Fundamental aspects of insulin therapy and management and the application to exercise and sport. The goal will be to deliver 3-4 management suggestions to decrease risk of hypo and hyperglycemia.
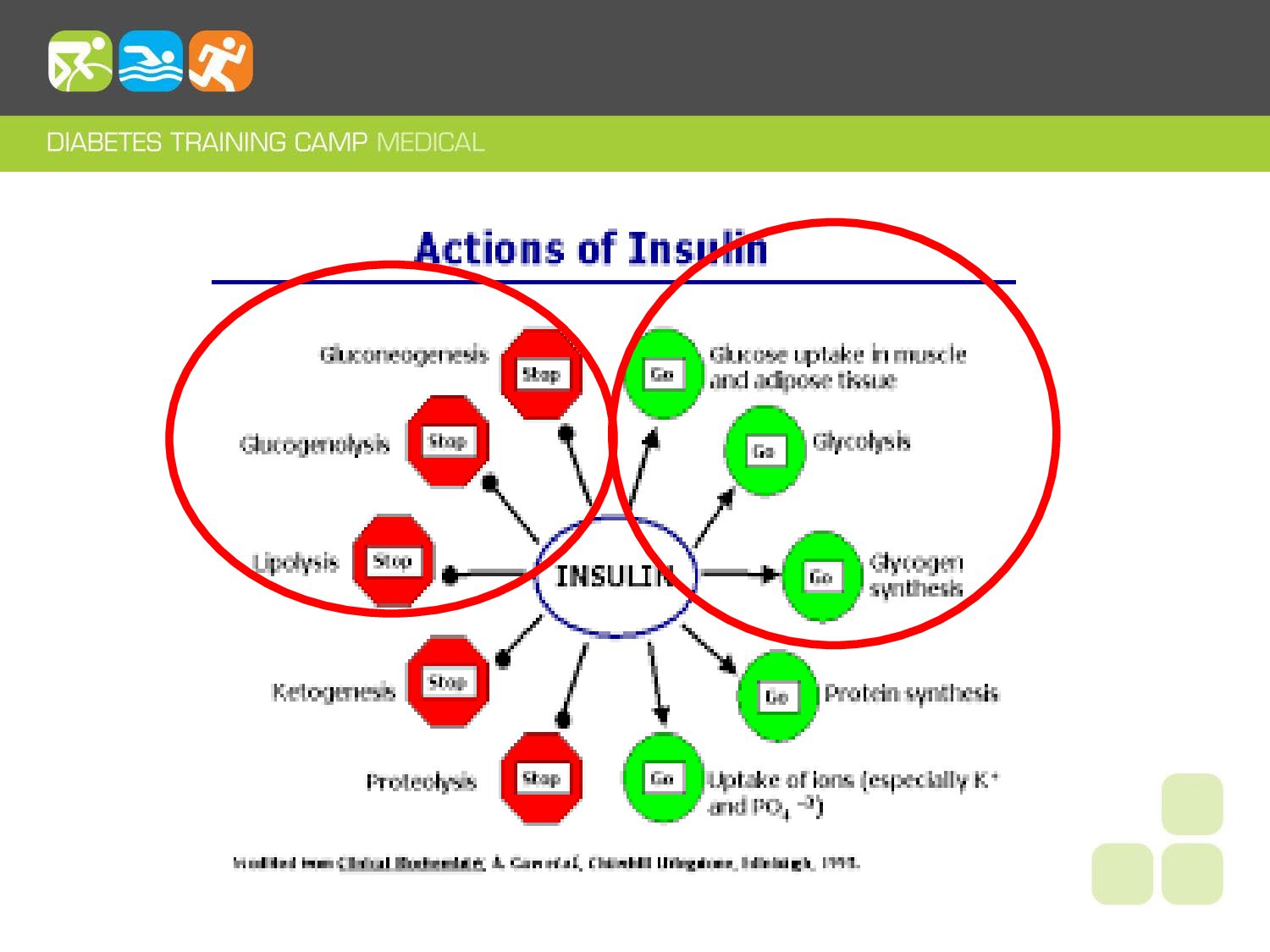
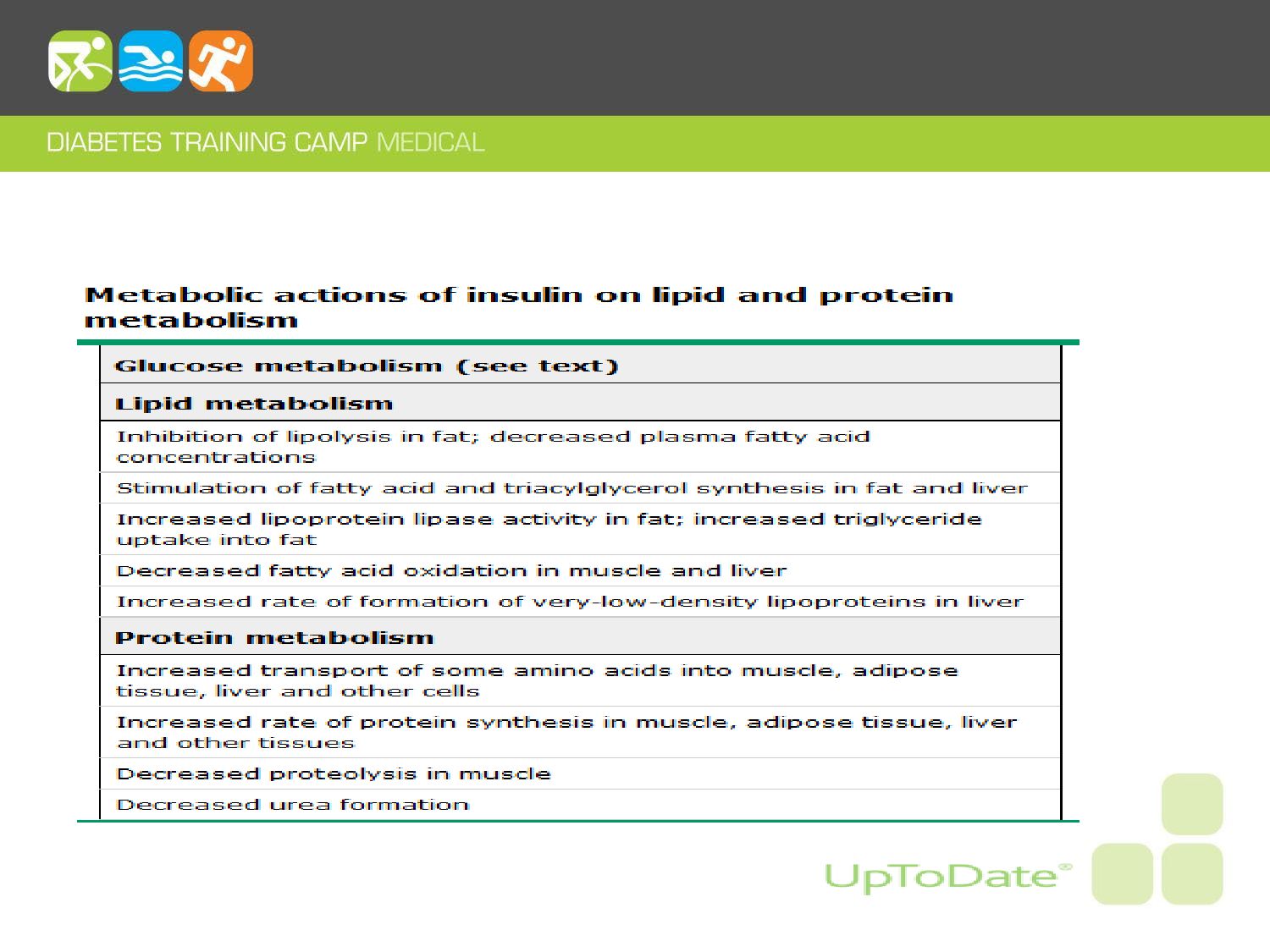
physical activity. • Review insulin action & its role in fuel mobilization for the working muscle. • Review impact of over-insulinization & risk of hypoglycemia. • Identify basic insulin management strategies to decrease risk of hypoglycemia and/or hyperglycemia in activity, exercise & sport.
