disorder characterized by compromised bone strength predisposing to an increased risk of fracture. NIH Consensus Development Conference, March 27-29, 2000 Normal Bone Osteoporotic Bone
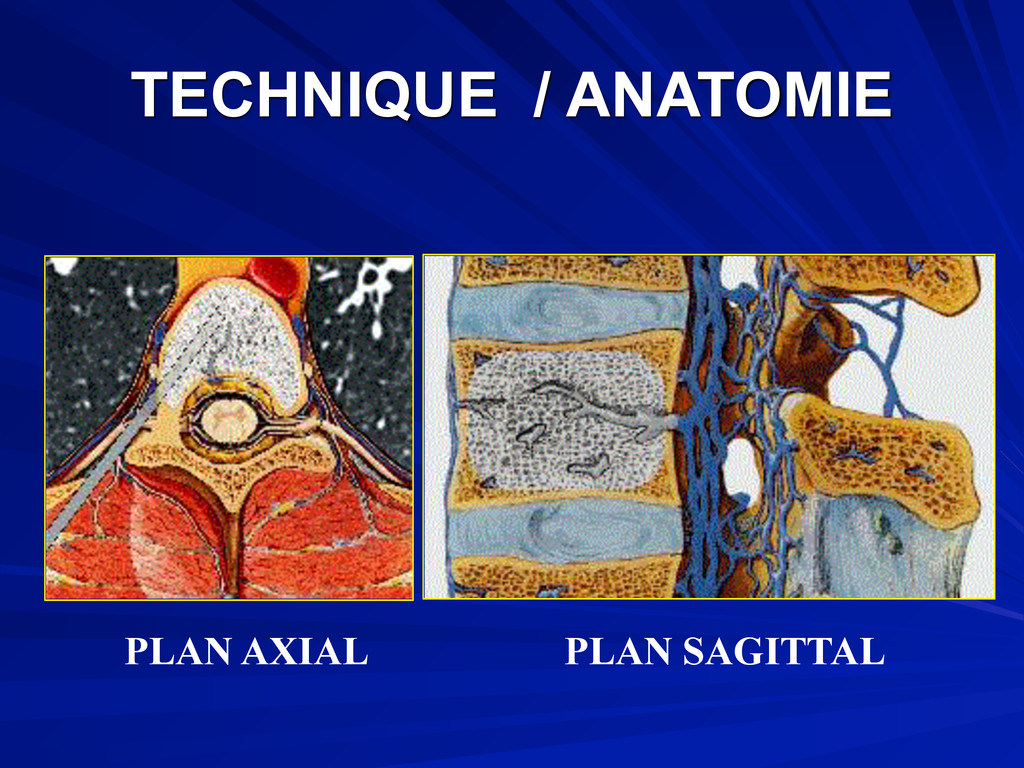
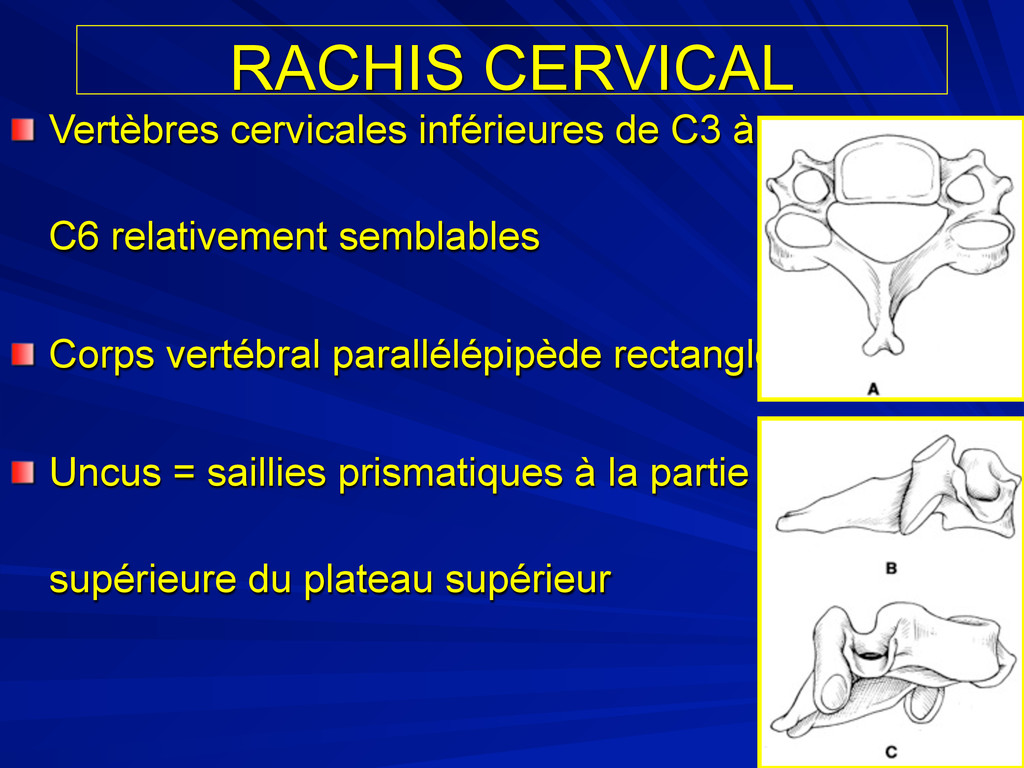
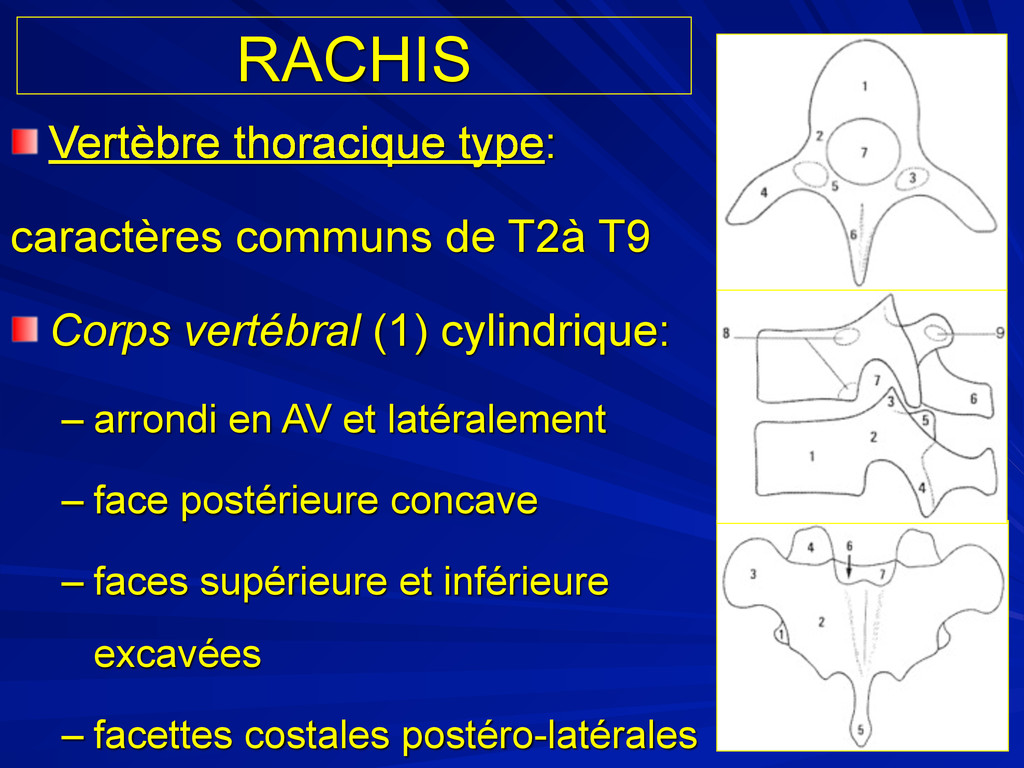
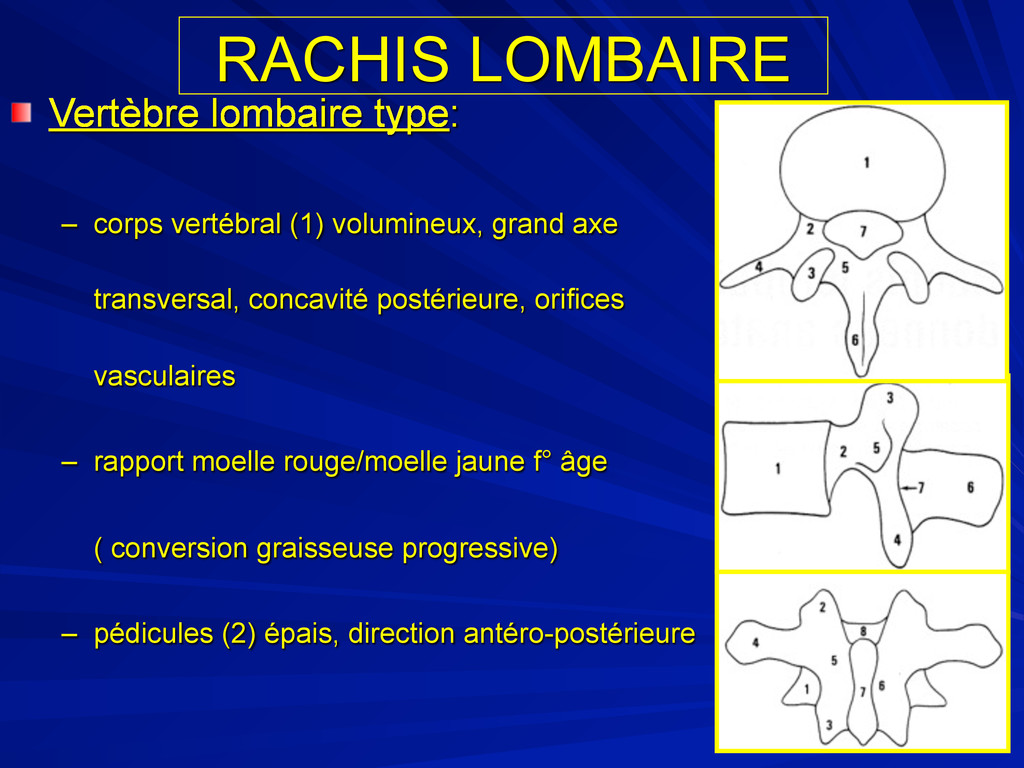
vertébral (1) cylindrique: – arrondi en AV et latéralement – face postérieure concave – faces supérieure et inférieure excavées – facettes costales postéro-latérales
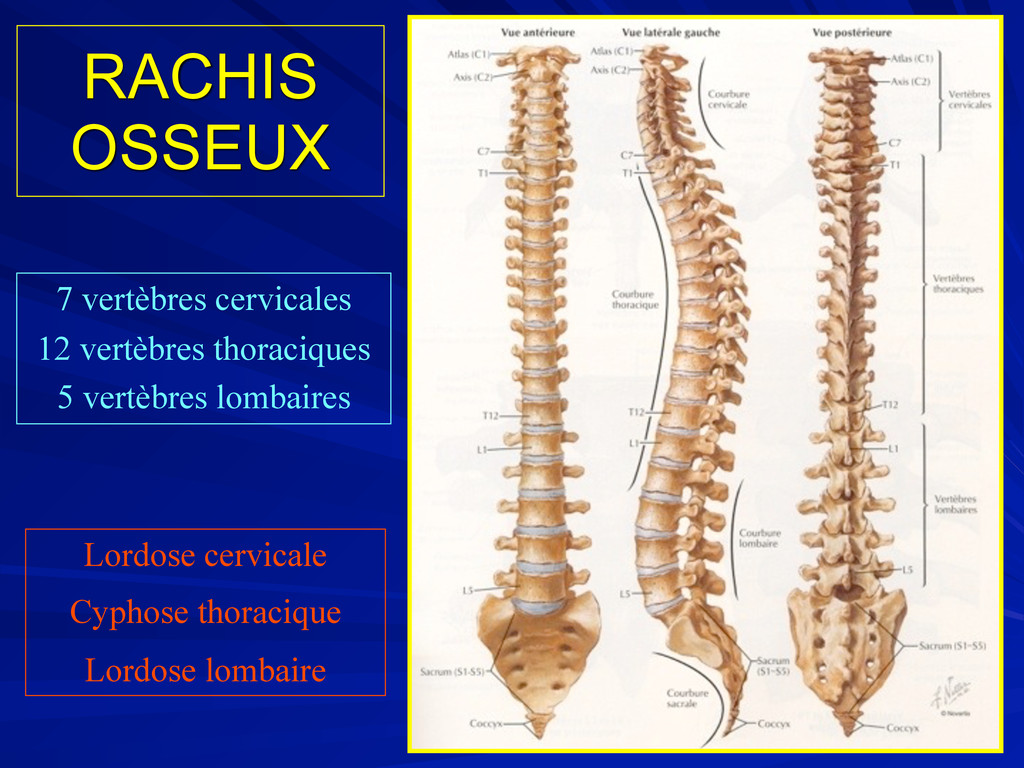
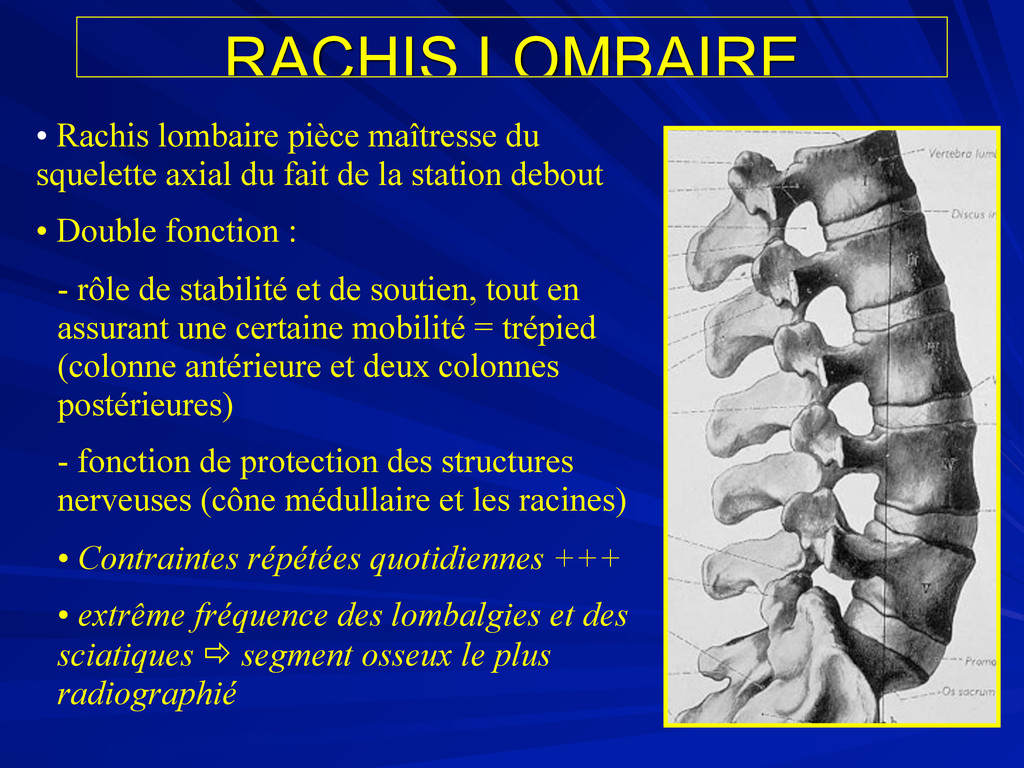
du fait de la station debout • Double fonction : - rôle de stabilité et de soutien, tout en assurant une certaine mobilité = trépied (colonne antérieure et deux colonnes postérieures) - fonction de protection des structures nerveuses (cône médullaire et les racines) • Contraintes répétées quotidiennes +++ • extrême fréquence des lombalgies et des sciatiques segment osseux le plus radiographié
