These slides concern more issues about performing and interpretation of F-18 FDG PET/CT scan, including patient preparation, techniques, normal and normal variants, as well as pitfalls in interpretation.
Imaging Technique ◦ Patient Preparation ◦ Imaging Protocol Interpretation and Reporting ◦ Normal and Normal Variants vs Pathologic Findings ◦ Pitfalls & Artifacts
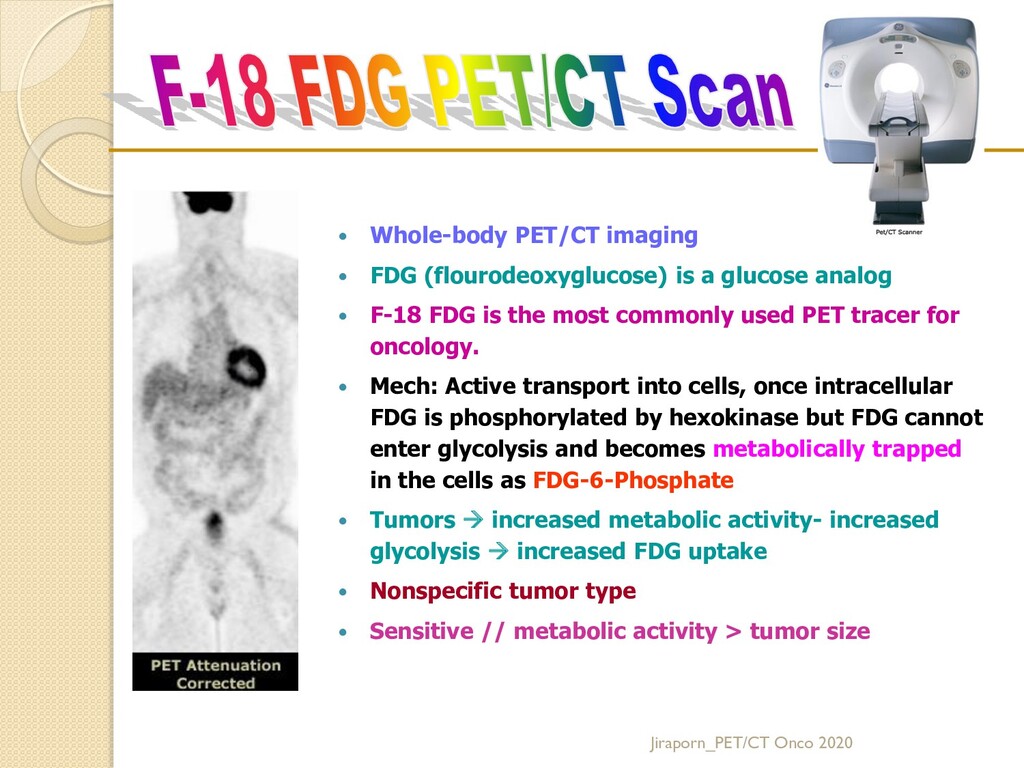
analog F-18 FDG is the most commonly used PET tracer for oncology. Mech: Active transport into cells, once intracellular FDG is phosphorylated by hexokinase but FDG cannot enter glycolysis and becomes metabolically trapped in the cells as FDG-6-Phosphate Tumors increased metabolic activity- increased glycolysis increased FDG uptake Nonspecific tumor type Sensitive // metabolic activity > tumor size Jiraporn_PET/CT Onco 2020
Dominique Delbeke, R. Edward Coleman, Milton J. Guiberteau, et al. J Nucl Med Vol. 47 No. 5 885-895, 2006 http://snmmi.files.cms-plus.com/docs/jnm30551_online.pdf Jiraporn_PET/CT Onco 2020
I. PURPOSE II. BACKGROUND INFORMATION AND DEFINITIONS III. EXAMPLES OF CLINICAL OR RESEARCH APPLICATIONS IV. PROCEDURE A. Patient preparartion B. Information Pertinent to Performing Procedure C. Precautions D. Radiopharmaceutical E. Image acquisition F. Interventions G. processing H. Interpretation: Normal physiologic distribution I. Reporting J. QC K. Sources of errors: Normal Variants, pitfalls & artifacts V. QUALIFICATION OF PERSONNELS VI.ISSUESREQUIRINGFURTHERCLARIFICATION Jiraporn_PET/CT Onco 2020
FDG PET/CT include: 1. Differentiating benign from malignant lesions 2. Searching for an unknown primary tumor when metastatic disease is discovered as the first manifestation of cancer or when the patient presents with a paraneoplastic syndrome 3. Staging known malignancies 4. Monitoring the effect of therapy on known malignancies 5. Determining whether residual abnormalities detected after treatment represent residual tumor or posttreatment fibrosis or necrosis 6. Detecting tumor recurrence, especially in the presence of elevated levels of tumor markers 7. Selecting the region of a tumor for biopsy 8. Guiding radiation therapy planning 9. F-18 FDG PET/CT is not equally effective for all malignancies, but other tracers are available. 10. Non-oncologic applications, such as evaluation of infection and atherosclerosis Jiraporn_PET/CT Onco 2020
minimize tracer uptake in normal tissues, such as the myocardium and skeletal muscle, while maintaining uptake in target tissues (neoplastic disease). 1. Before arrival a) Avoid strenuous activity at least 24 hours before PET scan b) Fast and do not consume beverages, except for water, for at least 4–6 h before the administration of F-18 FDG to decrease physiologic glucose levels and to reduce serum insulin levels to near basal levels. c) Oral hydration with water is encouraged. d) IV fluids containing dextrose or parenteral feedings also should be withheld for 4–6 h. e) IV contrast material should not be administered if serum creatinine > 2.0 mg/dL. Jiraporn_PET/CT Onco 2020
the patient should be in a quiet and dimly lit room since the injection throughout the uptake phase. b) For body imaging, the patient should remain seated or recumbent since the injection throughout uptake phase to avoid muscular uptake. c) Check blood glucose level Tumor uptake of 18F-FDG is reduced in hyperglycemic states. Most institutions reschedule the patient if the blood glucose level is greater than 150–200 mg/dL. Reducing the serum glucose level by administering insulin can be considered, but the administration of 18F-FDG should be delayed after insulin administration (duration of the delay depends on the type and route of administration of insulin). d) For CT scan, an intraluminal GI contrast agent may be administered for better visualization of the GI tract unless it is medically C/I or unnecessary for the clinical indication (see Section E.2.b.). Jiraporn_PET/CT Onco 2020
and site of cancer, dates of diagnosis and treatment (biopsy results, surgery, radiation, chemotherapy, and administration of bone marrow stimulants and steroids), and current medications. 2. History of diabetes, fasting state, and recent infection 3. Patient’s ability to lie still for the duration of the acquisition (15–45 min) 4. History of claustrophobia 5. Patient’s ability to put his or her arms overhead Jiraporn_PET/CT Onco 2020
