Introduction
A key component of respiratory therapy is pulmonary function testing (PFT), which is essential for both diagnosing and tracking lung problems. Knowing the ins and outs of PFT is crucial whether you’re a seasoned respiratory therapist looking for last-minute CEUs or are brand-new to the profession. This beginner’s guide will go into the fundamental concepts of PFT and provide you with information, advice, and tools to help you succeed in this important area of respiratory treatment.
Section 1: What is Pulmonary Function Testing?
Subtitle: Unraveling the Basics
A battery of tests called pulmonary function testing, or PFT, determines how effectively your lungs are working. These exams assess the capacity, airflow, and gas exchange of the lungs, among other aspects of lung health. PFTs are crucial in the diagnosis and treatment of respiratory conditions such pulmonary fibrosis, COPD, and asthma.
Section 2: Types of Pulmonary Function Tests
Subtitle: Exploring the Varieties
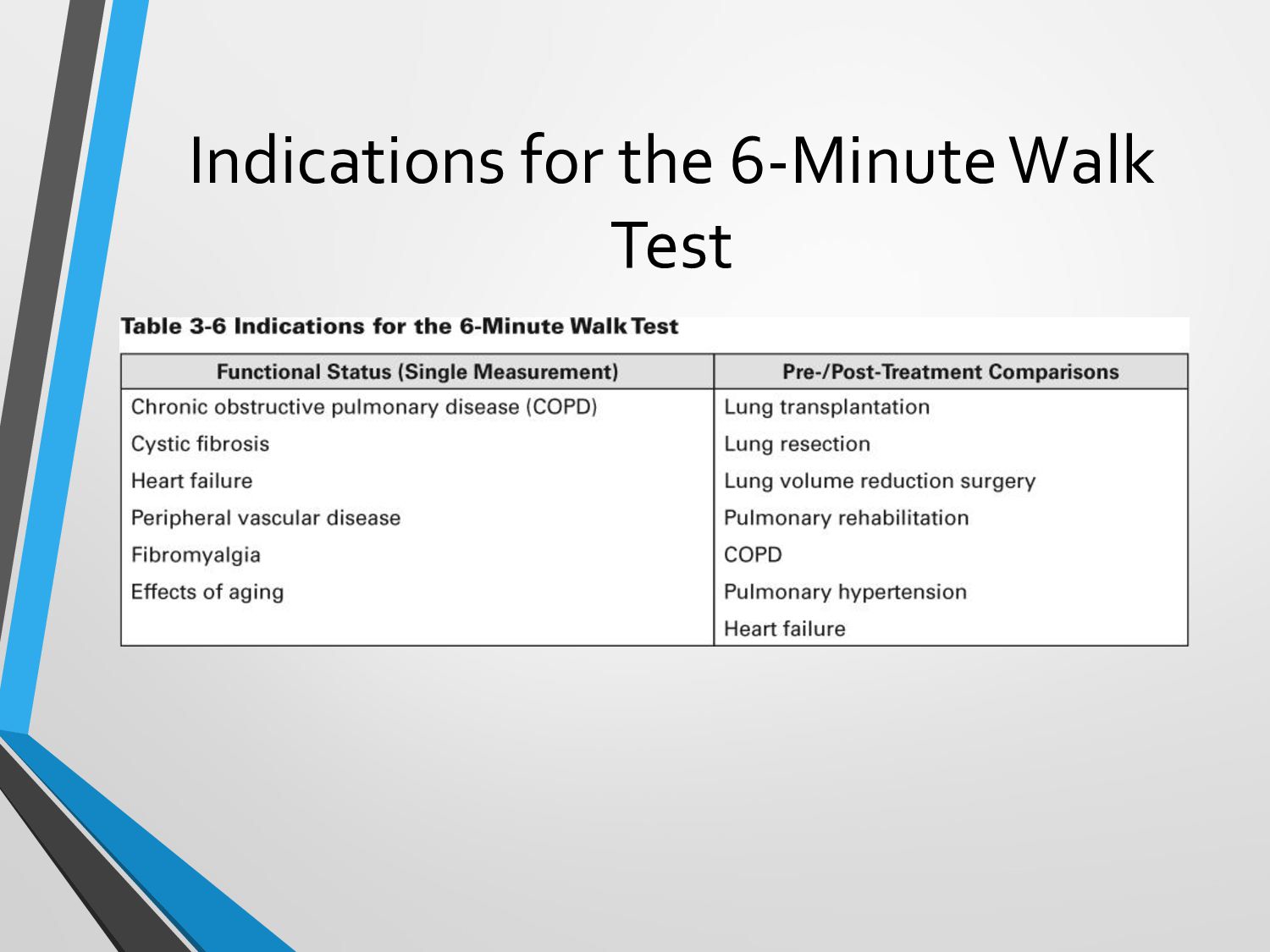
PFTs come in a variety of forms, each with a distinct function. Spirometry, lung volume testing, and gas exchange tests are a few examples of typical PFTs. For instance, lung volume tests identify lung capacity whereas spirometry assesses lung function and airflow. Effective patient care requires a thorough understanding of the various PFT types.
