girls ¡ Course: early onset, persistent but improved over lifetime for most ¡ Diagnostic Issues: ¡ Gender: Males are 5 times more likely to have ASD ¡ Highly heritable/Broad Autism Phenotype ¡ Co-morbid with intellectual disabilities, anxiety, depression
studies ¡ Better Methods of Assessment ¡ Sensitivity: Measures a test’s ability to find individuals that fit a criteria (e.g. True Positives) ¡ Specificity: Measures a test’s ability to identify individuals without criteria (e.g. True Negatives)
diagnosis and treatment of neurodevelopmental disorders is usually necessary for accurate and appropriate diagnosis. – Practice Parameter, Neurology, 2000 ¡ Training/Education: ¡ general level and specialized in the disorder ¡ Assessment: ¡ must include reliable and valid measures ¡ often multi-method with multiple informants
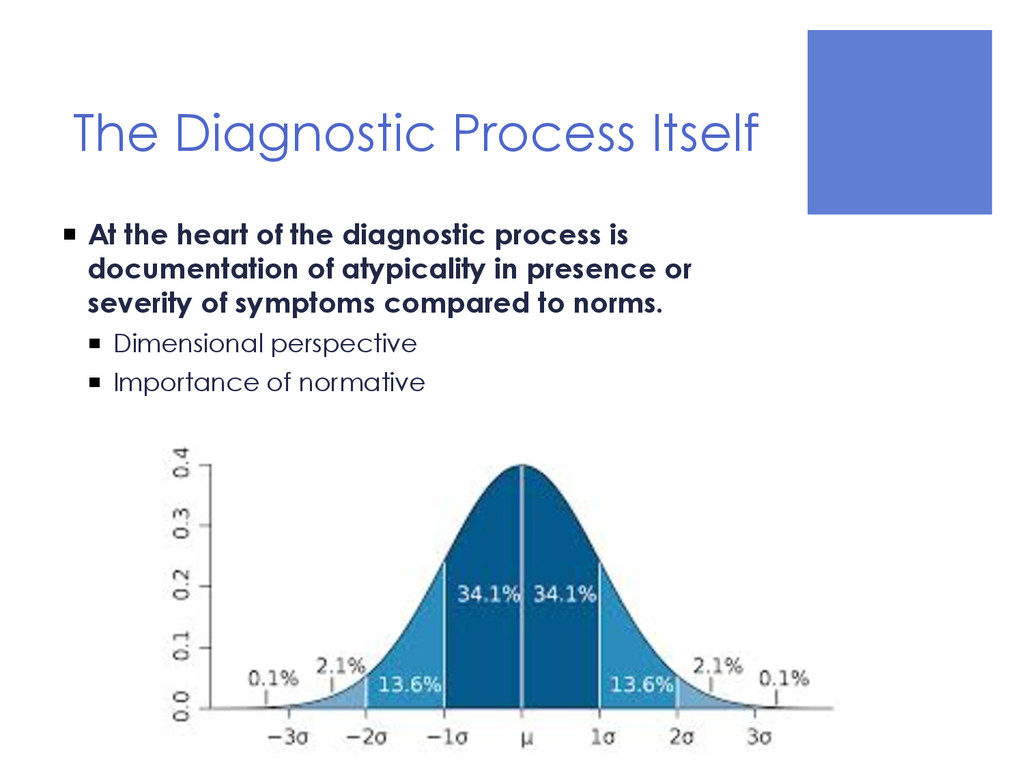
diagnostic process is documentation of atypicality in presence or severity of symptoms compared to norms. ¡ Dimensional perspective ¡ Importance of normative knowledge
of Mental Disorders (DSM) ¡ Published by American Psychiatric Association ¡ The main purpose of the DSM is to provide standard guidelines for clinicians to use for the diagnosis of different psychological disorders and conditions ¡ It is the primary manual used by clinicians to provide a formal diagnosis of autism and related disorders
Schizophrenic reaction, childhood type • Autism described as symptom ¡ 1968 (DSM-II) o Schizophrenia, childhood type; schizoid personality • Autism described as symptom in two disorders ¡ 1980 (DSM-III) o Pervasive Developmental Disorder: • Childhood Onset PDD • Infantile Autism • Atypical Autism