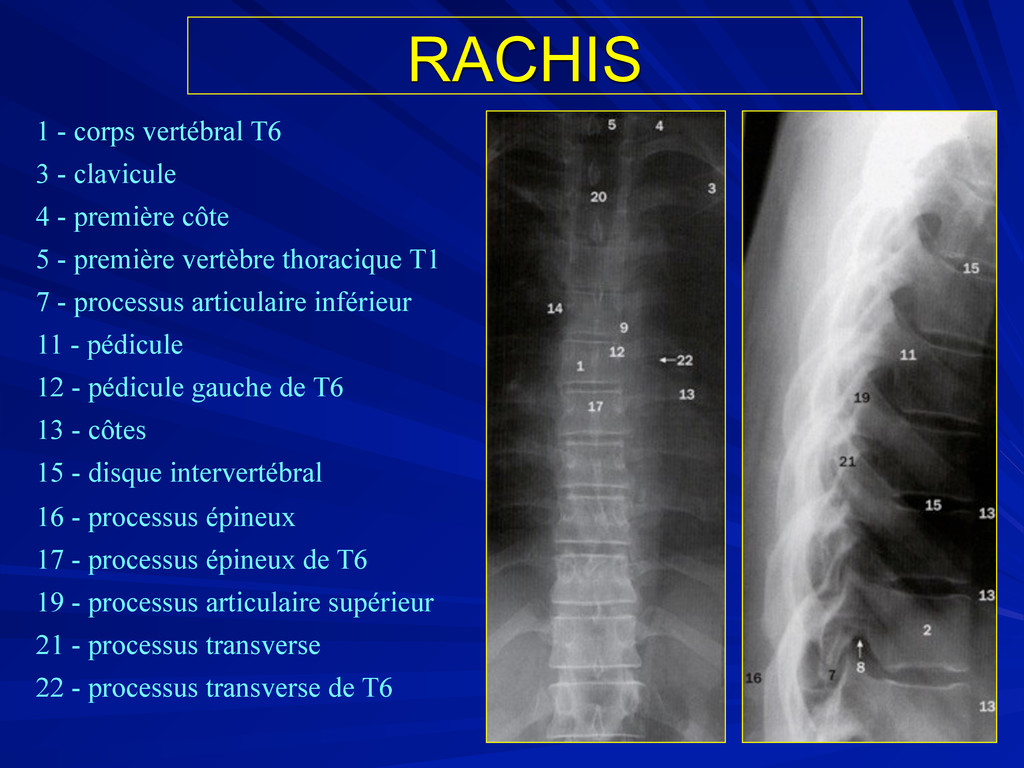
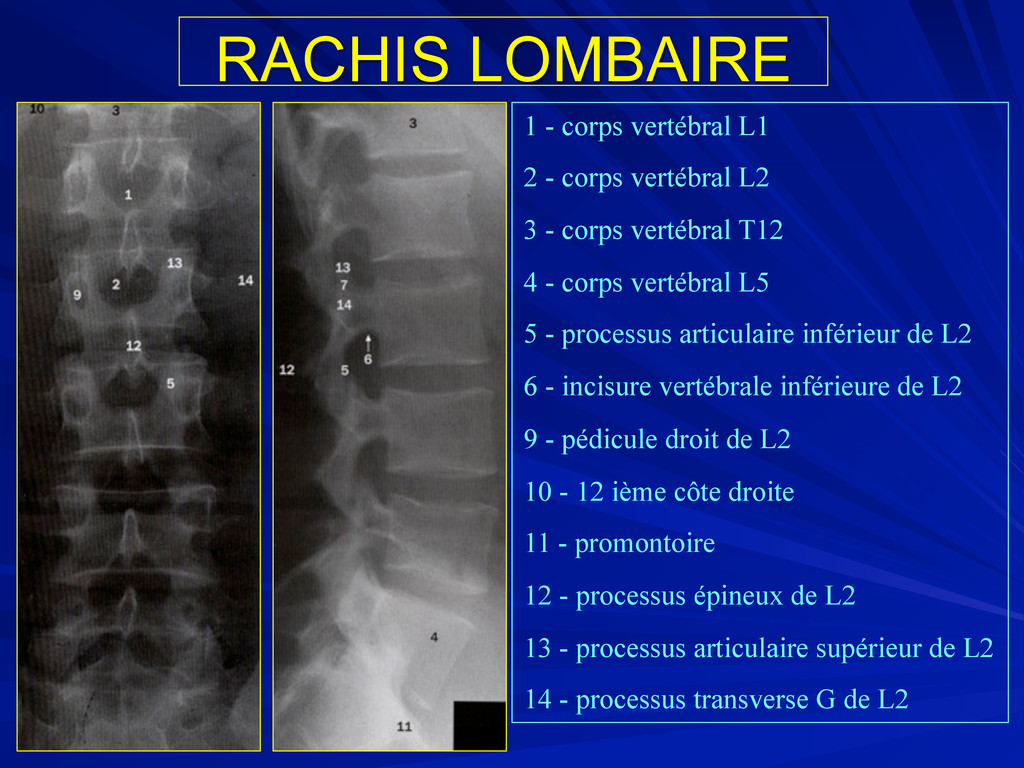
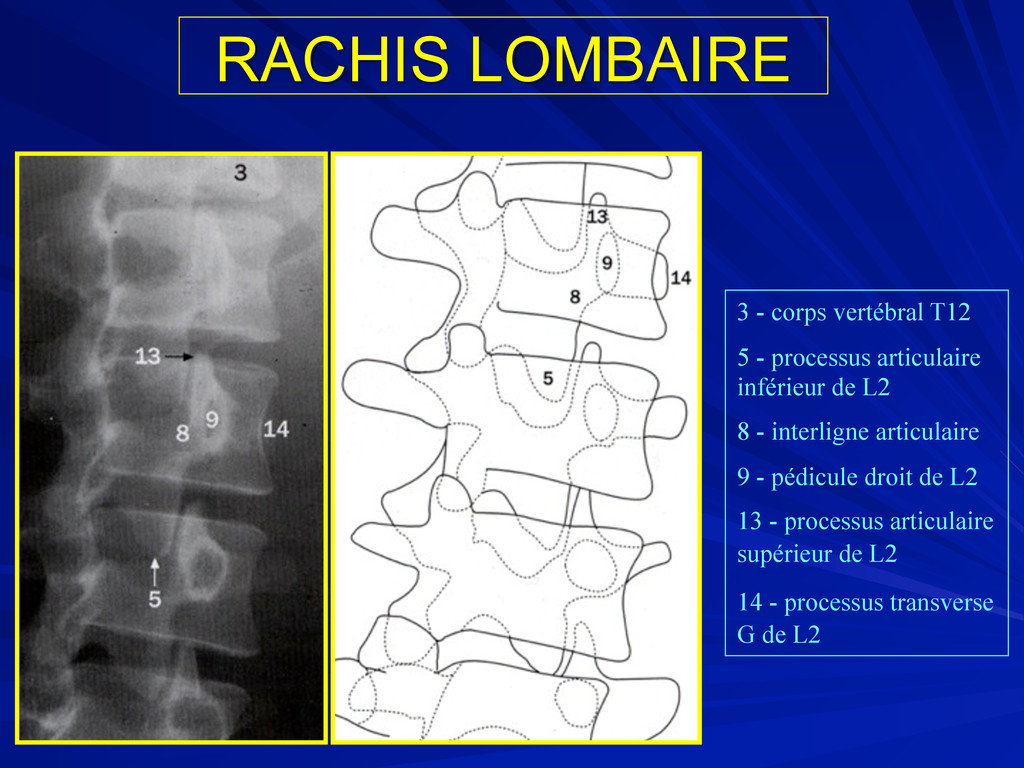
articulaire inférieur de L2 8 - interligne articulaire 9 - pédicule droit de L2 13 - processus articulaire supérieur de L2 14 - processus transverse G de L2
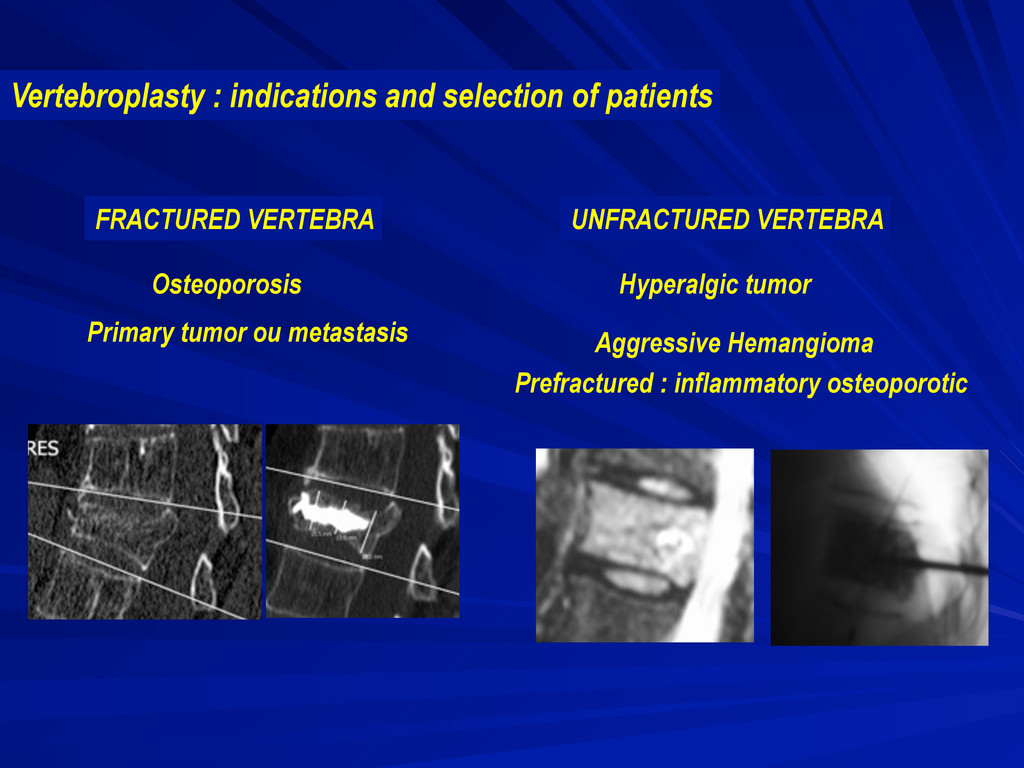
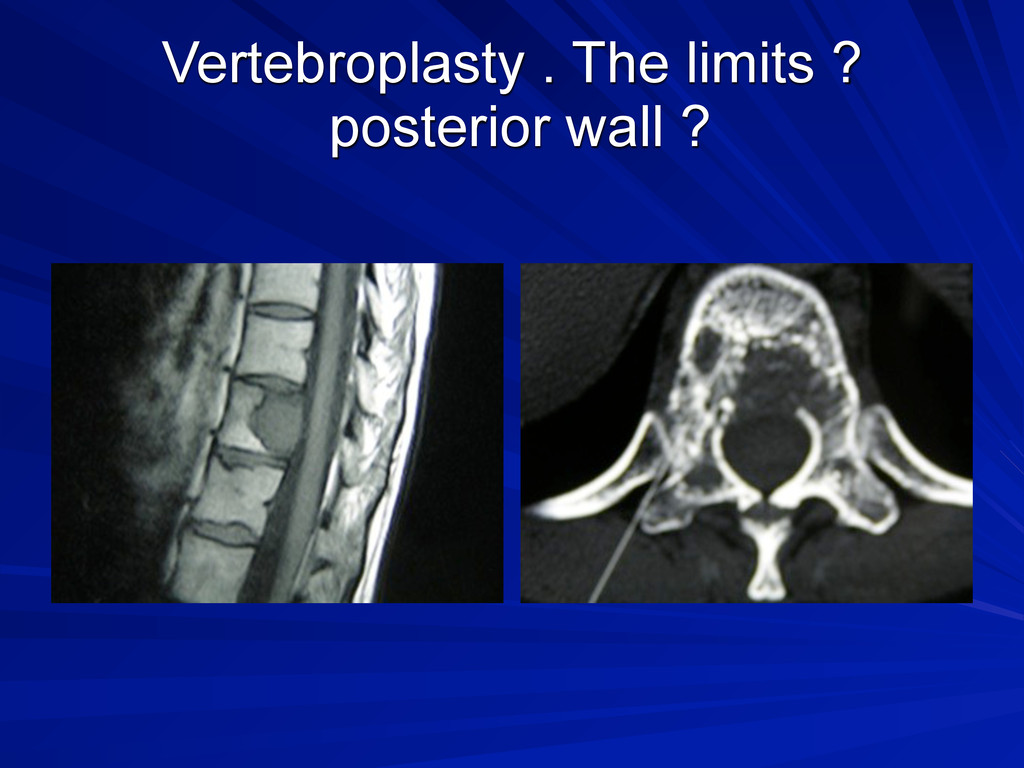
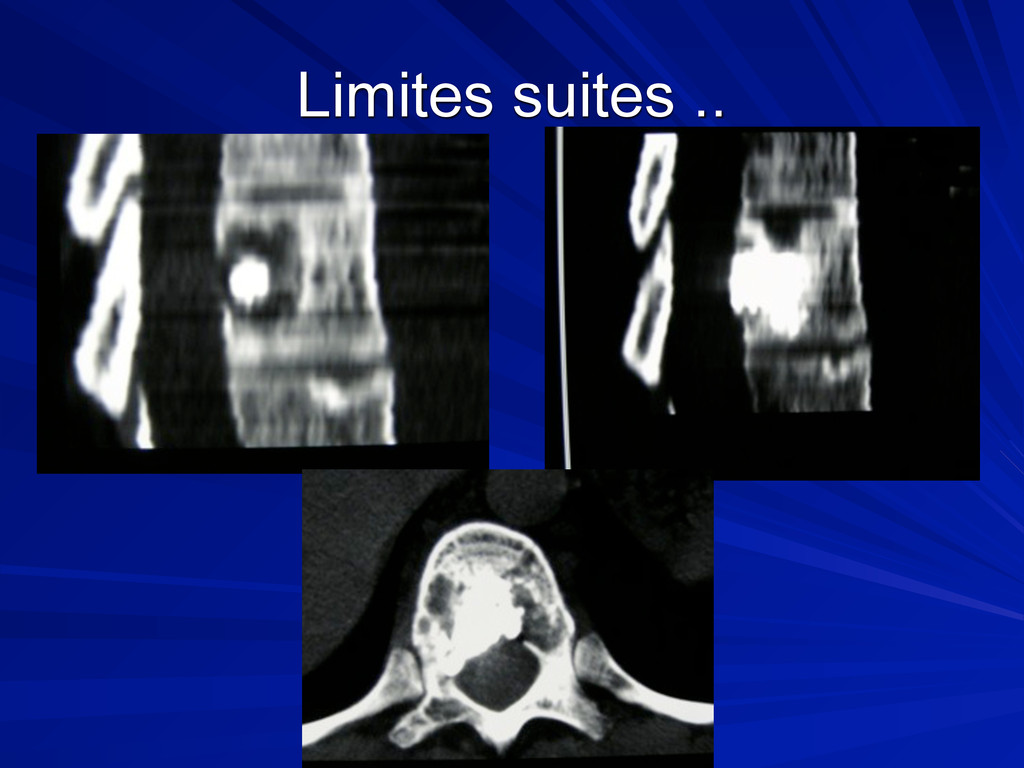
5 grandes ind. : Métas vert.,Myelome, Fr. Vert. Ostéoporotique , angiome vert. Symptomatique, fr. Vert. Traumatique Ds les fractures sur métas rachidienne l’effet antalgique est immédiat et sera complété par la radiothérapie la rupture du mur post. N’est pas une CI La présence de signe méd ou radiculaire sont le + svt une CI