2. Check for adverse reactions of any drug 3. Try to avoid radiation hazard to the patient; instrument, acq protocol, R’pharm dose 4. Minimizing radiation exposure to the patient’s family and to the general public, where appropriate. 5. Weight and size tolerances of equipment Pregnant women should not undergo F-18 FDG PET-CT. F-18 FDG does cross the placenta. Breast-feeding is not recommended for 12 hrs after administration of F-18 FDG. Jiraporn_PET/CT Onco 2020 EANM
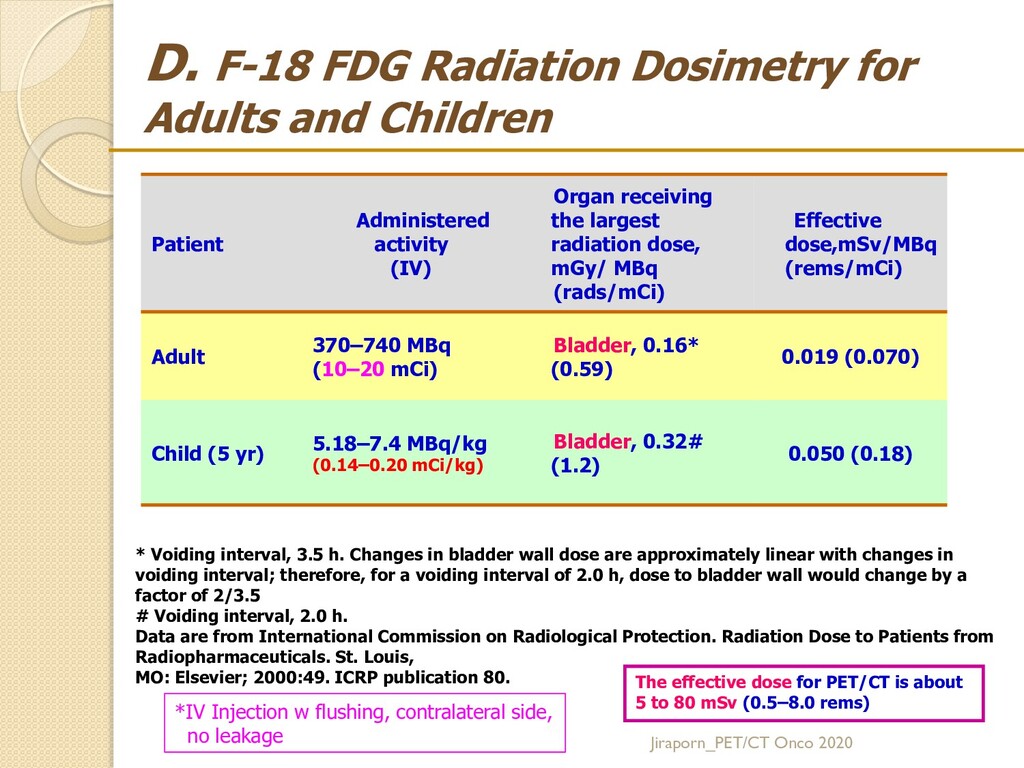
Administered activity (IV) Organ receiving the largest radiation dose, mGy/ MBq (rads/mCi) Effective dose,mSv/MBq (rems/mCi) Adult 370–740 MBq (10–20 mCi) Bladder, 0.16* (0.59) 0.019 (0.070) Child (5 yr) 5.18–7.4 MBq/kg (0.14–0.20 mCi/kg) Bladder, 0.32# (1.2) 0.050 (0.18) * Voiding interval, 3.5 h. Changes in bladder wall dose are approximately linear with changes in voiding interval; therefore, for a voiding interval of 2.0 h, dose to bladder wall would change by a factor of 2/3.5 # Voiding interval, 2.0 h. Data are from International Commission on Radiological Protection. Radiation Dose to Patients from Radiopharmaceuticals. St. Louis, MO: Elsevier; 2000:49. ICRP publication 80. The effective dose for PET/CT is about 5 to 80 mSv (0.5–8.0 rems) Jiraporn_PET/CT Onco 2020 *IV Injection w flushing, contralateral side, no leakage
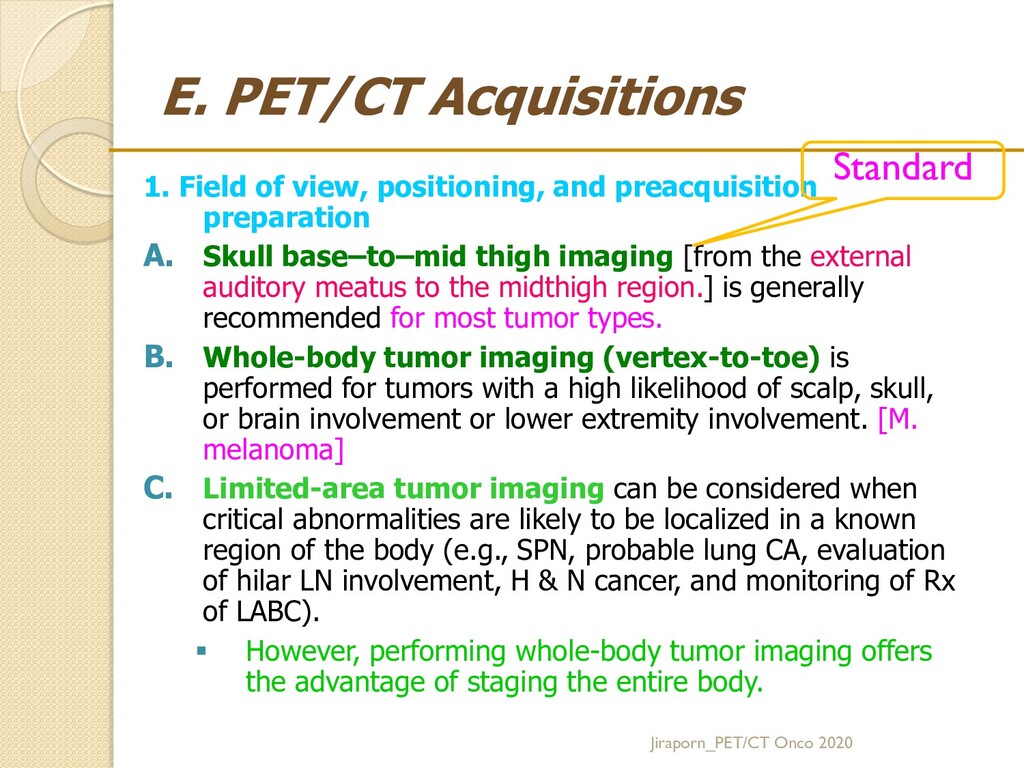
preparation A. Skull base–to–mid thigh imaging [from the external auditory meatus to the midthigh region.] is generally recommended for most tumor types. B. Whole-body tumor imaging (vertex-to-toe) is performed for tumors with a high likelihood of scalp, skull, or brain involvement or lower extremity involvement. [M. melanoma] C. Limited-area tumor imaging can be considered when critical abnormalities are likely to be localized in a known region of the body (e.g., SPN, probable lung CA, evaluation of hilar LN involvement, H & N cancer, and monitoring of Rx of LABC). However, performing whole-body tumor imaging offers the advantage of staging the entire body. Jiraporn_PET/CT Onco 2020 Standard
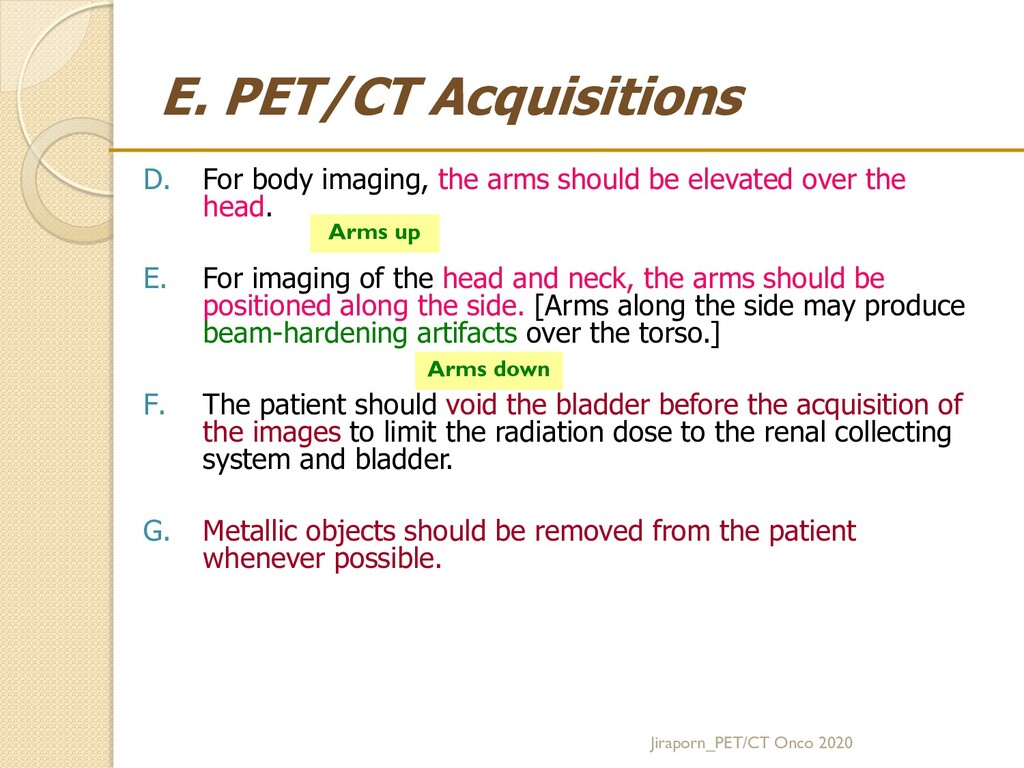
be elevated over the head. E. For imaging of the head and neck, the arms should be positioned along the side. [Arms along the side may produce beam-hardening artifacts over the torso.] F. The patient should void the bladder before the acquisition of the images to limit the radiation dose to the renal collecting system and bladder. G. Metallic objects should be removed from the patient whenever possible. Arms up Arms down Jiraporn_PET/CT Onco 2020
CT 2.2 diagnostic CT A. If the CT scan is obtained for AC/AL, a low mAs setting is recommended to decrease the radiation dose to the patient. B. For a diagnostic CT scan, standard CT mAs settings are recommended. IV or oral contrast material may be used. A separate CT acquisition may be necessary for a particular region of the body. High intravascular concentrations of IV contrast material may cause an attenuation correction artifact on the PET image, but the impact usually is modest. AC: Attenuation Correction AL: Anatomy Localization Jiraporn_PET/CT Onco 2020 CT มี 2 หน้าที่
intraluminal GI noncaloric contrast agent may be administered to provide adequate visualization of the GI tract unless it is medically contraindicated Collections of highly concentrated barium or iodinated contrast agents can result in an attenuation correction artifact that leads to a significant overestimation of the regional F-18 FDG concentration Diluted oral contrast agents cause less overestimation and do not affect PET image quality. Jiraporn_PET/CT Onco 2020
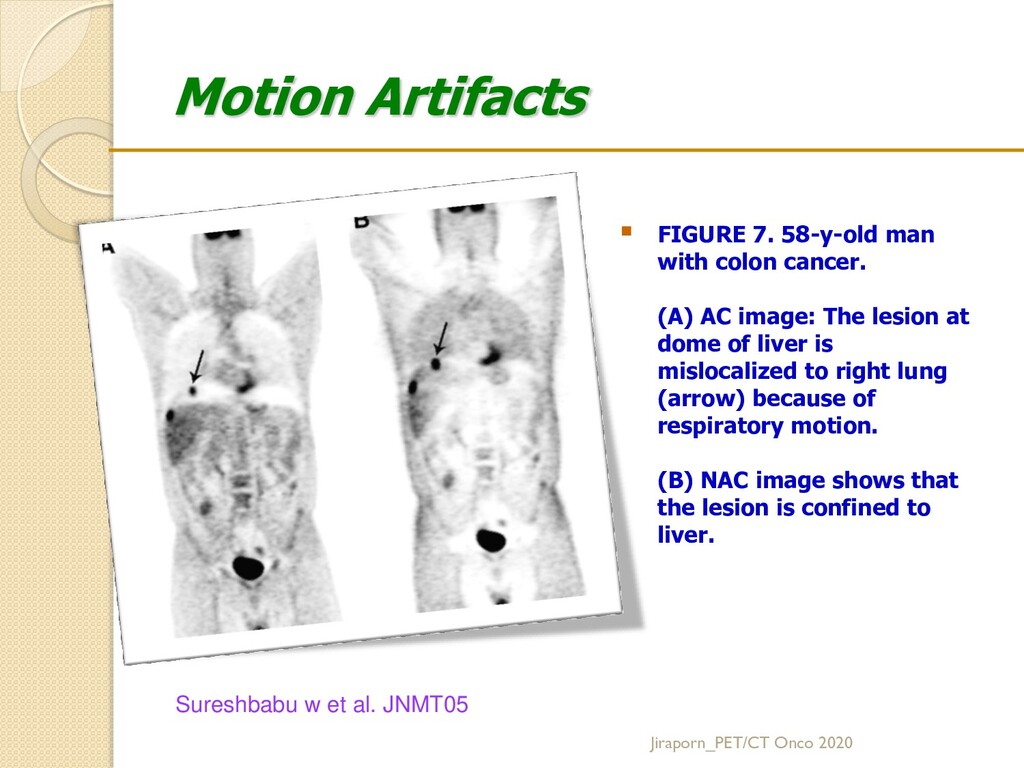
breathing during the CT acquisition is preferred. PET and CT images match as closely as possible Respiratory motion results in inaccurate localization of lesions at the base and periphery of the lungs, in the dome of the liver, or near any lung–soft tissue interface. Motion correction or respiratory gating is recommended when available. Jiraporn_PET/CT Onco 2020
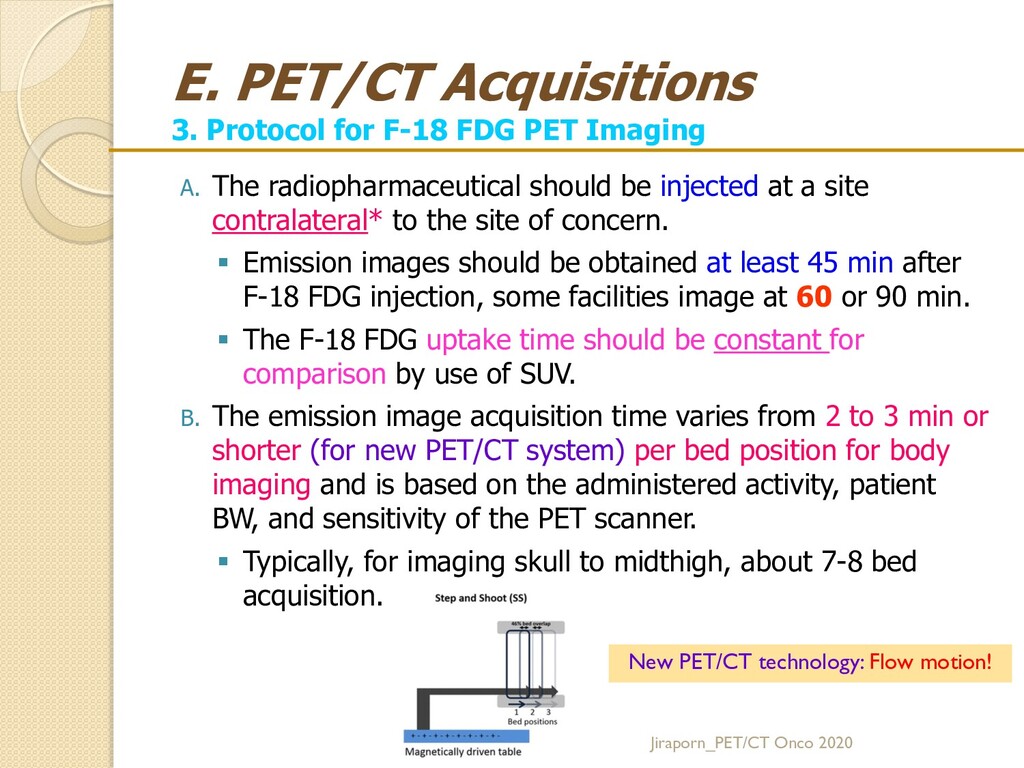
A. The radiopharmaceutical should be injected at a site contralateral* to the site of concern. Emission images should be obtained at least 45 min after F-18 FDG injection, some facilities image at 60 or 90 min. The F-18 FDG uptake time should be constant for comparison by use of SUV. B. The emission image acquisition time varies from 2 to 3 min or shorter (for new PET/CT system) per bed position for body imaging and is based on the administered activity, patient BW, and sensitivity of the PET scanner. Typically, for imaging skull to midthigh, about 7-8 bed acquisition. Jiraporn_PET/CT Onco 2020 New PET/CT technology: Flow motion!