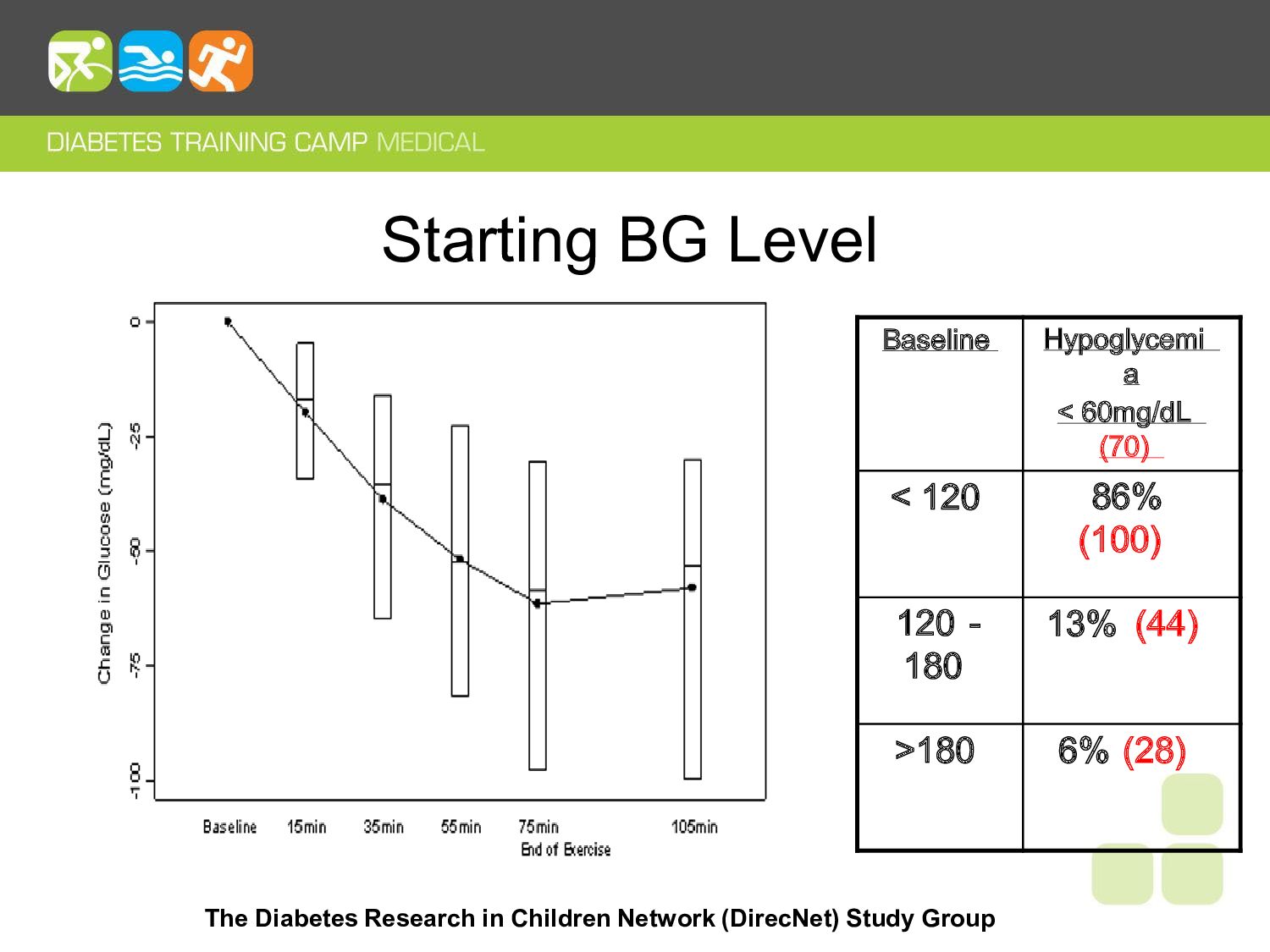
of at least 25%; Only 1 subject with meaningful increase in BG. • Average fall is 40% from baseline. • 52% drop to < 70 mg/dL and 30% drop to < 60 mg/dL. • I ncidence of hypoglycemia varies with baseline BG. • 15 grams CHO insufficient to reliably treat hypoglycemia in exercise
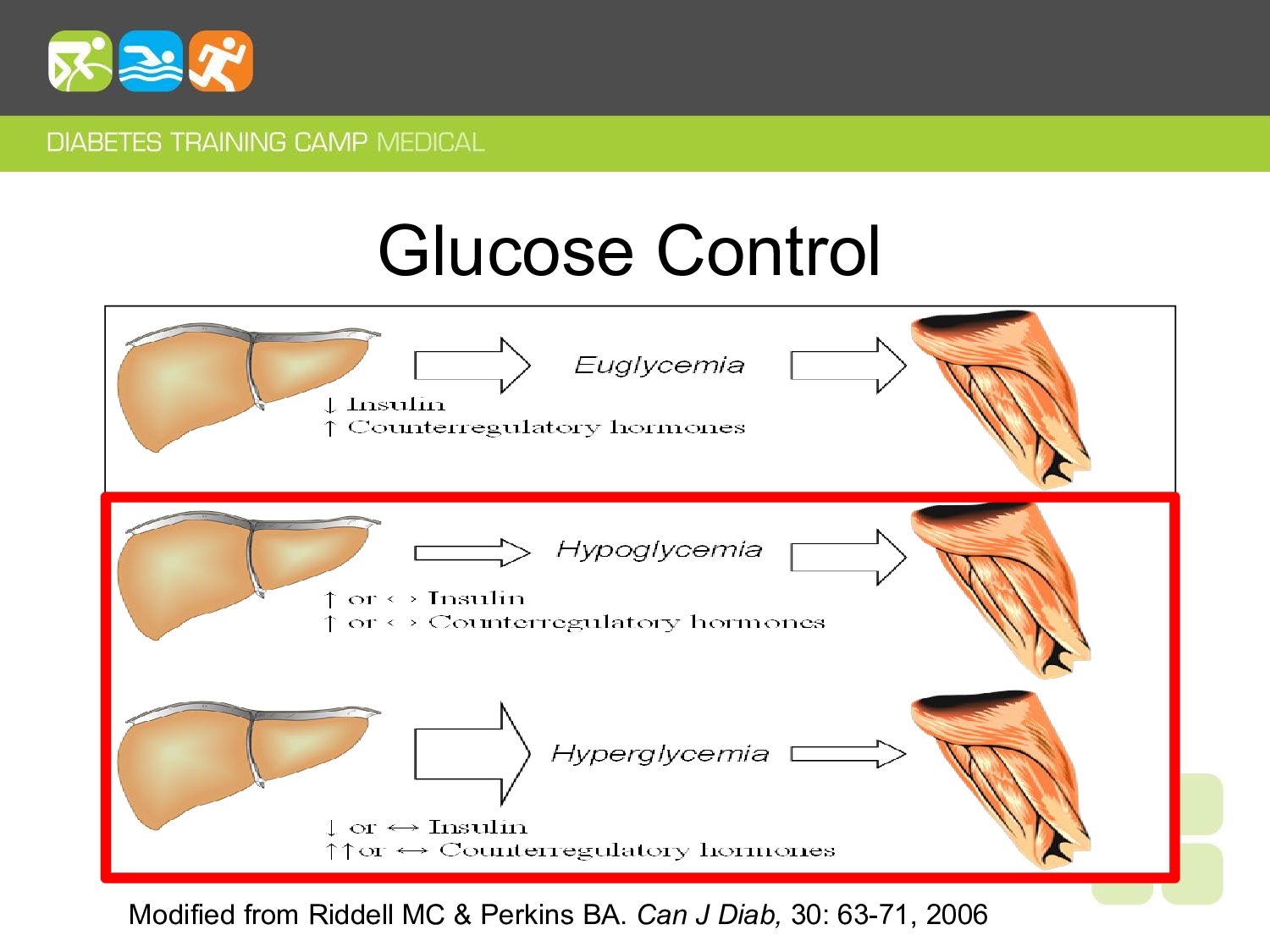
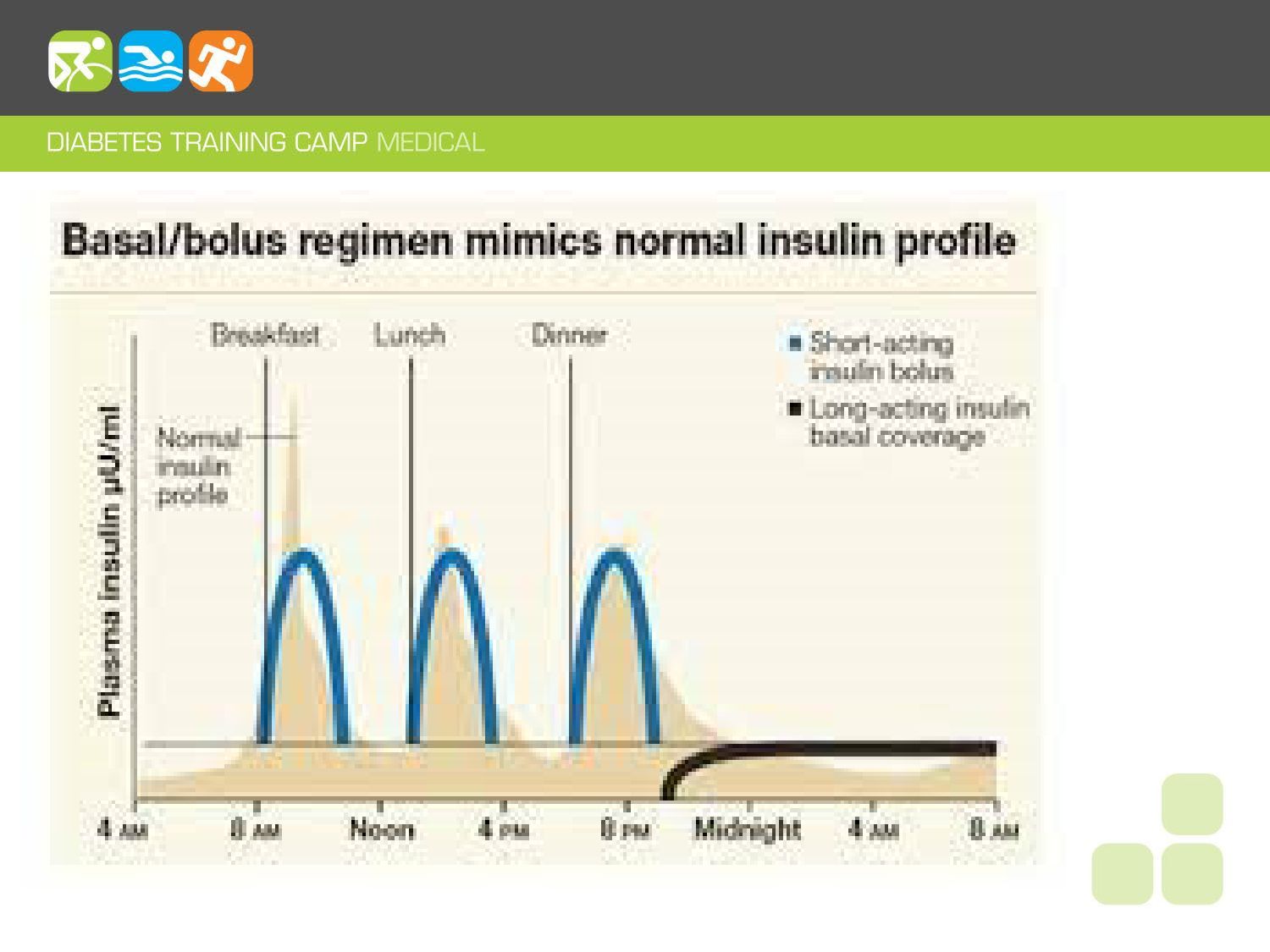
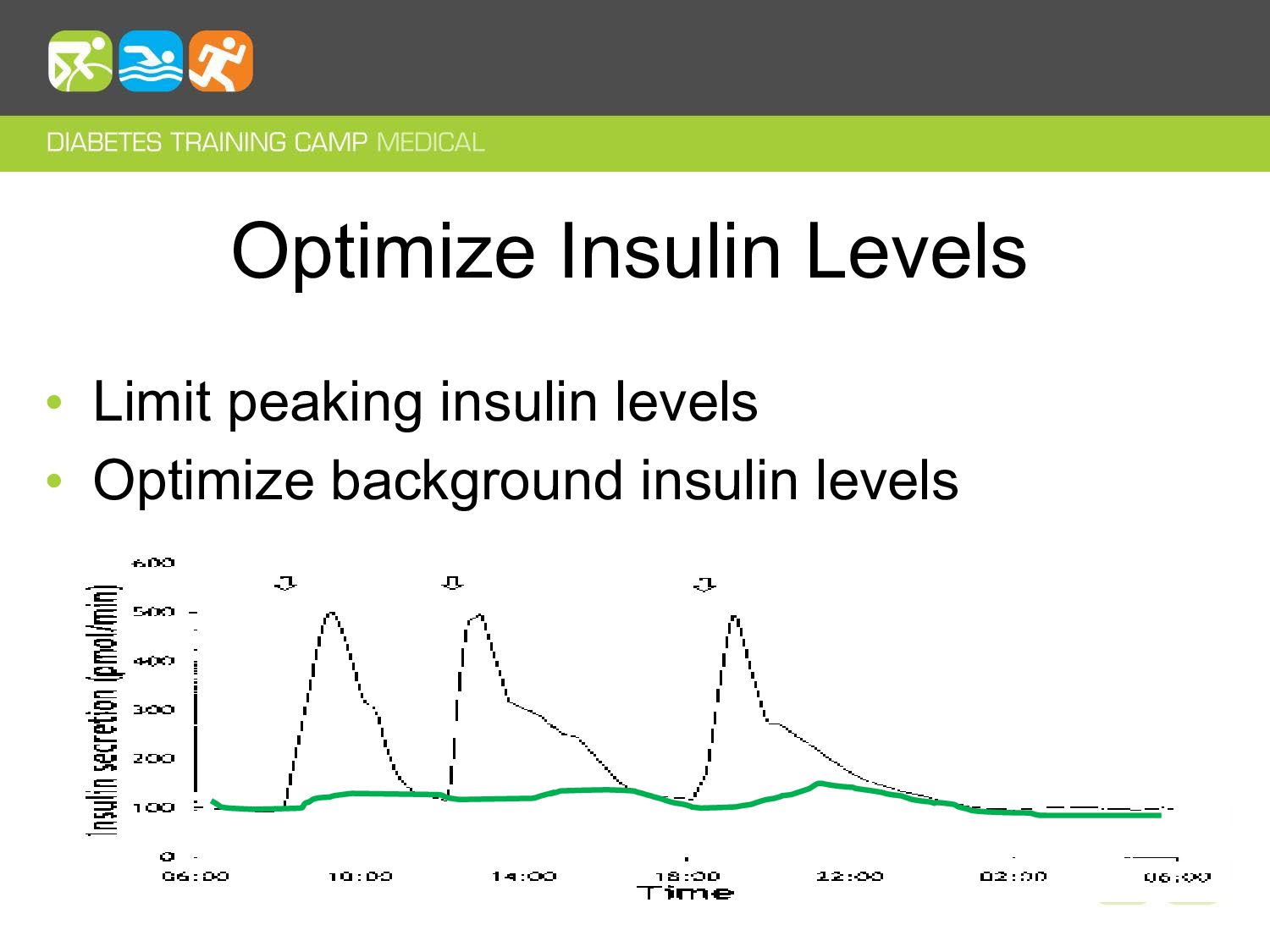
of our substrates for us to draw upon during times of need: fasting, sleep, physical activity, etc. • Insulin levels are steady and/or low during these times to allow for mobilization of stored fuels for brain function, muscular work, etc.
the level of physical activity that you are doing: • This limits: –ability to mobilize fuel stores –generate glucose as a substrate for the working muscle. –the body’s ability to keep up with the muscular glucose uptake during exercise.
