Trying to Balance Social Life, School, Family and Diabetes… this session will cover the hard topics that T1D teens face but rarely talk about. Learn how to help them survive the teen years.
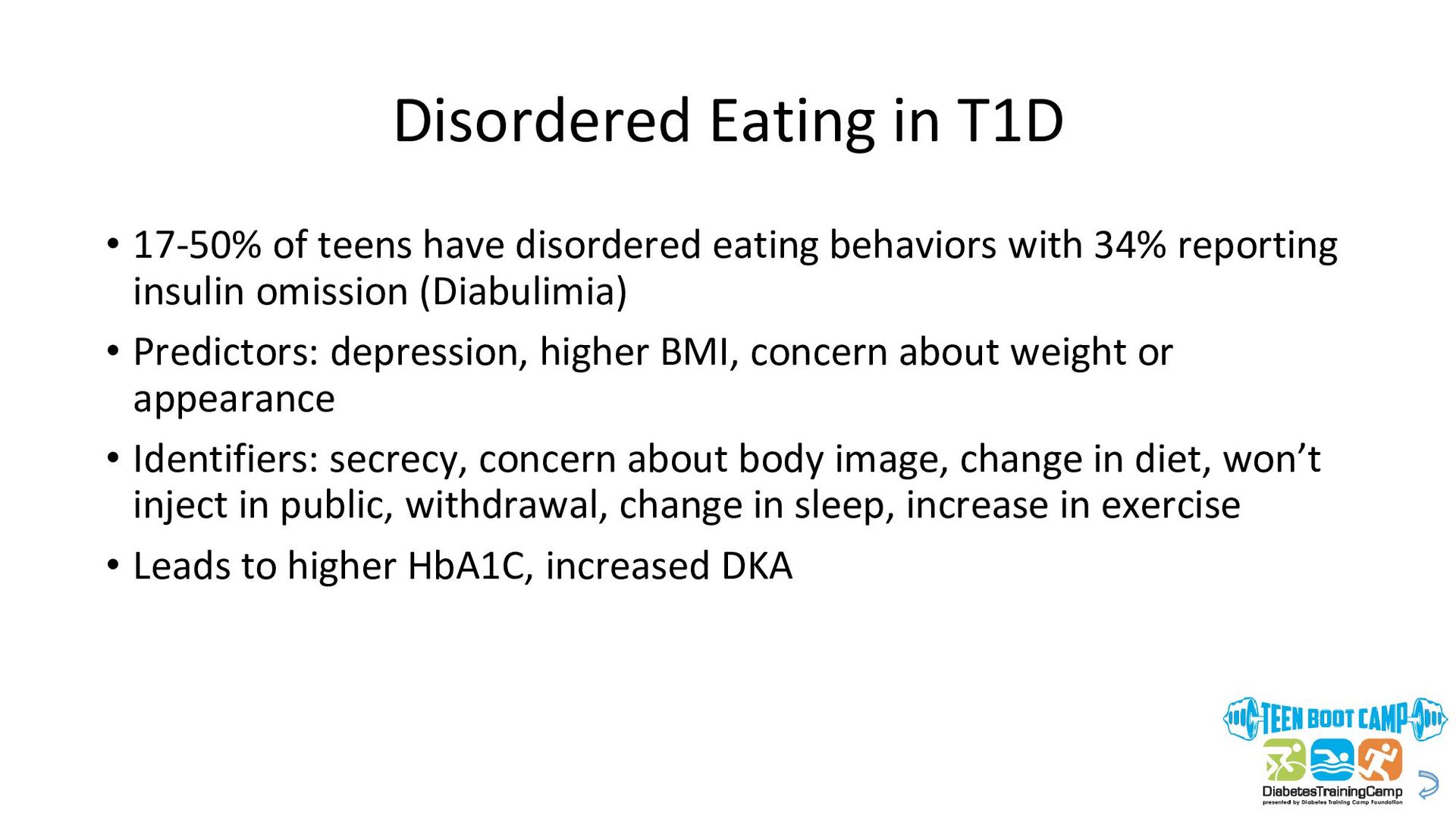
eating behaviors with 34% reporting insulin omission (Diabulimia) • Predictors: depression, higher BMI, concern about weight or appearance • Identifiers: secrecy, concern about body image, change in diet, won’t inject in public, withdrawal, change in sleep, increase in exercise • Leads to higher HbA1C, increased DKA
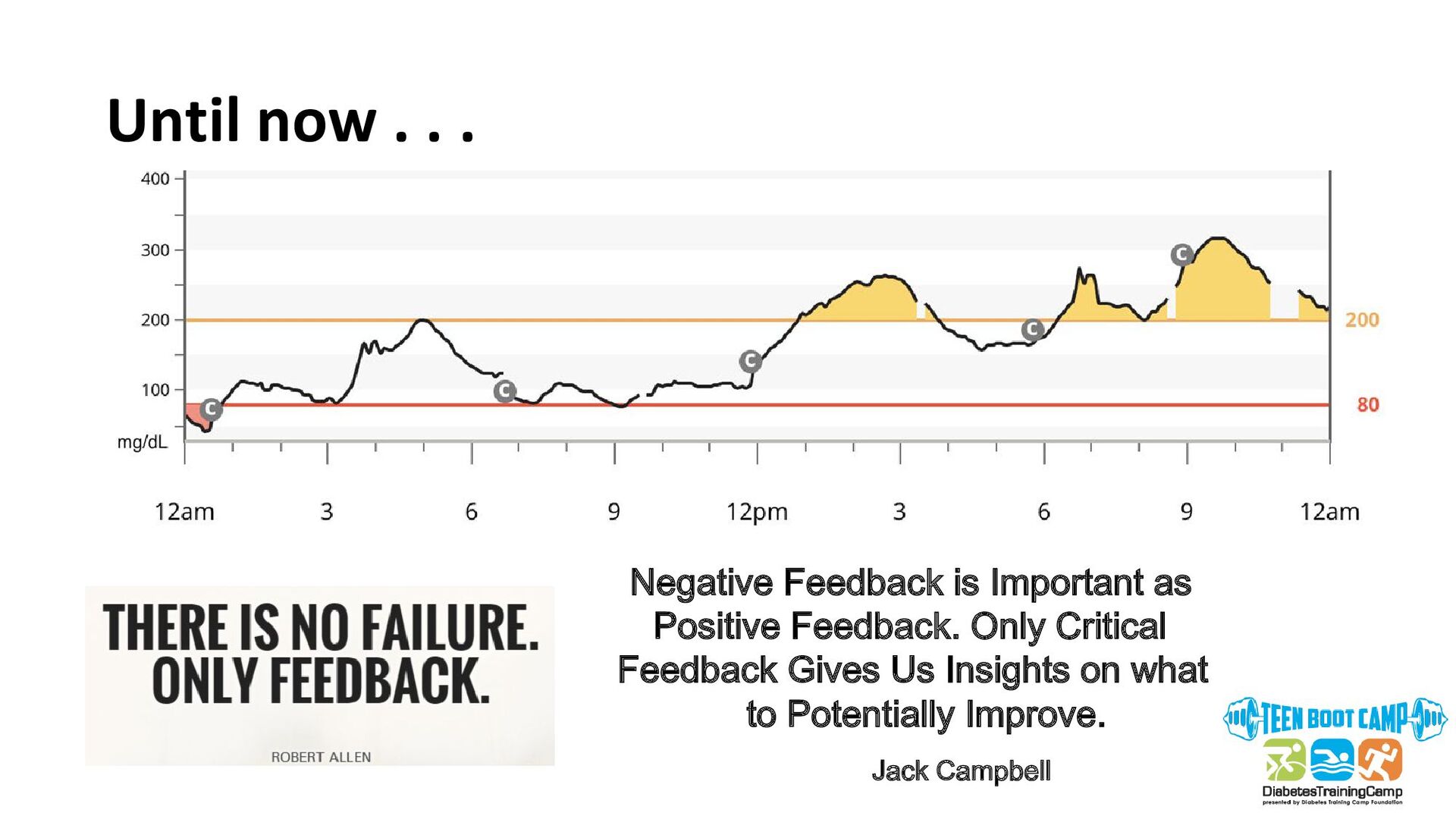
• HbA1C goes up • Decreased BG checks and possibly lying about this to parents • Diabetes vacation • Not doing site changes as often • Ignoring CGM alarms
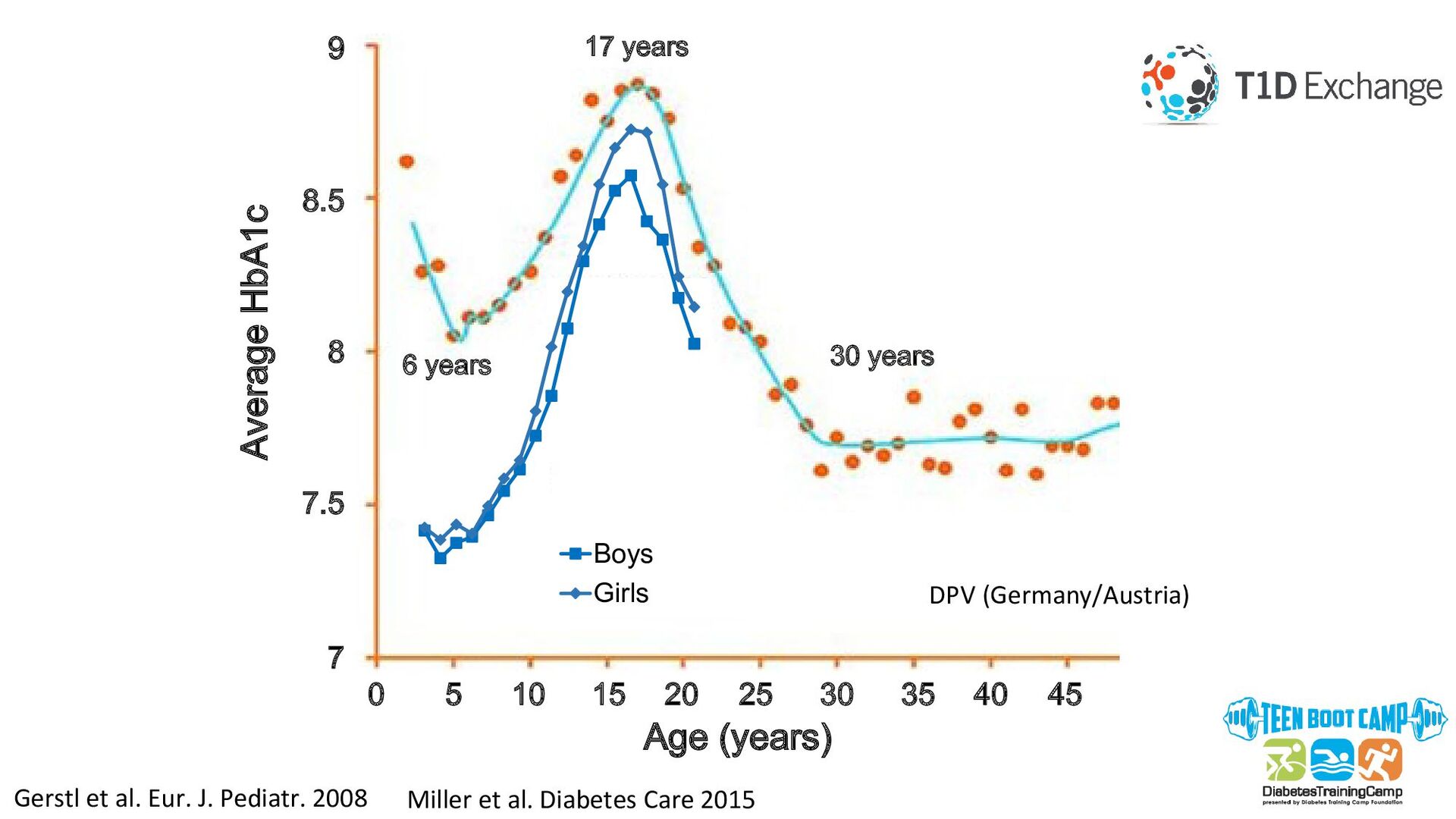
10 15 20 30 40 25 35 45 7 7.5 8 9 8.5 Average HbA1c Age (years) Miller et al. Diabetes Care 2015 DPV (Germany/Austria) Gerstl et al. Eur. J. Pediatr. 2008
• Notice the warning signs • Hit the RESET button • Ask for help • Control what you can • Be self-aware • Change things up • Acknowledgement goes a long way • Build in rewards