C. Semiquantitative estimation of tumor glucose metabolism by use of the SUV is based on relative lesion radioactivity measured on AC PET images and normalized for the injected dose and BW, lean body mass, or BSA. Individual PET/CT scanner Serum glucose level F-18 FDG dose administration Uptake time Type of reconstruction algorithms Type of attenuation maps Size of the ROI Uptake distribution in the body Methods of analysis (e.g., maximum and mean). D. Semiquantitative estimation of tumor metabolism can be based on the ratio of F-18 FDG uptake in a lesion to F-18 FDG uptake in internal reference regions, such as the mediastinal blood pool, liver, and cerebellum. Jiraporn_PET/CT Onco 2020
Ratio Semi-quantitative measurement of degree of F-18 FDG accumulation in the ROI to the total injected dose and the patient's BW. [R41. Lowe VJ, Naunheim KS. Thorax 1998] Malignant tumors: increased glycolytic rate increased glucose uptake high SUV Concentration in ROI (uCi/g) SUV BW = --------------------------------------- Injected Dose (mCi) / BW (kg). Jiraporn_PET/CT Onco 2020 High FDG uptake High SUV Poorer prognosis
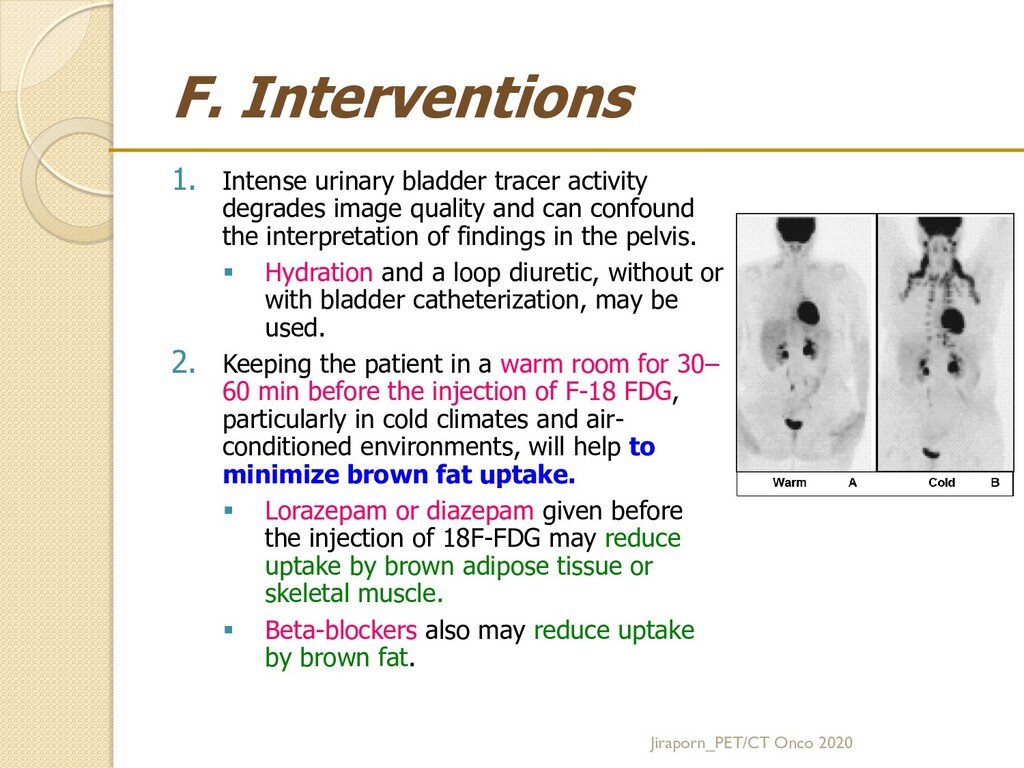
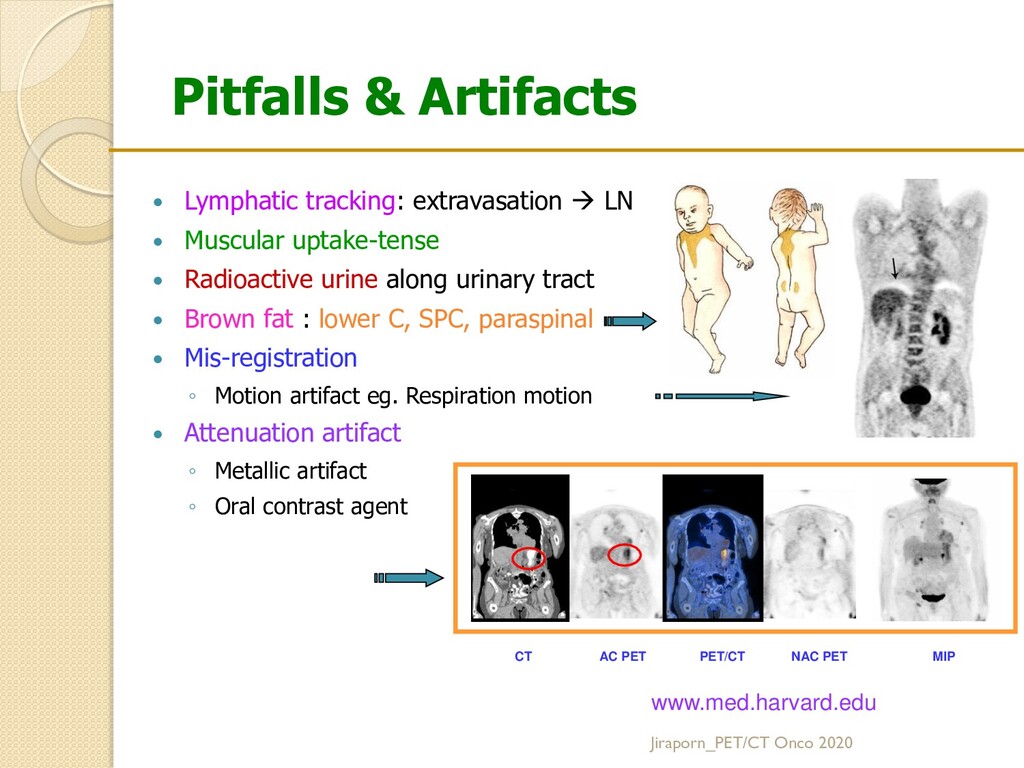
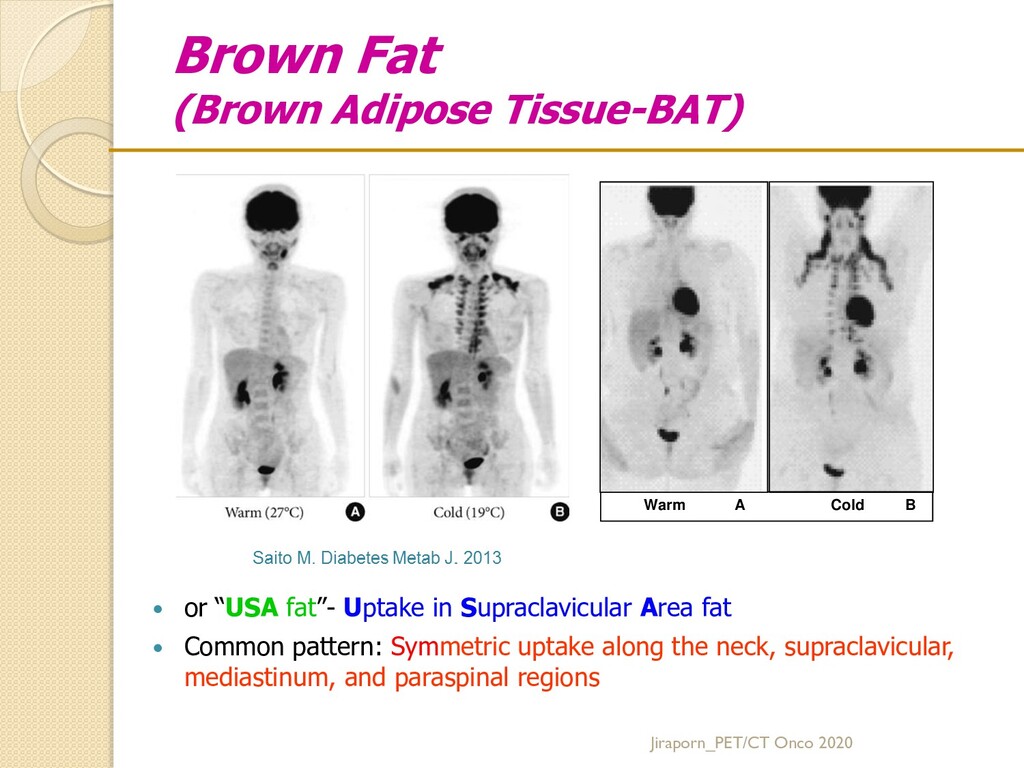
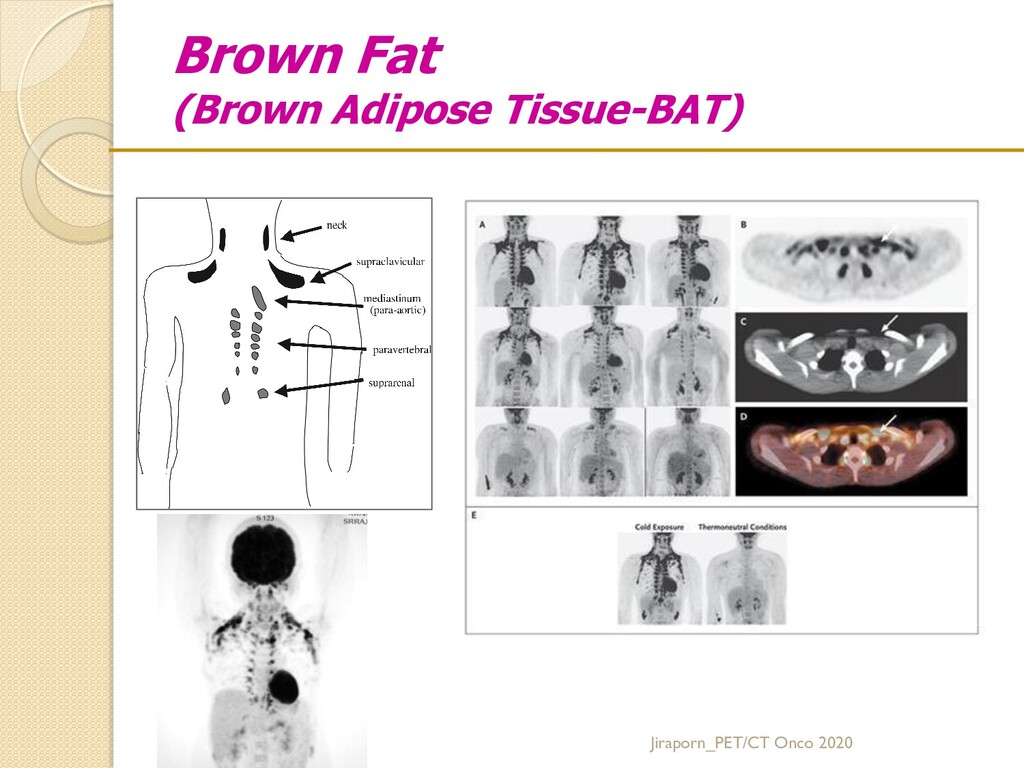
quality and can confound the interpretation of findings in the pelvis. Hydration and a loop diuretic, without or with bladder catheterization, may be used. 2. Keeping the patient in a warm room for 30– 60 min before the injection of F-18 FDG, particularly in cold climates and air- conditioned environments, will help to minimize brown fat uptake. Lorazepam or diazepam given before the injection of 18F-FDG may reduce uptake by brown adipose tissue or skeletal muscle. Beta-blockers also may reduce uptake by brown fat. Jiraporn_PET/CT Onco 2020
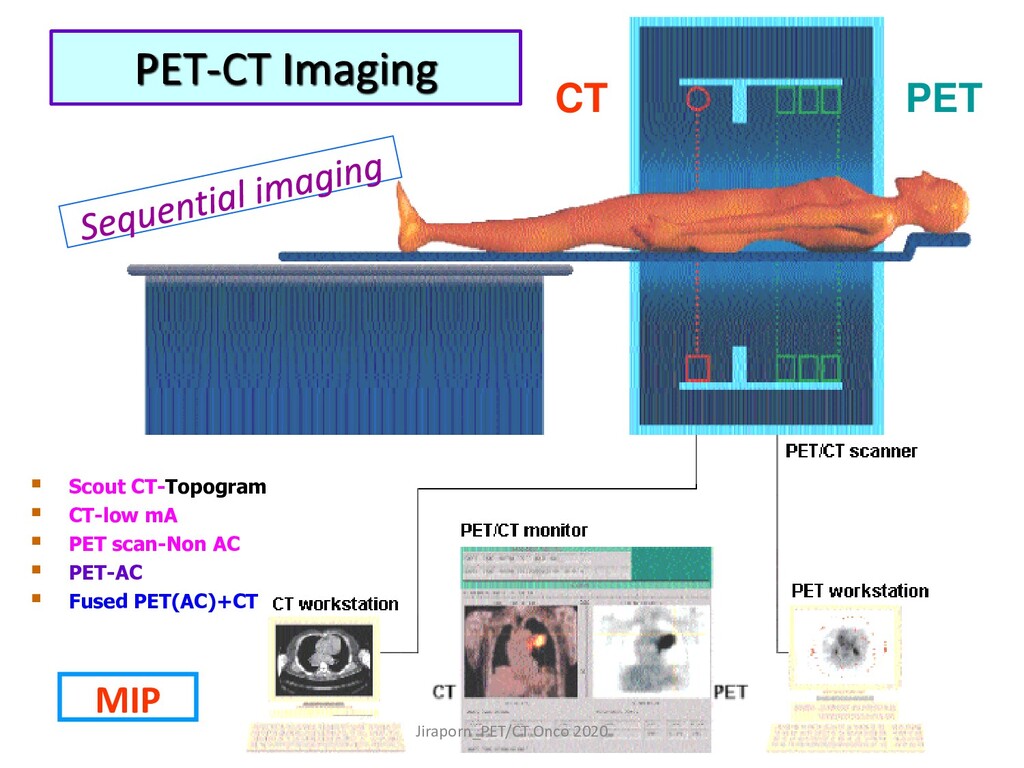
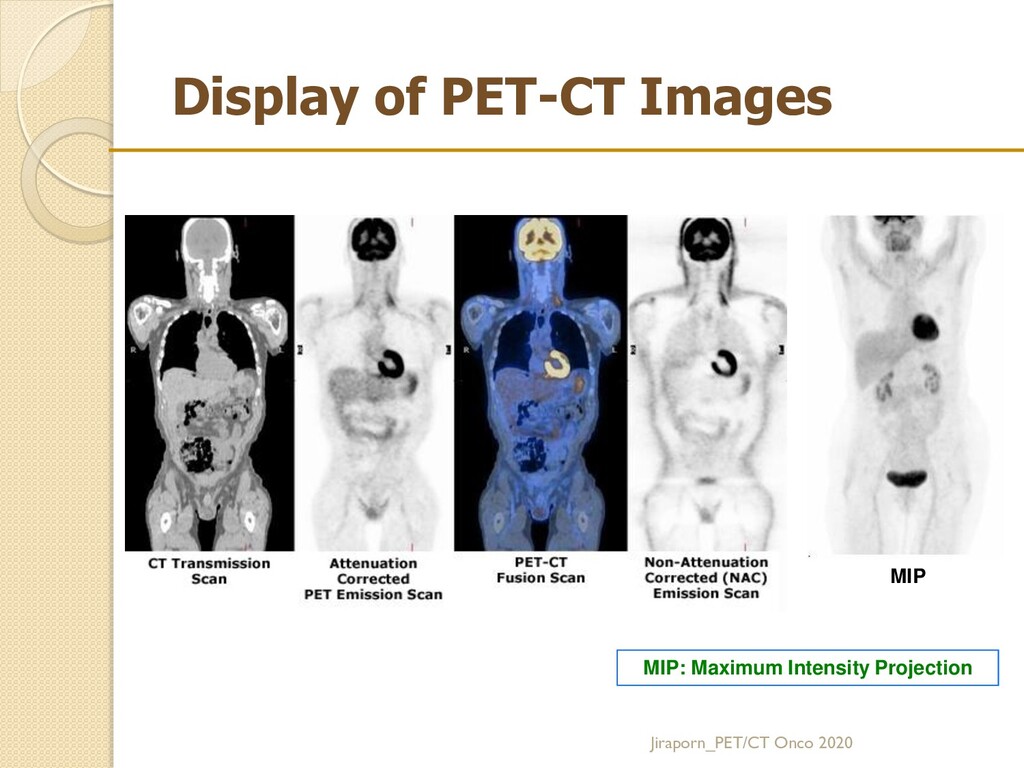
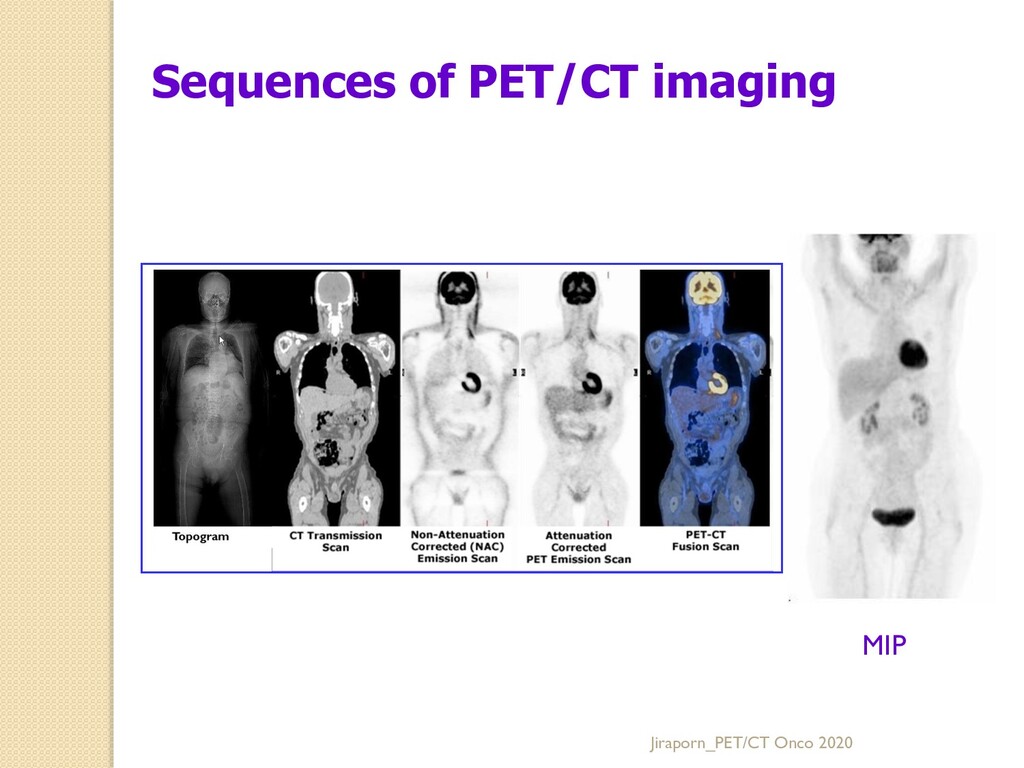