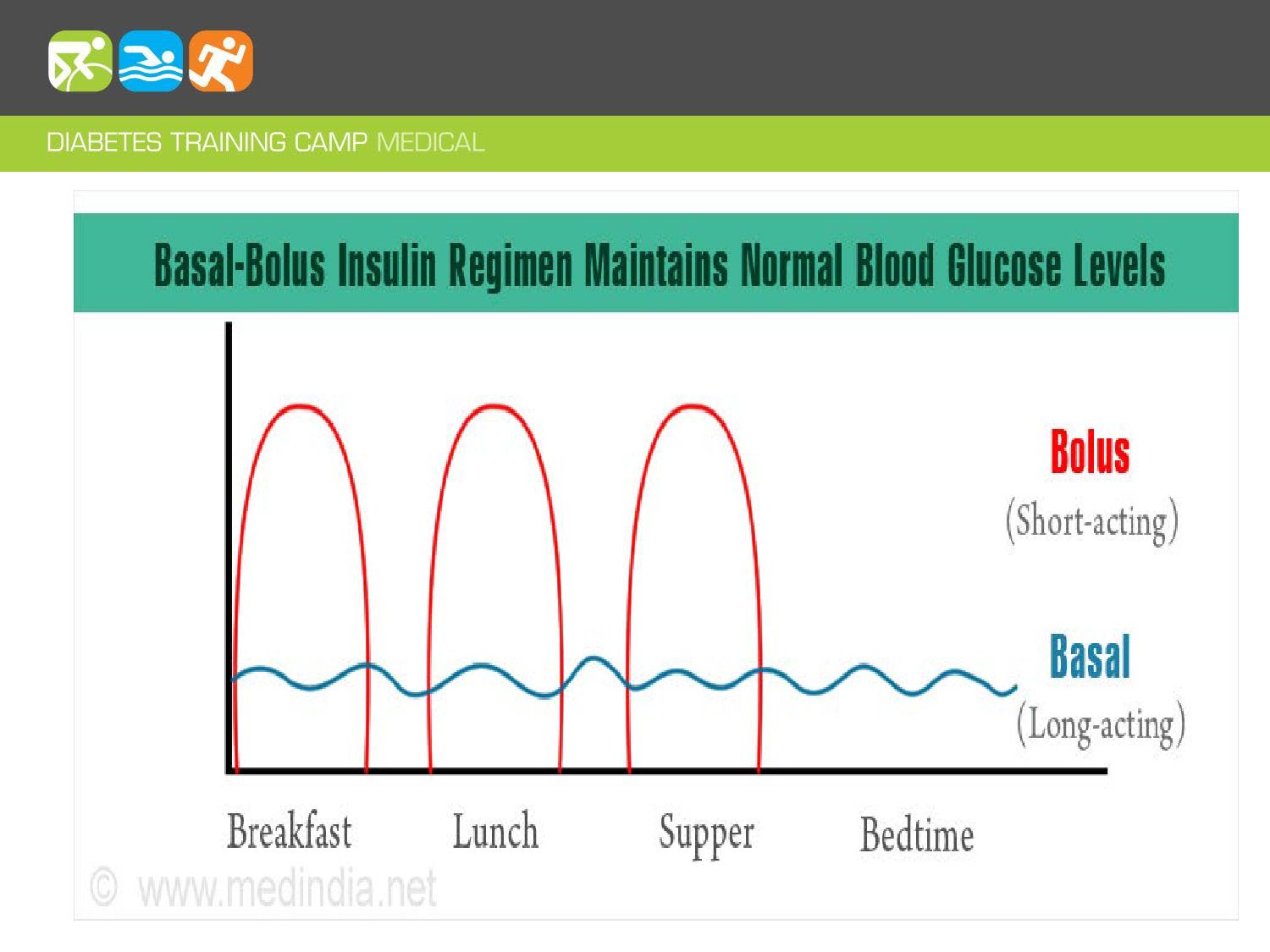
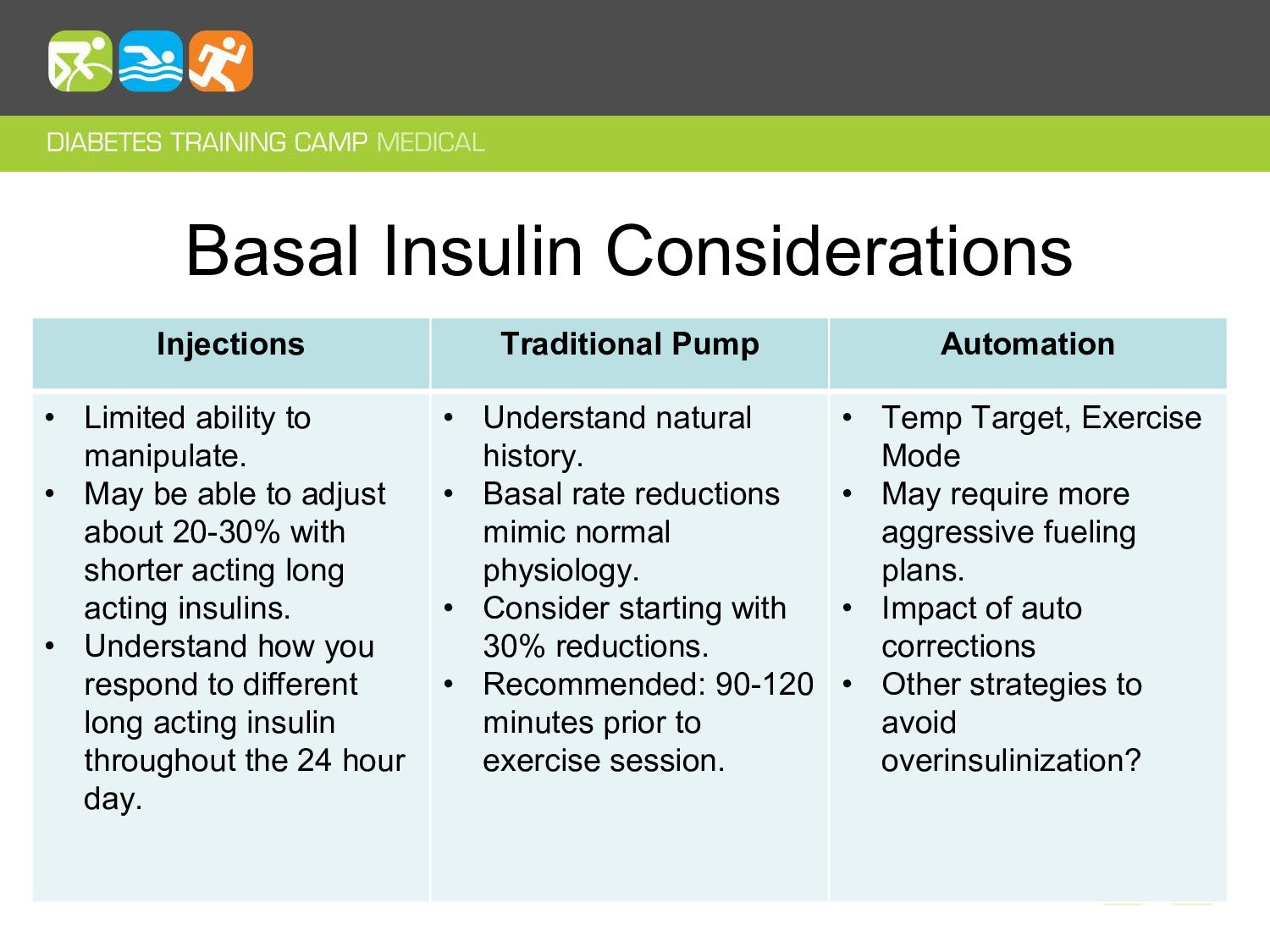
to manipulate. • May be able to adjust about 20-30% with shorter acting long acting insulins. • Understand how you respond to different long acting insulin throughout the 24 hour day. • Understand natural history. • Basal rate reductions mimic normal physiology. • Consider starting with 30% reductions. • Recommended: 90-120 minutes prior to exercise session. • Temp Target, Exercise Mode • May require more aggressive fueling plans. • Impact of auto corrections • Other strategies to avoid overinsulinization?
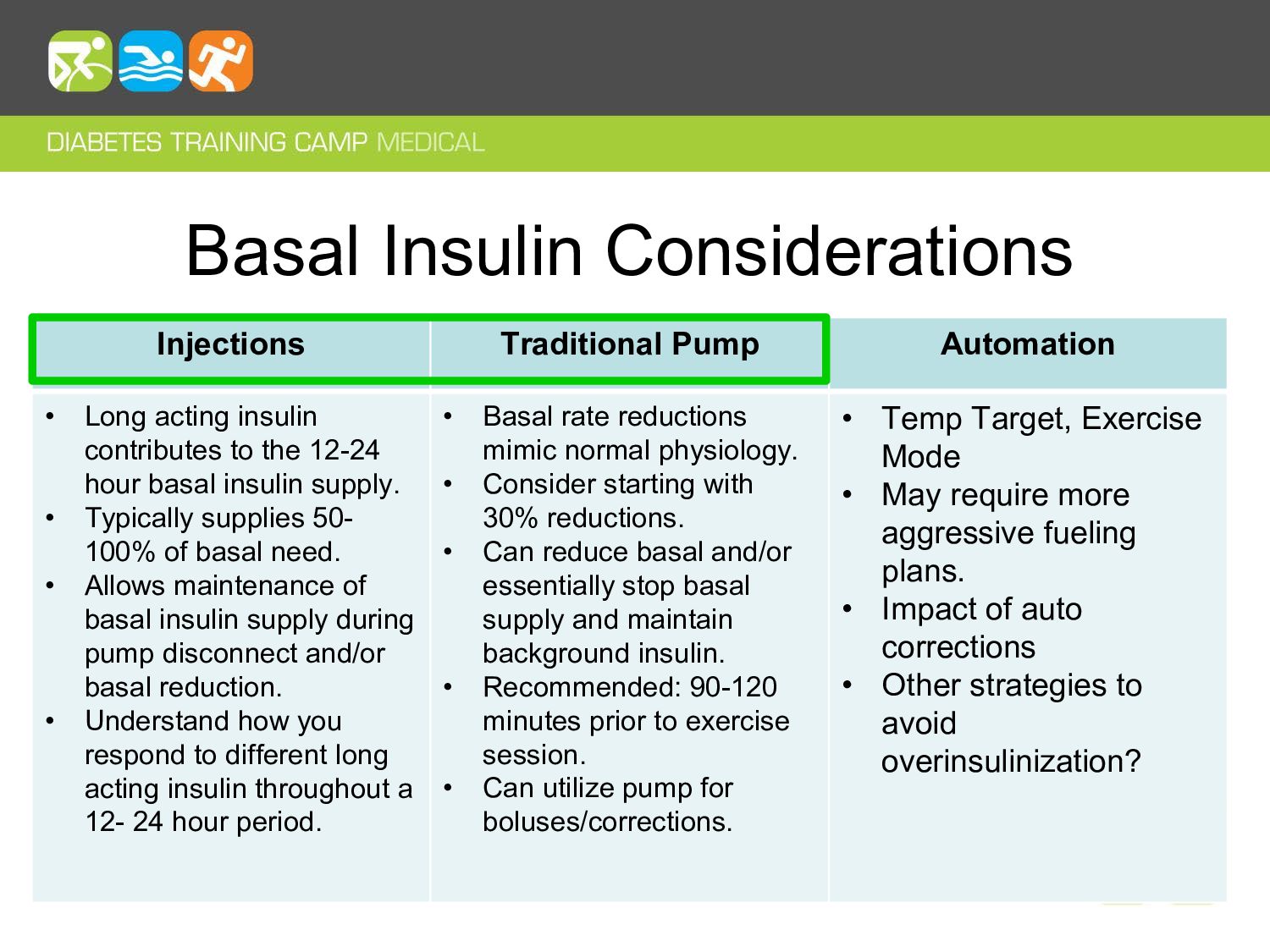
insulin contributes to the 12-24 hour basal insulin supply. • Typically supplies 50- 100% of basal need. • Allows maintenance of basal insulin supply during pump disconnect and/or basal reduction. • Understand how you respond to different long acting insulin throughout a 12- 24 hour period. • Basal rate reductions mimic normal physiology. • Consider starting with 30% reductions. • Can reduce basal and/or essentially stop basal supply and maintain background insulin. • Recommended: 90-120 minutes prior to exercise session. • Can utilize pump for boluses/corrections. • Temp Target, Exercise Mode • May require more aggressive fueling plans. • Impact of auto corrections • Other strategies to avoid overinsulinization?