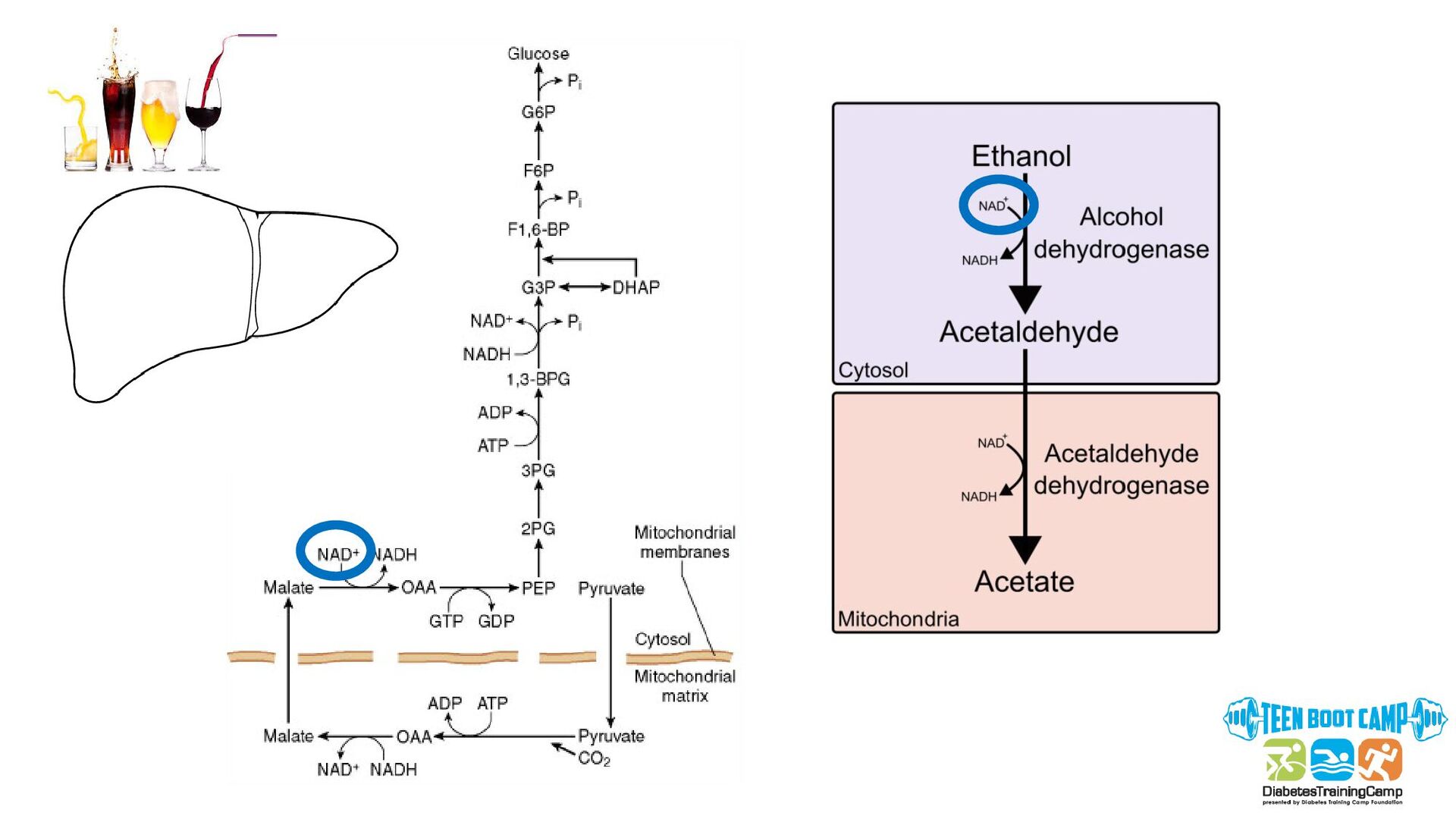
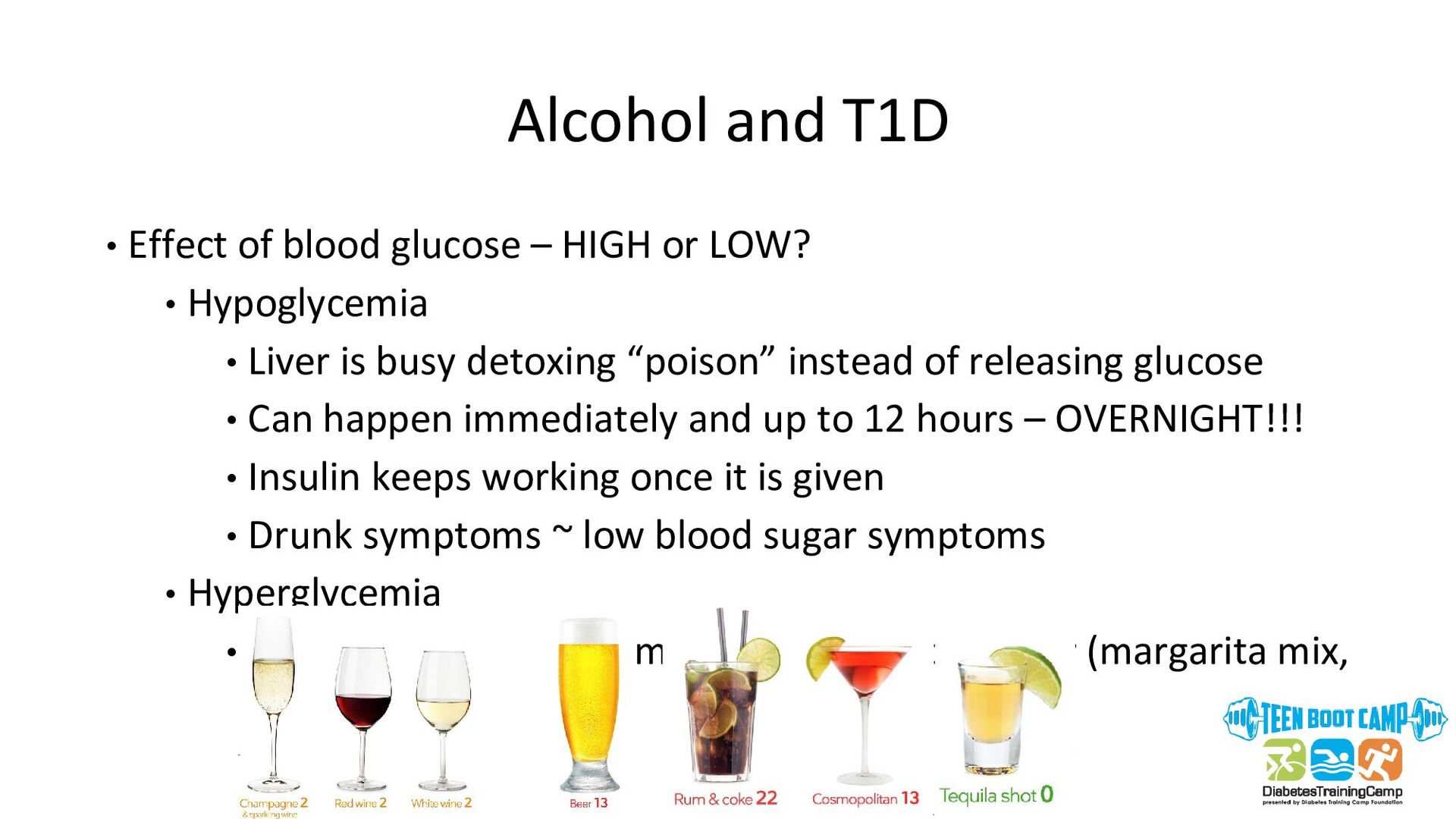
or LOW? • Hypoglycemia • Liver is busy detoxing “poison” instead of releasing glucose • Can happen immediately and up to 12 hours – OVERNIGHT!!! • Insulin keeps working once it is given • Drunk symptoms ~ low blood sugar symptoms • Hyperglycemia • Often sugar is used to make alcohol taste better (margarita mix, soda, etc.)
a T1D informed drinking buddy • DO NOT drink on an empty stomach – eat slow-acting carbs • Know your alcohol • Be prepared – BG meter or CGM, low BG treatment • Monitor BG before bed, overnight and first thing when waking up • Do not bolus for full amount of carbohydrates in a drink • Alternate alcoholic drinks with nonalcoholic drinks • Glucagon may not work well • Wear medical ID • Limit alcohol to help your brain reach it’s full potential and decrease changes for depression and addiction