of Neurodevelopmental Disorders workgroup (13 members, 16 advisors) in 2007 ¡ Kaufman (2012) reported that key work processes consisted of: • Biweekly teleconferences • Semi-annual in-person meetings • Additional web conferences • “Other meetings as needed” ¡ More than 2500 hours over the course of 5 years
Francesca Happe ¡ James Harris ¡ Walter Kaufmann ¡ Bryan King ¡ Catherine Lord ¡ Joseph Piven ¡ Sally Rogers ¡ Sarah Spence ¡ Susan Swedo, Chair ¡ Fred Volkmar (thru 2009) ¡ Amy Wetherby ¡ Harry Wright ****** ¡ 16 Advisors
research literature • Secondary data analysis • Clinical evaluations ¡ Work products and drafts were vetted through: • Public comments • Presentations at scientific meetings • Presentations to advocacy groups • Review by leading experts (i.e., Sir Michael Rutter, etc.) • Review by members of professional groups (i.e., International Society of Autism Research, etc.) Kaufman, 2012
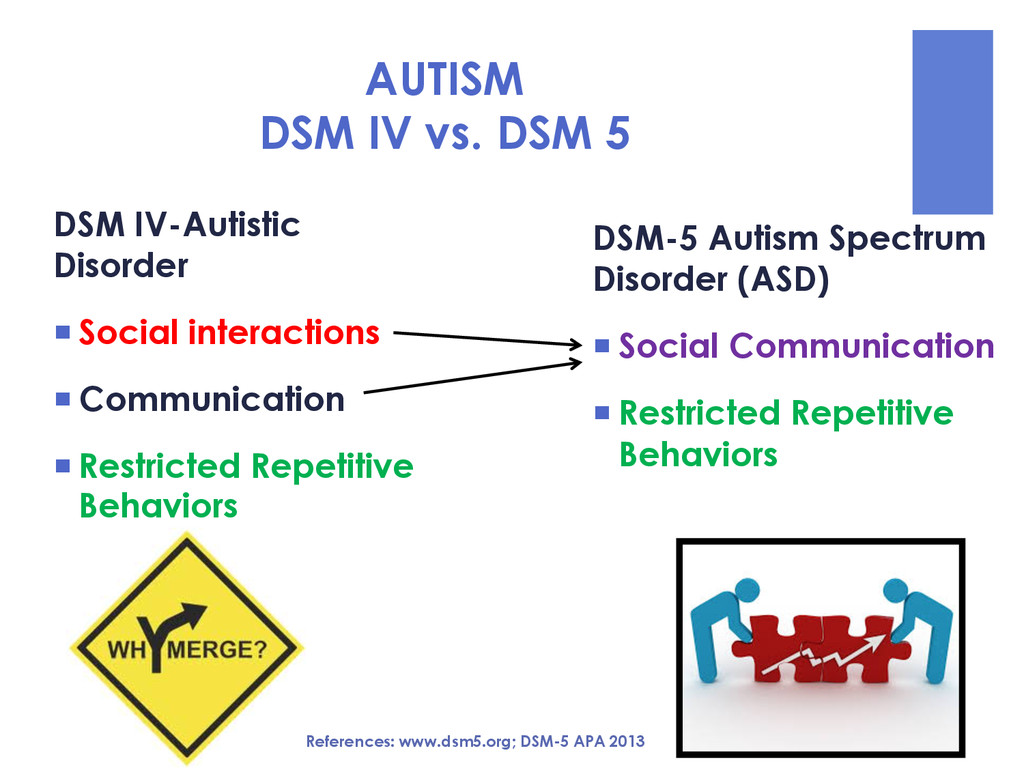
burgeoning research literature on ASD ¡ Identify the “essential shared features” of ASD ¡ Re-integrate Asperger’s Disorder and PDD-NOS into the autism spectrum ¡ Combine categorical and dimensional measures to formulate individual diagnosis Happe’, 2011
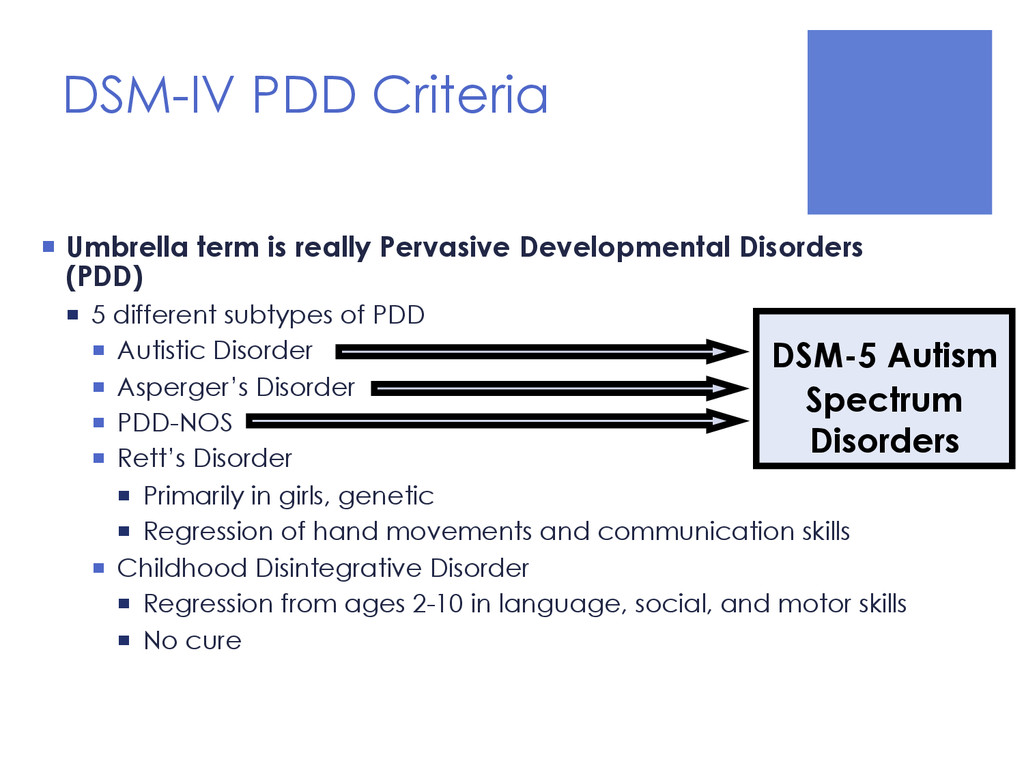
Disorders (PDD) ¡ 5 different subtypes of PDD ¡ Autistic Disorder ¡ Asperger’s Disorder ¡ PDD-NOS ¡ Rett’s Disorder ¡ Primarily in girls, genetic ¡ Regression of hand movements and communication skills ¡ Childhood Disintegrative Disorder ¡ Regression from ages 2-10 in language, social, and motor skills ¡ No cure DSM-5 Autism Spectrum Disorders
Syndrome ¡ ASD behaviors not salient in RS patients except for a brief period of time ¡ Symptoms are etiological not behavior based ¡ Can still be described under DSM-5 ASD criteria with specifier “with known genetic or medical condition” ¡ Child Disintegrative Disorder ¡ Rarity and difficulty in diagnosis ¡ Acuity and severity of regression ¡ Co-occurring physical symptoms (loss of bowel and bladder control)