lines of response (LOR) between detector pairs. The emission data must be corrected for detector efficiency (normalization), system dead time, random coincidences, scatter, attenuation, and sampling nonuniformity. Scanners with retractable septa can acquire data in both 2D and 3D modes, whereas scanners wo septa acquire data in the 3D mode only. Datasets acquired in the 3D mode can be rebinned into 2D data and reconstructed with a 2D algorithm or can be reconstructed with a fully 3D algorithm. Iterative reconstruction* are available in both 2D and 3D modes, replacing FBP methods used previously. For a given algorithm, the appropriate reconstruction parameters will depend on the acquisition mode, the type of scanner, and the imaging task. It is good to archive reconstructions both with and without AC [to resolve issues arising from potential artifacts generated by the CT-based AC procedure.] The reconstructed images can be displayed in transaxial, coronal, and sagittal planes and as a rotating maximum-intensity projection (MIP) image. G. Processing 1. PET reconstruction: Jiraporn_PET/CT Onco 2020 *OSEM: Ordered subset expectation maximization
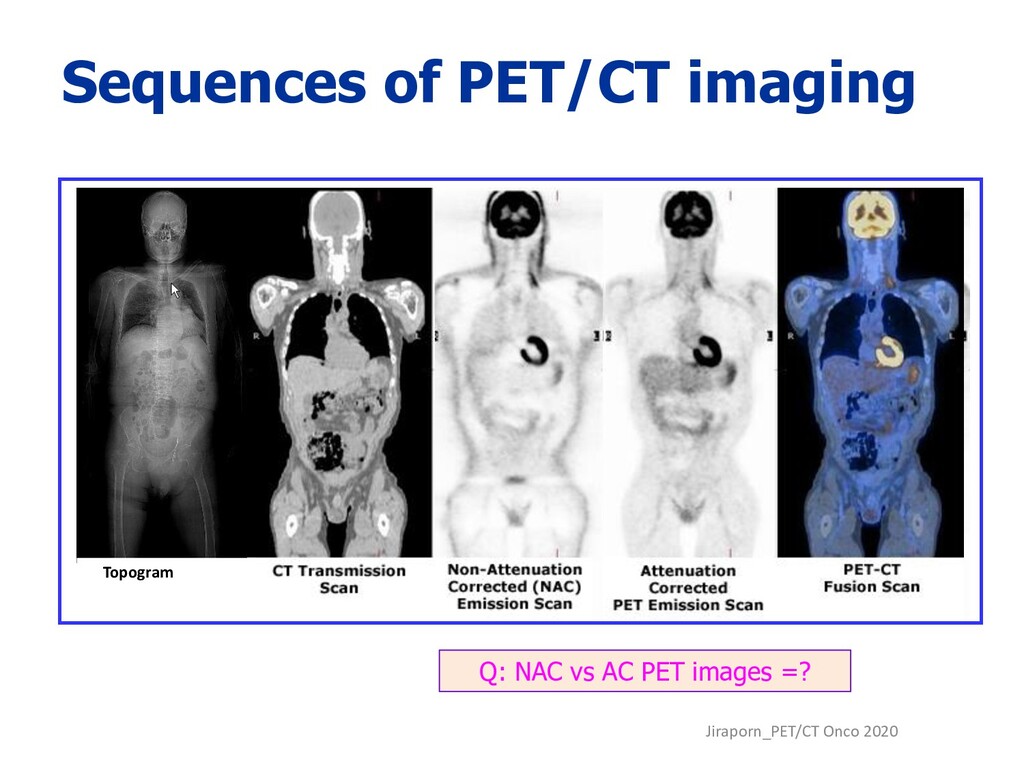
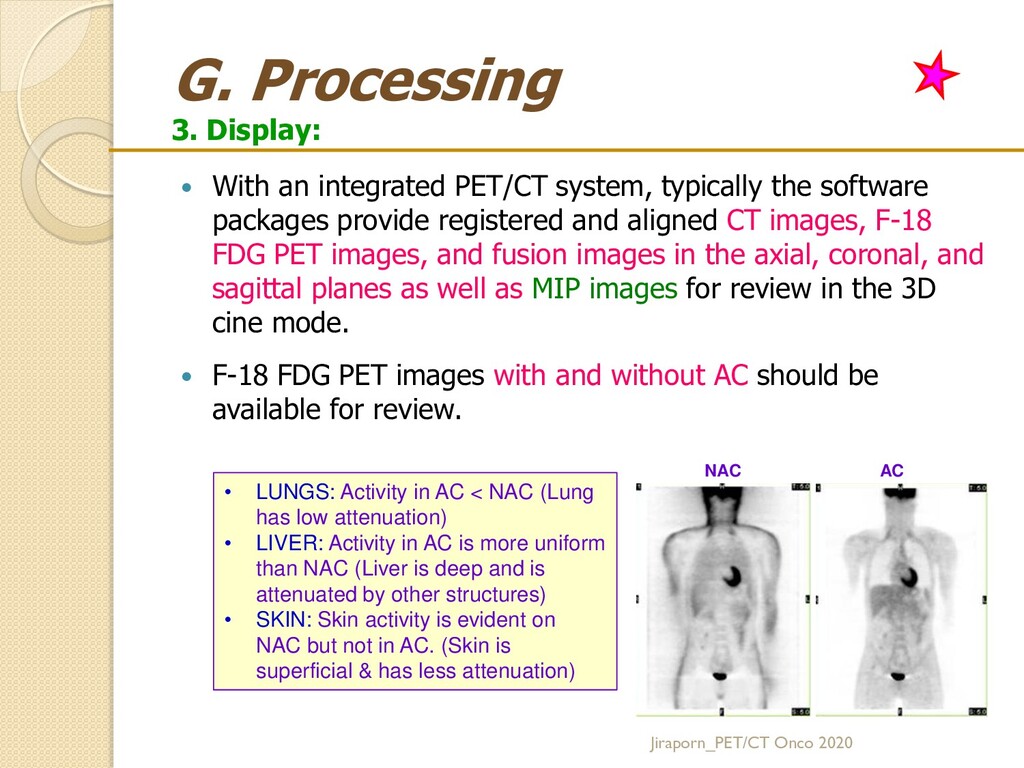
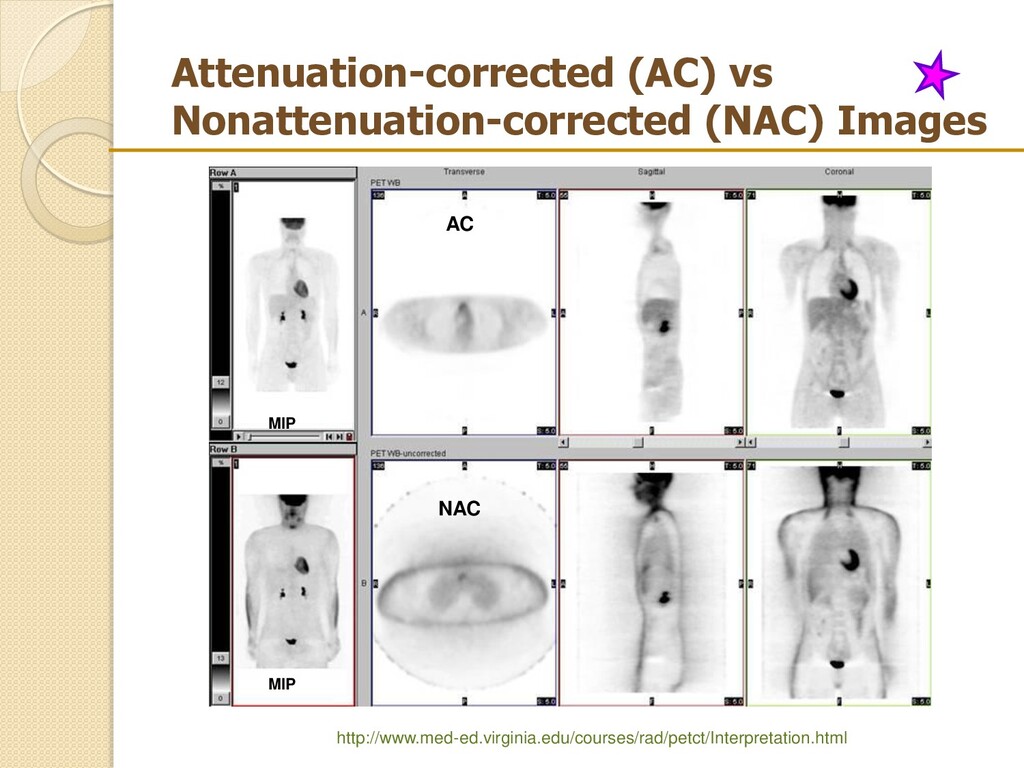
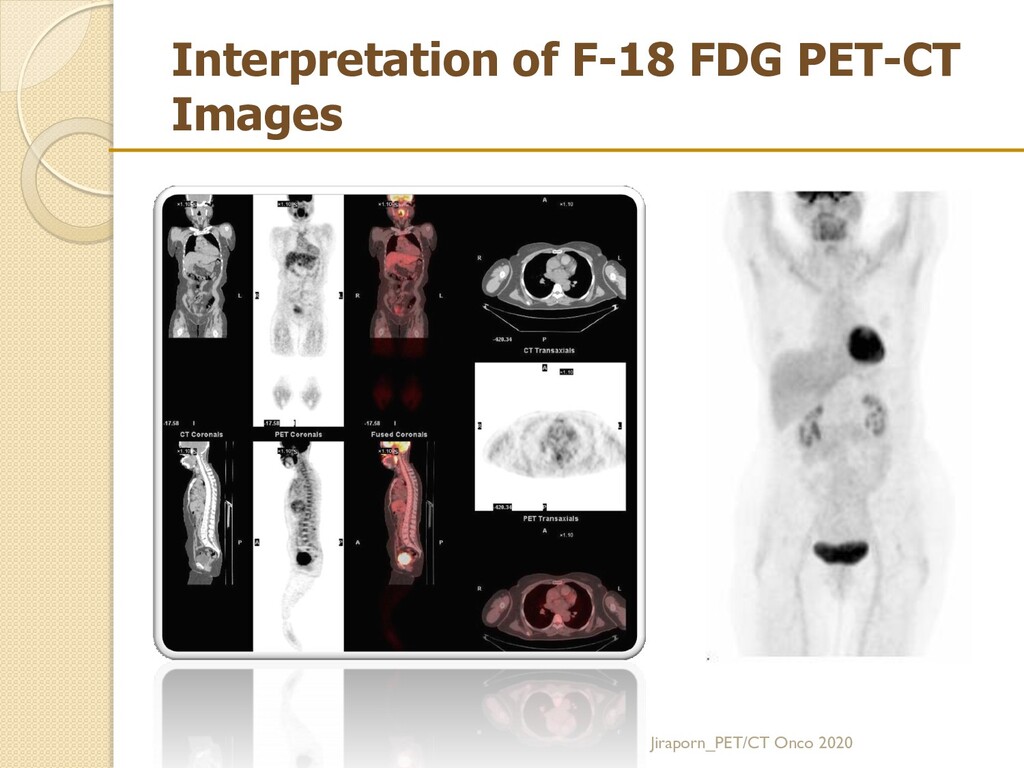
typically the software packages provide registered and aligned CT images, F-18 FDG PET images, and fusion images in the axial, coronal, and sagittal planes as well as MIP images for review in the 3D cine mode. F-18 FDG PET images with and without AC should be available for review. Jiraporn_PET/CT Onco 2020 • LUNGS: Activity in AC < NAC (Lung has low attenuation) • LIVER: Activity in AC is more uniform than NAC (Liver is deep and is attenuated by other structures) • SKIN: Skin activity is evident on NAC but not in AC. (Skin is superficial & has less attenuation) NAC AC
prior to FDG-PET study. FBS 70-110 mg/dL is ideal for FDG-PET > 200 mg/dL reschedule Hyperinsulinemia increase FDG uptake in skeletal muscle. No regular insulin SC injected within 4 hrs of having FDG administration. IV. inject 0.14-0.2 mCi/Kg of F-18 FDG (10-20 mCi) 60 minutes following iv. F-18 FDG, PET scan is performed. Skull base-to-mid-thigh or head-to-toe PET scan time: 2-3 min/ bed position CT scan: low mAs scan is adequate for attenuation correction & anatomical localization. High mAs scan is needed for diagnostic CT scan. Oral contrast and IV contrast for diagnostic CT ac requested. Jiraporn_PET/CT Onco 2020