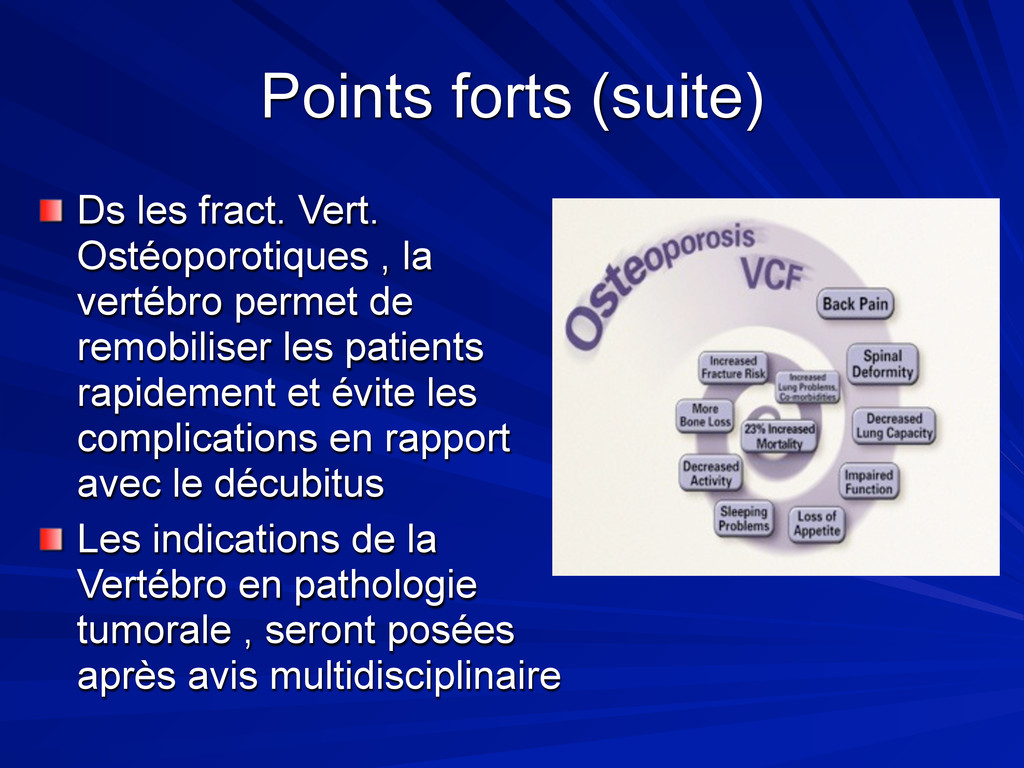
vertébro permet de remobiliser les patients rapidement et évite les complications en rapport avec le décubitus Les indications de la Vertébro en pathologie tumorale , seront posées après avis multidisciplinaire
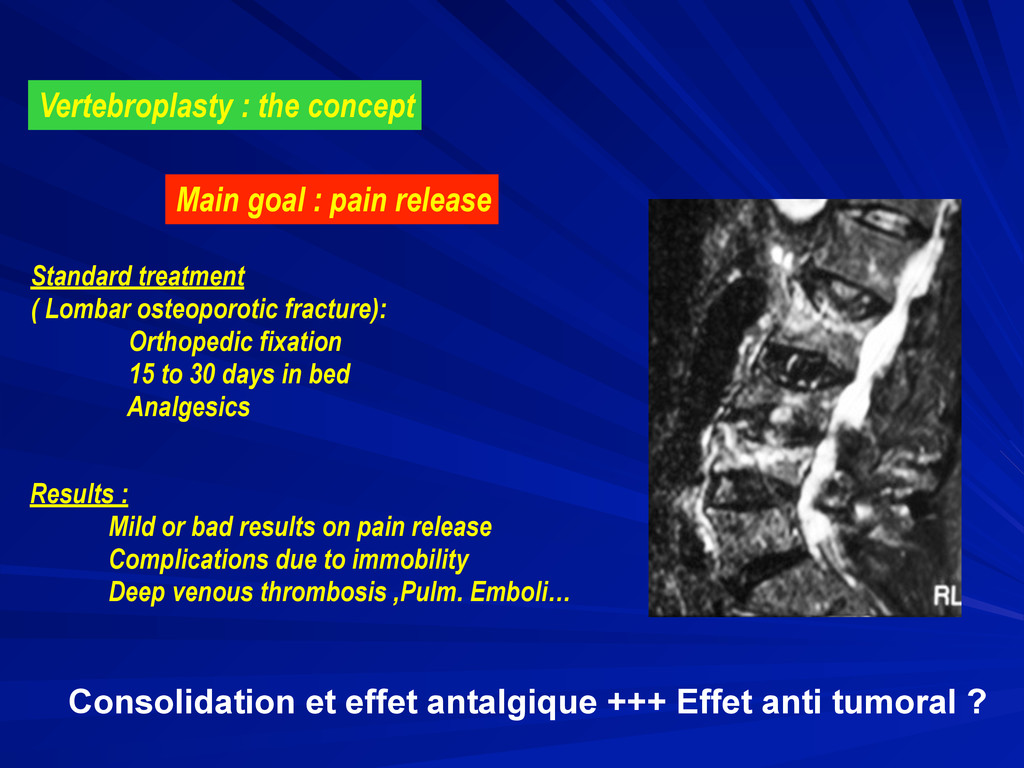
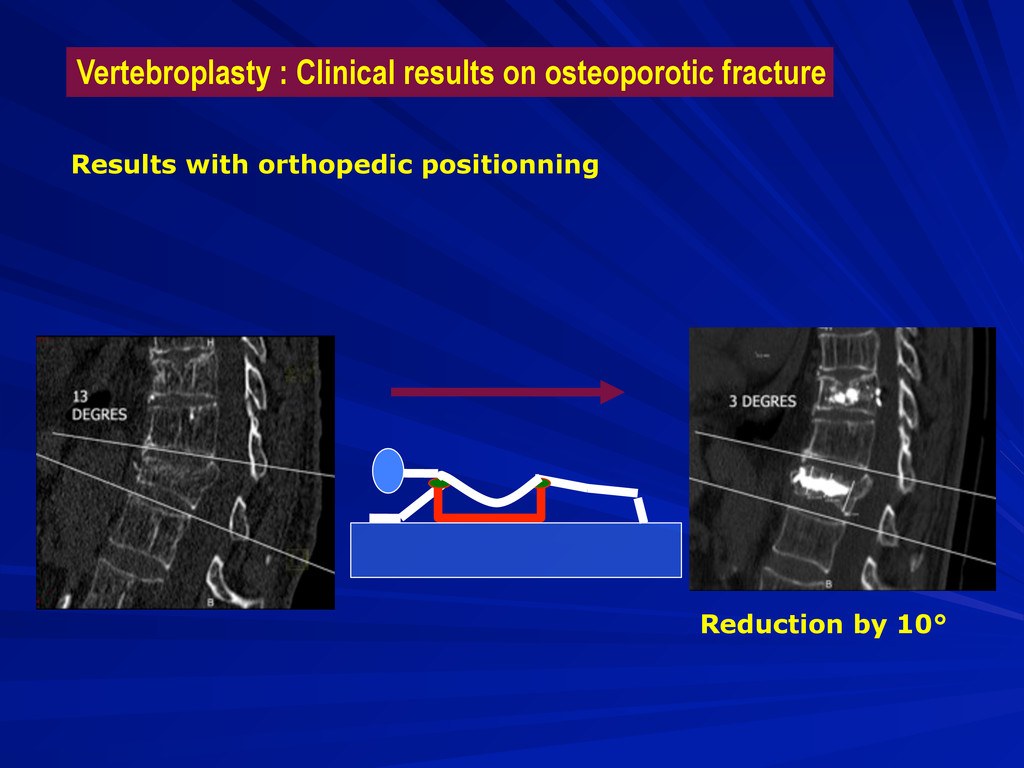
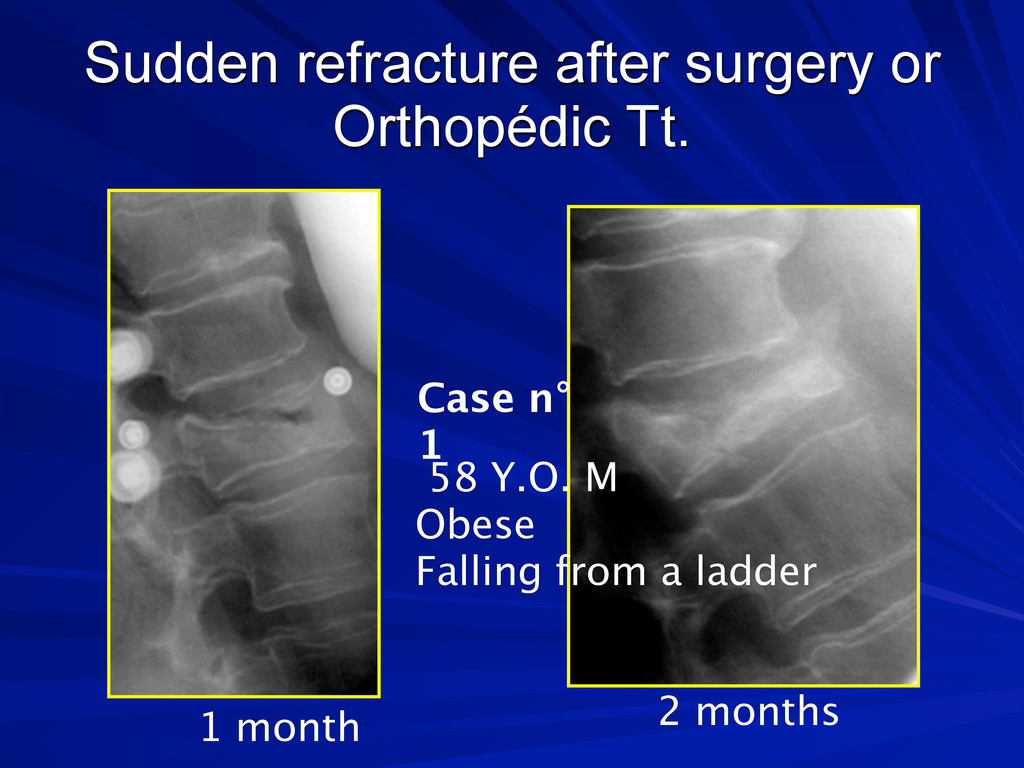
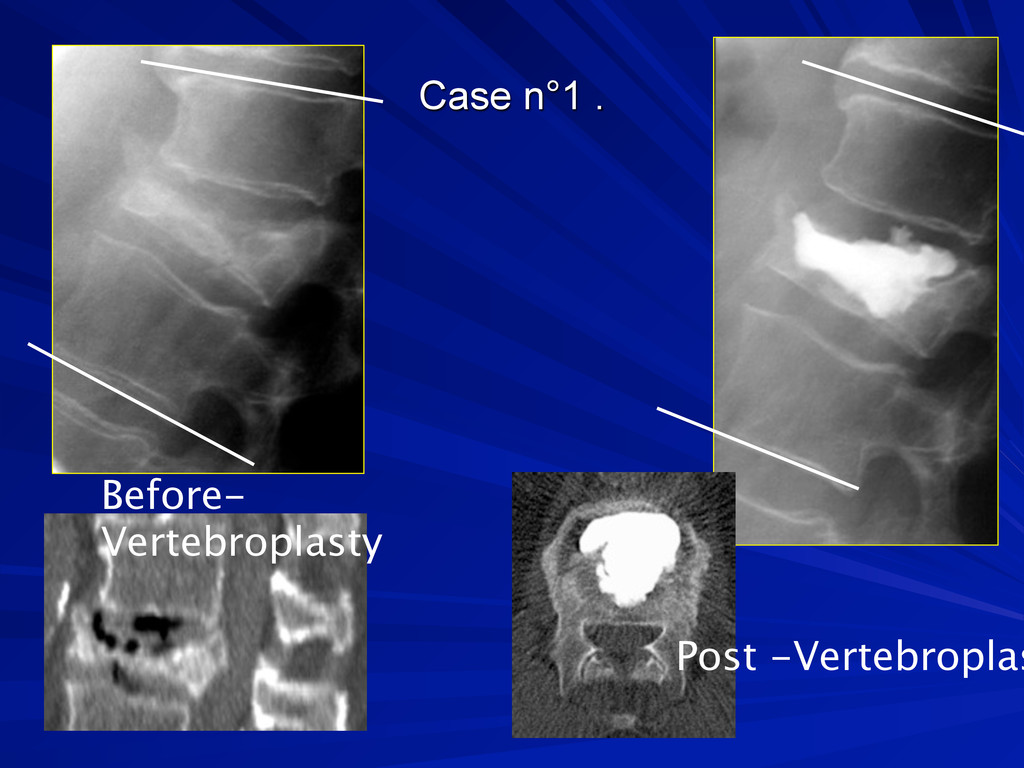
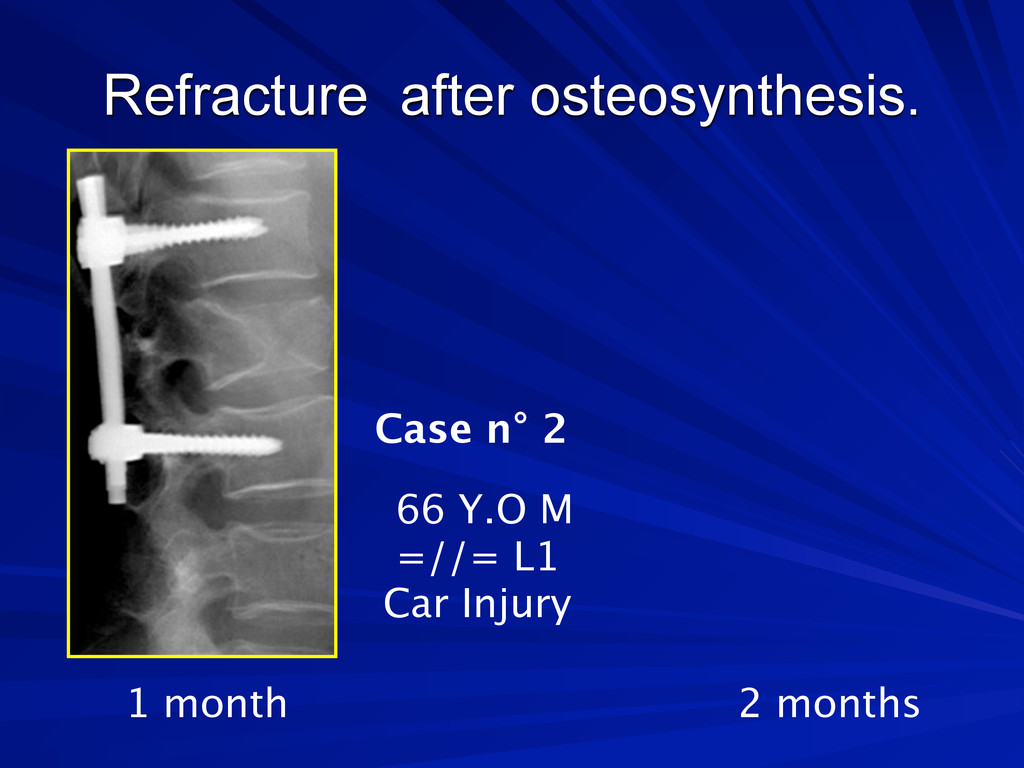
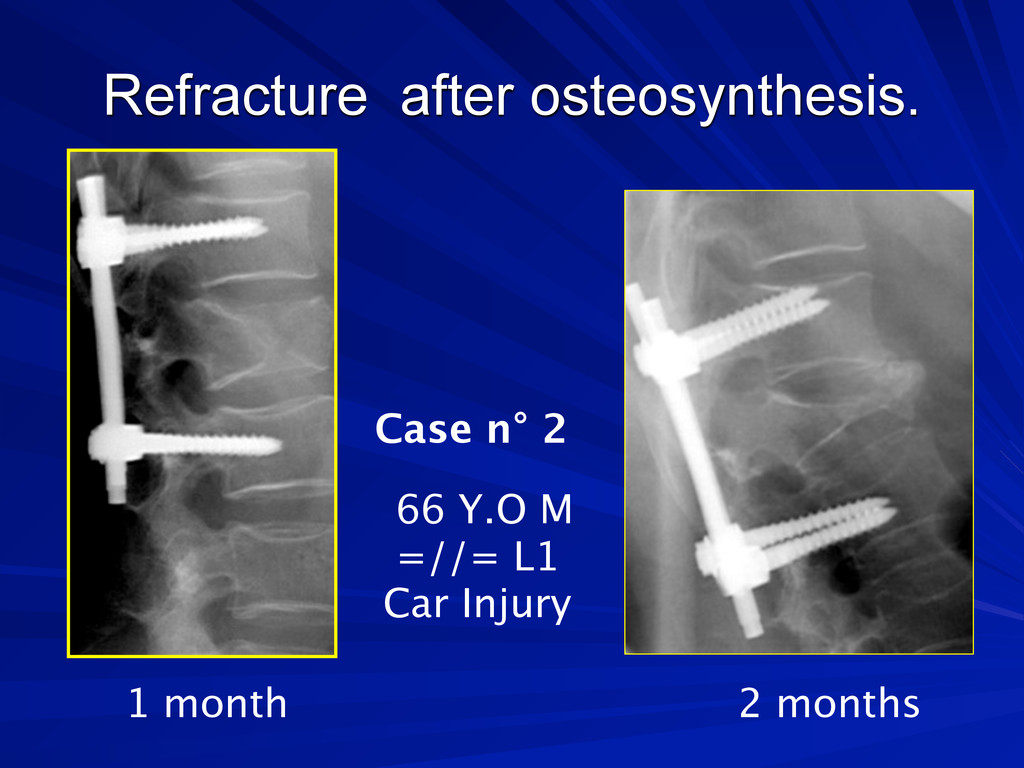
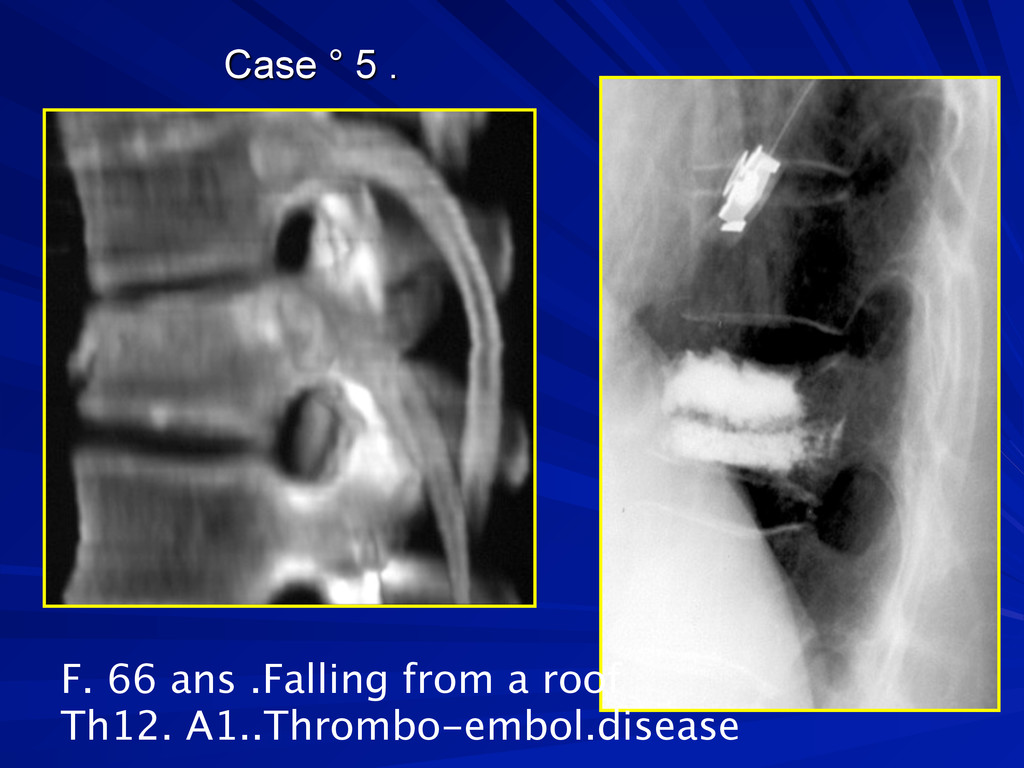
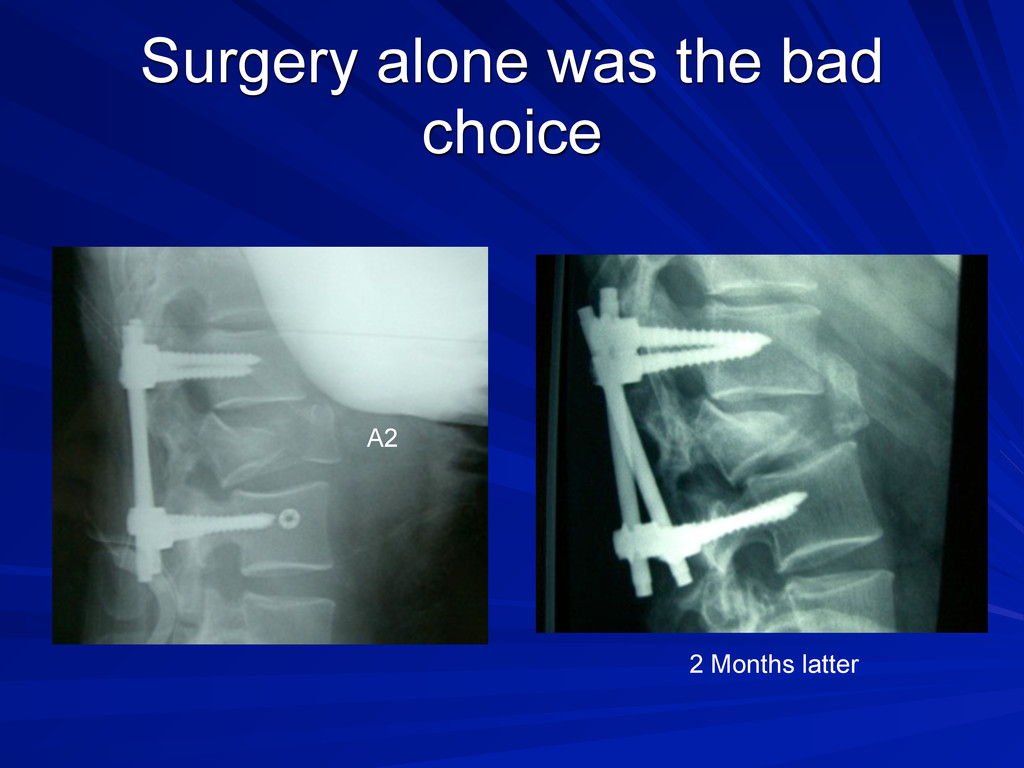
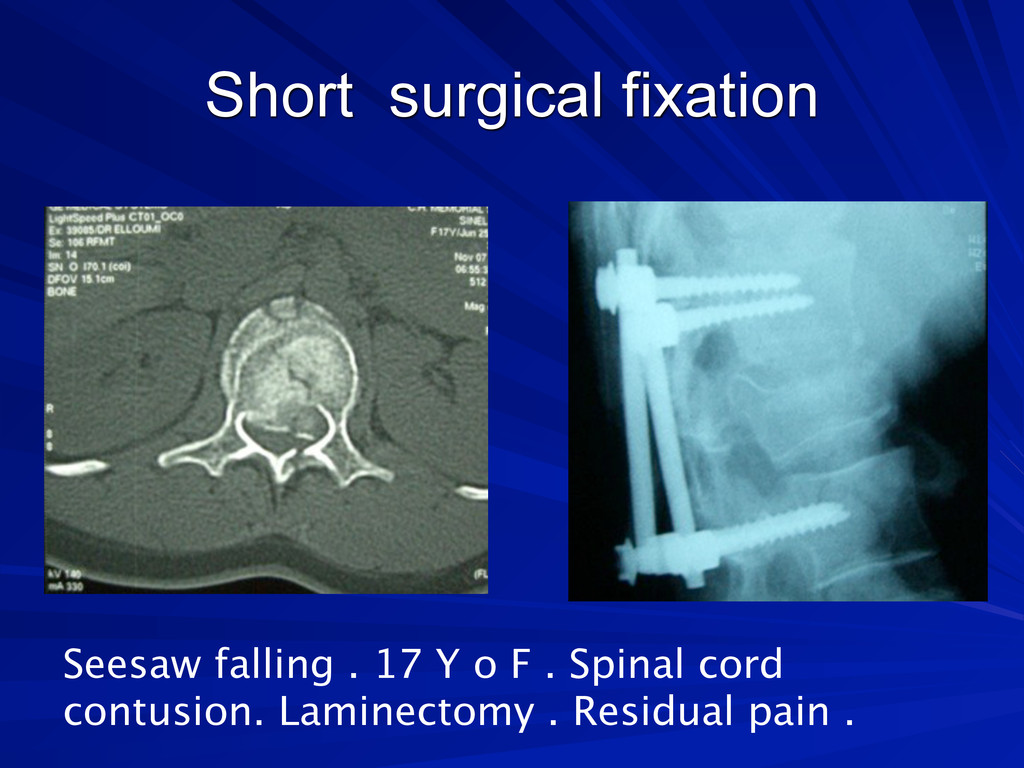
treatment ( Lombar osteoporotic fracture): Orthopedic fixation 15 to 30 days in bed Analgesics Results : Mild or bad results on pain release Complications due to immobility Deep venous thrombosis ,Pulm. Emboli… Consolidation et effet antalgique +++ Effet anti tumoral ?