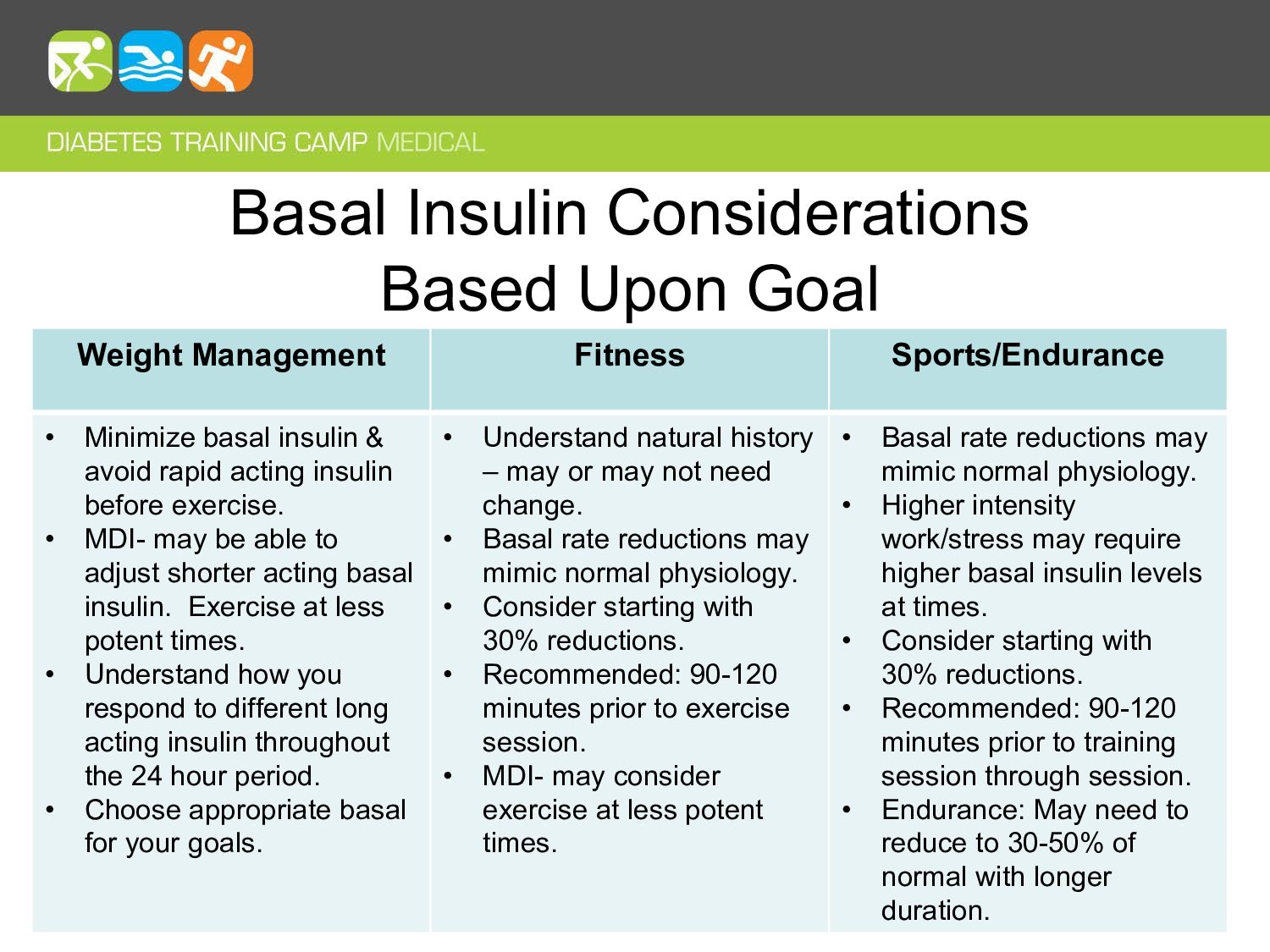
• Minimize basal insulin & avoid rapid acting insulin before exercise. • MDI- may be able to adjust shorter acting basal insulin. Exercise at less potent times. • Understand how you respond to different long acting insulin throughout the 24 hour period. • Choose appropriate basal for your goals. • Understand natural history – may or may not need change. • Basal rate reductions may mimic normal physiology. • Consider starting with 30% reductions. • Recommended: 90-120 minutes prior to exercise session. • MDI- may consider exercise at less potent times. • Basal rate reductions may mimic normal physiology. • Higher intensity work/stress may require higher basal insulin levels at times. • Consider starting with 30% reductions. • Recommended: 90-120 minutes prior to training session through session. • Endurance: May need to reduce to 30-50% of normal with longer duration.