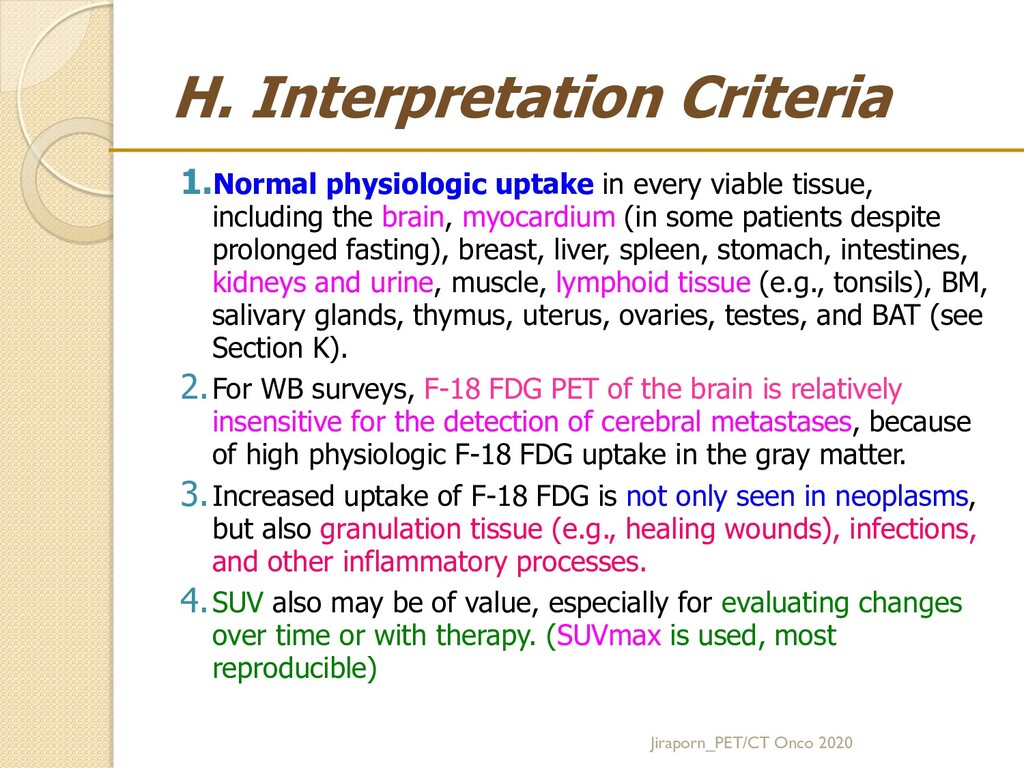
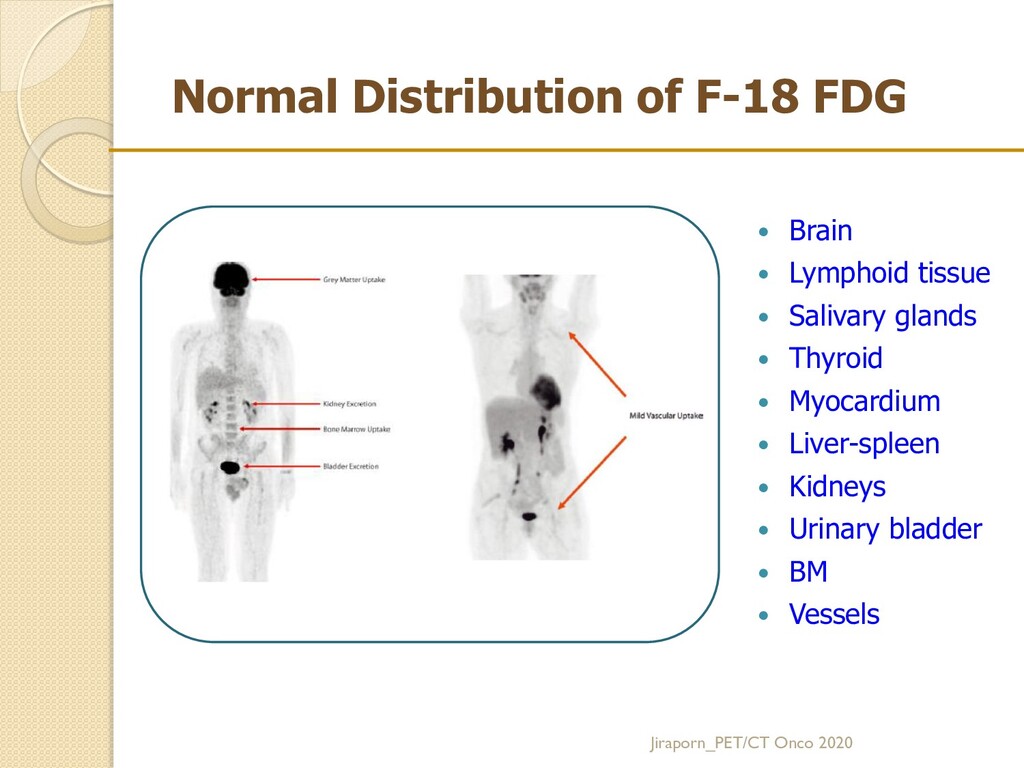
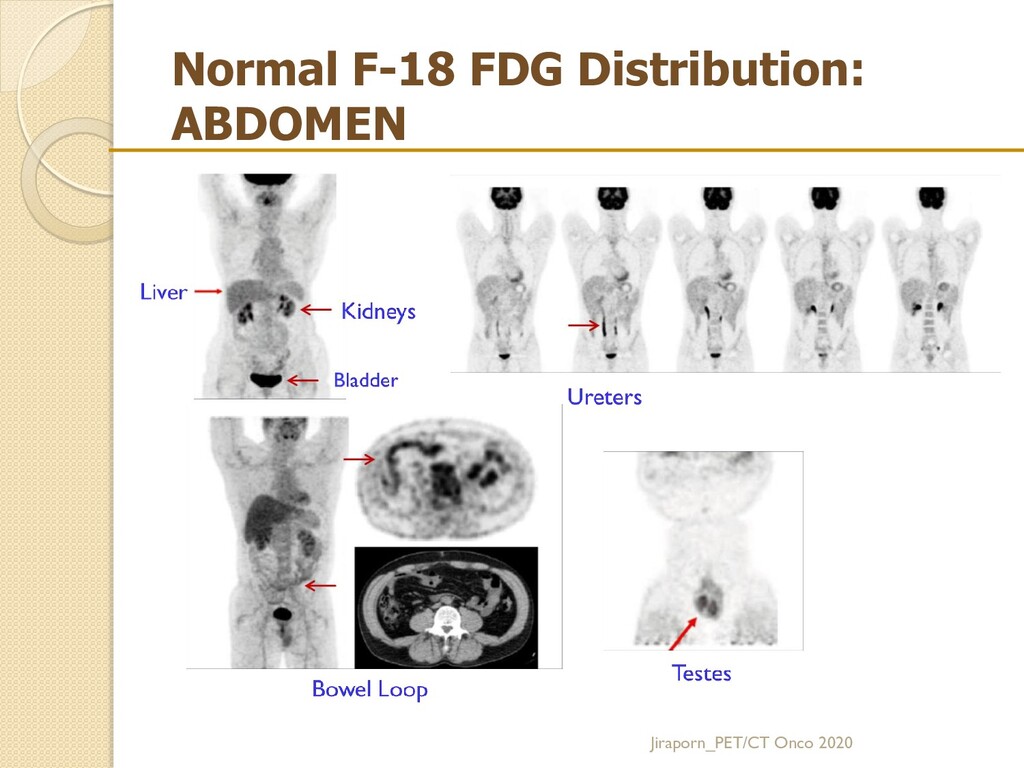
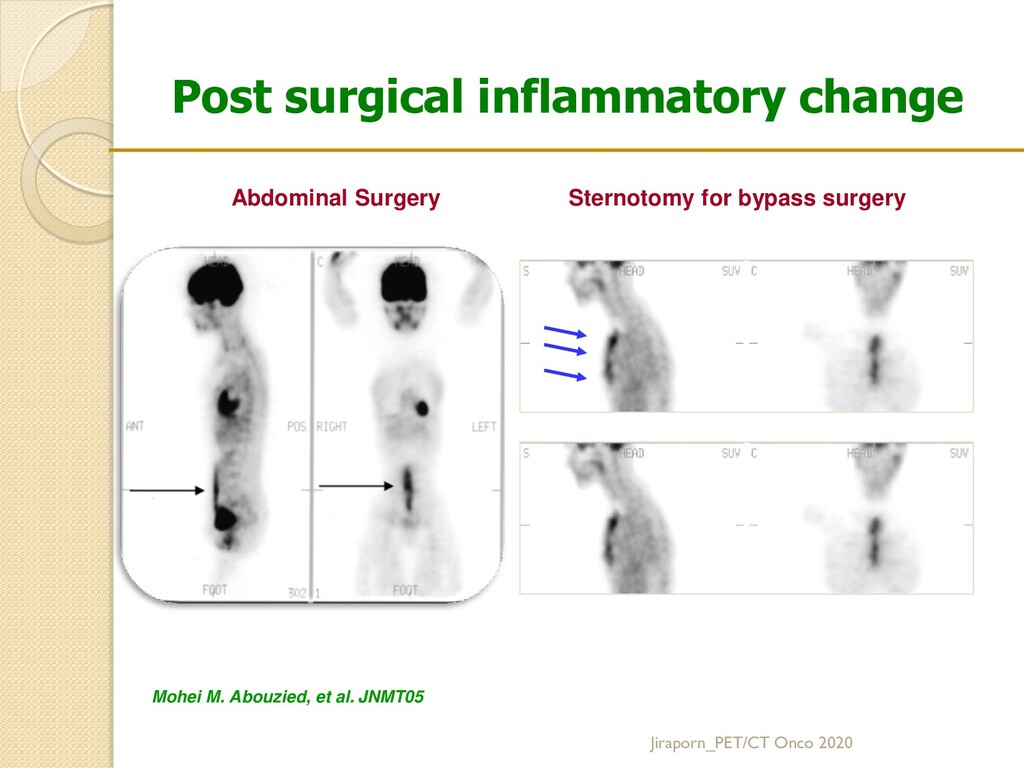
including the brain, myocardium (in some patients despite prolonged fasting), breast, liver, spleen, stomach, intestines, kidneys and urine, muscle, lymphoid tissue (e.g., tonsils), BM, salivary glands, thymus, uterus, ovaries, testes, and BAT (see Section K). 2.For WB surveys, F-18 FDG PET of the brain is relatively insensitive for the detection of cerebral metastases, because of high physiologic F-18 FDG uptake in the gray matter. 3.Increased uptake of F-18 FDG is not only seen in neoplasms, but also granulation tissue (e.g., healing wounds), infections, and other inflammatory processes. 4.SUV also may be of value, especially for evaluating changes over time or with therapy. (SUVmax is used, most reproducible) Jiraporn_PET/CT Onco 2020
for the study Relevant history Information needed for billing 3. Procedure description and imaging protocol Radiopharmaceutical, including amount of administered activity, route & site of administration, and 18F-FDG uptake time Other drugs administered and procedures performed, such as placement of IV line; hydration; insertion of Foley catheter (size); furosemide (amount and time), muscular relaxants, or pain medications; and sedation details in relation to the radiotracer injection, and patient condition at the conclusion of the PET study) Field of view and patient positioning: whole body, skull base to midthigh, or limited area and position of the arms Baseline glucose level CT transmission protocol (for AC/AL or diagnostic CT protocol with or without oral or intravenous contrast material and with the appropriate protocol for the clinical scenario and body region of interest) PET emission protocol Jiraporn_PET/CT Onco 2020