• Risk of gastroparesis • No known effect on blood glucose control • Vaping • May increase HbA1c • May accelerate kidney damage • Nicotine exposure has many health consequences
the conversation before it happens – having “elevator speeches” ready can make life easier. http://www.jdrf.org/swo/wp-content/uploads/sites/12/2016/01/Talking-T1D.pdf
risks for motor vehicle accidents • Additional risk exists for teens with T1D due to risk of hypoglycemia • Personal driver’s license laws and required documentation vary by state: http://www.diabetes.org/living-with-diabetes/know-your- rights/discrimination/drivers-licenses/drivers-license-laws-by- state.html • Commercial licenses for interstate travel can be obtained with physician clearance (new law in 2018)
before and during drive • CGM is very useful for this • Never check glucose while driving – pull over •Do not drive if glucose is low – wait until >70 mg/dl •Always have treatment for a low glucose in the car (nonperishable) within an arm’s reach •Always wear medical alert/ID •NO driving while drinking
Consensus Guidelines recommend routine screening for psychological co-morbidities in youth with T1D, including depression. • Rate of depression, anxiety, sleep disorders is 2-3x that of teens without T1D • Depression in up to 30% of patients with T1D • Depressive symptomology is associated with increased HbA1c • ~ 20% of children and adolescents with T1D experience anxiety symptoms or have an anxiety disorder • Diabetes specific anxieties: • Insulin injections/infusions • Fear of hypoglycemia Depression and Anxiety
in appetite • Change in sleep • Loss of energy • Decreased concentration • Feelings of guilt or worthlessness • Recurrent thoughts of death or suicide • Change in grades • Increased irritability (in kids and teens) • High A1C • Not checking
. • Problems with sleep • Problems with focus/concentration • Checking BGs too much (>12 times/day) or too little (<4 times/day) • High HbA1c - consistent under-dosing • Over treating lows • Frequent visits to RN office at school • Panic attacks
• Parental support/family support is key but THERAPY is also KEY • Seek help early! • Therapy (CBT) allows family to learn coping skills, set expectations and learn strategies for integrating T1D in everyday life • Medication is sometimes required due to a hormonal imbalance
diagnosed T1D afraid of needles; 50% of these picked up by HCP • 10% of children fear blood sugar checks; 33% fear injections or changing insulin pump sets • Needle anxiety 🡪🡪 increased HbA1c • Often resolves, but some can be severe • Adaptive coping strategies (i.e. distraction) may be helpful
than fathers or adults with T1D • In adolescents, fear of hypoglycemia is associated with: • Frequency of hypoglycemic episodes • Hypoglycemia during school • Longer T1D duration • “Hypoglycemia avoidance behaviors” often used to prevent lows • Lack of interventions to treatment of fear of hypoglycemia
Confused. Angry. Fragile. Pathetic. On the verge of tears. Depressed. Anxious. Ready to give up. Annoying. I’m just a burden. Distant. Lonely. Bitter. Heartbroken. Crushed. I don’t know if I can do this. Defeated. Never good enough. Guilty. So tired. “How are you?” “Fine.”