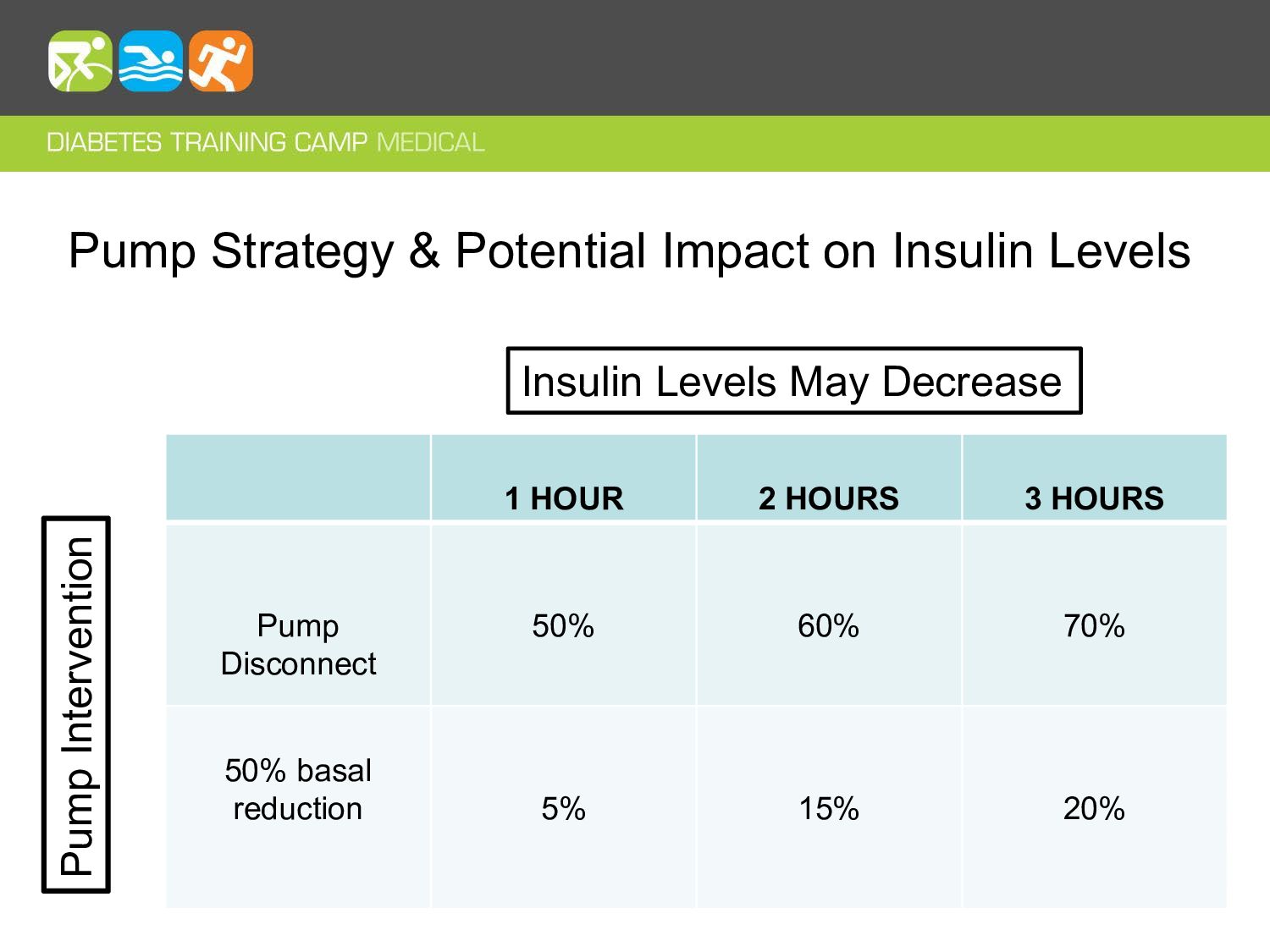
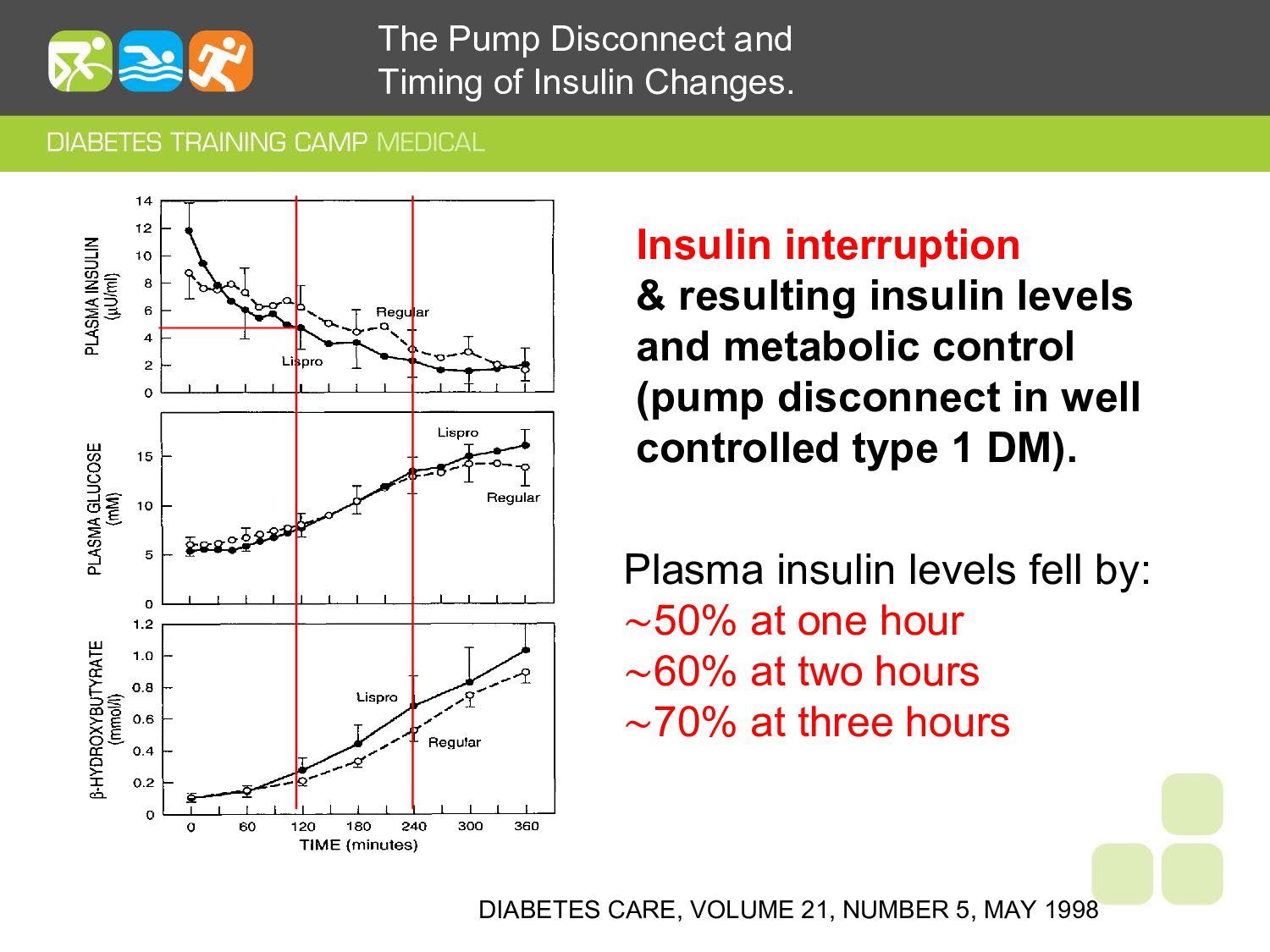
& resulting insulin levels and metabolic control (pump disconnect in well controlled type 1 DM). The Pump Disconnect and Timing of Insulin Changes. Plasma insulin levels fell by: ∼50% at one hour ∼60% at two hours ∼70% at three hours
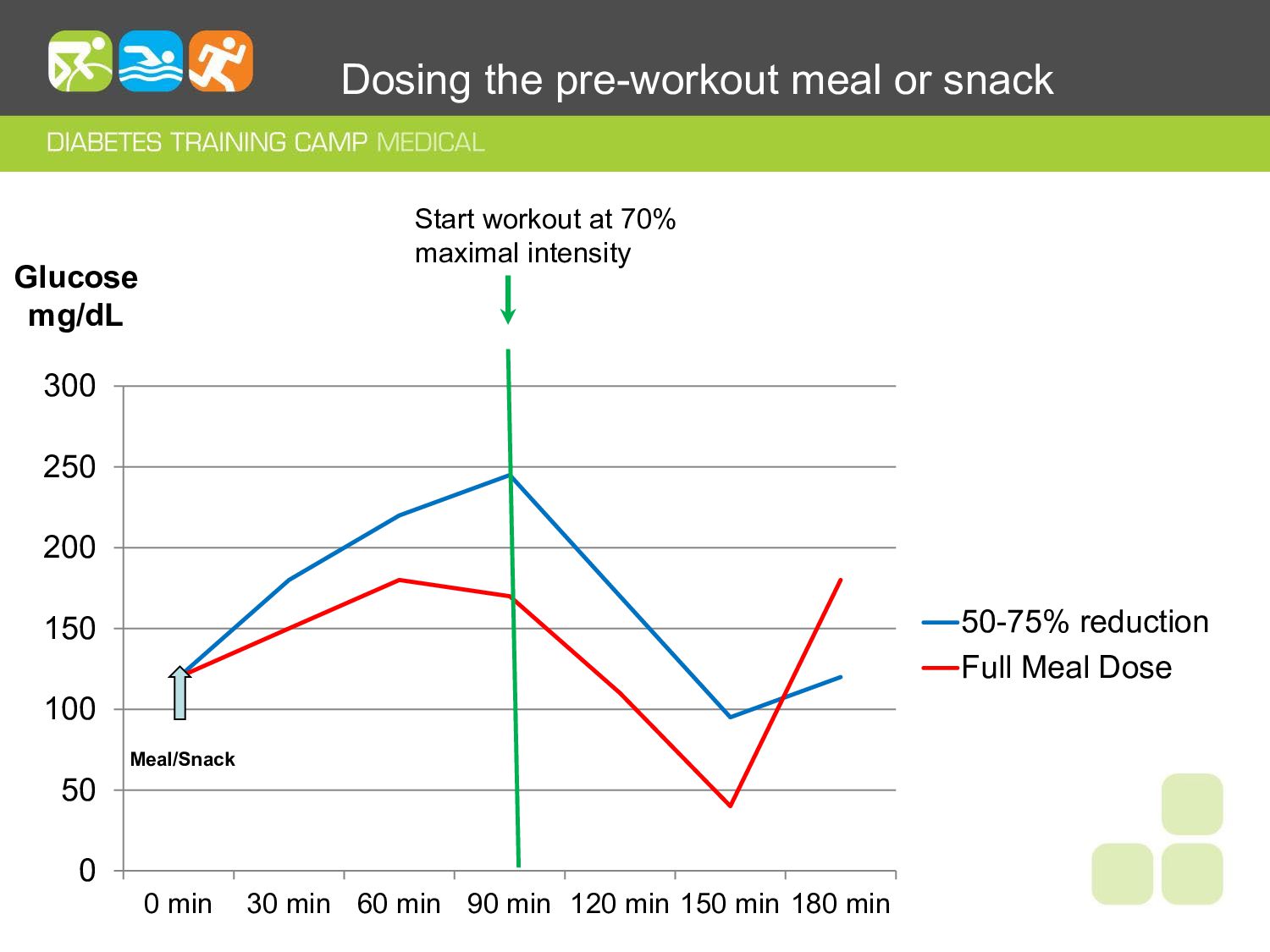
min 60 min 90 min 120 min 150 min 180 min 50-75% reduction Full Meal Dose Meal/Snack Start workout at 70% maximal intensity Glucose mg/dL Dosing the pre-workout meal or snack
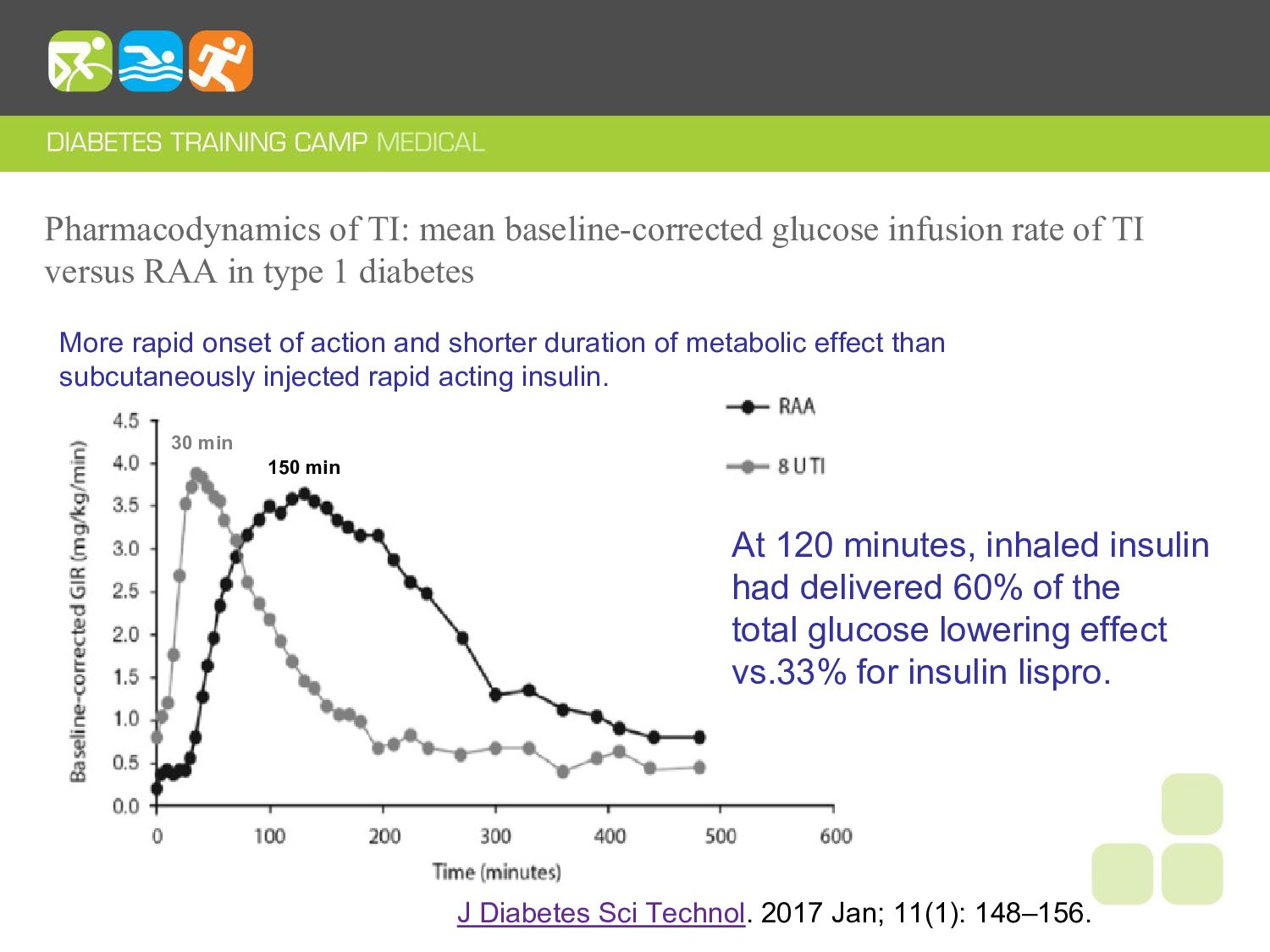
versus RAA in type 1 diabetes J Diabetes Sci Technol. 