for example, limited because of motion, muscular uptake, or hyperglycemia B. Describe the location, extent, and intensity of abnormal 18F-FDG uptake in relation to uptake in normal comparable tissues and describe the relevant morphologic (CT) findings related to PET abnormalities. An estimate of the intensity of F-18 FDG uptake by the SUV or describe as mild, moderate, or intense or in relation to the uptake in reference areas eg. normal liver, mediastinal blood-pool activity. The integrated PET/CT report should include incidental CT findings that are relevant to patient care. Diagnostic CT scan may be reported separately. C. Limitations: identify factors that can limit the sensitivity and specificity of the examination (e.g., small lesions or an inflammatory process) Jiraporn_PET/CT Onco 2020
answer any pertinent clinical questions raised in the request for the imaging examination E. Comparative data Comparisons with previous examinations and reports, whenever possible. When PET/CT is performed for monitoring therapy, a comparison of the extent and intensity of uptake may be summarized as metabolic progressive disease, metabolic stable disease, metabolic partial response, or metabolic complete response. However, the technical protocol and analysis of images need to be consistent in the 2 sets of images. Jiraporn_PET/CT Onco 2020
precise diagnosis should be given. When appropriate, a differential diagnosis should be given. When appropriate, follow-up and additional diagnostic studies needed to clarify or confirm the impression should be recommended. Jiraporn_PET/CT Onco 2020
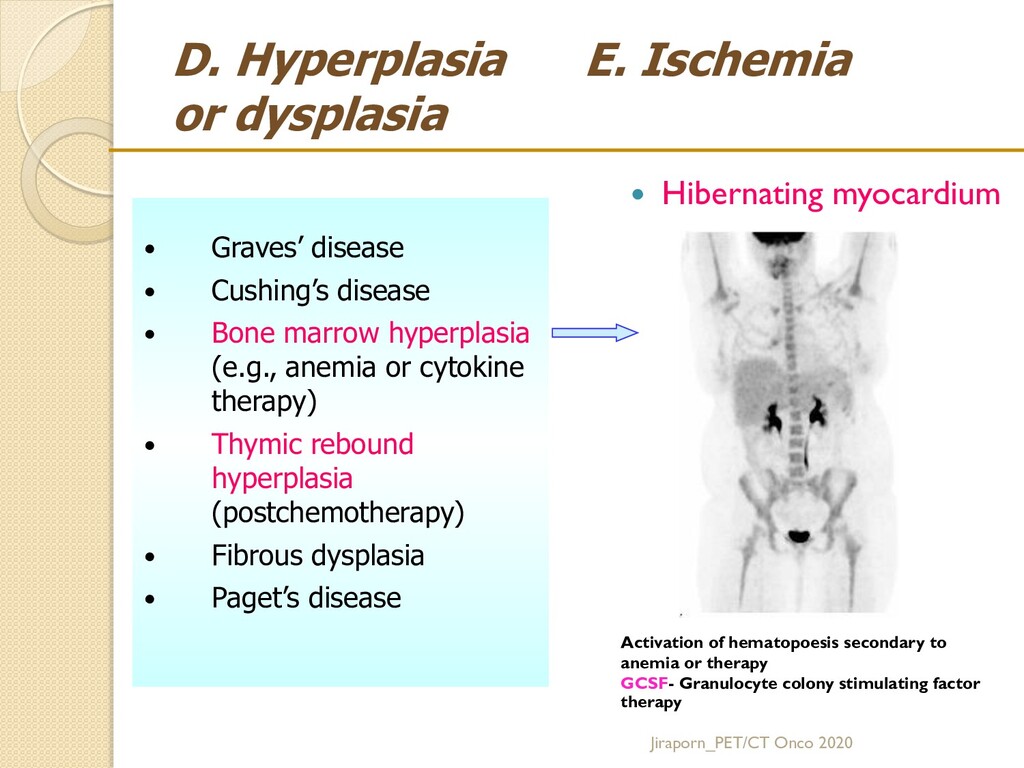
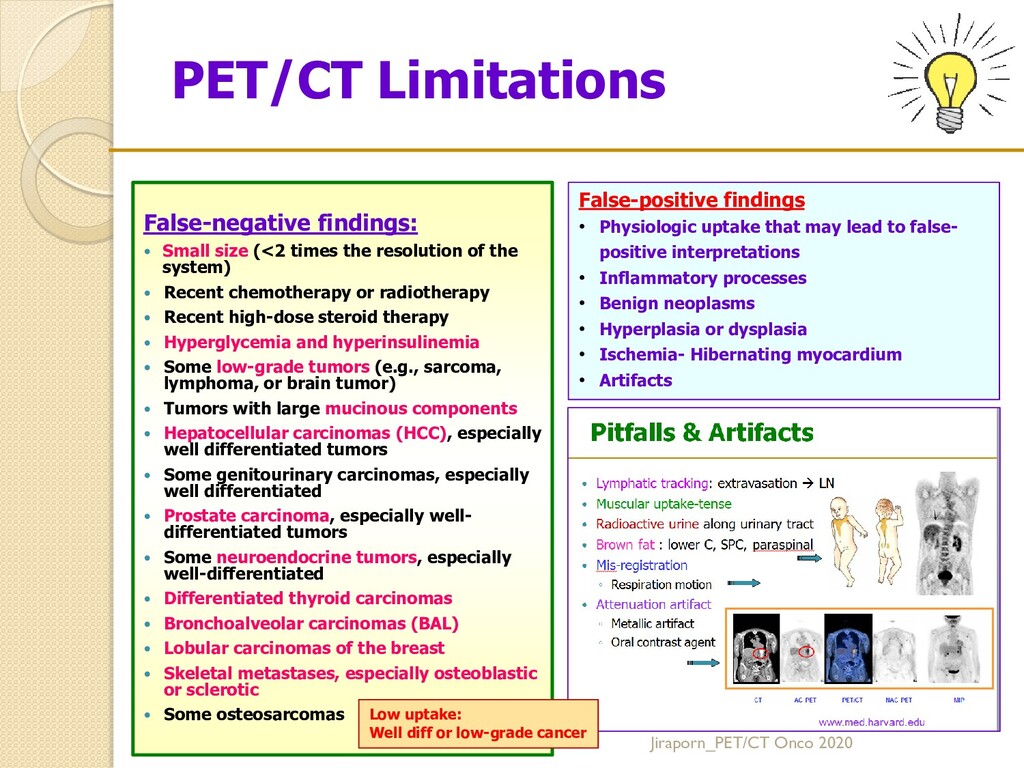
cause false positive and false-negative results. 1. False-positive findings A. Physiologic uptake that may lead to false-positive interpretations B. Inflammatory processes C. Benign neoplasms D. Hyperplasia or dysplasia E. Ischemia- Hibernating myocardium F. Artifacts Jiraporn_PET/CT Onco 2020
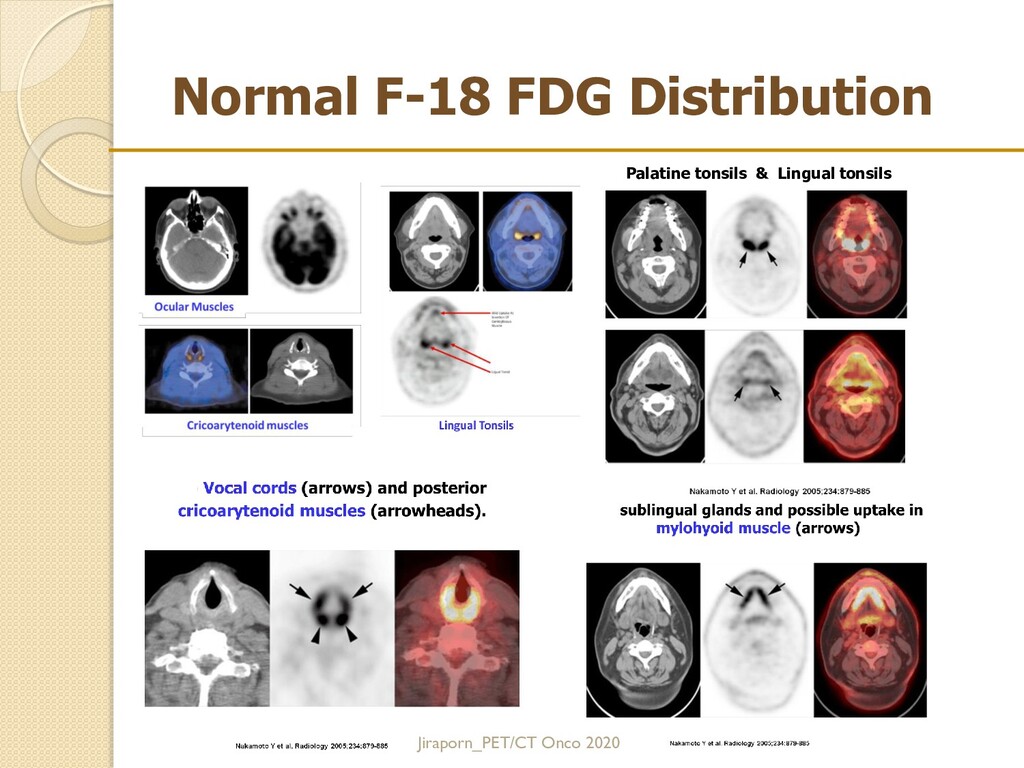
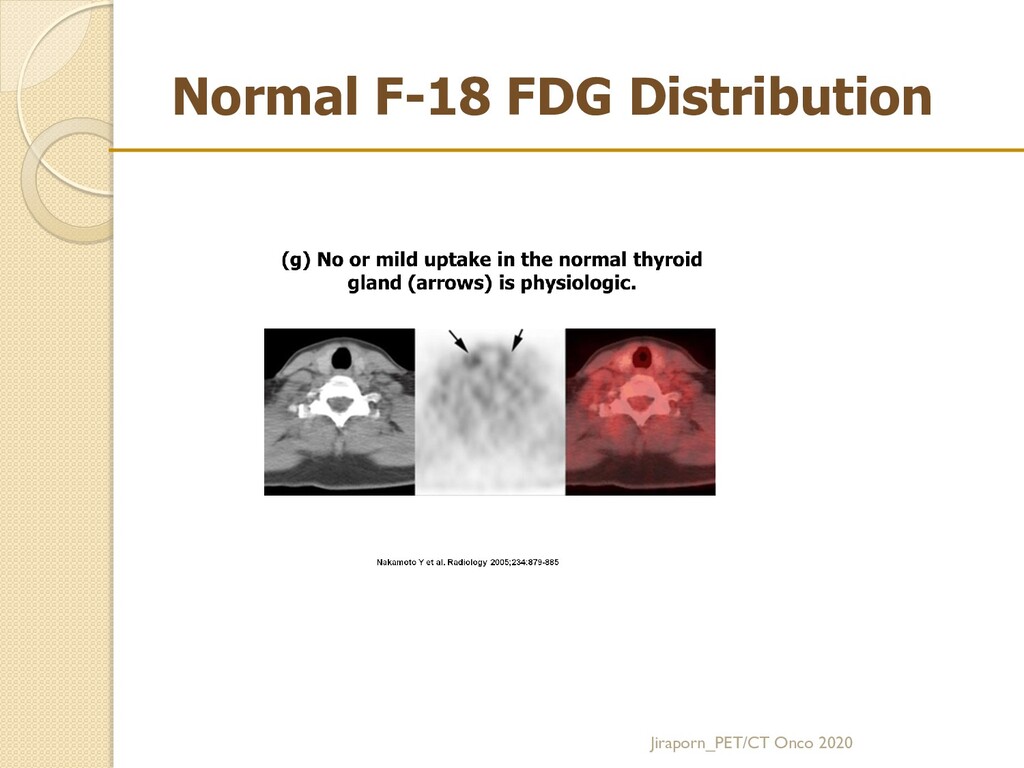
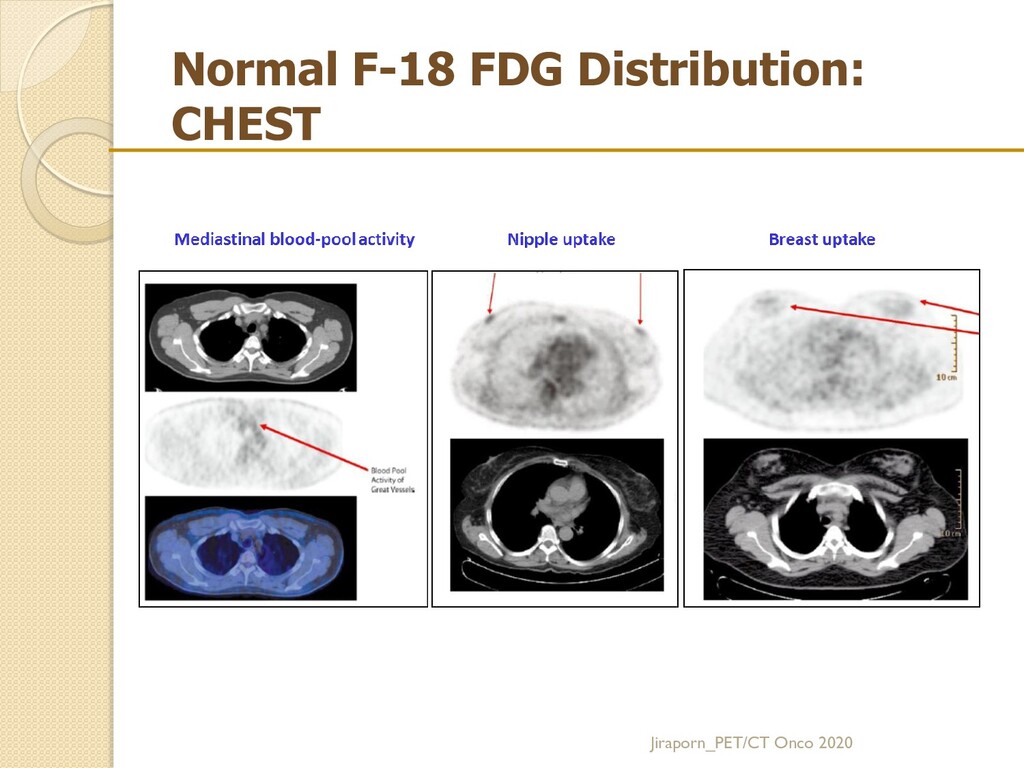
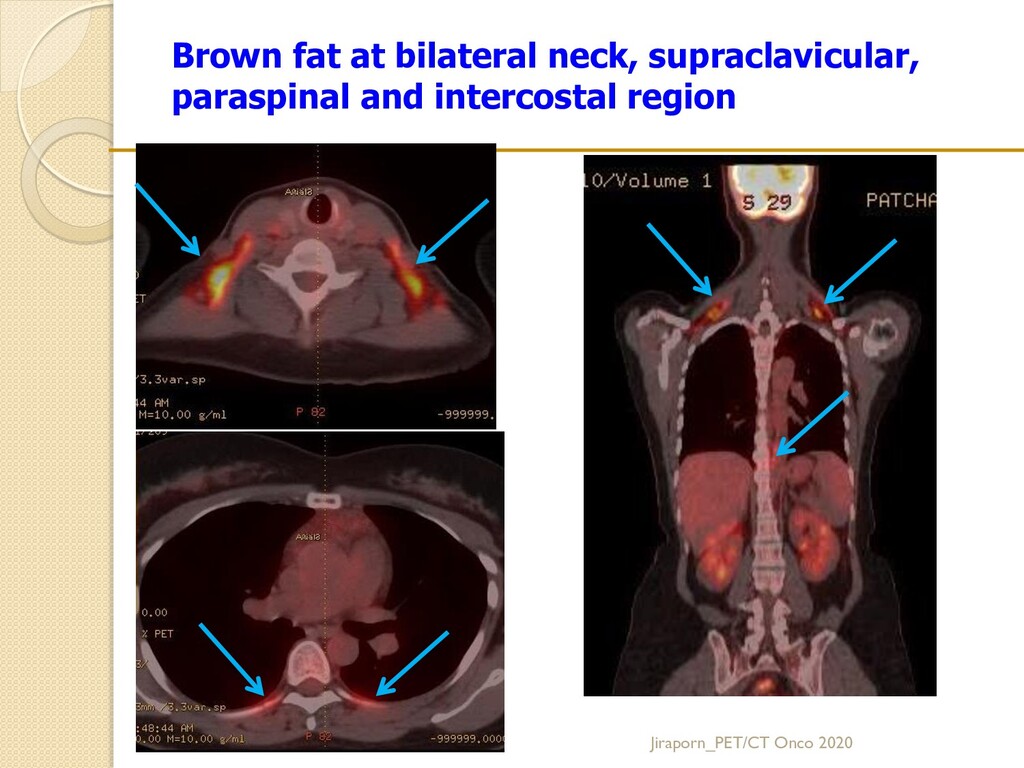
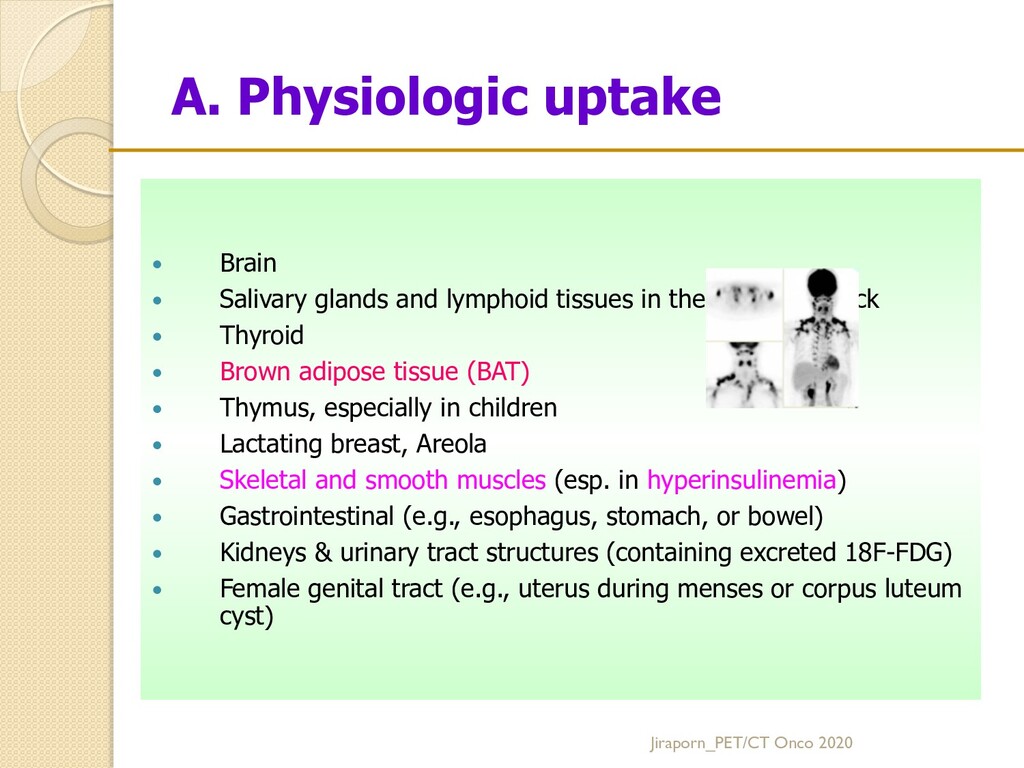