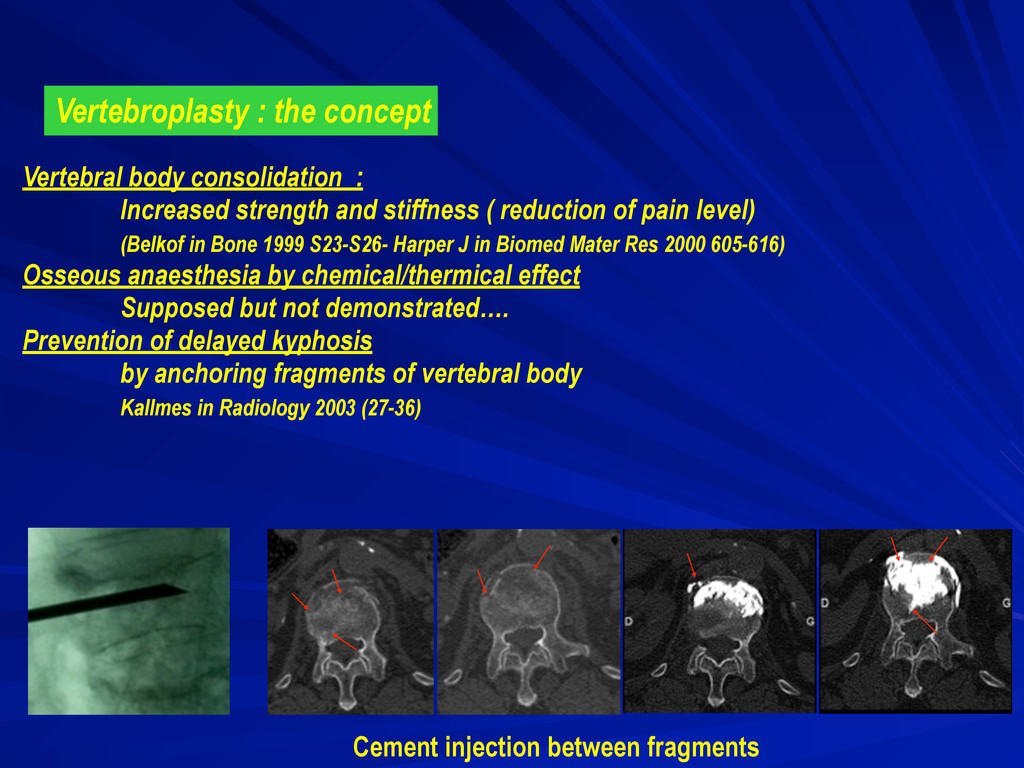
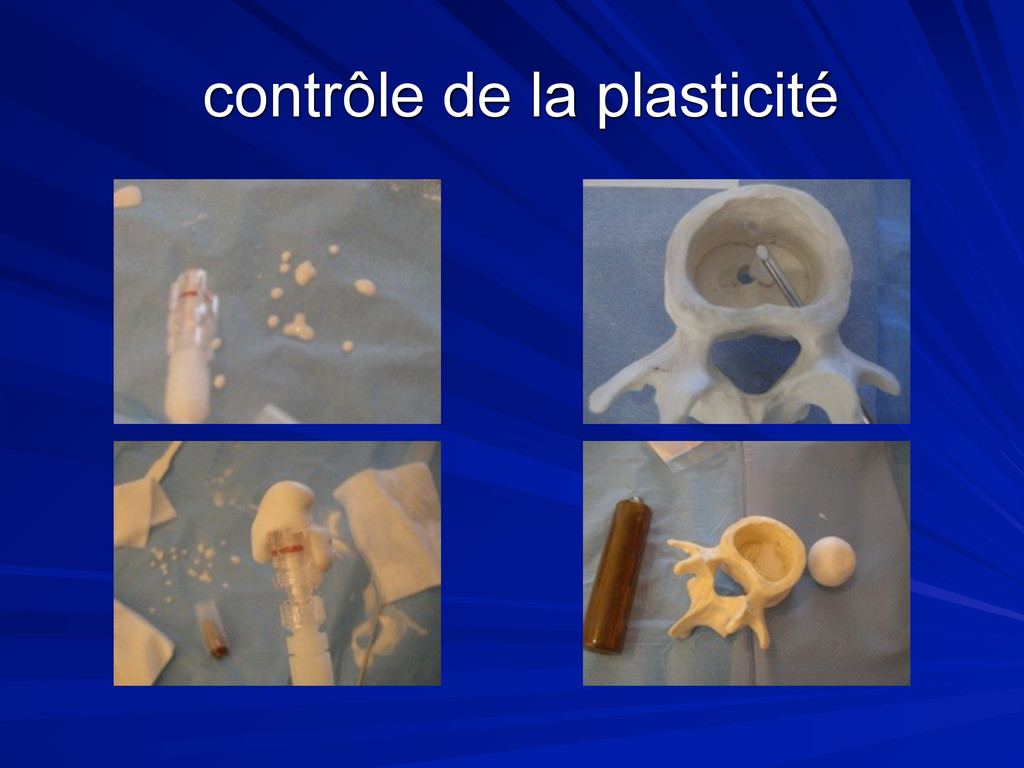
and stiffness ( reduction of pain level) (Belkof in Bone 1999 S23-S26- Harper J in Biomed Mater Res 2000 605-616) Osseous anaesthesia by chemical/thermical effect Supposed but not demonstrated…. Prevention of delayed kyphosis by anchoring fragments of vertebral body Kallmes in Radiology 2003 (27-36) Cement injection between fragments
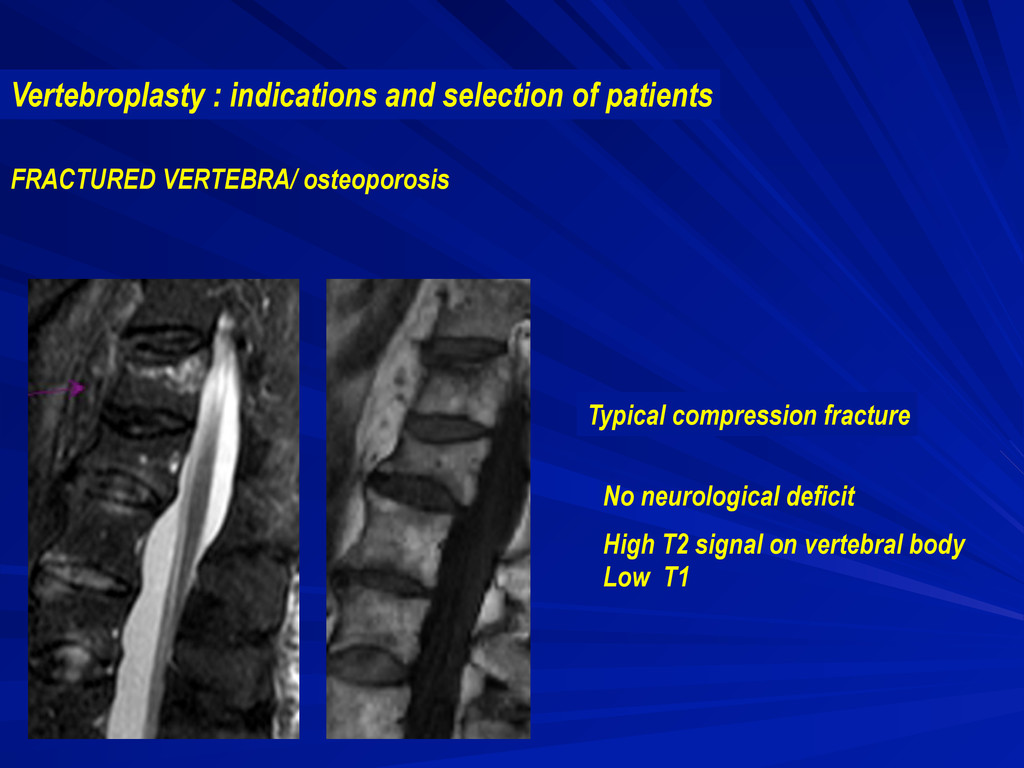
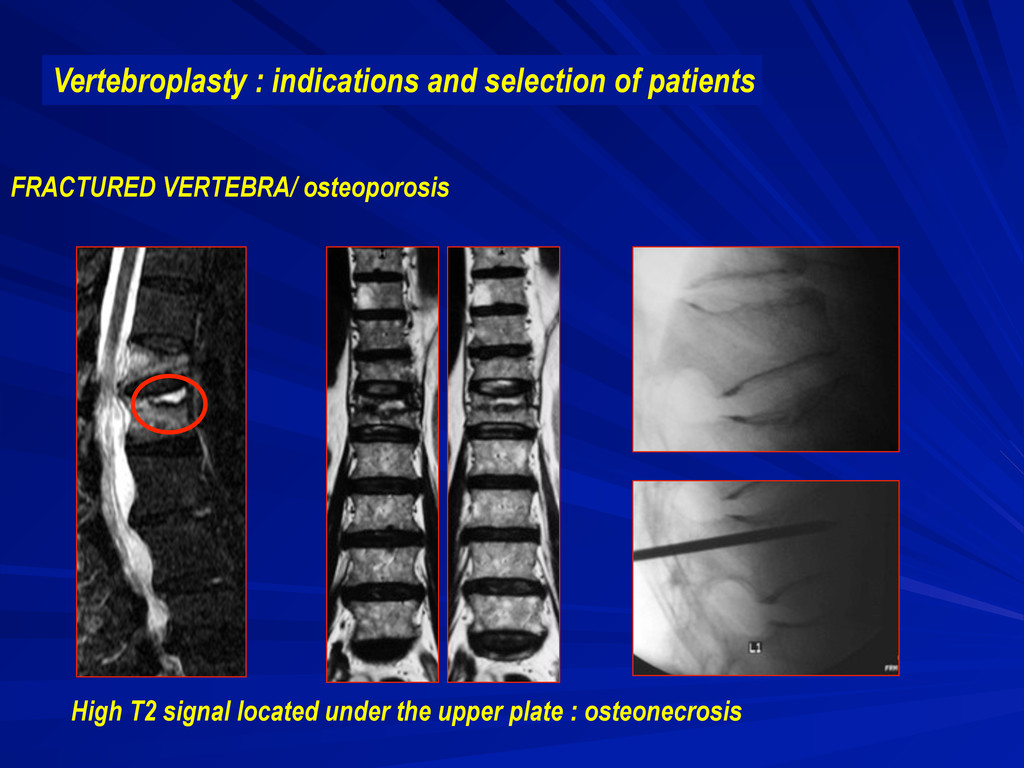
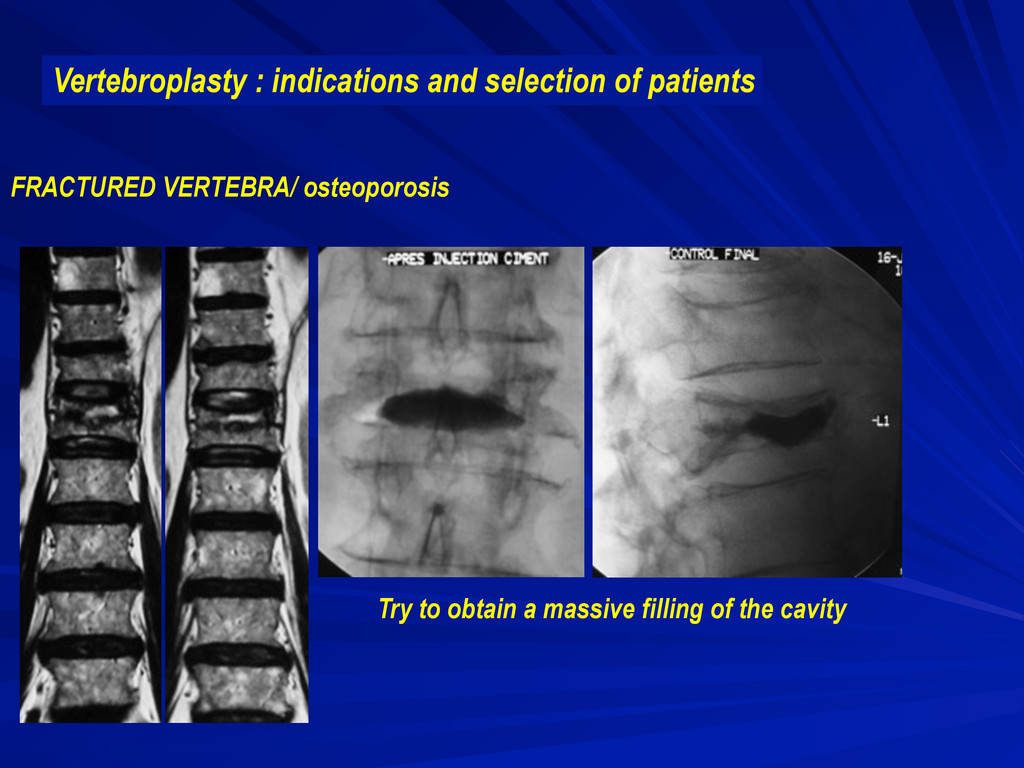