Section 3: Importance of PFTs in Respiratory Care
Subtitle: The Clinical Significance
PFTs provide insightful information about a patient’s respiratory health. They support the diagnosis of lung disorders, evaluate the severity of diseases, and track the success of treatments. PFT findings are used by respiratory therapists to create individualized care programs and monitor patients’ advancement over time.
Section 4: Interpreting PFT Results
Subtitle: Decoding the Numbers
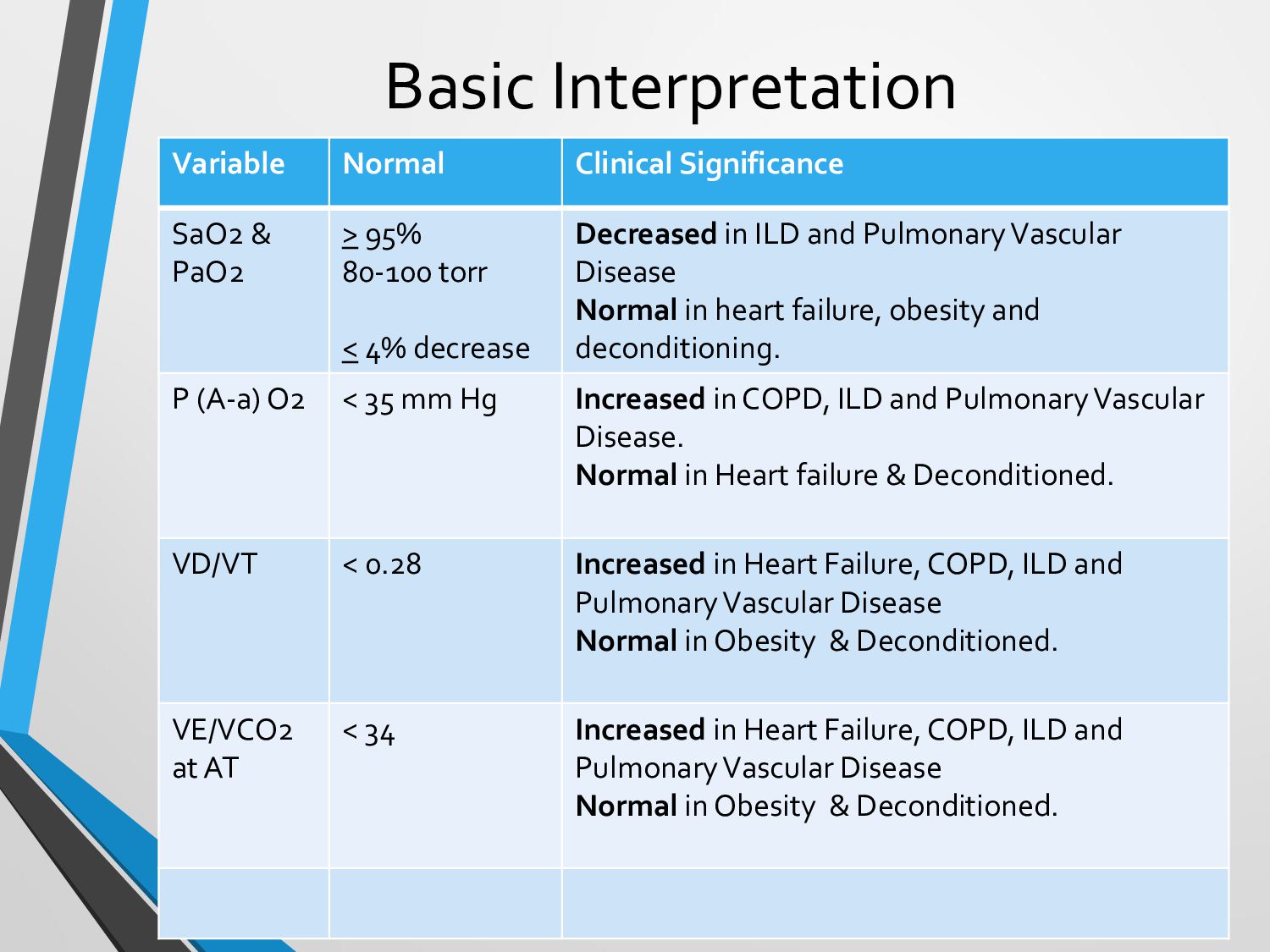
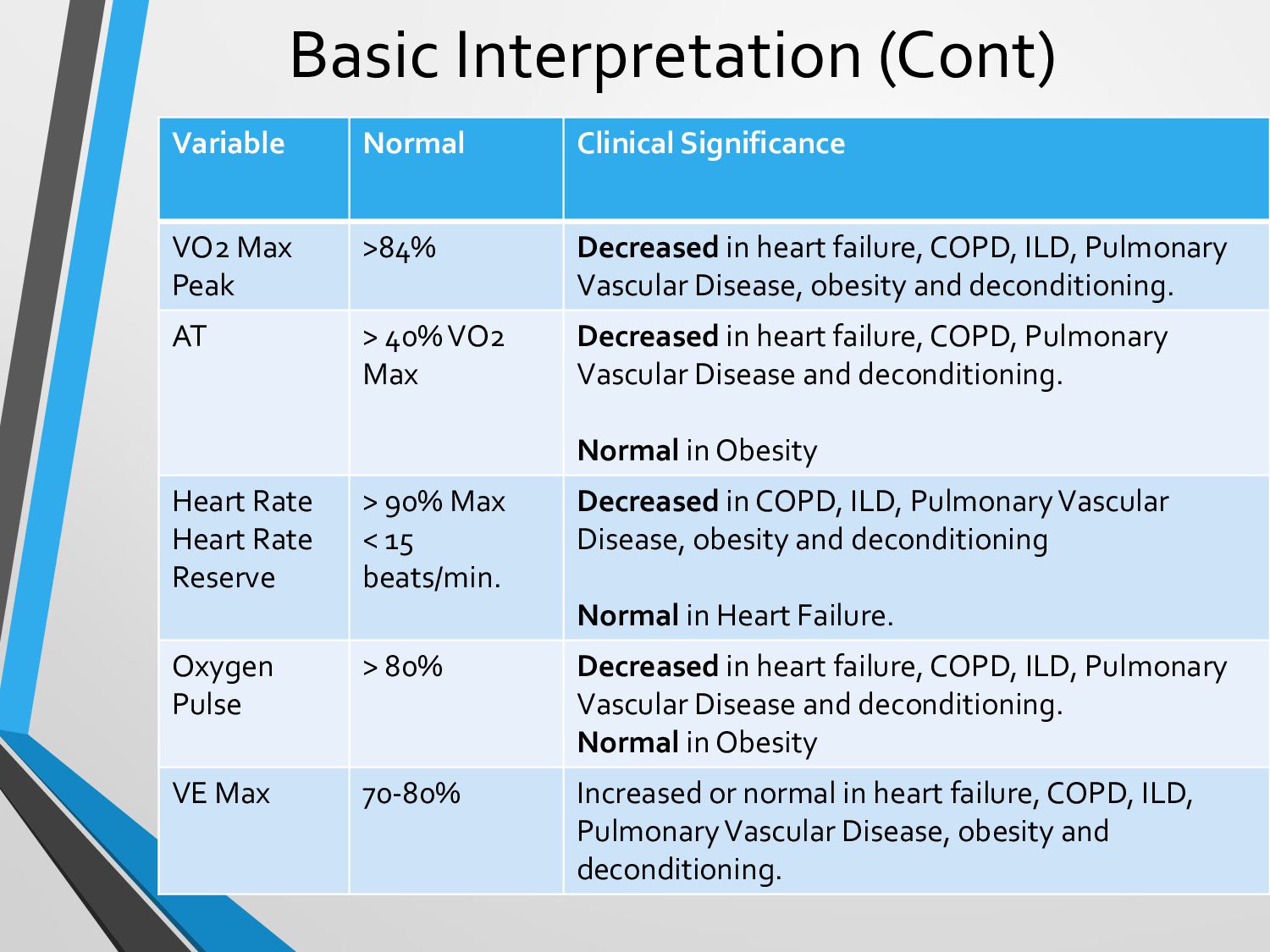
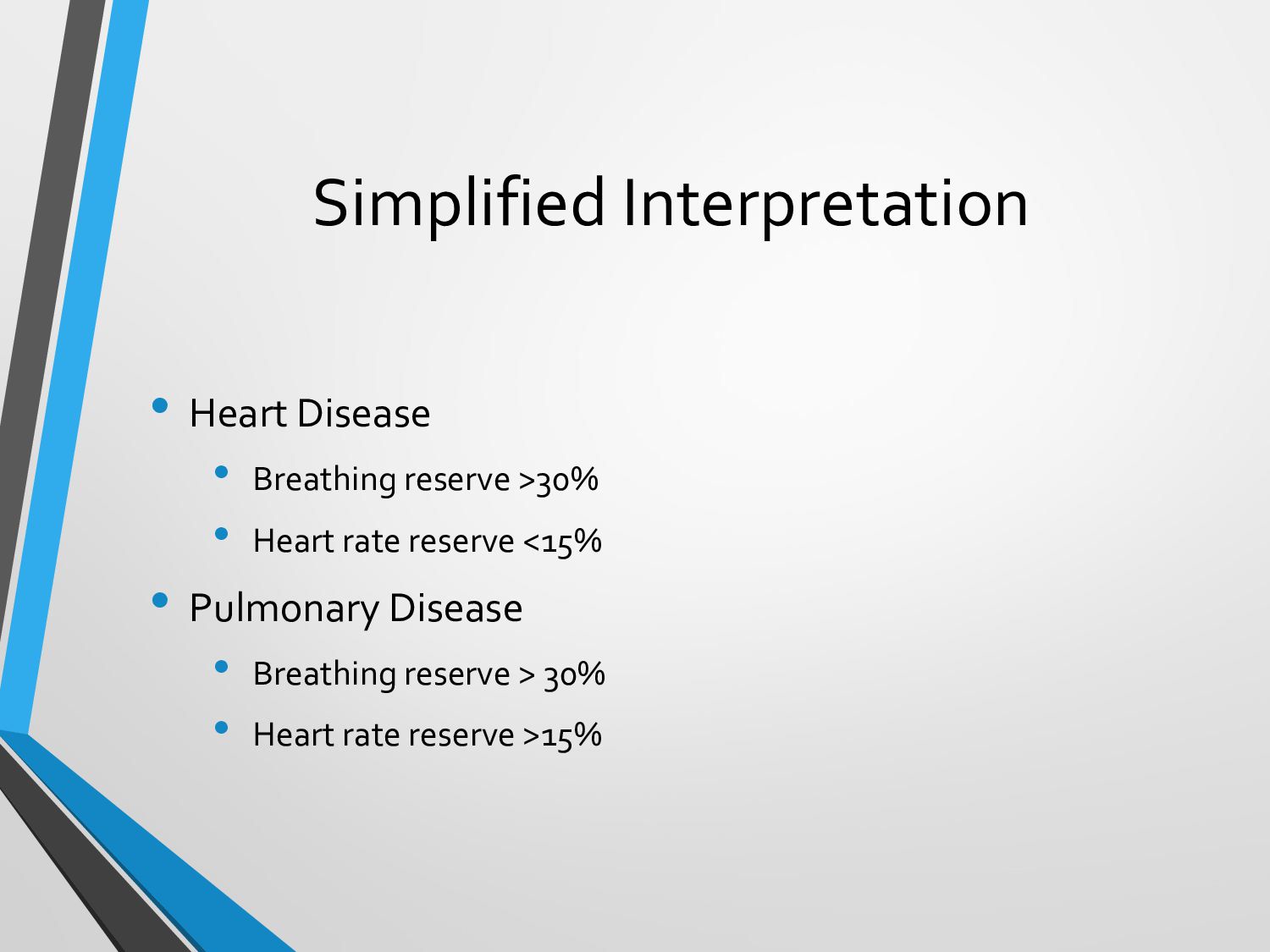
Although it might be challenging, understanding PFT results is an essential ability for respiratory therapists. The forced vital capacity (FVC), forced expiratory volume in one second (FEV1), and the FEV1/FVC ratio are important measurements to look for. These figures offer important details about lung health and the presence of any blockages.