tissues in the head and neck Thyroid Brown adipose tissue (BAT) Thymus, especially in children Lactating breast, Areola Skeletal and smooth muscles (e.g., neck or paravertebral; hyperinsulinemia) Gastrointestinal (e.g., esophagus, stomach, or bowel) Kidneys & urinary tract structures (containing excreted 18F-FDG) Female genital tract (e.g., uterus during menses or corpus luteum cyst) Jiraporn_PET/CT Onco 2020
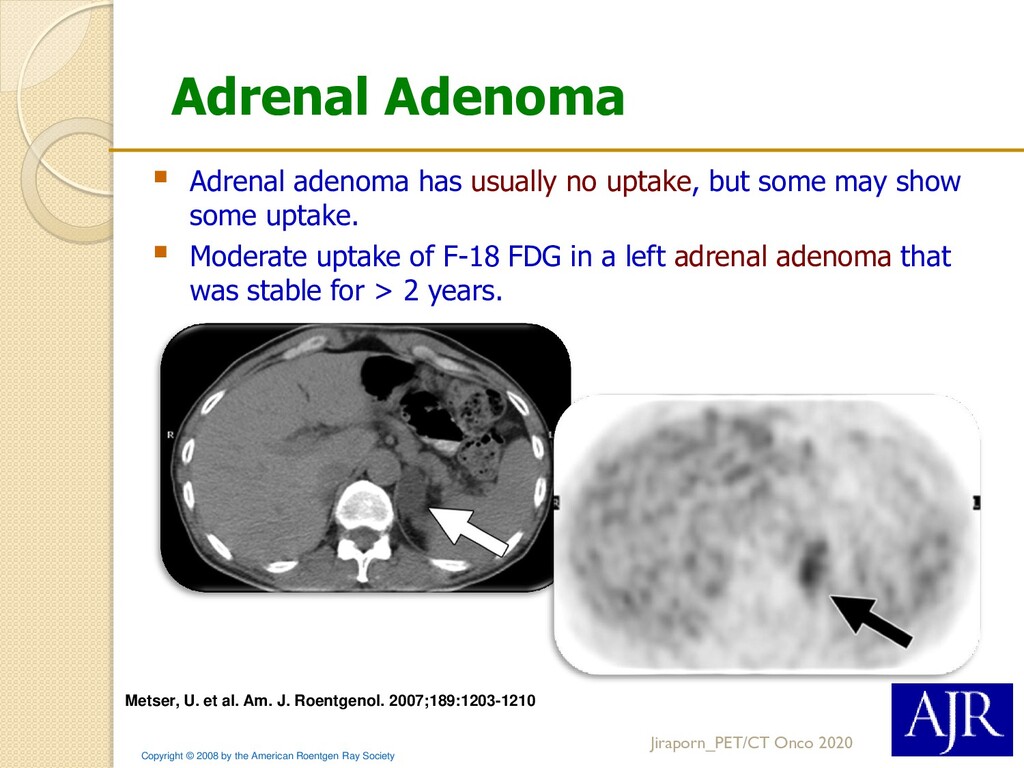
Society Metser, U. et al. Am. J. Roentgenol. 2007;189:1203-1210 Adrenal adenoma has usually no uptake, but some may show some uptake. Moderate uptake of F-18 FDG in a left adrenal adenoma that was stable for > 2 years. Jiraporn_PET/CT Onco 2020
(<2 times the resolution of the system) Recent chemotherapy or radiotherapy Recent high-dose steroid therapy Hyperglycemia and hyperinsulinemia Some low-grade tumors (e.g., sarcoma, lymphoma, or brain tumor) Tumors with large mucinous components Hepatocellular carcinomas (HCC), especially well differentiated tumors Some genitourinary carcinomas, especially well differentiated Prostate carcinoma, especially well-differentiated tumors Some neuroendocrine tumors, especially well-differentiated Differentiated thyroid carcinomas Bronchoalveolar carcinomas (BAL) Lobular carcinomas of the breast Skeletal metastases, especially osteoblastic or sclerotic Some osteosarcomas < 10 mm Jiraporn_PET/CT Onco 2020
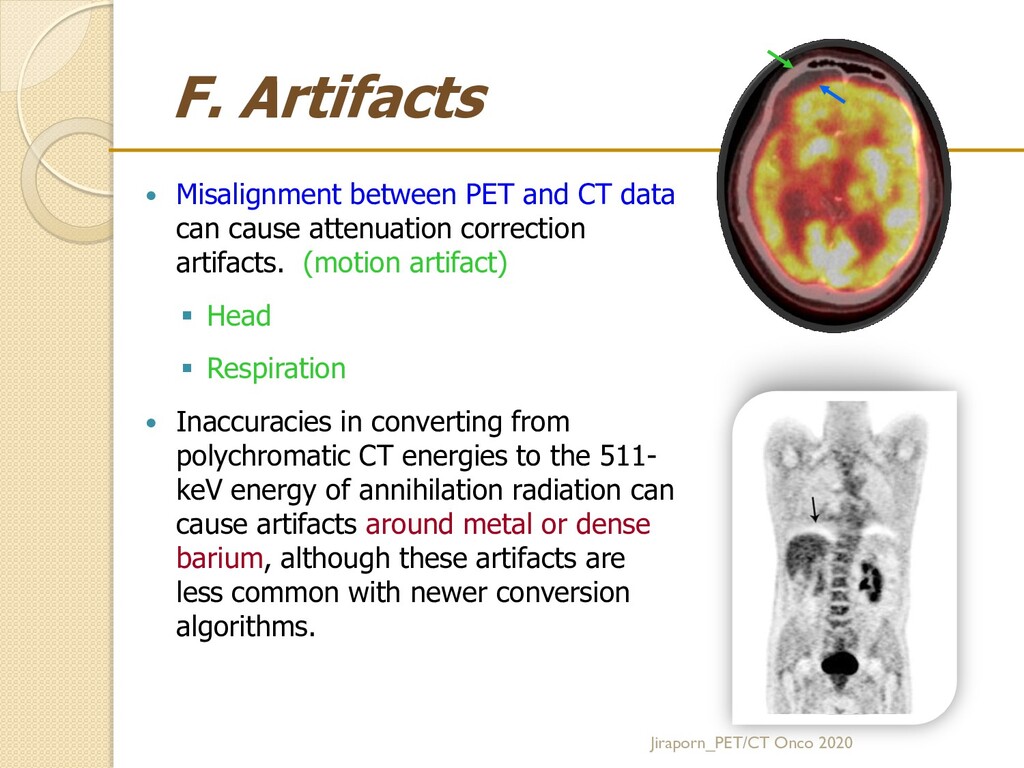
cause attenuation correction artifacts. (motion artifact) Head Respiration Inaccuracies in converting from polychromatic CT energies to the 511- keV energy of annihilation radiation can cause artifacts around metal or dense barium, although these artifacts are less common with newer conversion algorithms. Jiraporn_PET/CT Onco 2020
“USA fat”- Uptake in Supraclavicular Area fat Common pattern: Symmetric uptake along the neck, supraclavicular, mediastinum, and paraspinal regions Warm A Cold B
FIGURE 7. 58-y-old man with colon cancer. (A) AC image: The lesion at dome of liver is mislocalized to right lung (arrow) because of respiratory motion. (B) NAC image shows that the lesion is confined to liver.