much of this is covered? • Are there any resources to help? • How long can we see this doctor? • How/where do I fill prescriptions? • How can I get a sensor/pump? Dealing with the Diagnosis • Emotional impact • Guilt/shame: Did we/I do something wrong? Why my baby, why me??? • Overwhelmed with so much information at once (HbA1c, BG checks, insulin injections, carbohydrate counting, CGMs, pumps • Worry: Complications, will I die? Will we (the family) be ok? • Confusion: Why can’t I take a pill? Is it related to my weight?
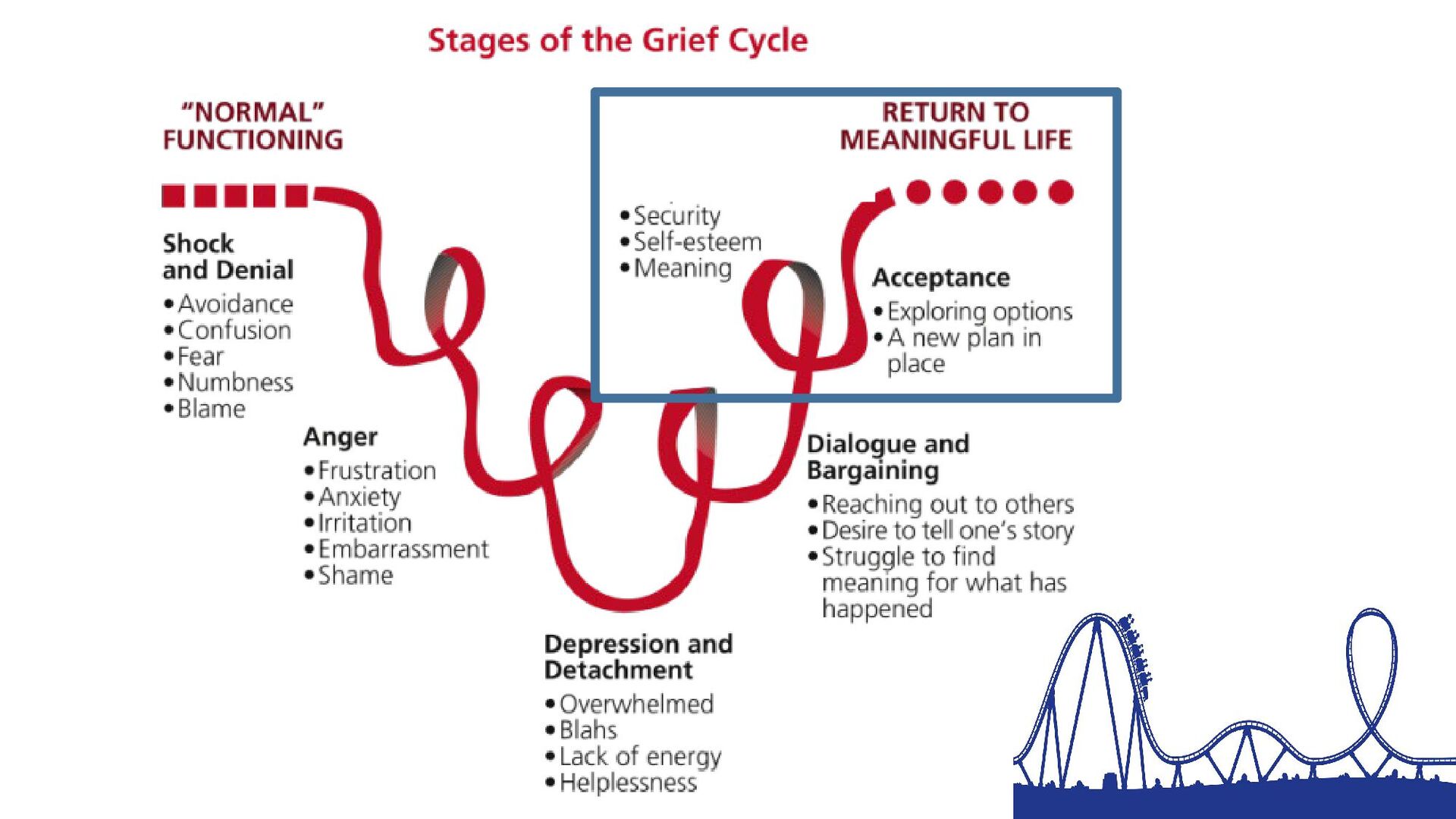
and diabetes impacts their lives in new and different ways, they will have a new grief response. Preschool School Age Tween Teen Slide courtesy B. Frohenrt, MD, PhD
varies with information disclosing • Letting people know about T1D can feel VERY vulnerable • What are some reasons why it is good to talk to others about your diabetes? • Who do you think you should talk to about your diabetes? Telling People can be Difficult
(accommodations at work or school) • People around you who know what to do if something is wrong • Closer relationships with people in your life • It builds trust, allows for support, allows you to talk and take care of diabetes more freely. • Less ignorance, more understanding
we want others to know and understand about T1D? • Create an “elevator speech” Brainstorm: What are creative ways that you can share with others about your Diabetes Story? Video, Snap Chat, Text, Drawing etc.
