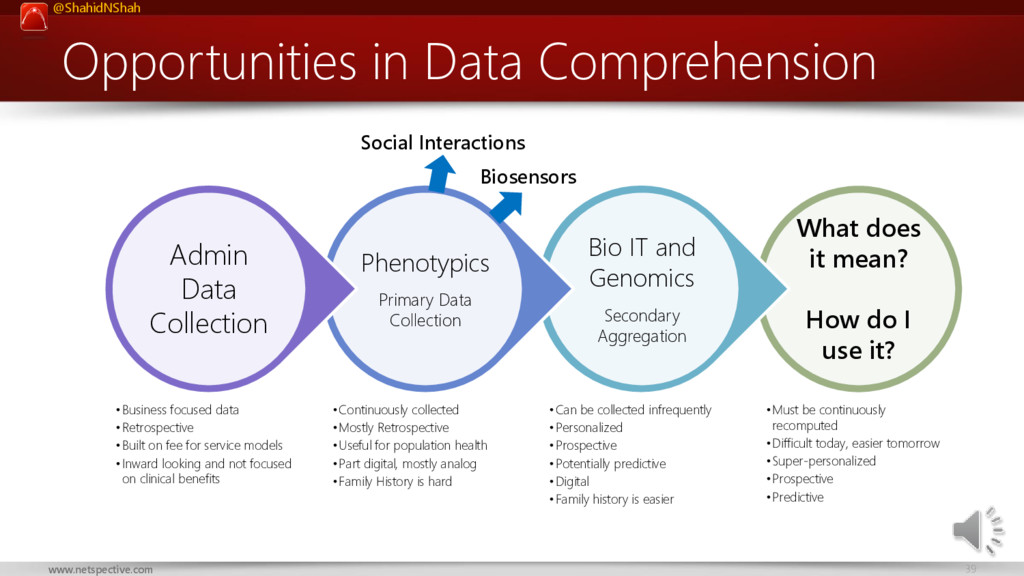
mean? How do I use it? •Must be continuously recomputed •Difficult today, easier tomorrow •Super-personalized •Prospective •Predictive Bio IT and Genomics Secondary Aggregation •Can be collected infrequently •Personalized •Prospective •Potentially predictive •Digital •Family history is easier Phenotypics Primary Data Collection •Continuously collected •Mostly Retrospective •Useful for population health •Part digital, mostly analog •Family History is hard Admin Data Collection •Business focused data •Retrospective •Built on fee for service models •Inward looking and not focused on clinical benefits Biosensors Social Interactions
per procedure / treatment going up but without ability to explain why Cost for same procedure / treatment plan highly variable across localities Unable to compare drug efficacy across patient populations Unable to compare health treatment effectiveness across patients Variability in fees and treatments promotes fraud Lack of visibility of entire patient record causes medical errors
Wellness Specific Prevention Self Service Physiologics Self Service Monitoring Self Service Diagnostics Care Team Monitoring Care Team Diagnostics Healthcare Professional Monitoring Healthcare Professional Diagnostics Hospital Monitoring Hospital Diagnostics
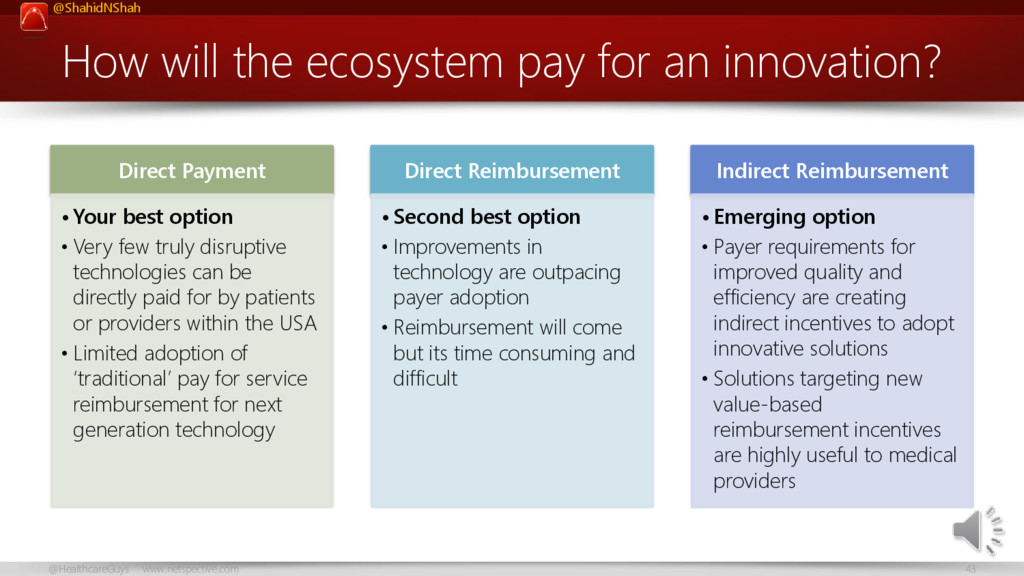
an innovation? Direct Payment • Your best option • Very few truly disruptive technologies can be directly paid for by patients or providers within the USA • Limited adoption of ‘traditional’ pay for service reimbursement for next generation technology Direct Reimbursement • Second best option • Improvements in technology are outpacing payer adoption • Reimbursement will come but its time consuming and difficult Indirect Reimbursement • Emerging option • Payer requirements for improved quality and efficiency are creating indirect incentives to adopt innovative solutions • Solutions targeting new value-based reimbursement incentives are highly useful to medical providers
Therapeutic Tools Diagnostic Tools Patient Administration Patient Education Target the right market so you understand the regulatory impacts Most Regulation Least Regulation Be aware of regulations, don’t fear them, don’t speculate about them, use them as a competitive advantage Proteomics Genomics Biochemical Behavioral Phenotypics Admin Economics Data types