Disorder Specifiers ¡ With or without accompanying intellectual impairment ¡ With or without accompanying language impairment ¡ Associated with a known medical or genetic condition or environmental factor ¡ With catatonia References: www.dsm5.org; DSM-5 APA 2013
Disorder ¡ Requires severity ratings for both categories ¡ Level 1 – Requiring Support ¡ Level 2 -- Requiring Substantial Support ¡ Level 3 – Requiring Very Substantial Support References: www.dsm5.org; DSM-5 APA 2013
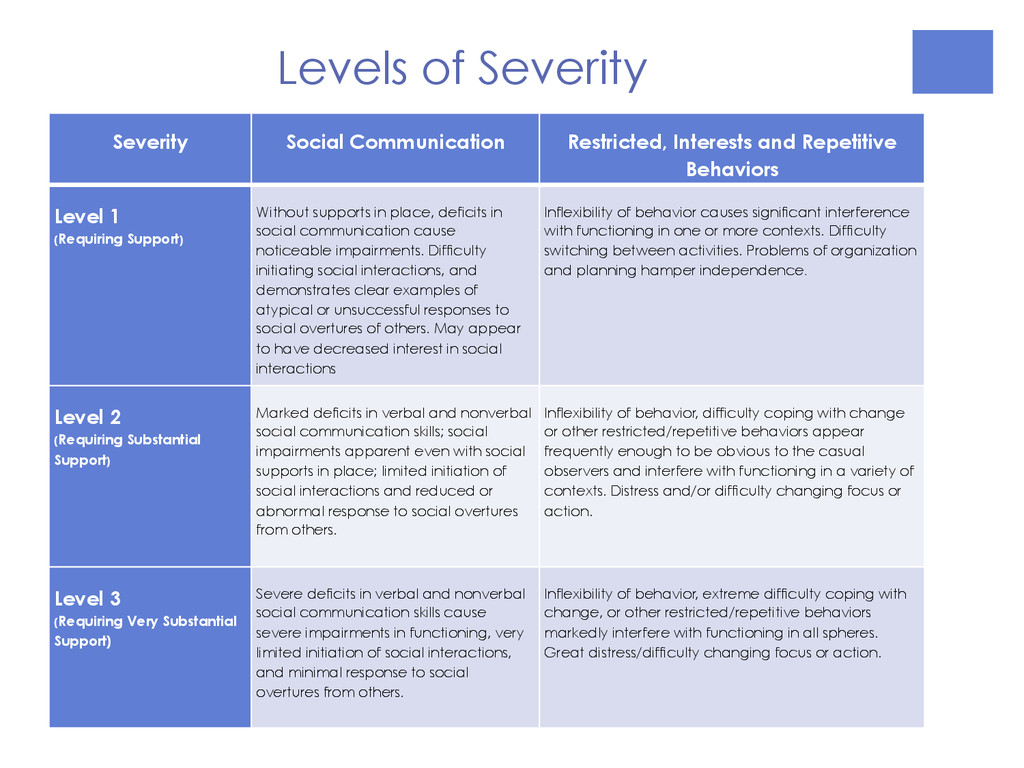
Level 1 (Requiring Support) Without supports in place, deficits in social communication cause noticeable impairments. Difficulty initiating social interactions, and demonstrates clear examples of atypical or unsuccessful responses to social overtures of others. May appear to have decreased interest in social interactions Inflexibility of behavior causes significant interference with functioning in one or more contexts. Difficulty switching between activities. Problems of organization and planning hamper independence. Level 2 (Requiring Substantial Support) Marked deficits in verbal and nonverbal social communication skills; social impairments apparent even with social supports in place; limited initiation of social interactions and reduced or abnormal response to social overtures from others. Inflexibility of behavior, difficulty coping with change or other restricted/repetitive behaviors appear frequently enough to be obvious to the casual observers and interfere with functioning in a variety of contexts. Distress and/or difficulty changing focus or action. Level 3 (Requiring Very Substantial