Saturation Target Range for Extremely Preterm Infants Manja V, Lakshminrusimha S, Cook DJ. Oxygen saturation target range for extremely preterm infants: a systematic review and meta- analysis. JAMA Pediatr. Published online February 9, 2015. doi: 10.1001/jamapediatrics.2014.3307.
oxygen saturation (SpO2 ) target for extremely preterm infants has been the focus of 5 randomized clinical trials (Surfactant, Positive Pressure, and Oxygenation Randomized Trial [SUPPORT], Benefits of Oxygen Saturation Targeting II [BOOST II] in the United Kingdom, Australia, and New Zealand, and Canadian Oxygen Trial [COT]). • Study Objective – To assess whether targeting a lower SpO2 range (85%-89% restricted oxygen) has an effect on mortality and severe disability, mortality alone, bronchopulmonary dysplasia, neurodevelopmental outcome, hearing loss, necrotizing enterocolitis, or severe retinopathy of prematurity compared with targeting a higher SpO2 range (91%-95% liberal oxygen) after accounting for the risk of bias of each included study as well as the quality of evidence for each outcome. • Study Design – Meta-analysis and systematic review. Introduction
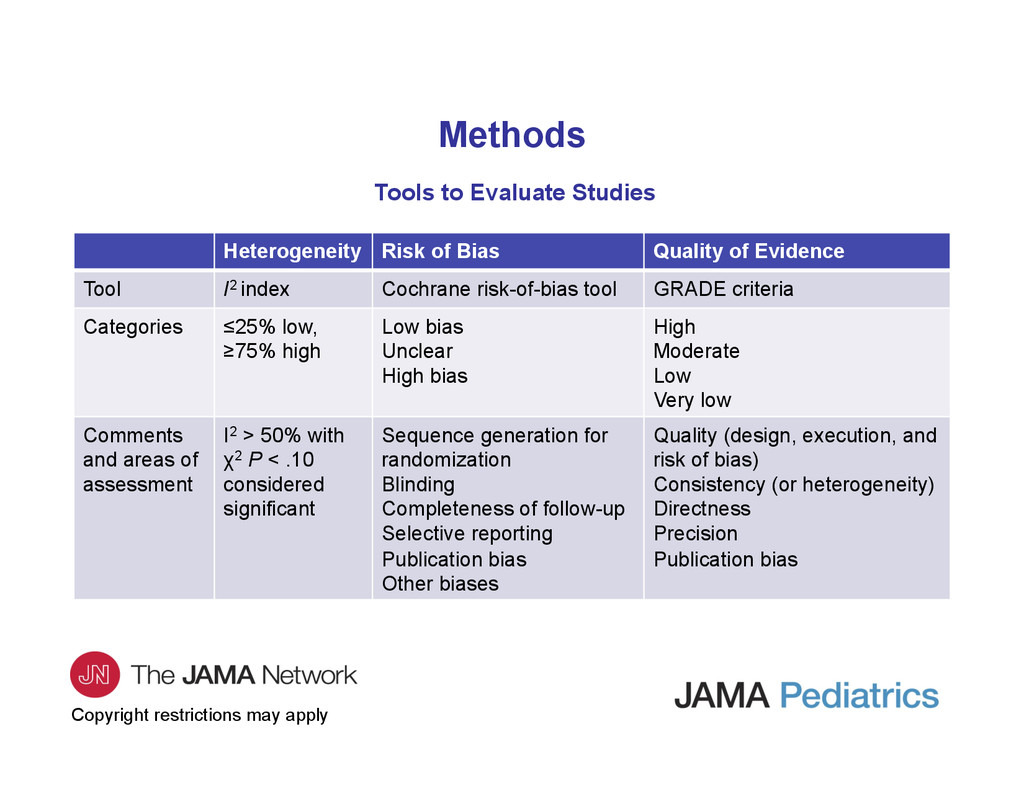
of Bias Quality of Evidence Tool I2 index Cochrane risk-of-bias tool GRADE criteria Categories ≤25% low, ≥75% high Low bias Unclear High bias High Moderate Low Very low Comments and areas of assessment I2 > 50% with χ2 P < .10 considered significant Sequence generation for randomization Blinding Completeness of follow-up Selective reporting Publication bias Other biases Quality (design, execution, and risk of bias) Consistency (or heterogeneity) Directness Precision Publication bias Methods