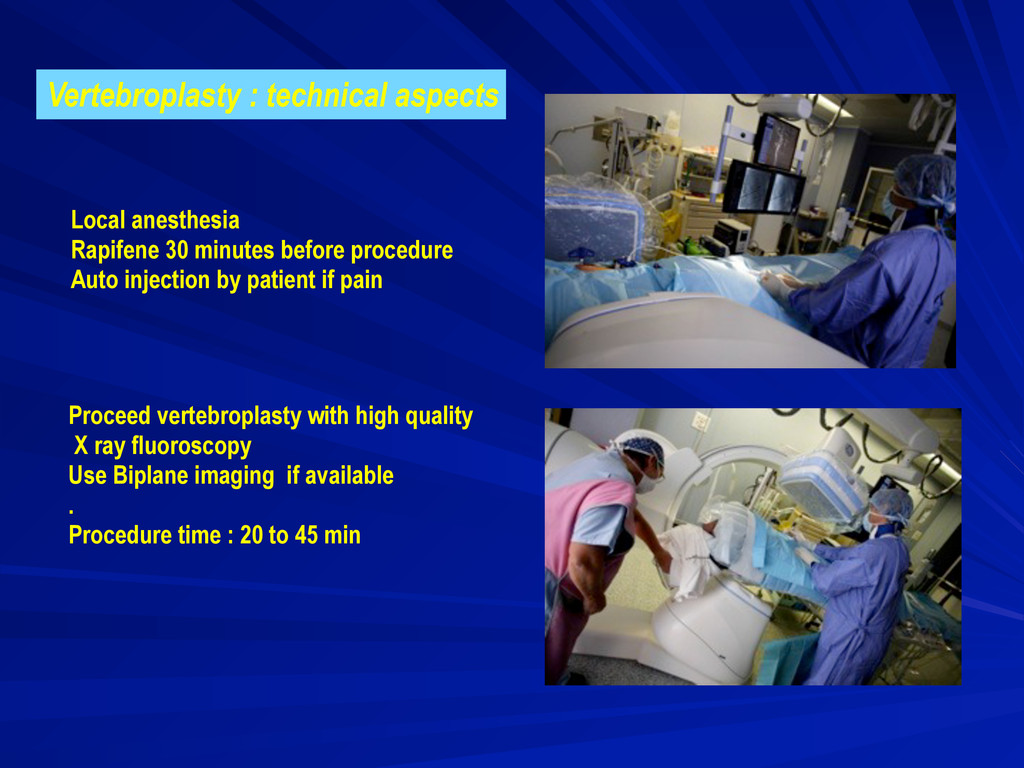
osteoporosis Best and most popular indication in France for vertebroplasty 800 000 Vertebral compression fracture every year in the world Almost all patient can be treated because contra-indications are very rare. Local anesthesia No neurological deficit
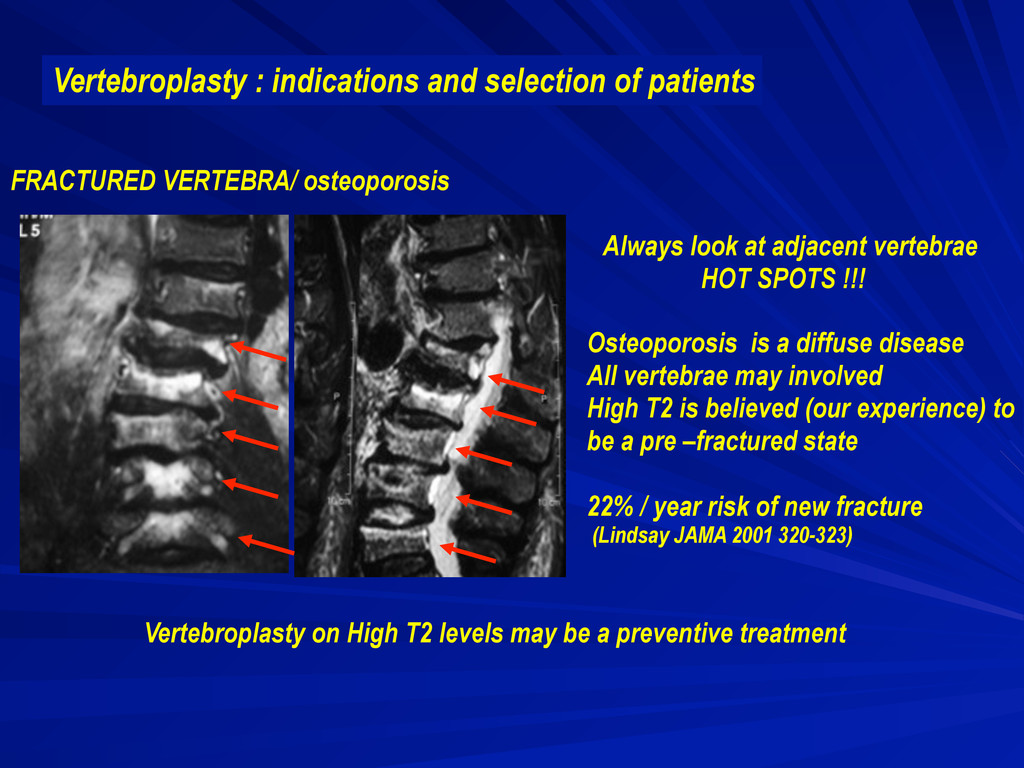
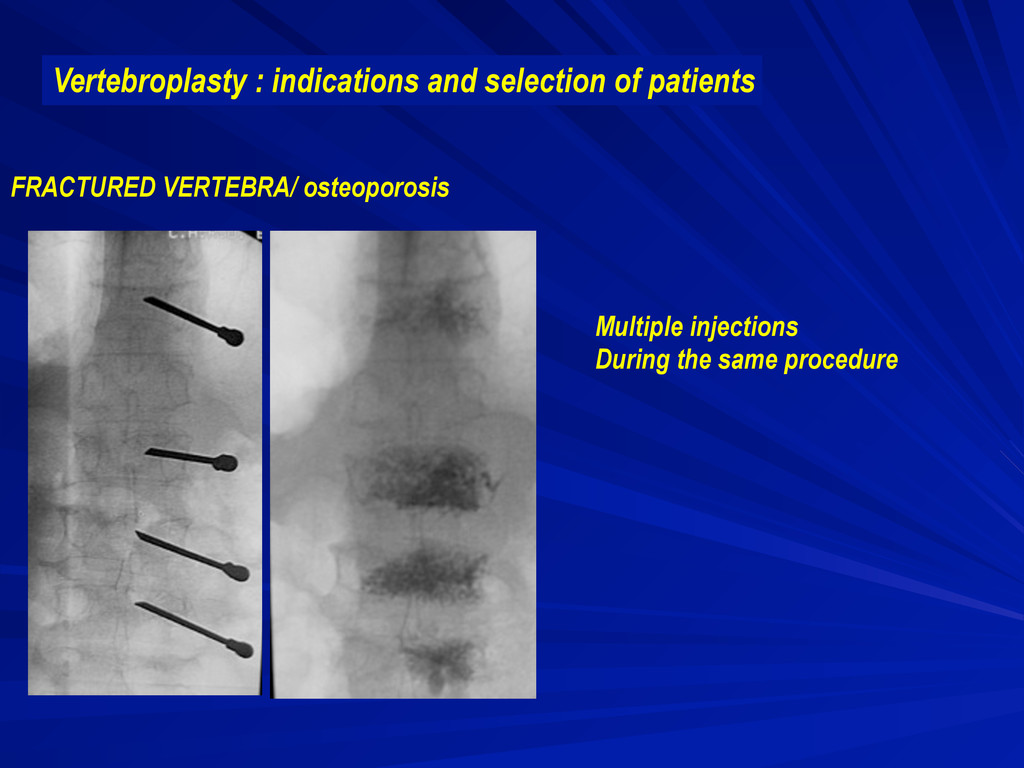
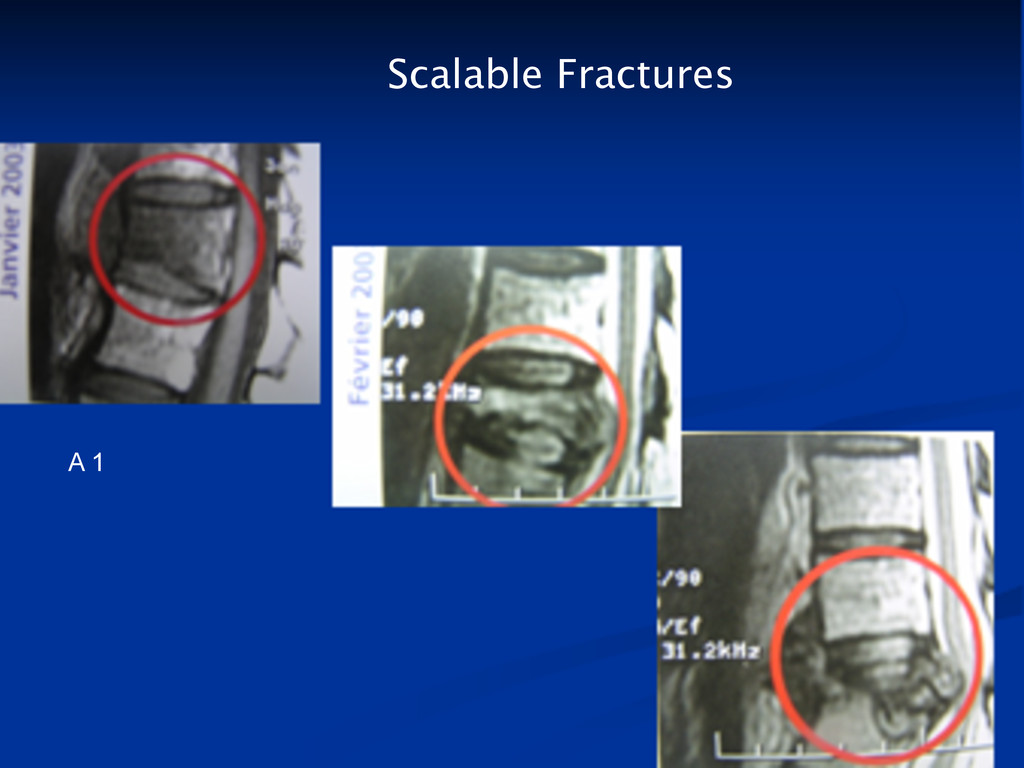
Always look at adjacent vertebrae HOT SPOTS !!! Osteoporosis is a diffuse disease All