Support) Severe deficits in verbal and nonverbal social communication skills cause severe impairments in functioning, very limited initiation of social interactions, and minimal response to social overtures from others. Inflexibility of behavior, extreme difficulty coping with change, or other restricted/repetitive behaviors markedly interfere with functioning in all spheres. Great distress/difficulty changing focus or action. Levels of Severity
multiple contexts § Deficits in social-emotional reciprocity § Deficits in nonverbal communicative behaviors used for social interaction § Deficits in developing, maintaining and understanding relationships DSM-5- Autism Spectrum Disorders
manifested by at least two of the following: § Stereotyped or repetitive motor movements, use of objects or speech § Insistence on sameness, inflexible adherence to routines, or ritualized patterns of verbal or nonverbal behavior § Highly restricted, fixated interests that are abnormal in intensity or focus § Hyper-or hyporeactivity to sensory input or unusual interests in sensory aspects of the environment DSM-5- Autism Spectrum Disorders
Tools for Autism Spectrum Disorders and General Infant Development § Ages and Stages Questionnaire (ASQ) § Modified Checklist for Autism in Toddlers (M-CHAT) § Communication and Symbolic Behavior Scales (CSBS) § Screening Tool for Autism in Toddlers and Young Children (STAT) ¡ Diagnostic Measures Specific to Autism § ADI-R: Clinical diagnostic interview “gold standard” § ADOS: Semi-structured clinical assessment “ gold standard” § CARS: Brief paper and pencil assessment typically based on parent report ¡ Measures of Developmental Level, IQ and Adaptive Skills are also typically recommended for a comprehensive diagnostic evaluation.