Section 5: Common Pitfalls and Challenges
Subtitle: Navigating Roadblocks
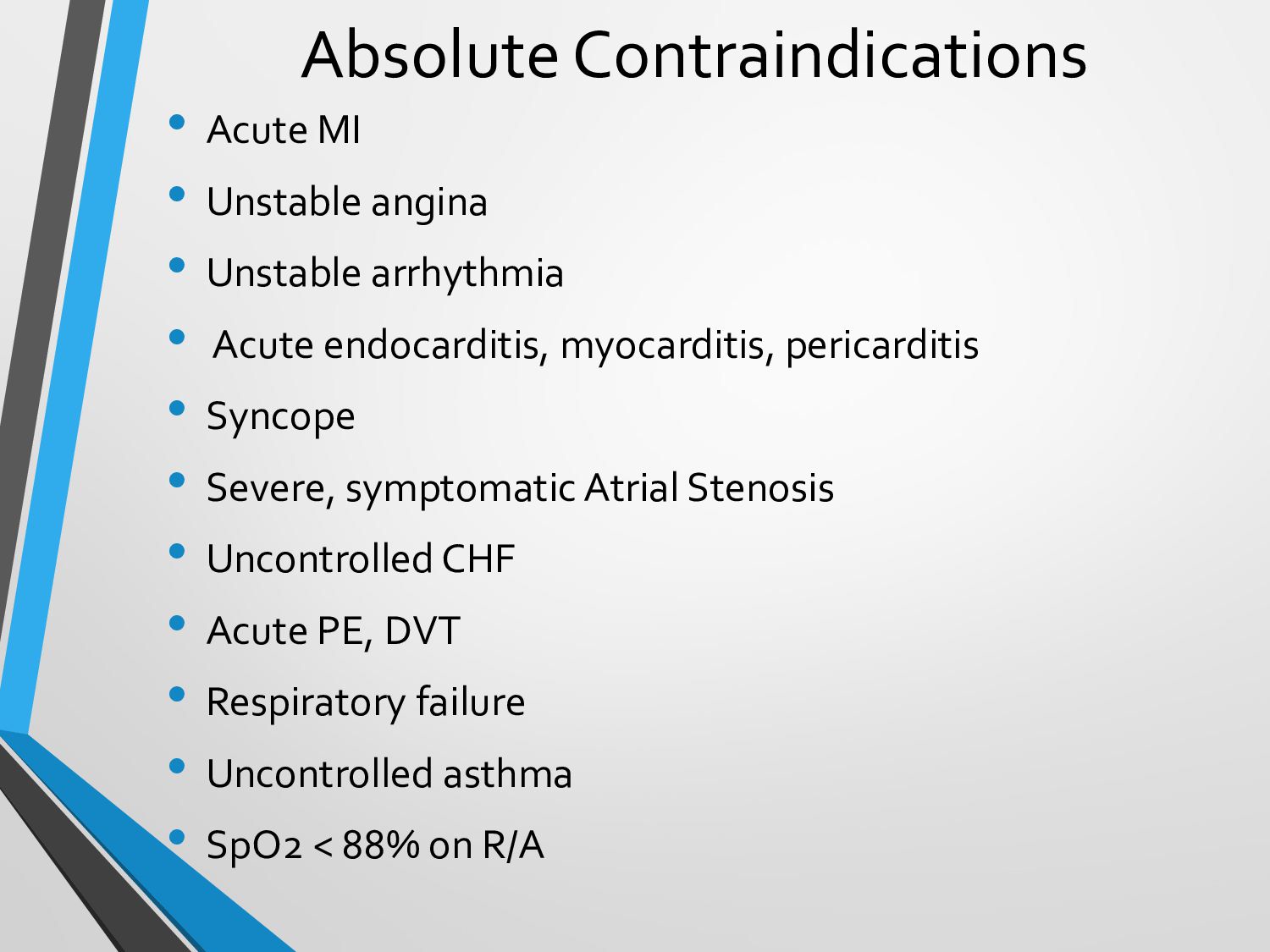
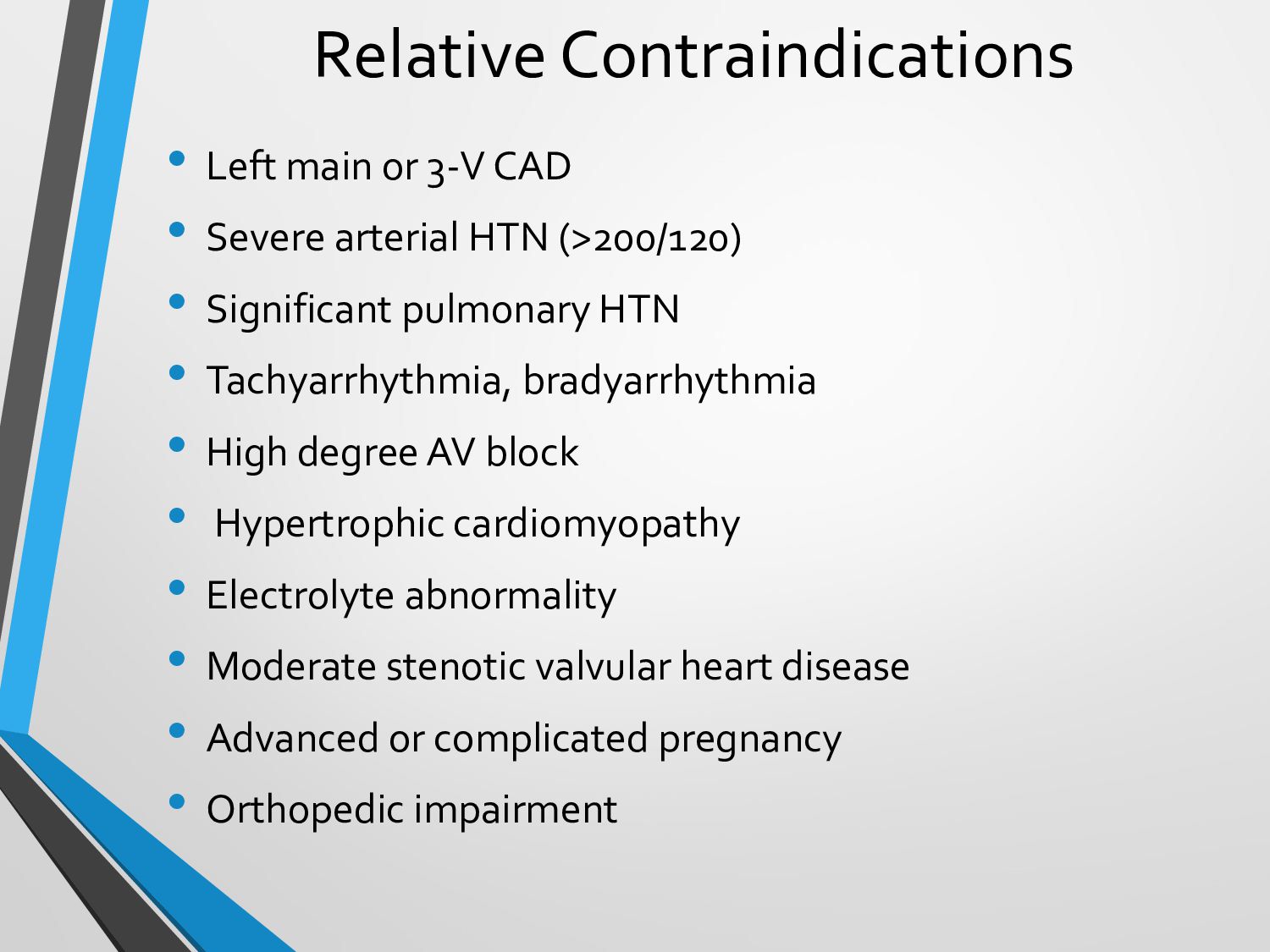
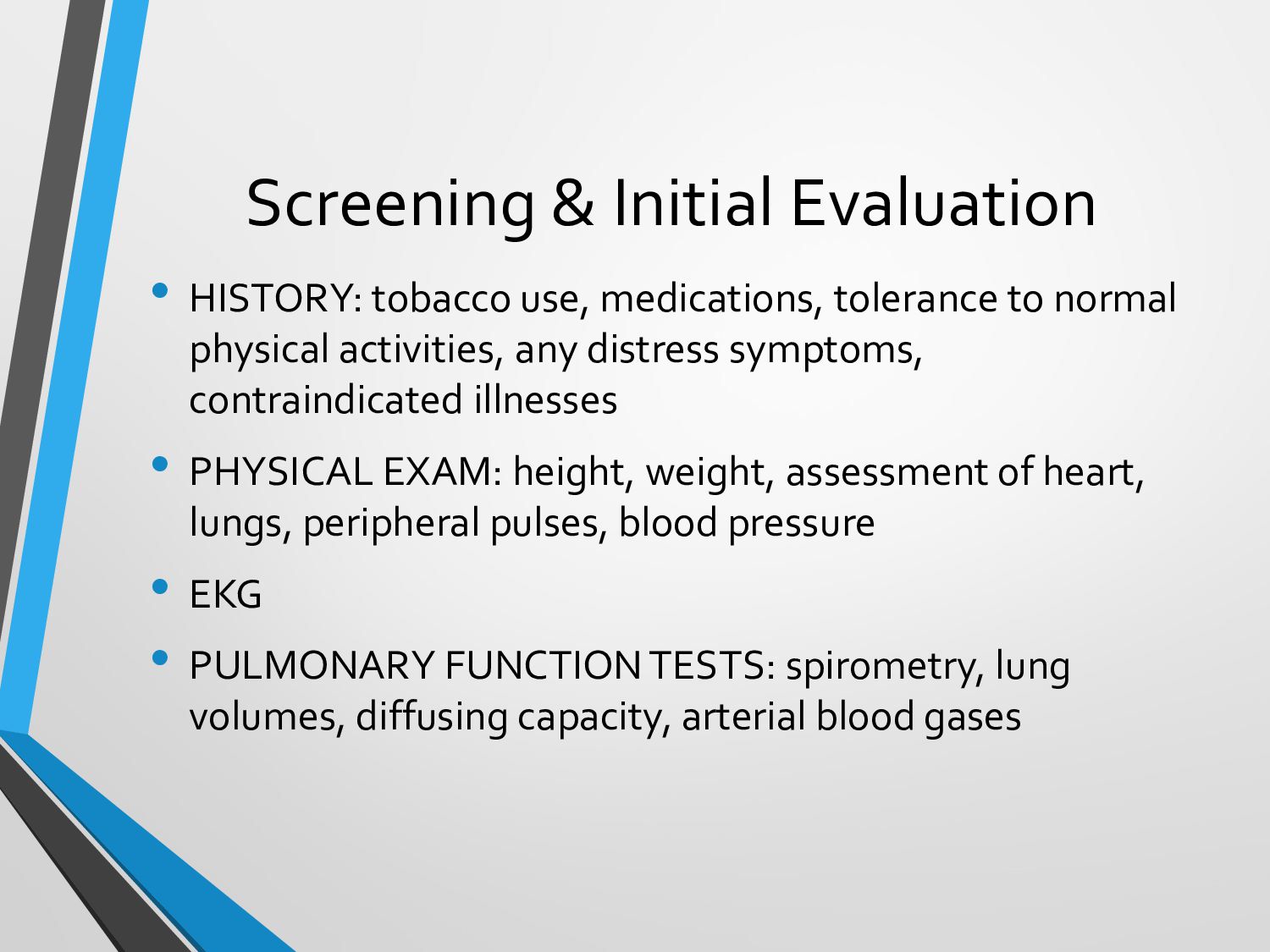
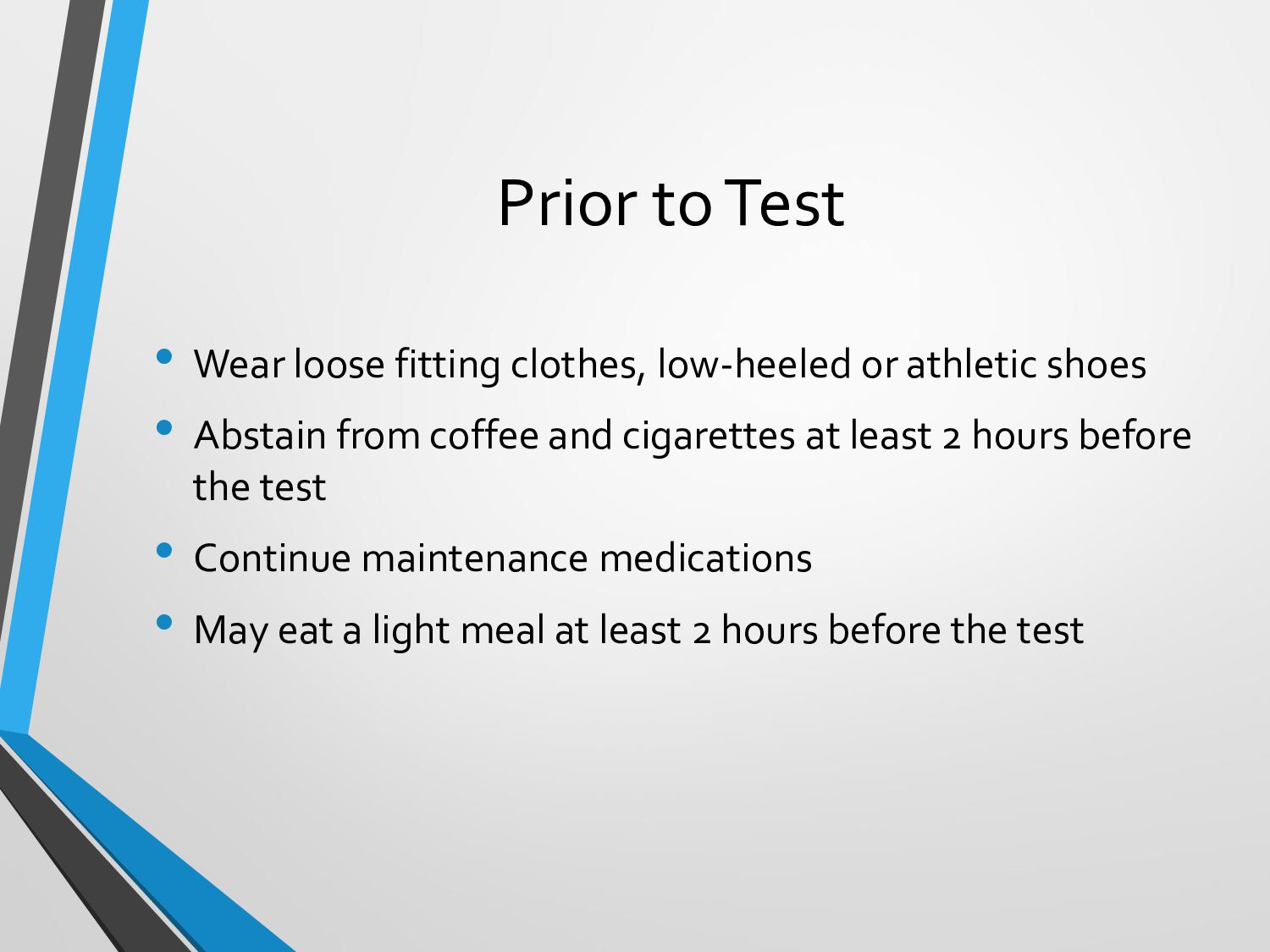
PFTs have their difficulties, much as any diagnostic test. The outcomes can be affected by patient cooperation, sound technique, and external variables. To achieve accurate assessments, it’s critical to be aware of potential dangers and work toward reducing inaccuracies.
Section 6: Resources for Respiratory Therapists
Subtitle: CEUs and Learning Opportunities
It’s essential for respiratory therapists to keep learning. There are tools accessible if you’re trying to find CEUs (Continuing Education Units) at a discount or last-minute CEUs. Courses for respiratory therapists are available on websites like “CEUs for Less”. Furthermore, the AARC (American Association for Respiratory Care) offers free CEUs for respiratory therapists that have been approved by the AARC, guaranteeing that you stay up to speed with the most recent developments in pulmonary function testing.
Conclusion:
Knowing How the Pulmonary System Works A crucial component of respiratory therapy is testing. These tests are an essential tool in the field because they offer crucial information for identifying and treating lung problems. To improve your knowledge and abilities as a respiratory therapist, keep in mind to evaluate results cautiously, face problems with confidence, and utilize tools like AARC-approved free CEUs.
visit our site : unlimited ceu
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}