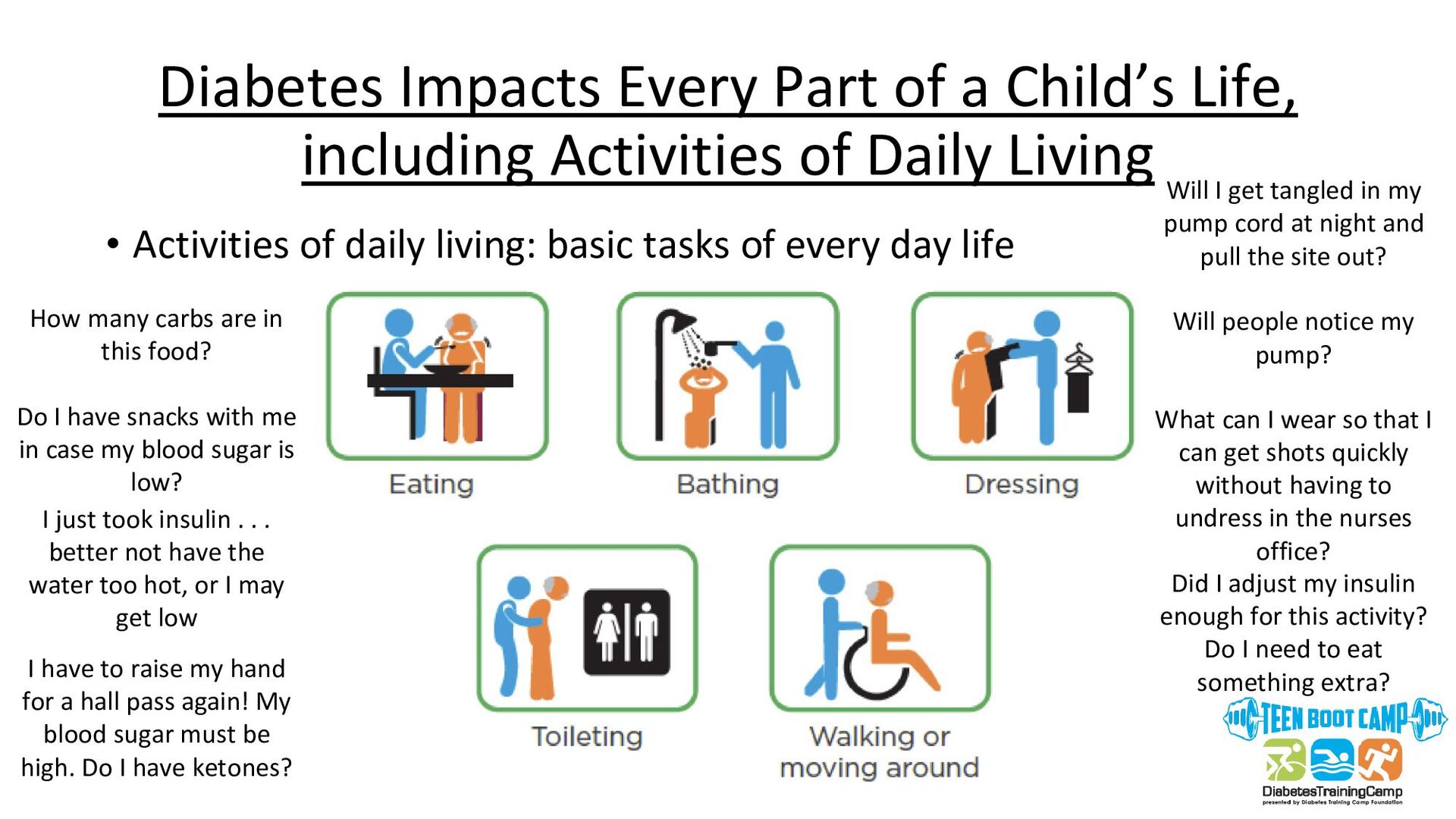
of Daily Living • Activities of daily living: basic tasks of every day life How many carbs are in this food? Do I have snacks with me in case my blood sugar is low? Will I get tangled in my pump cord at night and pull the site out? Will people notice my pump? What can I wear so that I can get shots quickly without having to undress in the nurses office? I just took insulin . . . better not have the water too hot, or I may get low I have to raise my hand for a hall pass again! My blood sugar must be high. Do I have ketones? Did I adjust my insulin enough for this activity? Do I need to eat something extra?