that includes both a current intellectual deficit and a deficit in adaptive functioning with onset during the developmental period ¡ This is no longer based only on IQ level
by both clinical assessment and individualized, standardized intelligence testing ¡ B. Deficits in adaptive functioning that cause impairment in the absence of support. ¡ C. Onset during the developmental period References: www.dsm5.org; DSM-5 APA 2013
clinical severity level cannot be reliably assessed. ¡ Diagnosed when an individual fails to meet expected developmental milestones in several areas of intellectual functioning ¡ Can apply to individuals who are unable to undergo systematic assessments of intellectual functioning, including children who are too young to participate in standardized testing. ¡ Requires reassessment after a period of time. References: www.dsm5.org; DSM-5 APA 2013
mixed receptive-expressive language disorders) ¡ Speech Sound Disorder (new name for phonological disorder) ¡ Childhood-onset fluency disorder (new name for stuttering) ¡ Social Communication Disorder-new condition reflecting poor pragmatic skills References: www.dsm5.org; DSM-5 APA 2013
most common and stuttering least ¡ Course: early onset, improved by adulthood ¡ DX Issues: ¡ Highly heritable ¡ Co-morbid with learning disabilities, multiple communication disorders
¡ Deficits in both Communication & Repetitive/Restricted Behaviors ¡ Only Deficits in Communication: ¡ Social Communication Disorder (SCD) ¡ Deficiencies in pragmatic language that interfere with communication, social functioning and learning, with onset in early childhood. ¡ Only Deficits in Repetitive Behaviors ¡ Stereotypic Movement Disorder ¡ Repetitive, seemingly driven, apparently purposeless motor behavior not better explained by ASD
is a necessary but insufficient basis for making qualified diagnoses of ASD ¡ Requires education and training specific to the disorder along with knowledge of measurement. ¡ Rule in and rule out disorders ¡ Determine “significant” and “impairment” ¡ Select and administer appropriate measures ¡ Consider multiple sources of information and integrate them accurately
diagnosis of PDD-NOS and Asperger’s Syndrome? ¡ Research (Kim et al., 2014) supports that the estimated prevalence of autism will decrease ¡ More children will be identified with social communication disorder (SCD) ¡ 83% of children who received a diagnosis of autism under DSM-IV criteria will still receive diagnosis with DSM-5 ¡ 14 percent would meet criteria for SCD
who met DSM-IV criteria for autism will now receive DSM-5 diagnosis of SCD (Kim et al., 2014) ¡ Concerns about treatment guidelines for SCD ¡ PDD-NOS ¡ 71% will now be diagnosed with ASD, 22% with SCD, 7% with another non-autism disorder ¡ Asperger’s Disorder ¡ 91% would be diagnosed with ASD, 6% with SCD, and 3% with another non-autism disorder ¡ Autistic Disorder ¡ 99% diagnosed with ASD and 1% with SCD
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}