vertebrae may involved High T2 is believed (our experience) to be a pre –fractured state 22% / year risk of new fracture (Lindsay JAMA 2001 320-323) Vertebroplasty on High T2 levels may be a preventive treatment
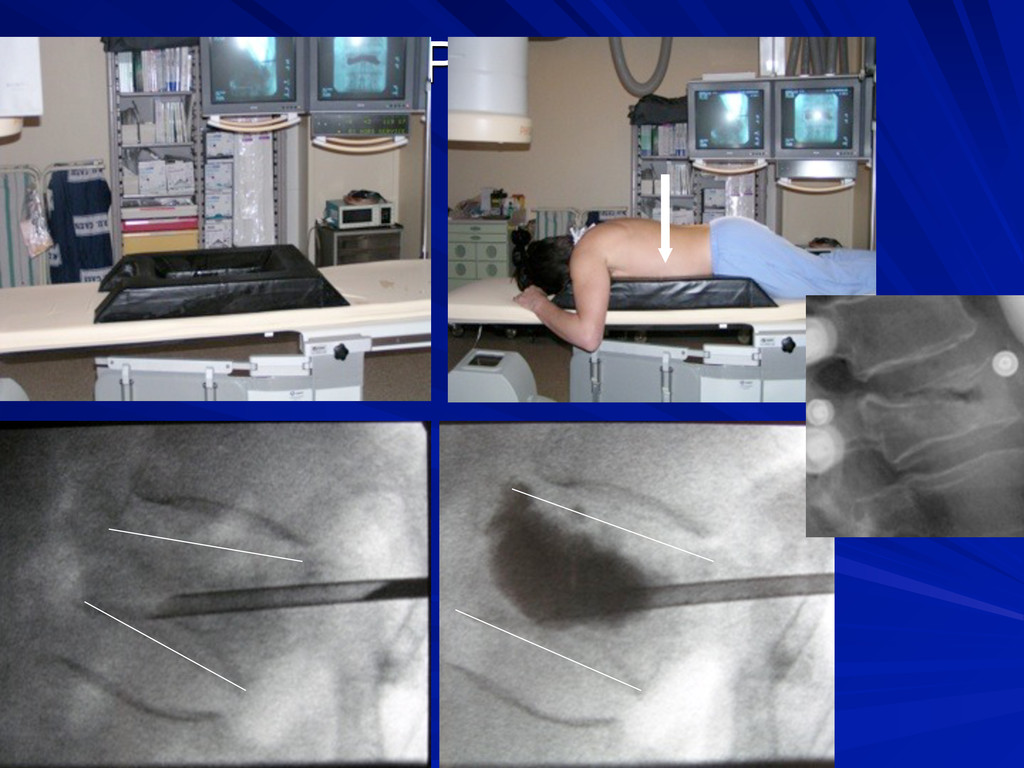
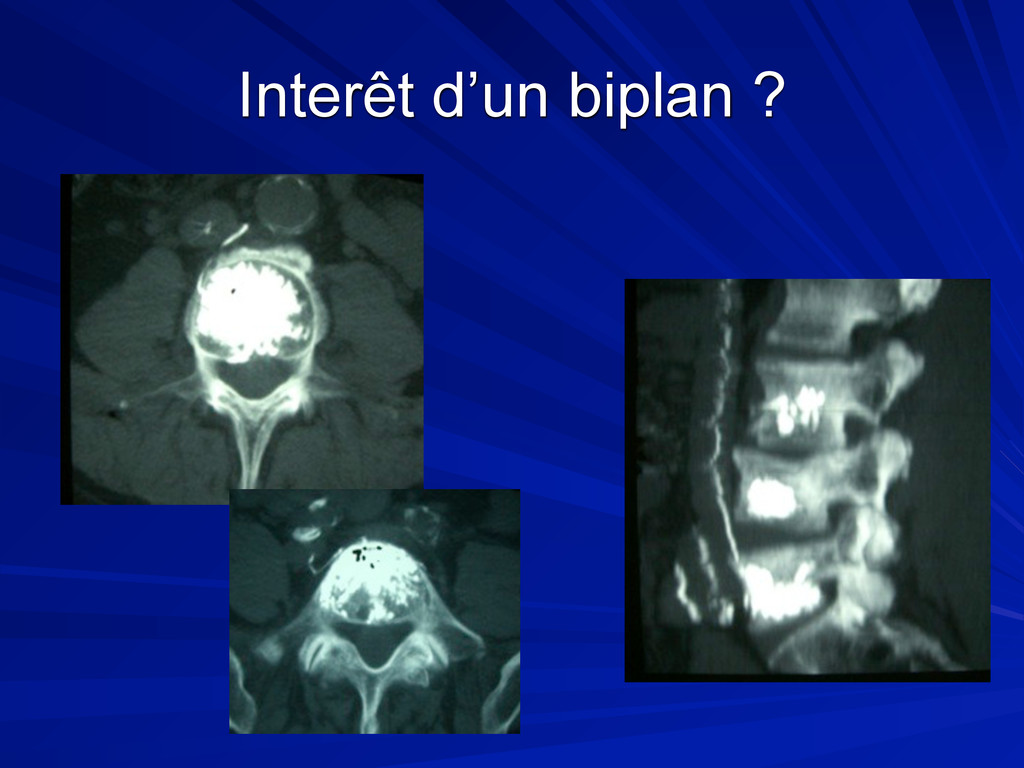
procedure Auto injection by patient if pain Proceed vertebroplasty with high quality X ray fluoroscopy Use Biplane imaging if available . Procedure time : 20 to 45 min
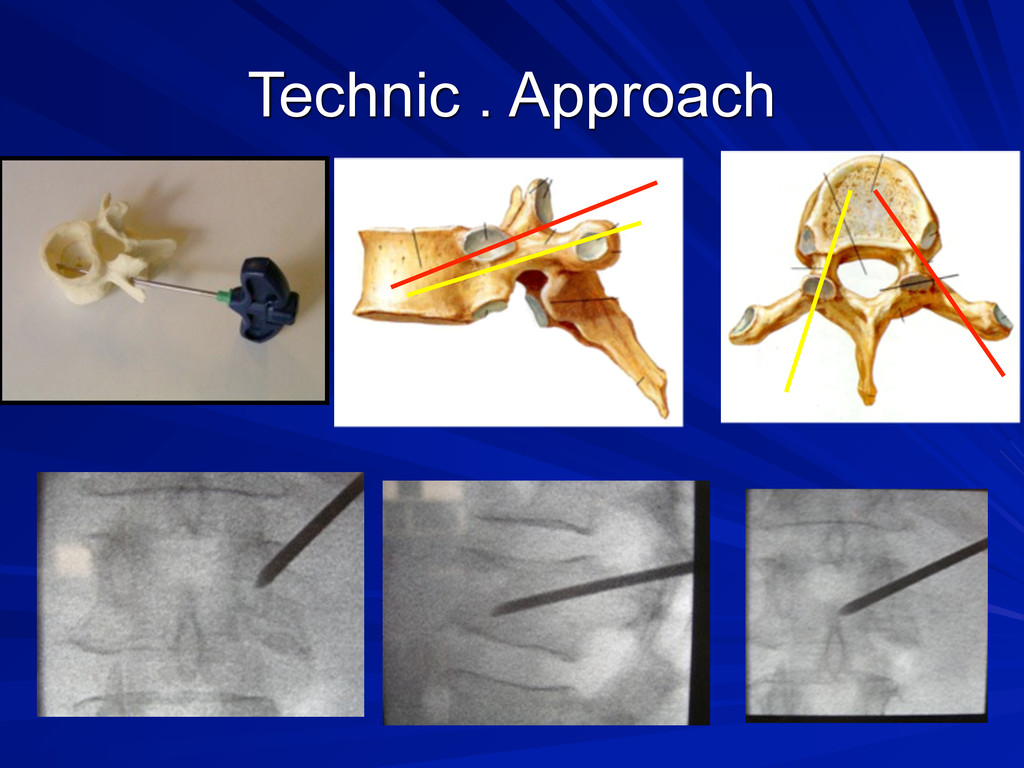