treatment effect and equal weight is given to each subject (large study, proportionately larger weight in meta- analysis). • Random-effects model incorporates between-study variance. If a group of studies is homogeneous, fixed-effect and random-effects study-specific weights are equal. With increasing heterogeneity, the 2 weights will become increasingly different. • Random-effects model was chosen to analyze results in this study because – The goal was to estimate the mean effect in all studies and not let the overall estimate be overly influenced by 1 study. – These studies were performed by different researchers using similar outlines but operating independently. – These studies are not functionally equivalent due to variability in patients, protocols (pulse oximeter algorithms). – Random-effects model is more suitable to generalize results to a range of clinical scenarios. Methods
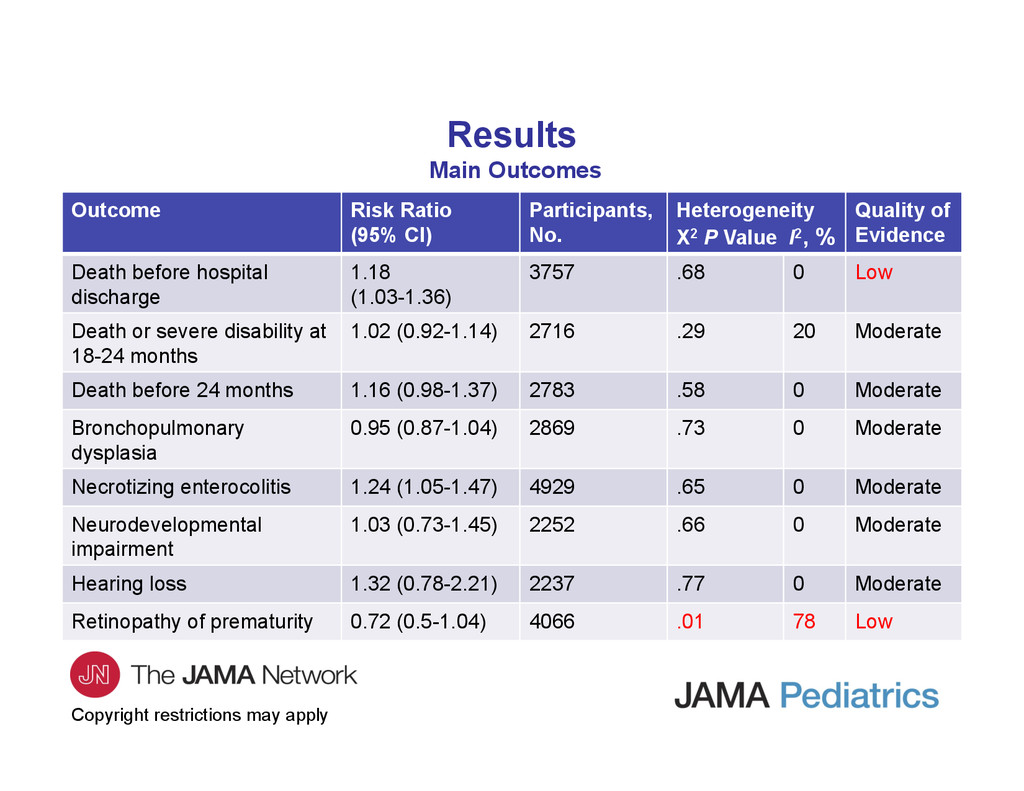
was statistically significantly higher in the restricted oxygen group (risk ratio = 1.18; 95% CI, 1.03-1.36). This was not a prespecified outcome in any of the studies. • Necrotizing enterocolitis occured more frequently in the restricted oxygen group (risk ratio = 1.24; 95% CI, 1.05-1.47). • There was no significant difference in the outcomes of death or disability before age 2 years, death before 24 months, bronchopulmonary dysplasia, hearing loss, and retinopathy of prematurity. • The quality of evidence was low for the outcomes of death before hospital discharge and retinopathy of prematurity. It was moderate for all other outcomes.