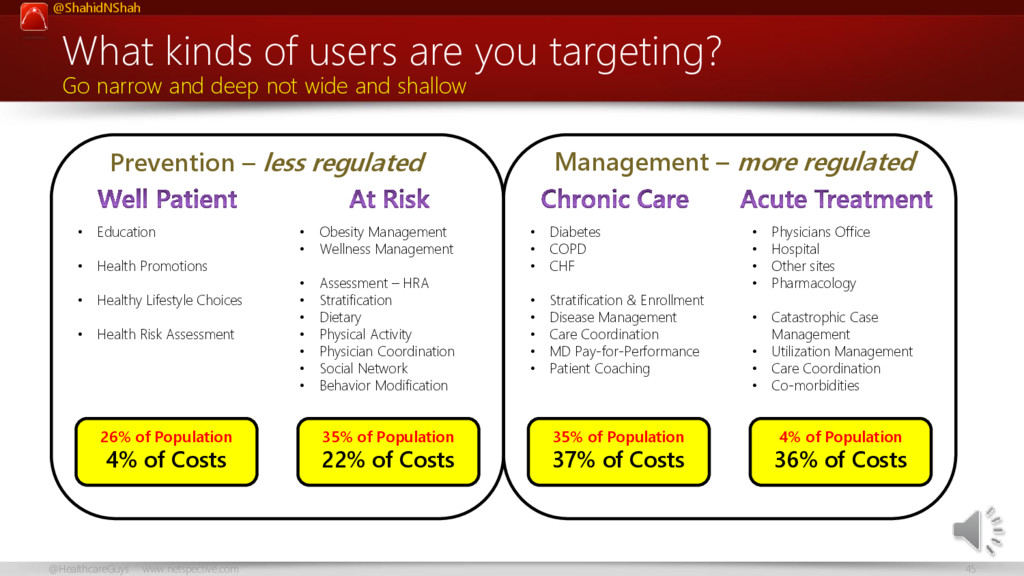
targeting? Go narrow and deep not wide and shallow • Obesity Management • Wellness Management • Assessment – HRA • Stratification • Dietary • Physical Activity • Physician Coordination • Social Network • Behavior Modification • Education • Health Promotions • Healthy Lifestyle Choices • Health Risk Assessment • Diabetes • COPD • CHF • Stratification & Enrollment • Disease Management • Care Coordination • MD Pay-for-Performance • Patient Coaching • Physicians Office • Hospital • Other sites • Pharmacology • Catastrophic Case Management • Utilization Management • Care Coordination • Co-morbidities Prevention – less regulated Management – more regulated 26% of Population 4% of Costs 35% of Population 22% of Costs 35% of Population 37% of Costs 4% of Population 36% of Costs
Improve medical science? Improve access to care? Reduce costs? Improve therapies? Improve diagnostics? Improve drug design? Improve drug delivery? Create better payment models? Focus on jobs that always need to be done, not what you want to build
Circumstance • The specific problems a customer cares about • The way they assess solutions Context • Find a way to be with the customer when they encounter a problem and • Watch how they try to solve it Constraints • Develop an innovative means around a barrier constraining consumption Compensating behaviors • Determining whether a job is important enough to consider targeting • One clear sign is a customer spending money trying to solve a problem Criteria • Customers look at jobs through functional, emotional, and social lenses From “Jobs to be Done” to the “Five Cs of Opportunity Identification” Source: http://blogs.hbr.org/anthony/2012/10/the_five_cs_of_opportunity_identi.html
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
![Thank You Visit http://www.netspective.com http://www.healthcareguy.com E-mail [email protected] Follow @ShahidNShah @HealthcareGuys](https://files.speakerdeck.com/presentations/c2018b09485046098baceb1f4c86e6b8/slide_46.jpg){kind=link}
{kind=link}
{kind=link}
{kind=link}