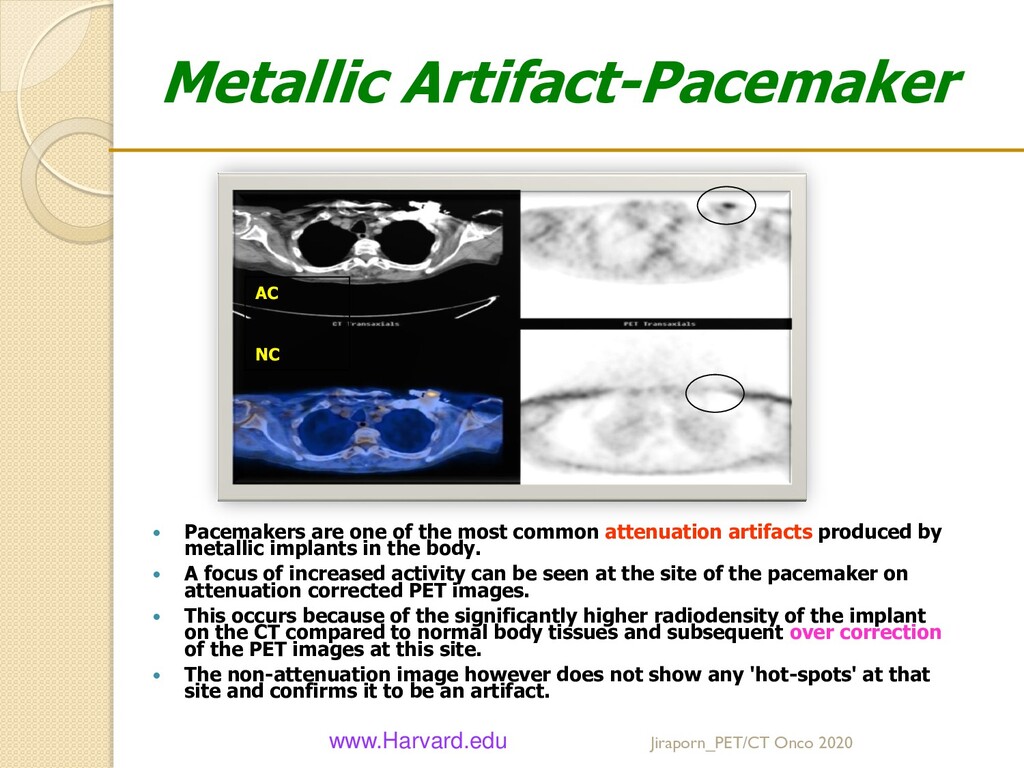
attenuation artifacts produced by metallic implants in the body. A focus of increased activity can be seen at the site of the pacemaker on attenuation corrected PET images. This occurs because of the significantly higher radiodensity of the implant on the CT compared to normal body tissues and subsequent over correction of the PET images at this site. The non-attenuation image however does not show any 'hot-spots' at that site and confirms it to be an artifact. www.Harvard.edu AC NC Jiraporn_PET/CT Onco 2020
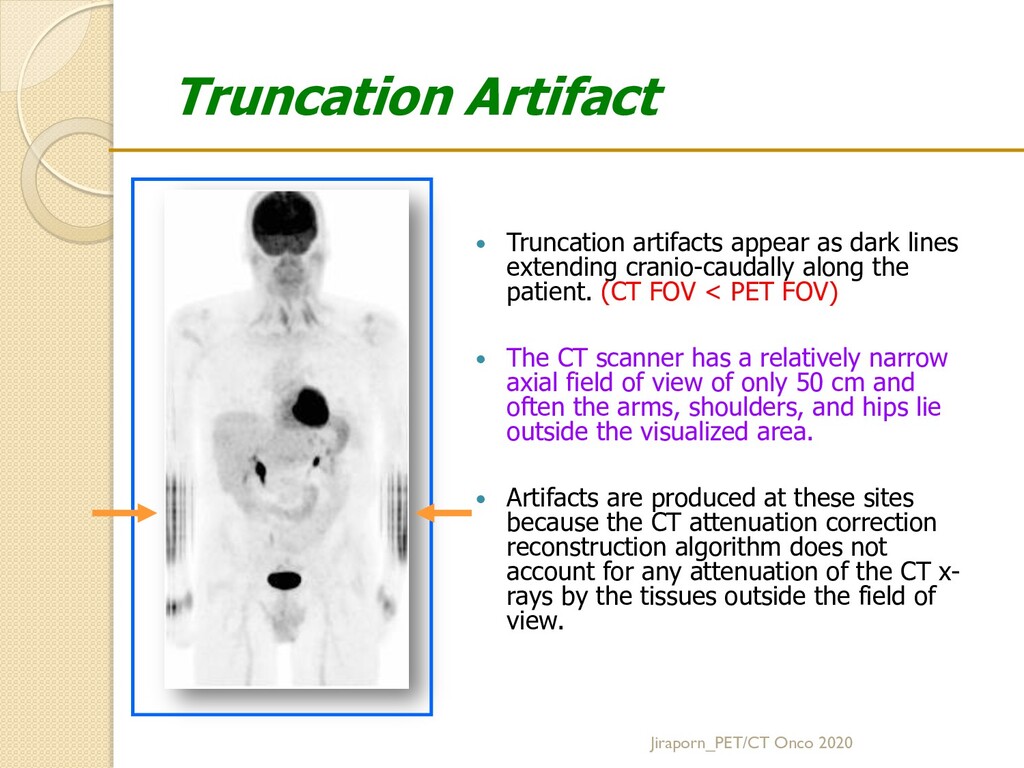
dark lines extending cranio-caudally along the patient. (CT FOV < PET FOV) The CT scanner has a relatively narrow axial field of view of only 50 cm and often the arms, shoulders, and hips lie outside the visualized area. Artifacts are produced at these sites because the CT attenuation correction reconstruction algorithm does not account for any attenuation of the CT x- rays by the tissues outside the field of view.
functional and anatomical information. F-18 FDG is the most commonly used PET tracer for oncologic PET/CT study. F-18 FDG is sensitive for detection most of cancers but it’s not really specific ! Appropriate timing of PET/CT exam after therapeutic intervention and careful evaluation with knowledge will provide accurate interpretation.
from malignant lesions 2. Selecting biopsy site 3. Searching for an unknown primary tumor 4. Staging known malignancies – Prior Rx 5. Guiding radiation therapy planning 6. Treatment Monitoring for known malignancies – During Rx 7. DDx residual tumor or posttreatment fibrosis or necrosis – Post complete Rx 8. Detecting tumor recurrence (elevated levels of tumor markers) – After Rx Please keep in mind that … F-18 FDG PET/CT is not equally effective for all malignancies and is not a tumor- specific agent! Jiraporn_PET/CT Onco 2020 • Staging guide for appropriate Rx • Monitoring considering continue or change Rx • After complete treatment • Early: Complete remission? • Late: Suspected tumor recurrence
tissues in the head and neck Thyroid Brown adipose tissue (BAT) Thymus, especially in children Lactating breast, Areola Skeletal and smooth muscles (esp. in hyperinsulinemia) Gastrointestinal (e.g., esophagus, stomach, or bowel) Kidneys & urinary tract structures (containing excreted 18F-FDG) Female genital tract (e.g., uterus during menses or corpus luteum cyst) Jiraporn_PET/CT Onco 2020
that may lead to false- positive interpretations • Inflammatory processes • Benign neoplasms • Hyperplasia or dysplasia • Ischemia- Hibernating myocardium • Artifacts False-negative findings: Small size (<2 times the resolution of the system) Recent chemotherapy or radiotherapy Recent high-dose steroid therapy Hyperglycemia and hyperinsulinemia Some low-grade tumors (e.g., sarcoma, lymphoma, or brain tumor) Tumors with large mucinous components Hepatocellular carcinomas (HCC), especially well differentiated tumors Some genitourinary carcinomas, especially well differentiated Prostate carcinoma, especially well- differentiated tumors Some neuroendocrine tumors, especially well-differentiated Differentiated thyroid carcinomas Bronchoalveolar carcinomas (BAL) Lobular carcinomas of the breast Skeletal metastases, especially osteoblastic or sclerotic Some osteosarcomas Low uptake: Well diff or low-grade cancer
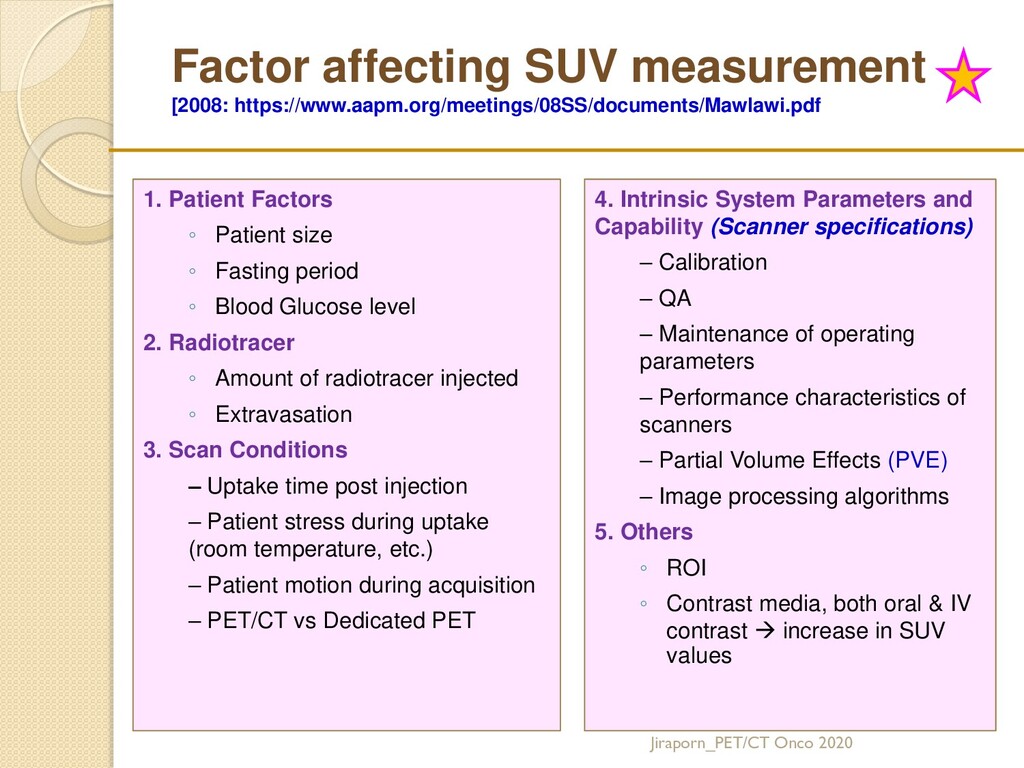
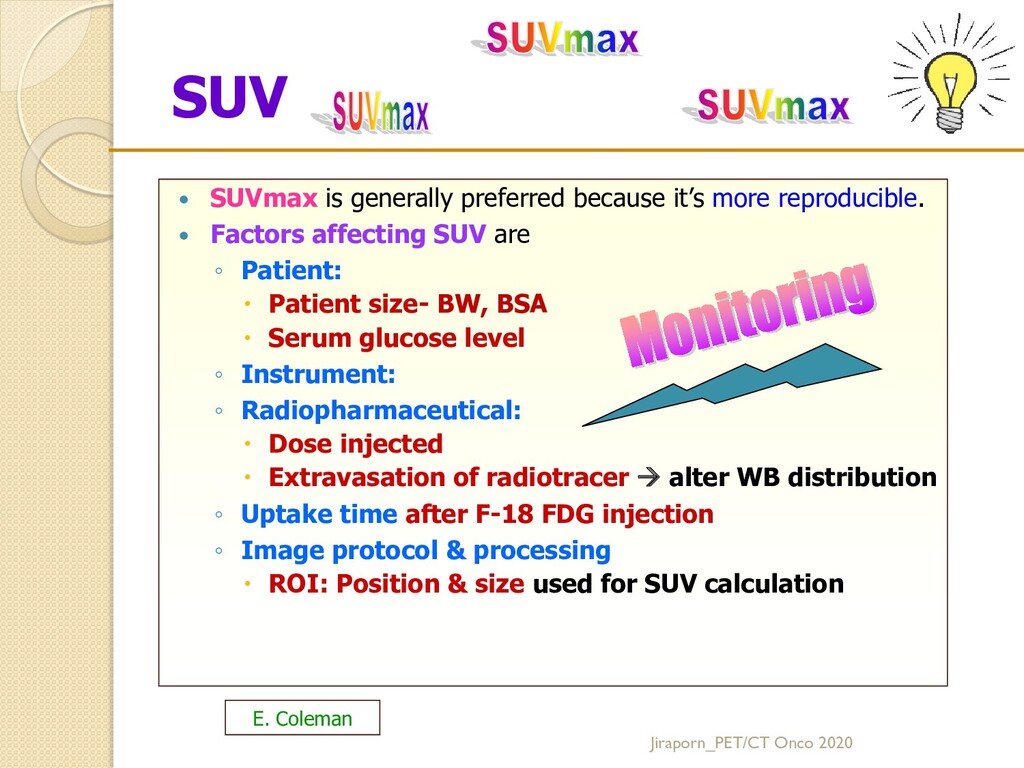
it’s more reproducible. Factors affecting SUV are ◦ Patient: Patient size- BW, BSA Serum glucose level ◦ Instrument: ◦ Radiopharmaceutical: Dose injected Extravasation of radiotracer alter WB distribution ◦ Uptake time after F-18 FDG injection ◦ Image protocol & processing ROI: Position & size used for SUV calculation E. Coleman
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}