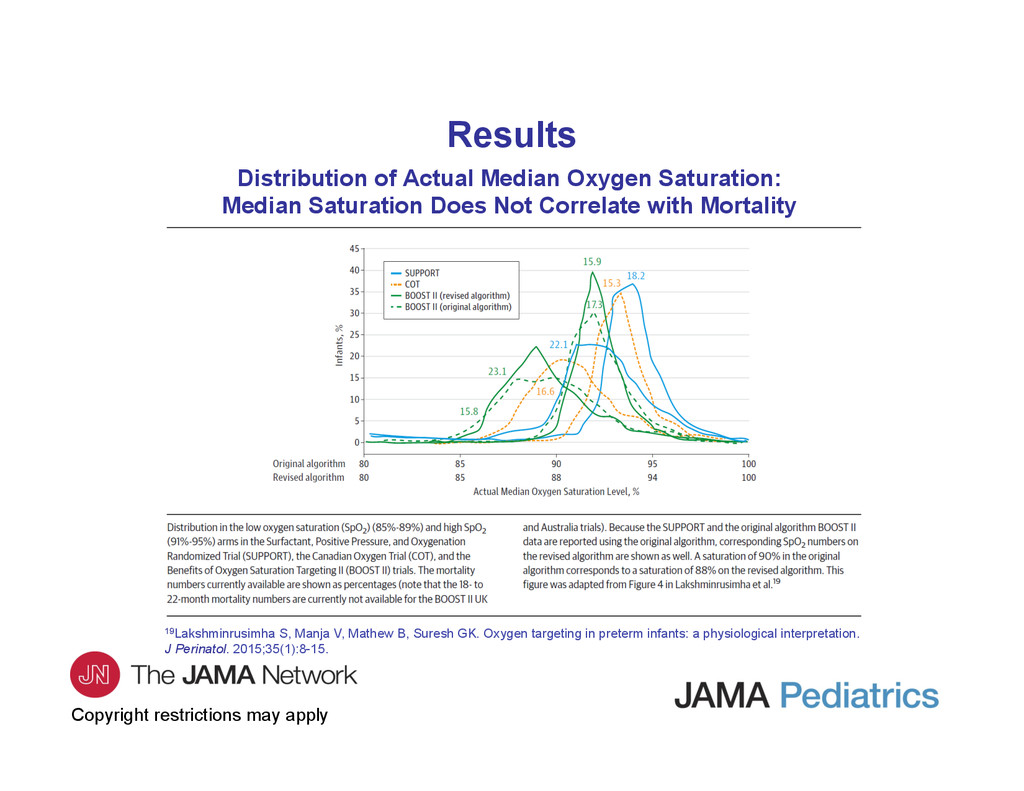
Median Saturation Does Not Correlate with Mortality 19Lakshminrusimha S, Manja V, Mathew B, Suresh GK. Oxygen targeting in preterm infants: a physiological interpretation. J Perinatol. 2015;35(1):8-15. Results
the importance of assessing the risk of bias in studies and of the level of confidence in the estimate of effect of each outcome. • Although SUPPORT, BOOST II, and COT were well-designed and mostly well-executed studies, the significant overlap in oxygenation between the intervention and comparator arms makes it difficult to conclude that the results obtained were predominantly due to difference in oxygenation. • Death before hospital discharge was not a prespecified outcome in any of these trials. The confidence in this outcome is lower for this reason. • Significant heterogeneity existed between studies for the outcome of retinopathy of prematurity, resulting in lowering of the level of confidence for the estimate of effect for this outcome.
factors that need to be considered before making treatment recommendations based on systematic reviews of available literature. • The assessment of quality of evidence can be subjective; however, using GRADE, the rationale for the quality assessment is clearly stated and the subjective nature of this process acknowledged. • This review reveals that there continues to be significant uncertainty about the optimal target range for SpO2 in extremely preterm infants. This is in contrast to previous reviews, which did not consider the quality of evidence in their final evaluation. • Information from the planned prospective individual-patient meta-analysis and practical considerations (difficulty in maintaining SpO2 in a narrow range) should be included when making practice recommendations. Conclusions
contact the corresponding author: – Satyan Lakshminrusimha, MD, Division of Neonatal-Perinatal Medicine, Department of Pediatrics, Women and Children’s Hospital of Buffalo, 219 Bryant St, Buffalo, NY 14222 ([email protected]). Funding/Support • This work was supported by grant 5 R01 HD072929 (optimal oxygenation in neonatal lung injury) (Dr Lakshminrusimha). Conflict of Interest Disclosures • Dr Lakshminrusimha was a member of the speaker’s bureau for Ikaria LLC. No other disclosures are reported. Contact Information
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}