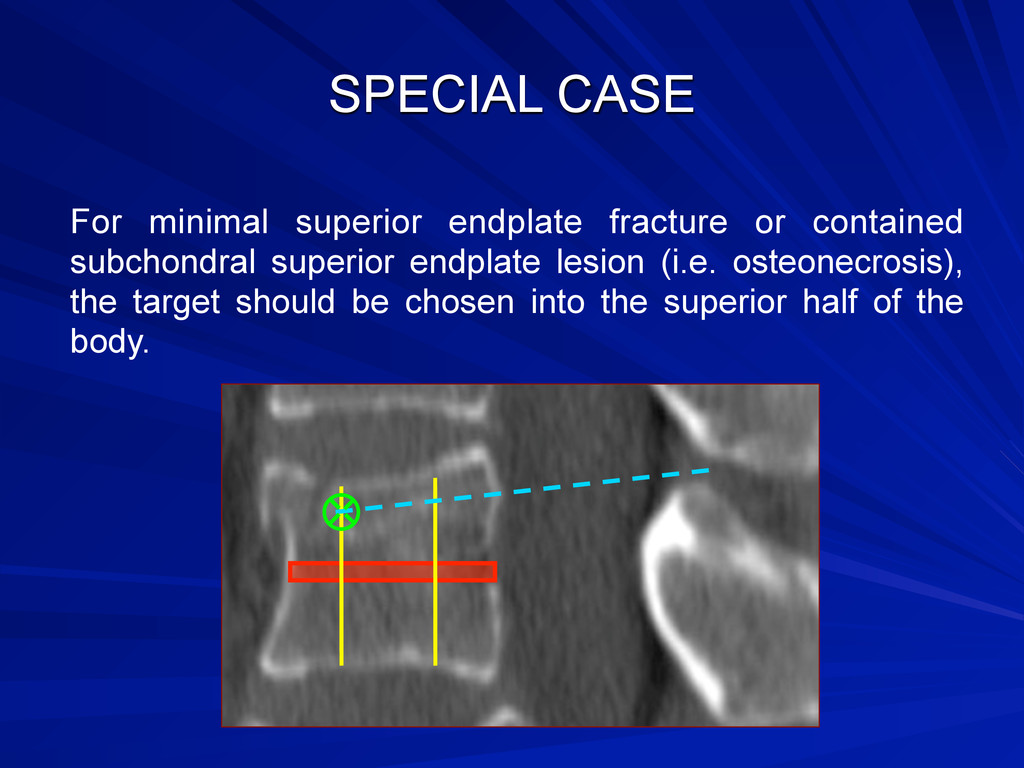
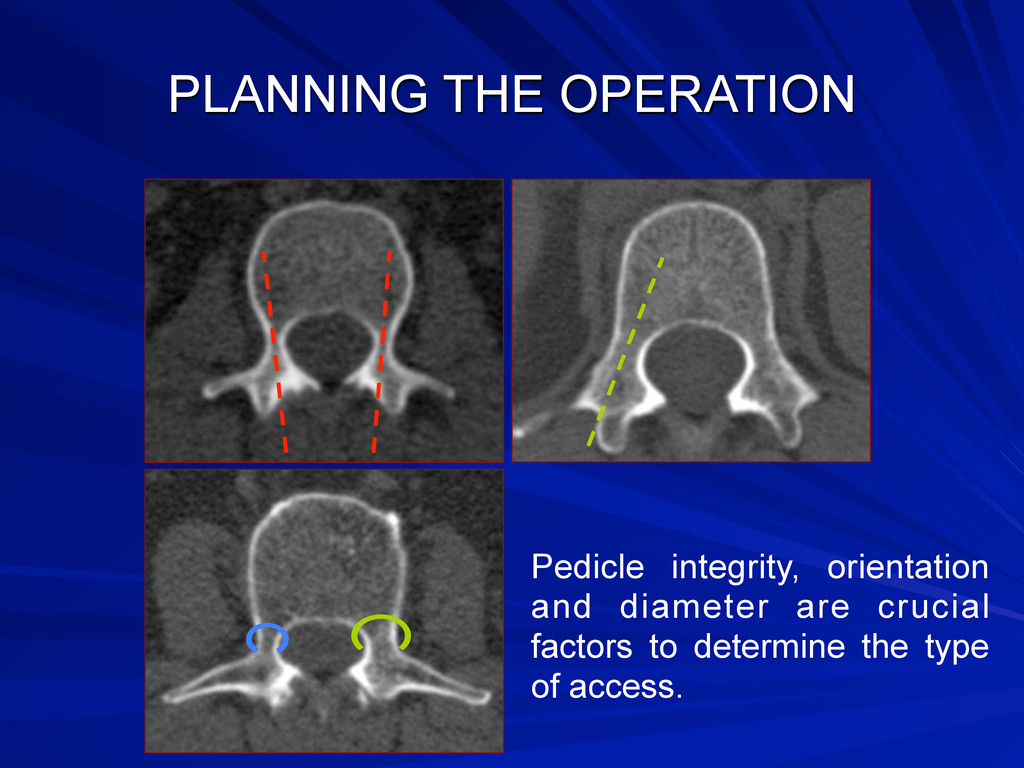
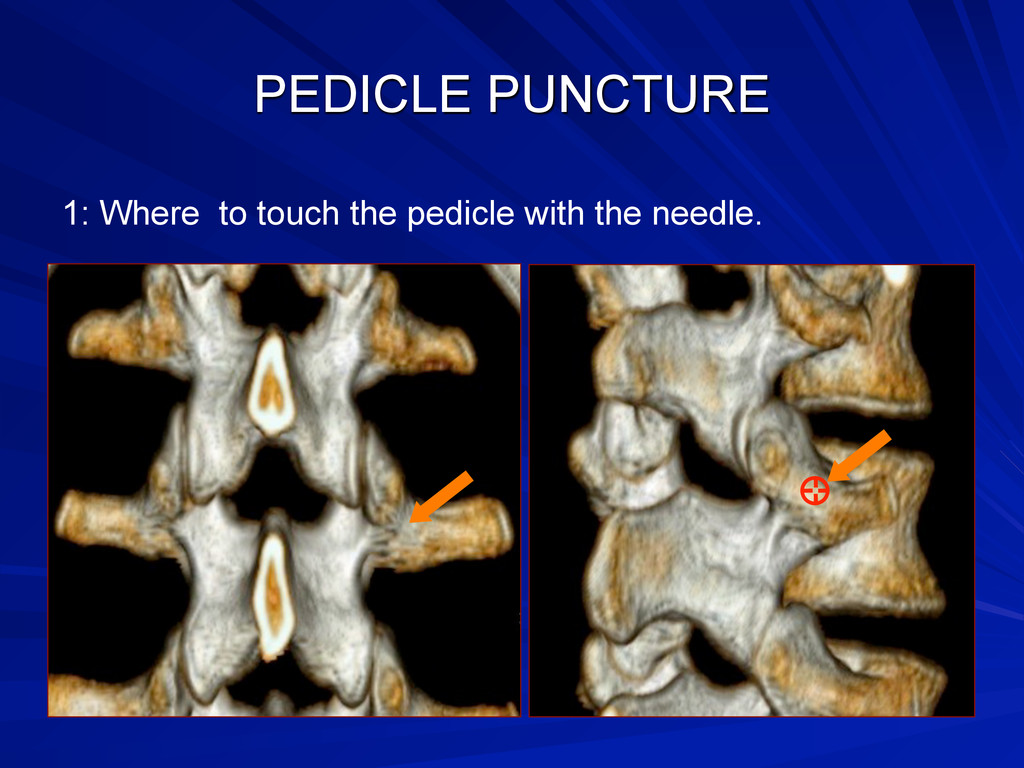
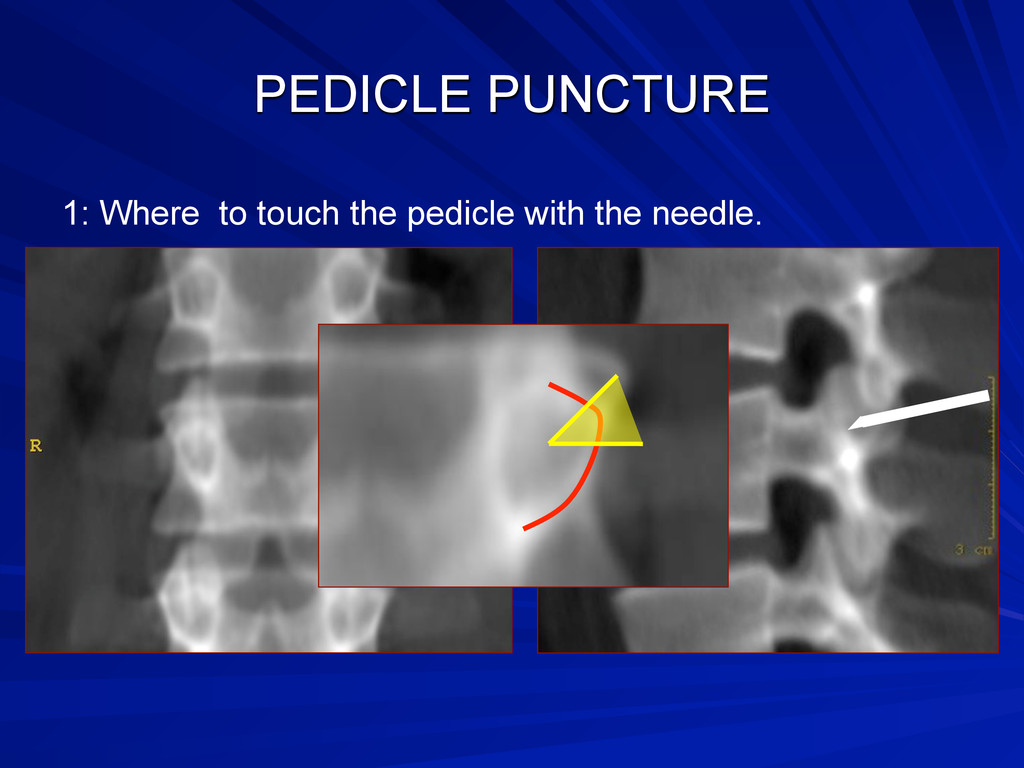
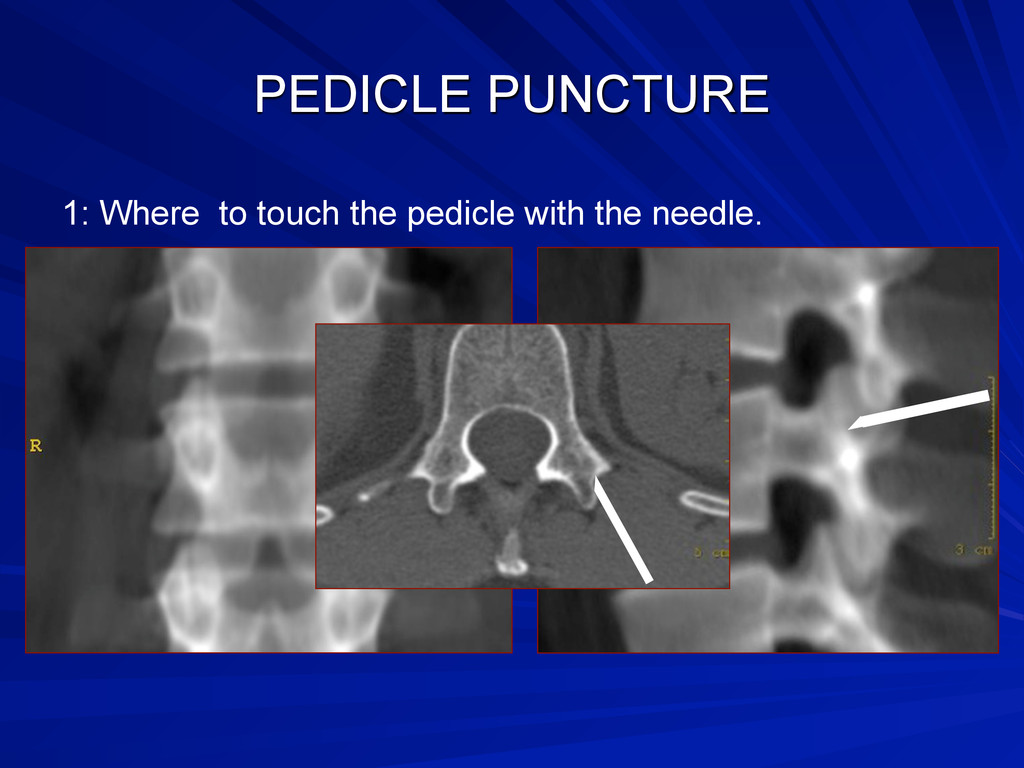
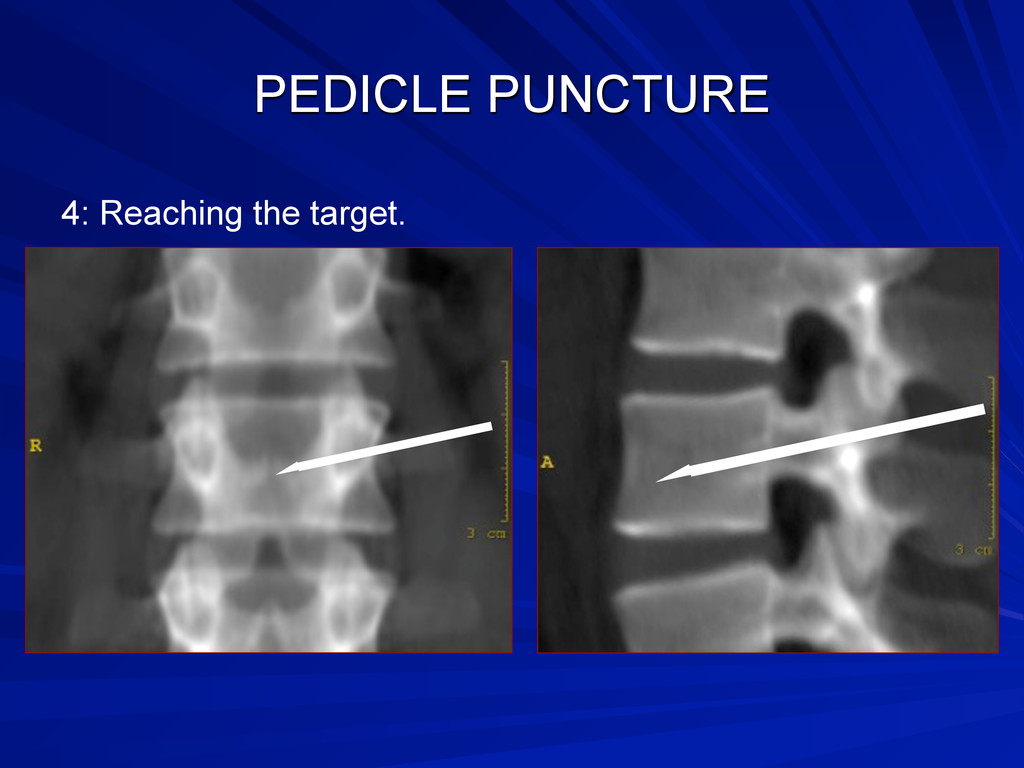
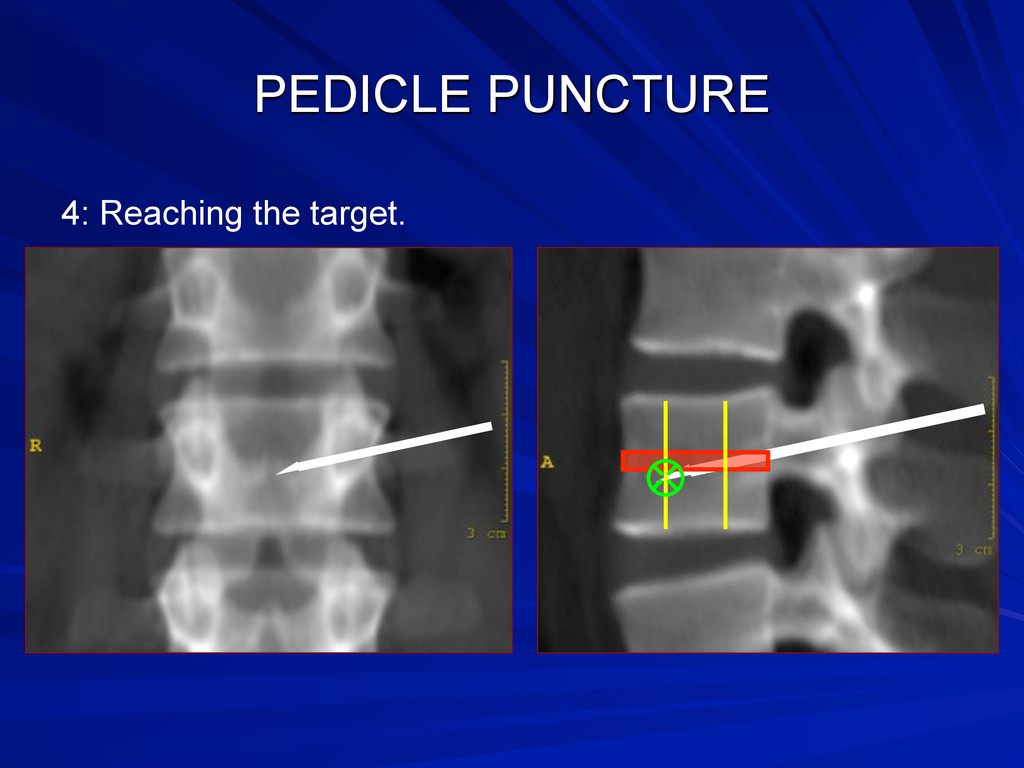
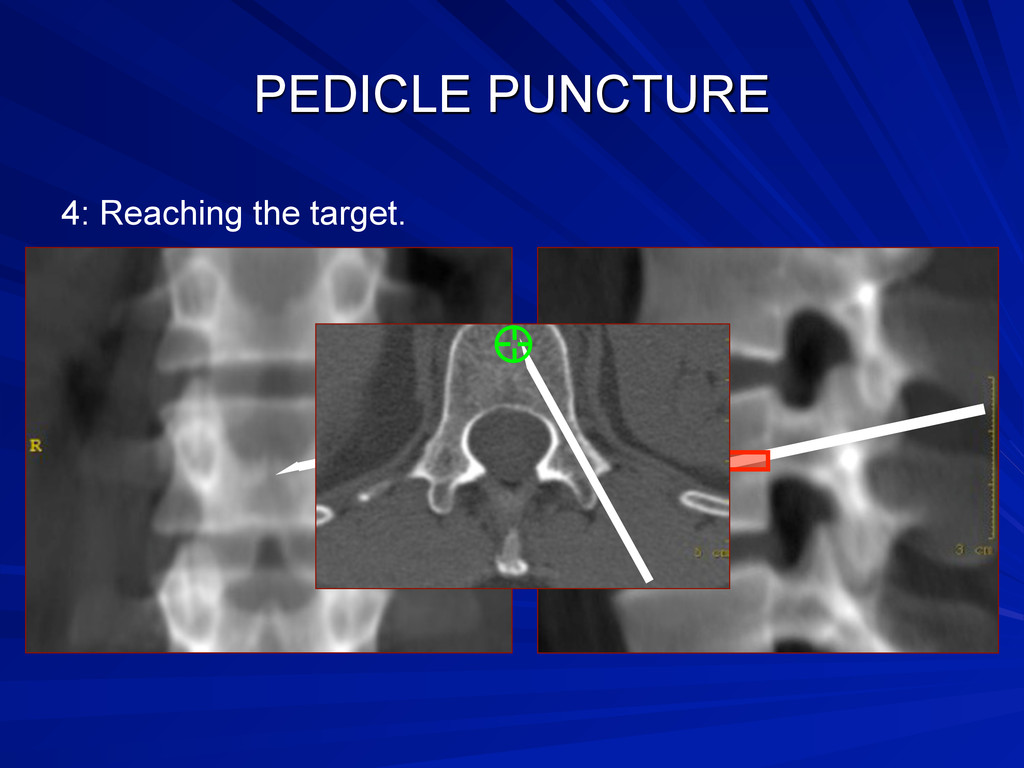
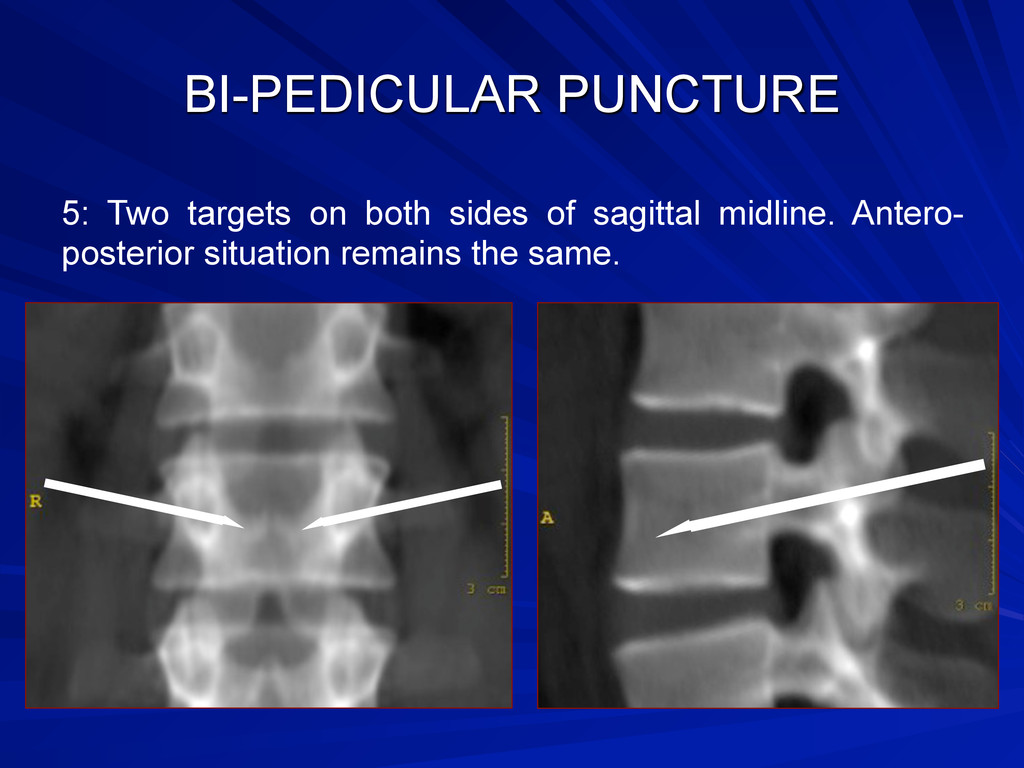
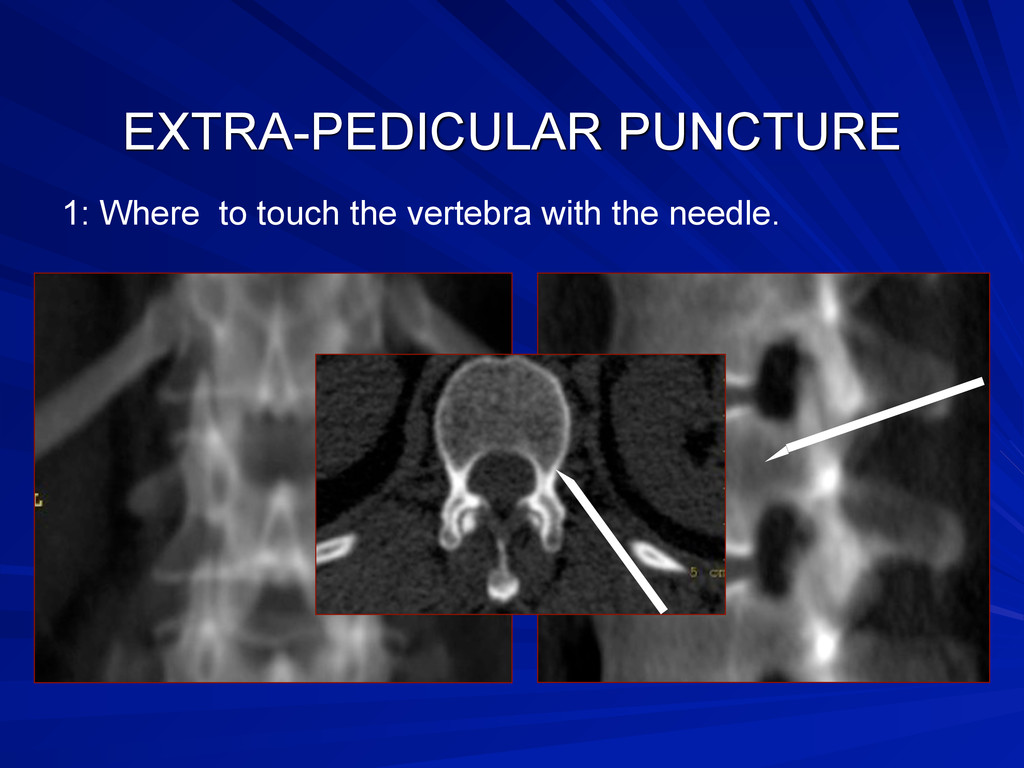
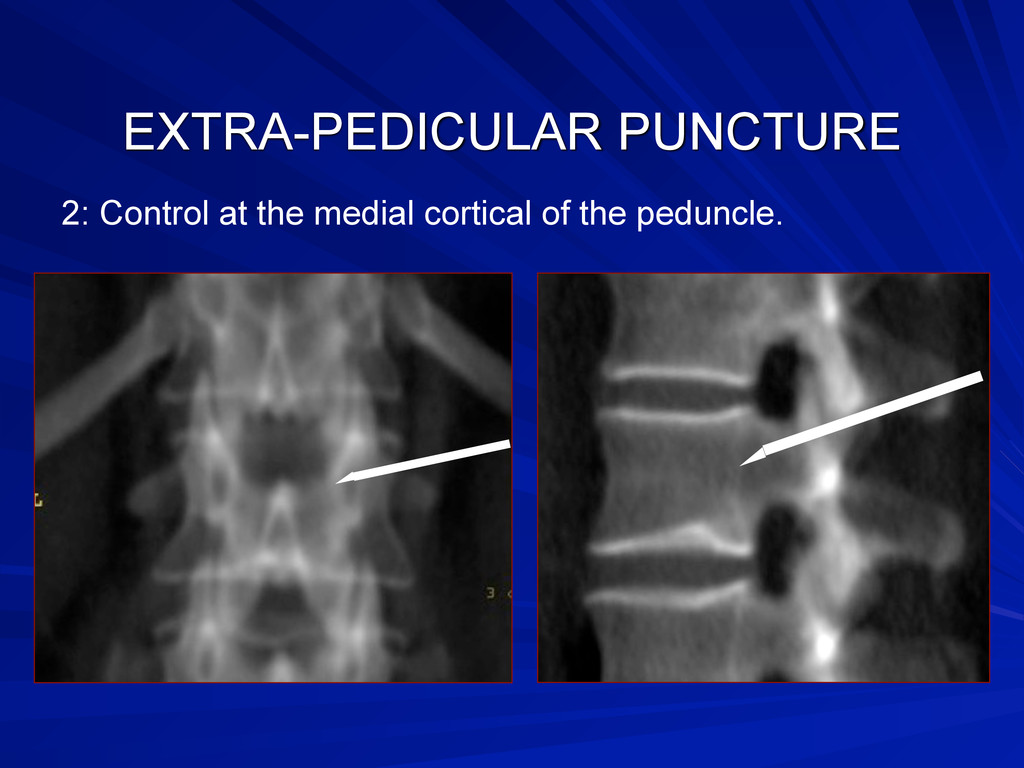
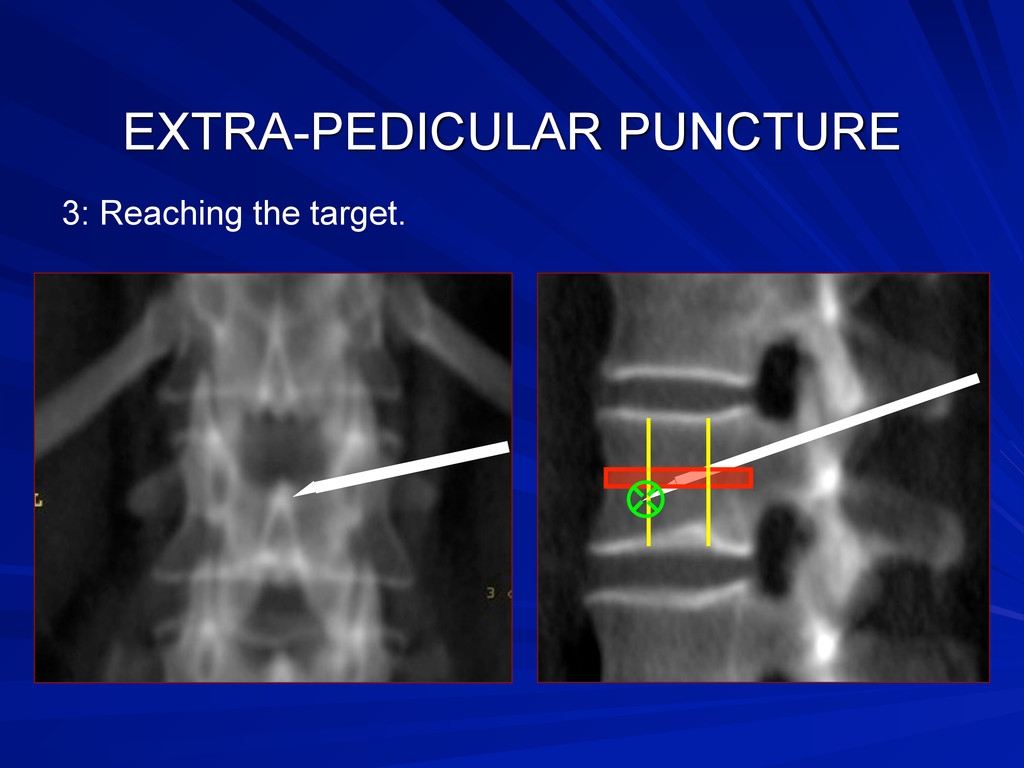
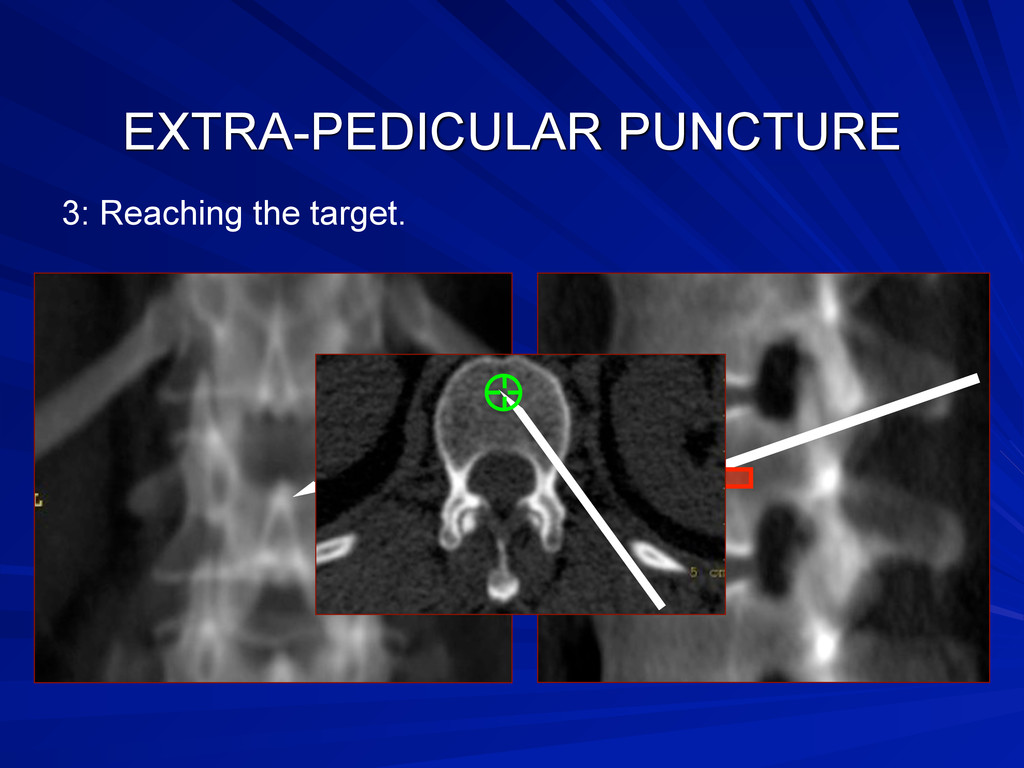