2017 Jan; 11(1): 148–156. More rapid onset of action and shorter duration of metabolic effect than subcutaneously injected rapid acting insulin. 30 min 150 min At 120 minutes, inhaled insulin had delivered 60% of the total glucose lowering effect vs.33% for insulin lispro.
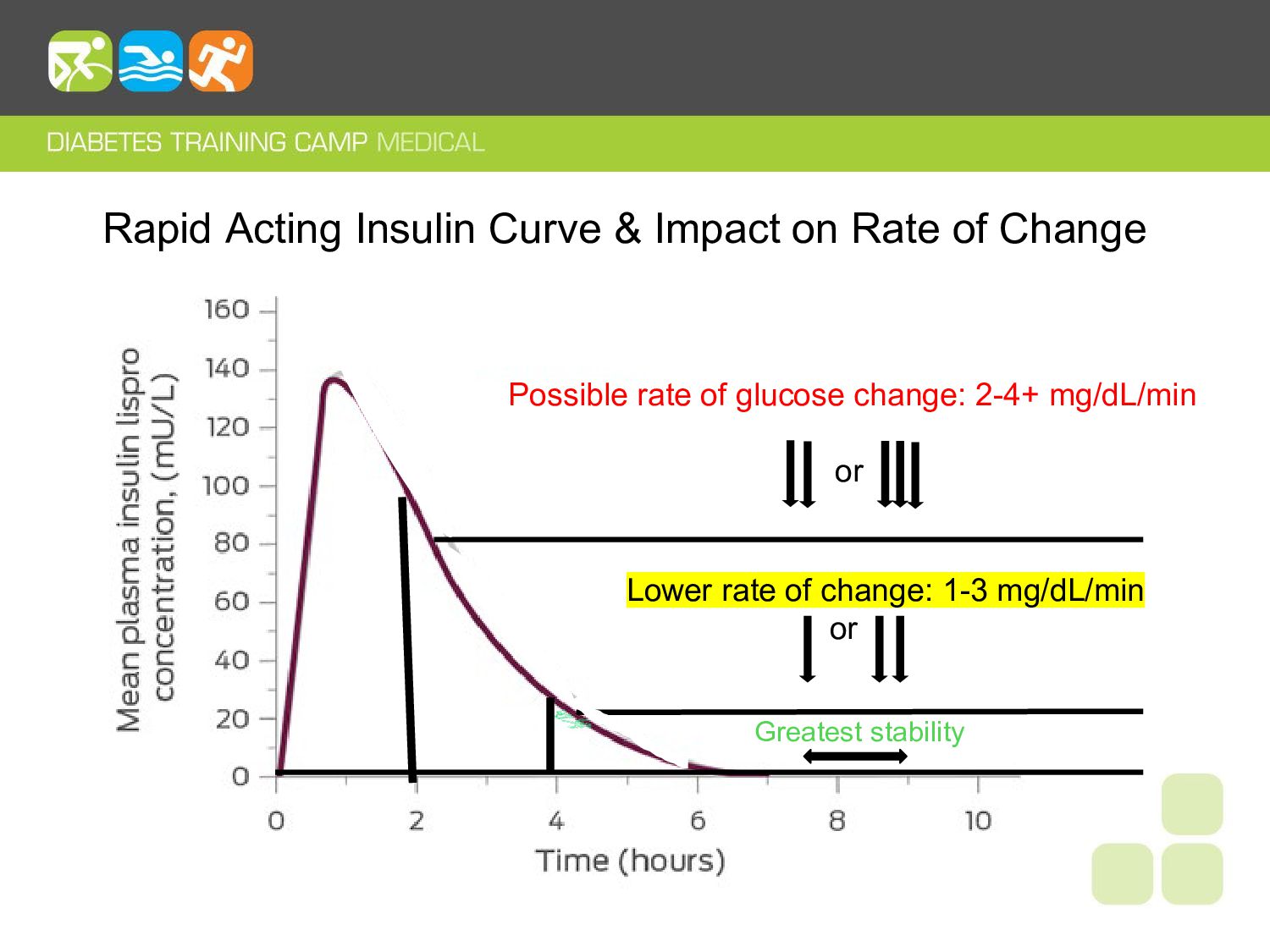
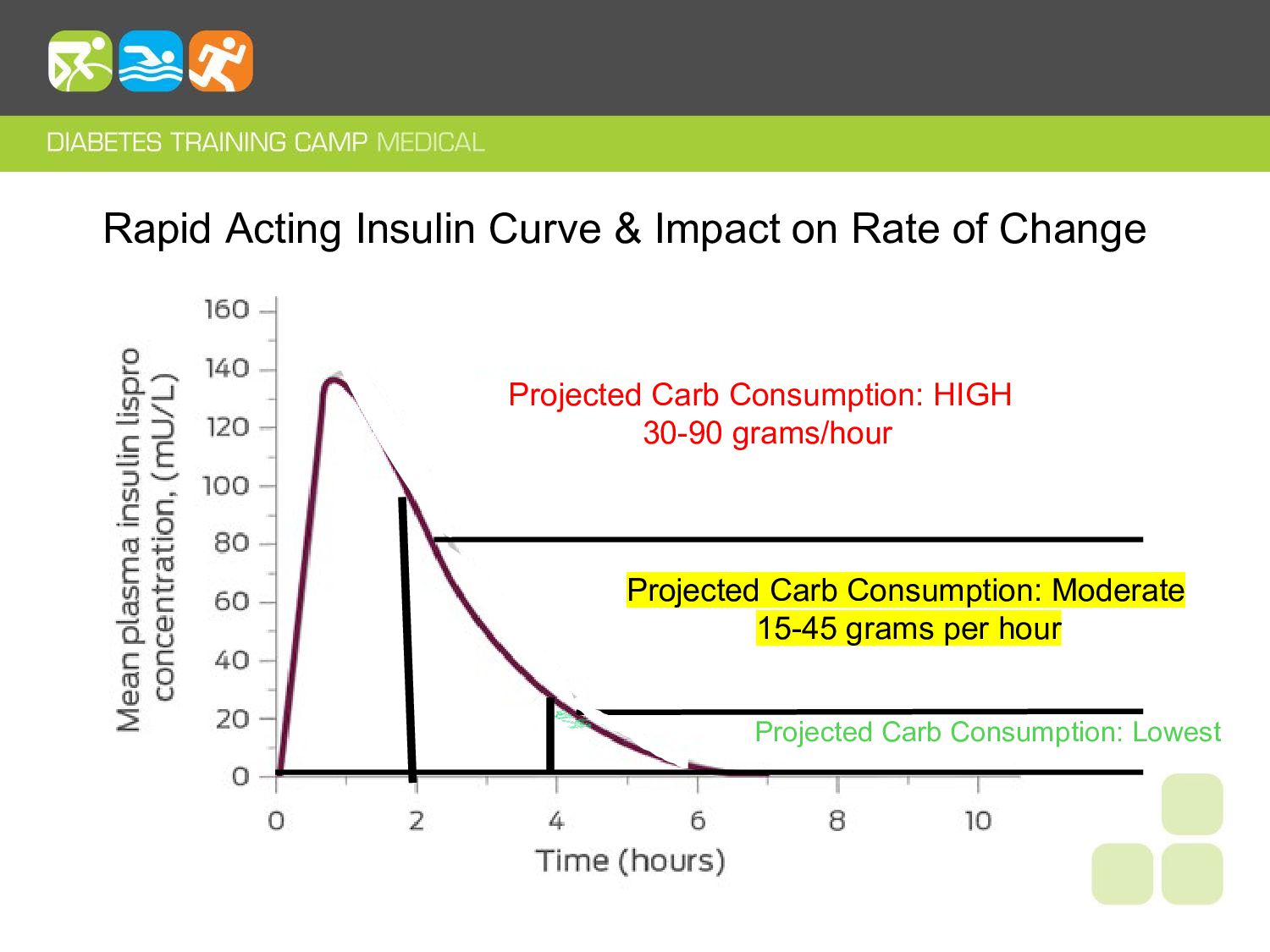
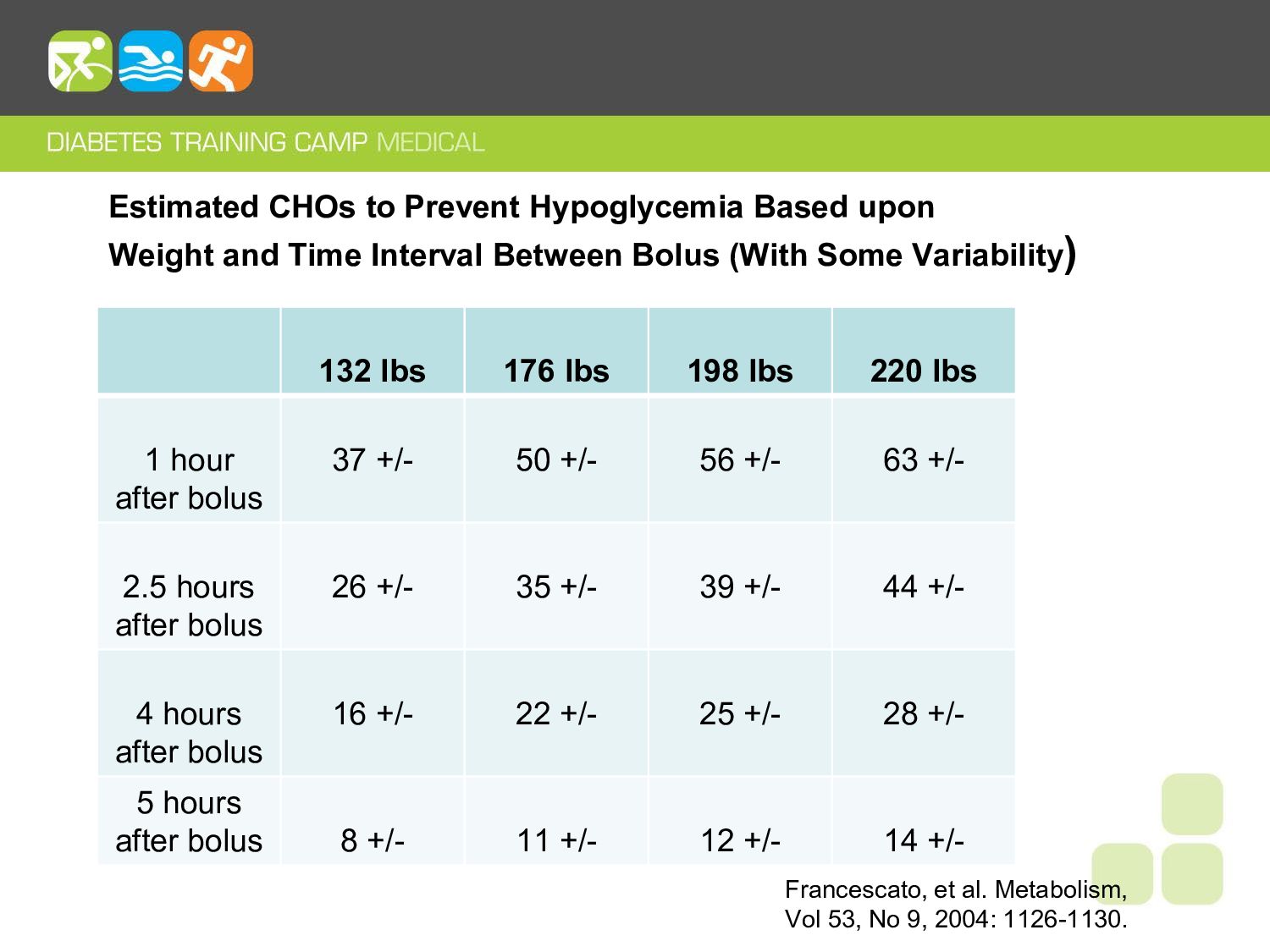
and consider starting conservatively. • Separate exercise and/or training and meal boluses by 3-4 hours, or more - Exercise in AM before breakfast and/or before meals. • If exercising within 1-2 hours of meal bolus, strongly consider 25-75% reduction depending upon duration and intensity. • Need for carbohydrate consumption will, in part, be based upon peaking insulin levels (IOB).
to simplify, minimize the variables & impact your performance and results: • Work out and train on basal insulin only as much as possible & 3 to 4 hours removed from rapid acting boluses. – Consider starting with 70% of normal basal insulin levels. • Minimize the action of rapid acting boluses/peaking insulin. • Utilize adequate carbohydrates to prevent hypoglycemia(as necessary) and/or fuel longer duration activities. • Avoid hypoglycemia as much as possible. Strive to stay above 70 mg/dl. Hypoglycemia is a vicious cycle and it will create havoc over the next 24 hours or more.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}