have T1D? • How do you tell someone that you have T1D? • How do you explain type 1 versus 2? • Do you take your pump off when intimate? • How long can you take it off? • Pregnancy must be planned – contraception is A MUST Relationships and Dating
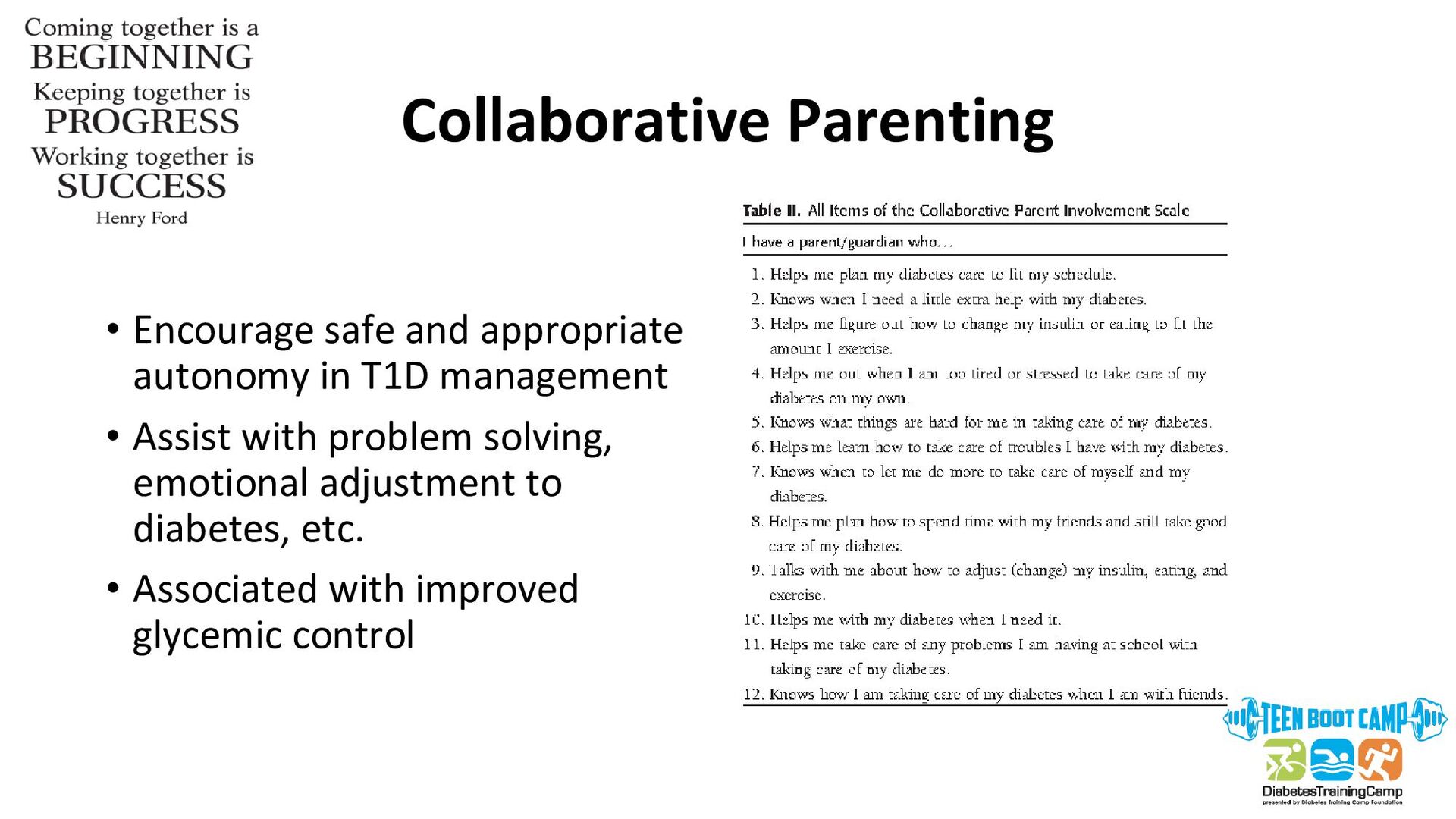
• Parent’s expect teens to take over more control and parent’s participation in management often decreases 🡪🡪 higher HbA1c, more family conflict • Family conflict higher in Type 1 Diabetes vs general population • Predicts low quality of life, suboptimal glycemic control, more depressive symptoms
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}