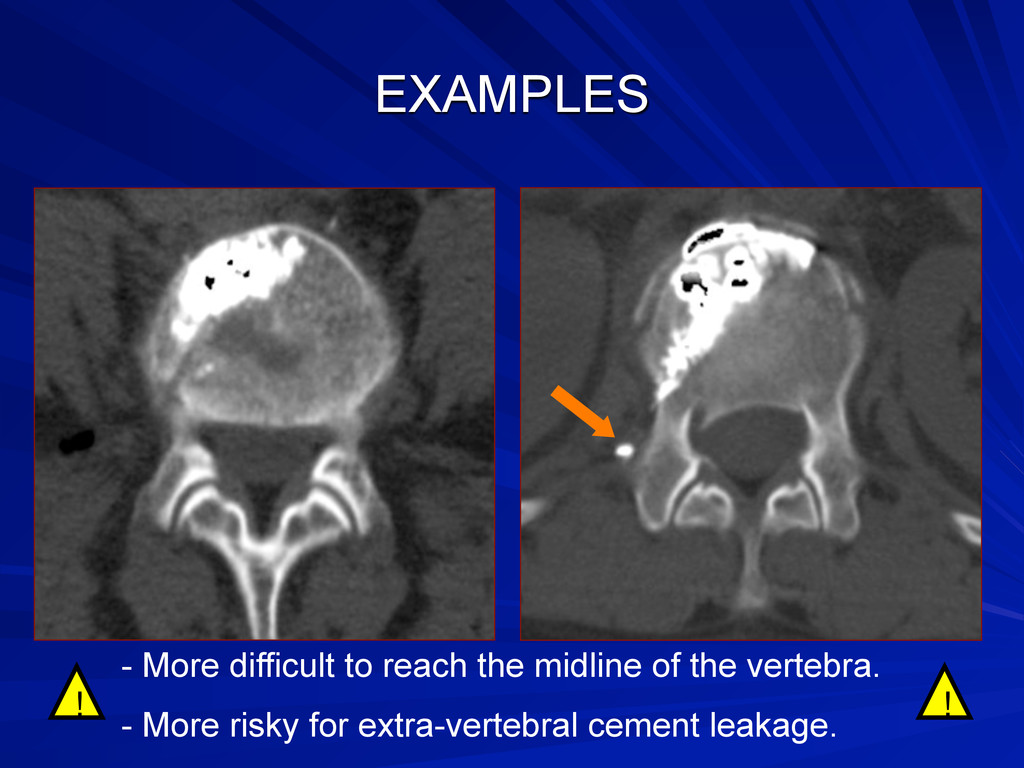
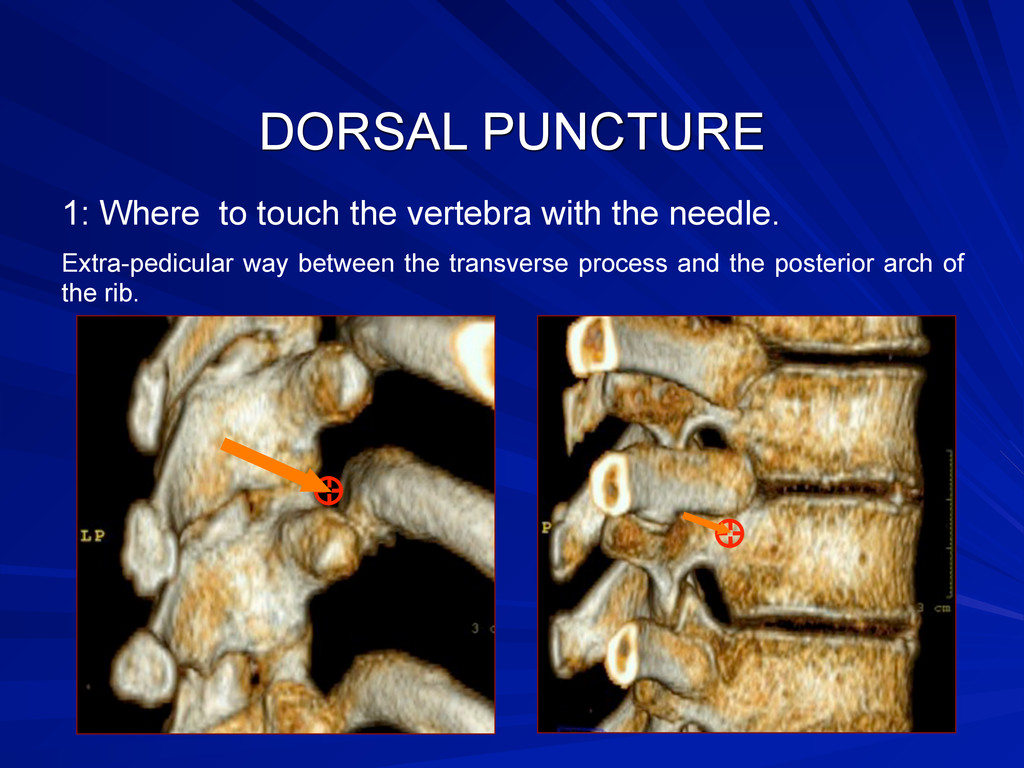
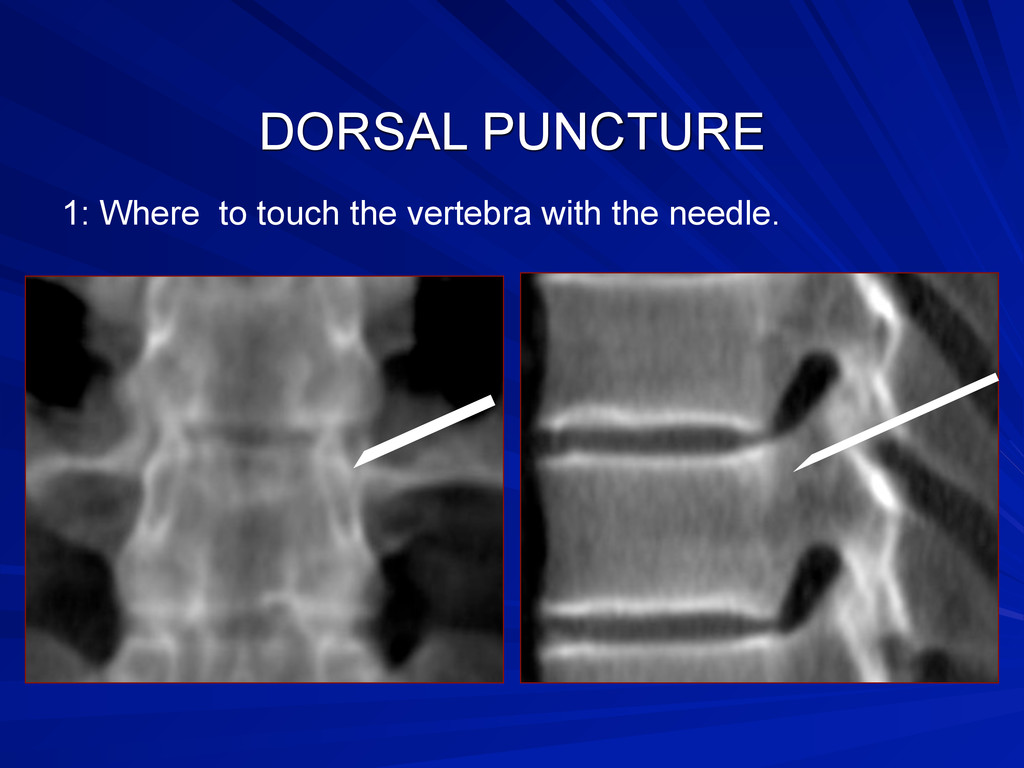
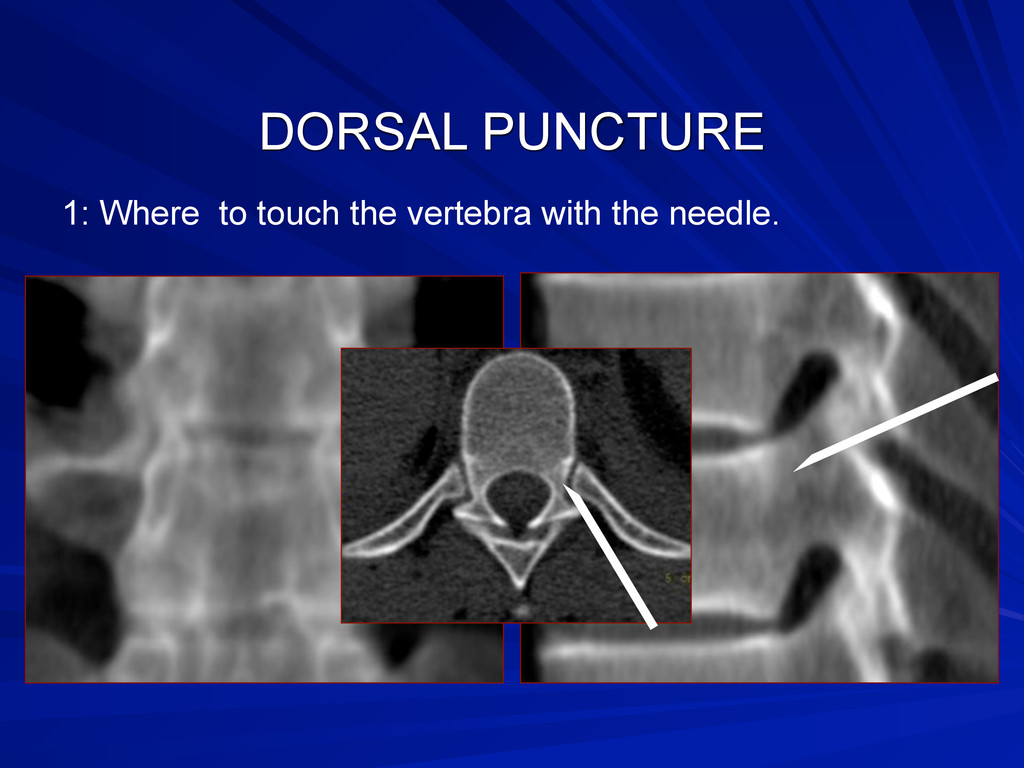
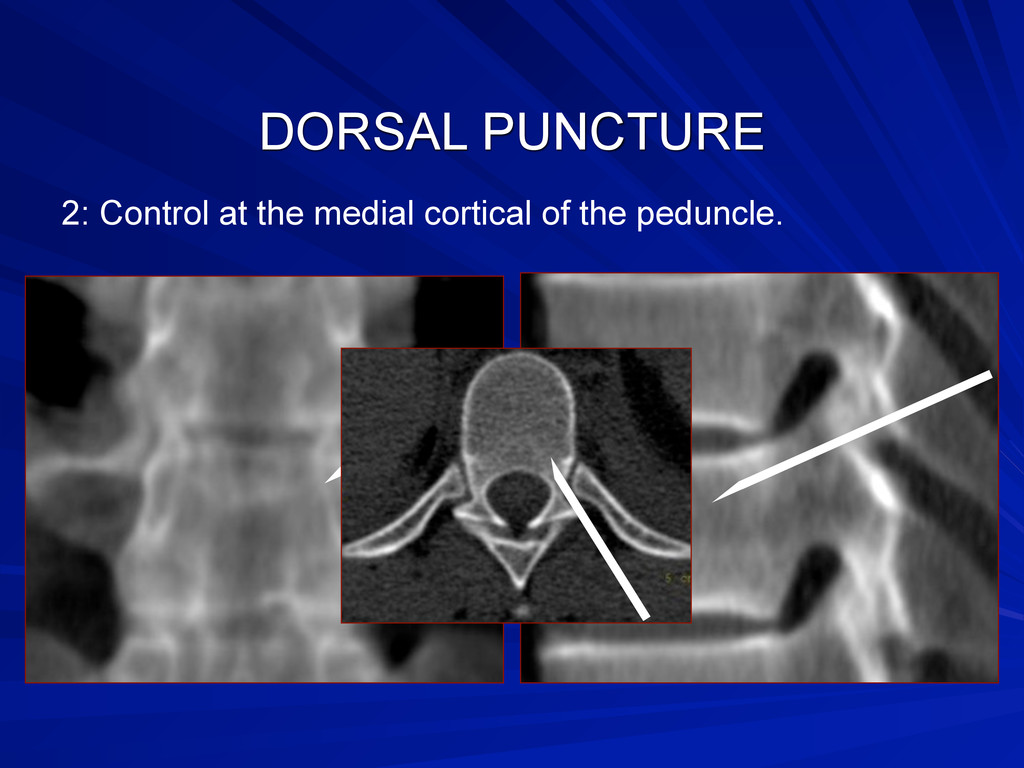
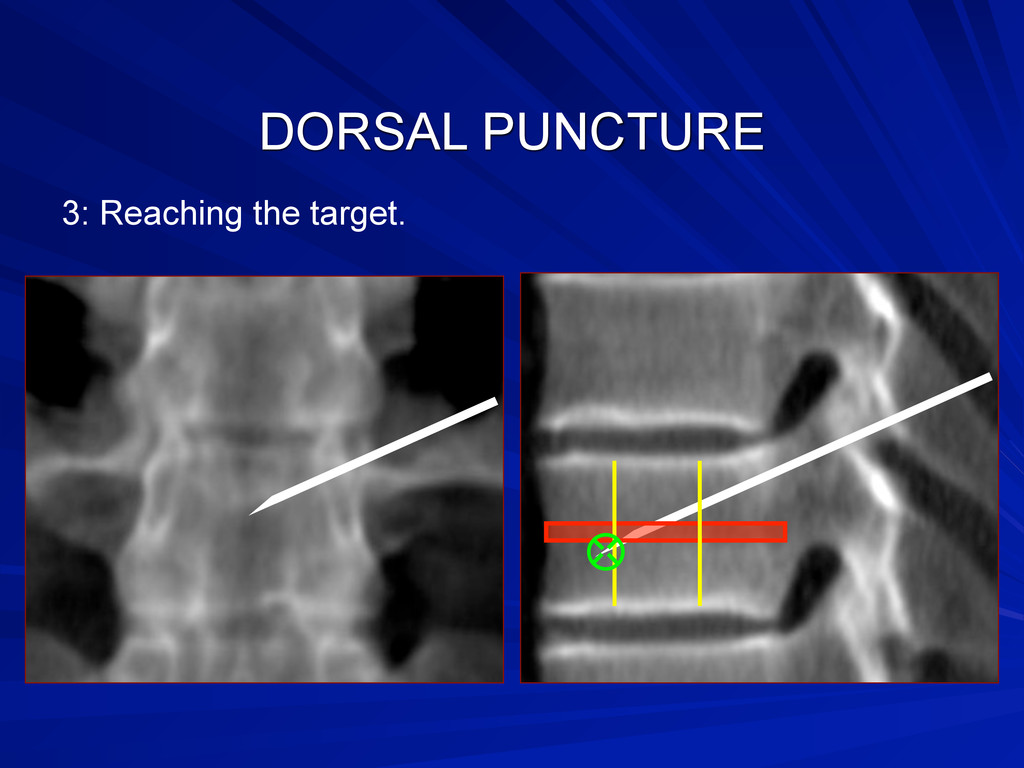
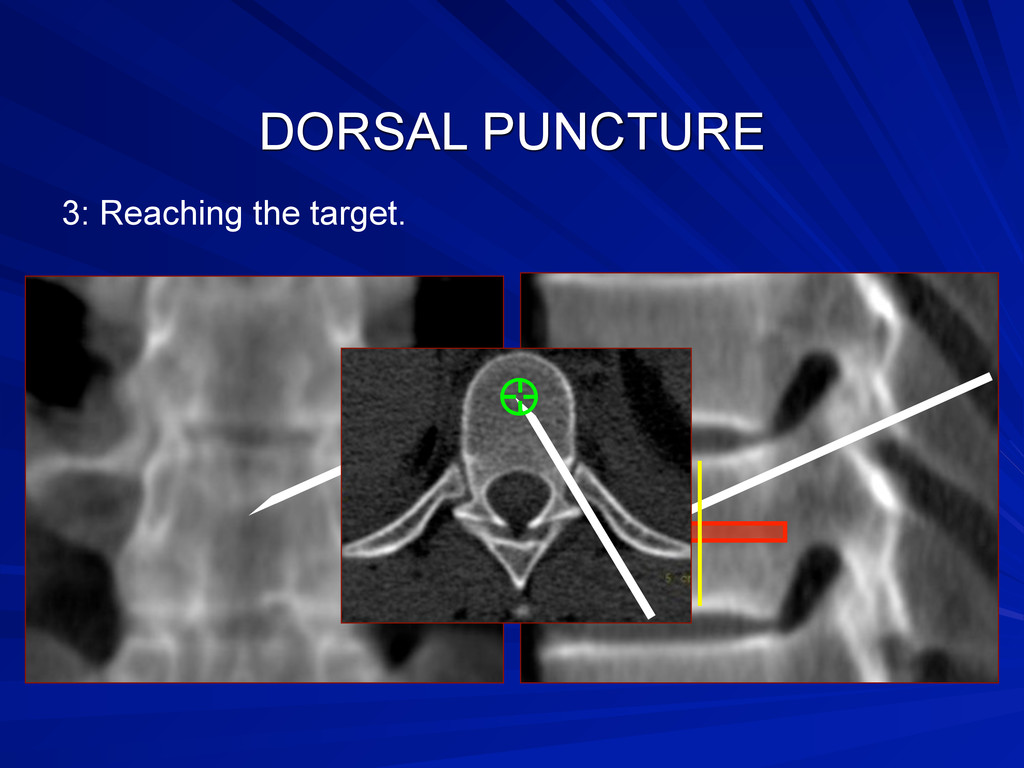
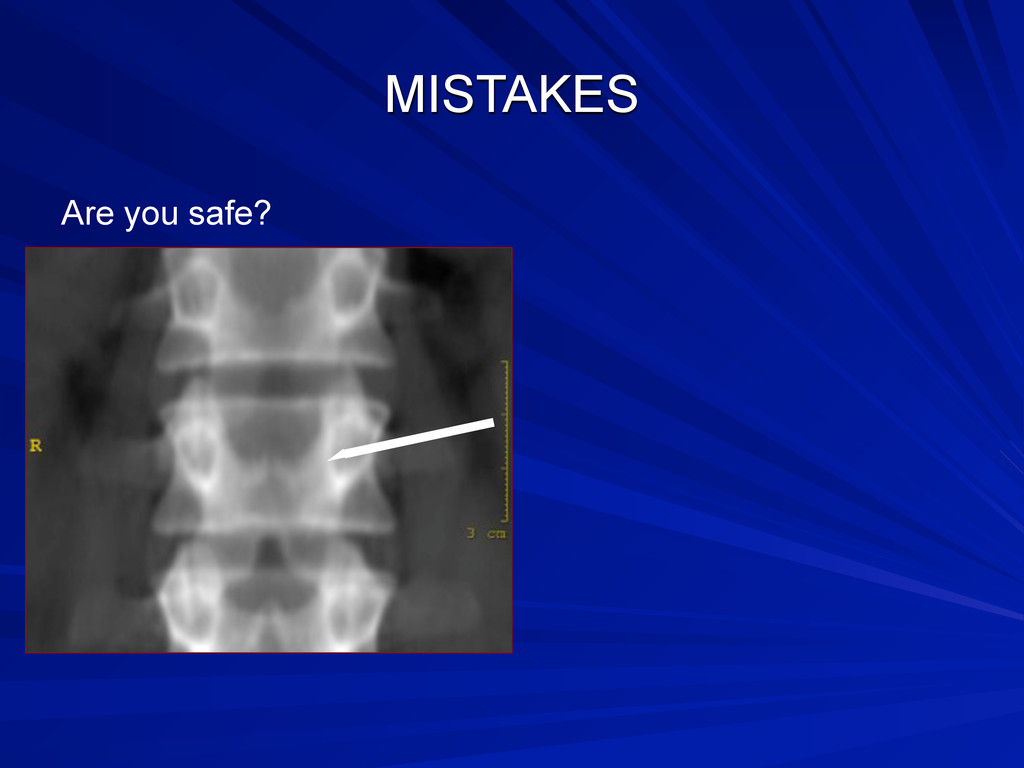
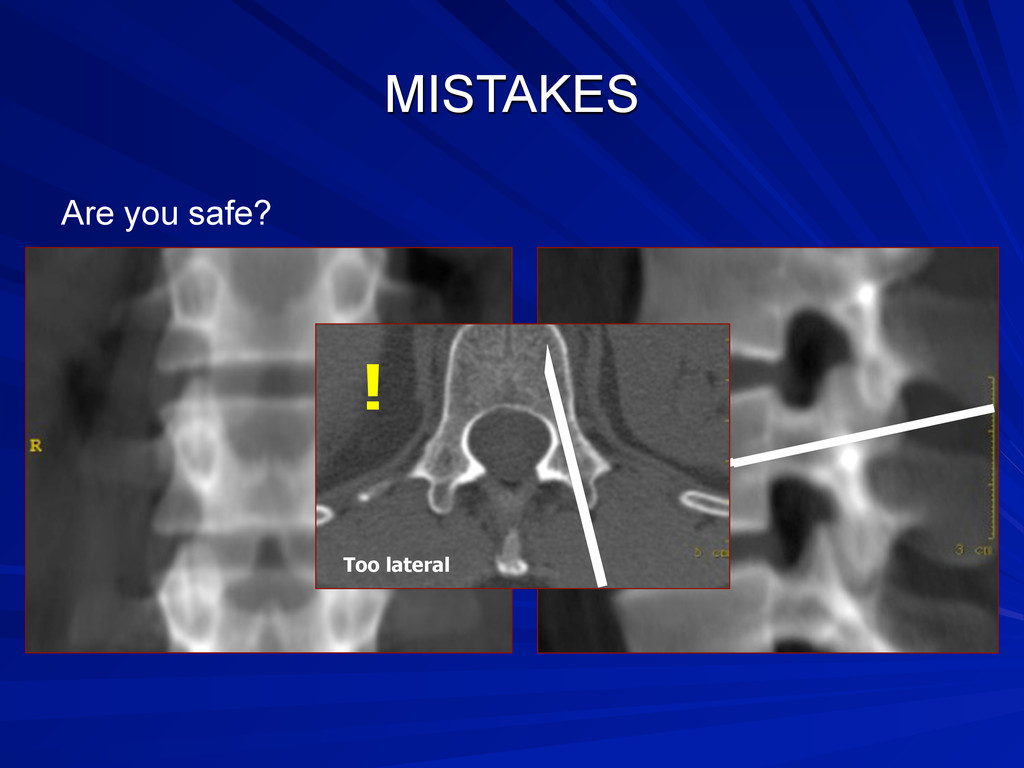
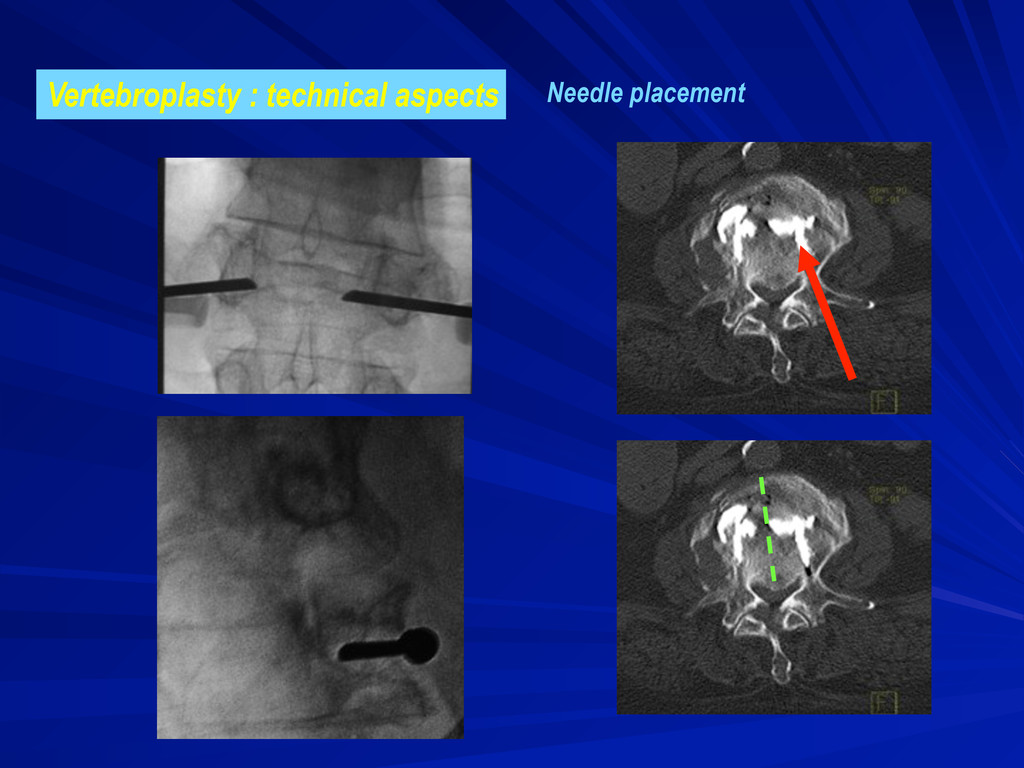
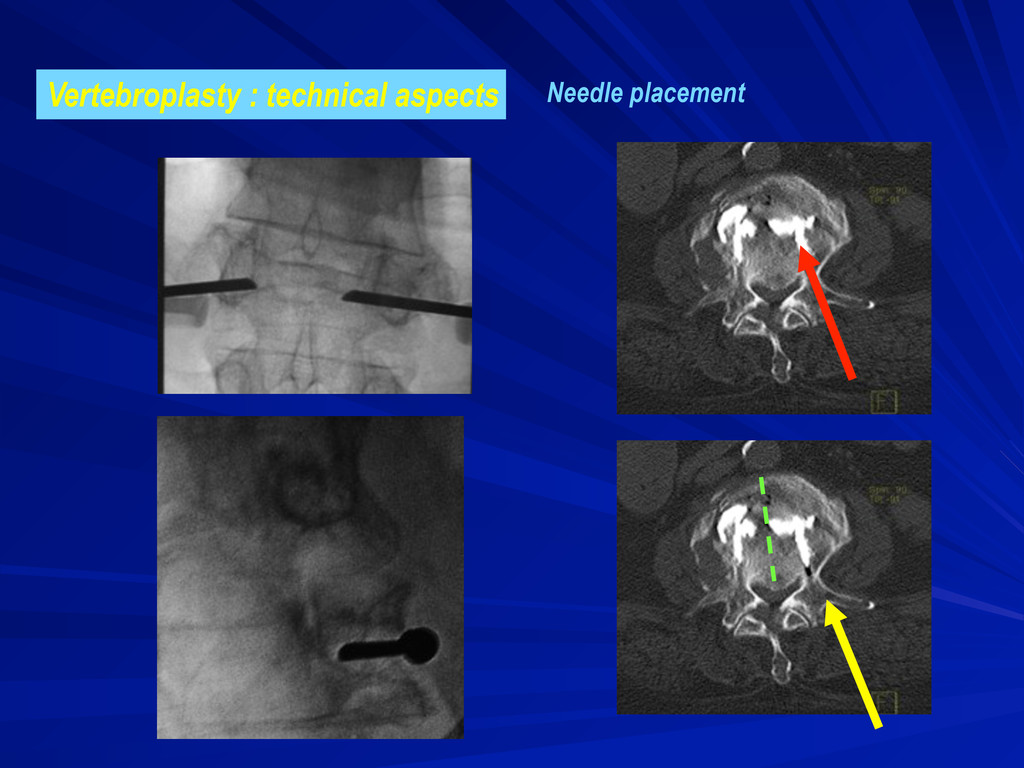
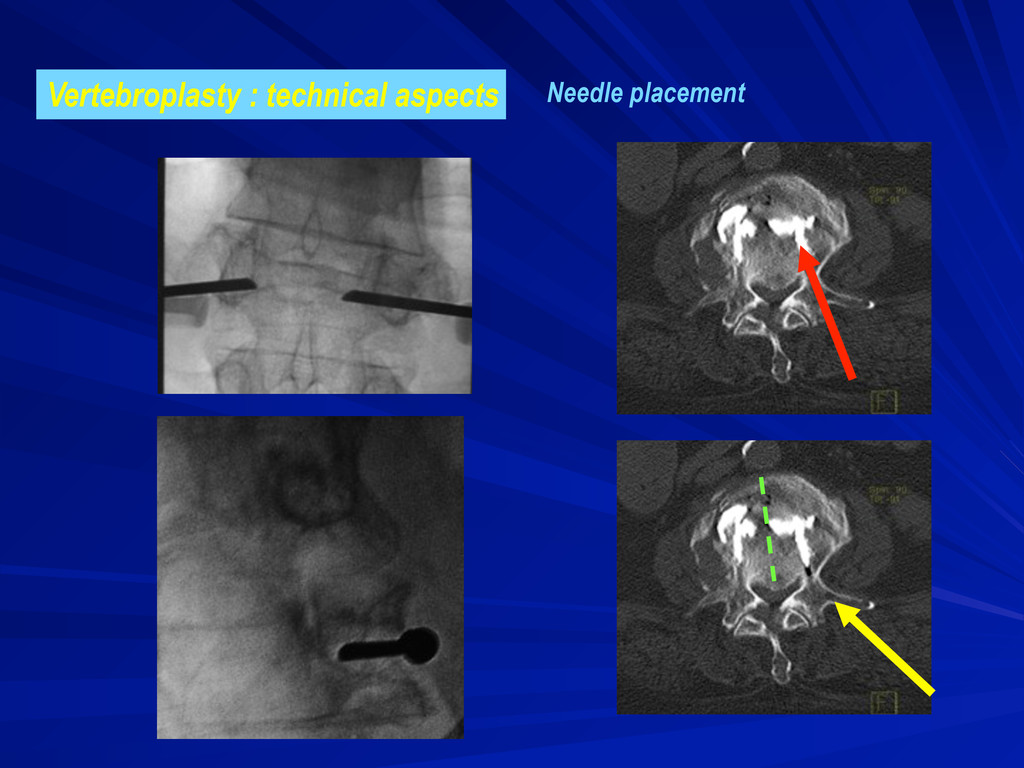
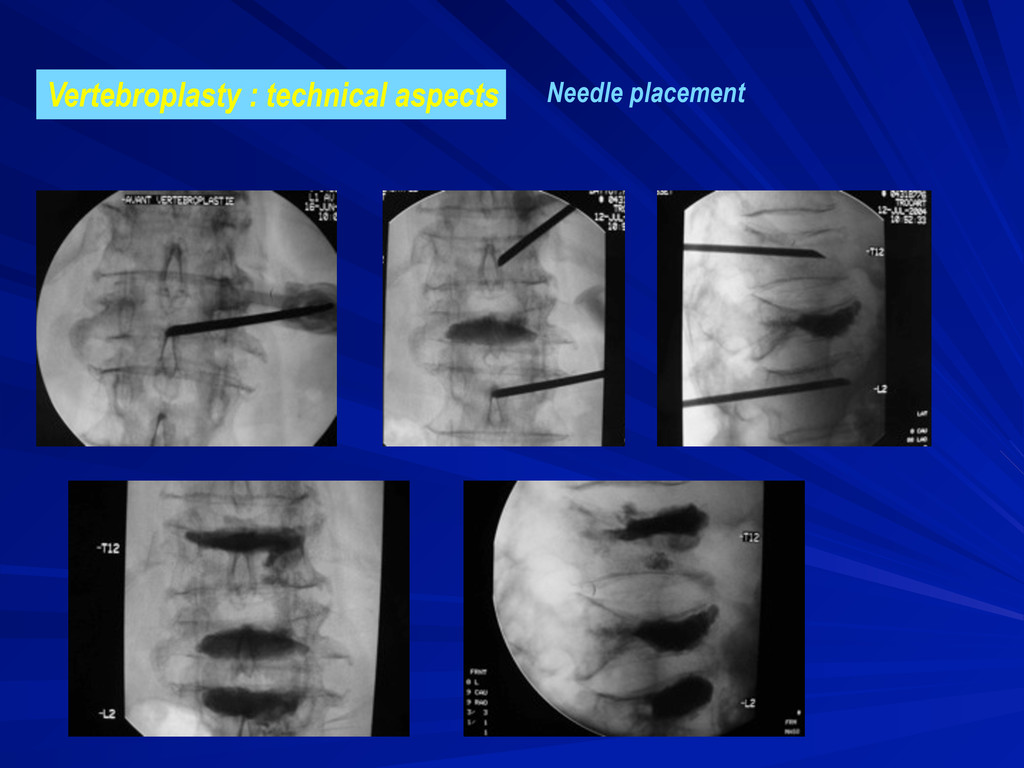
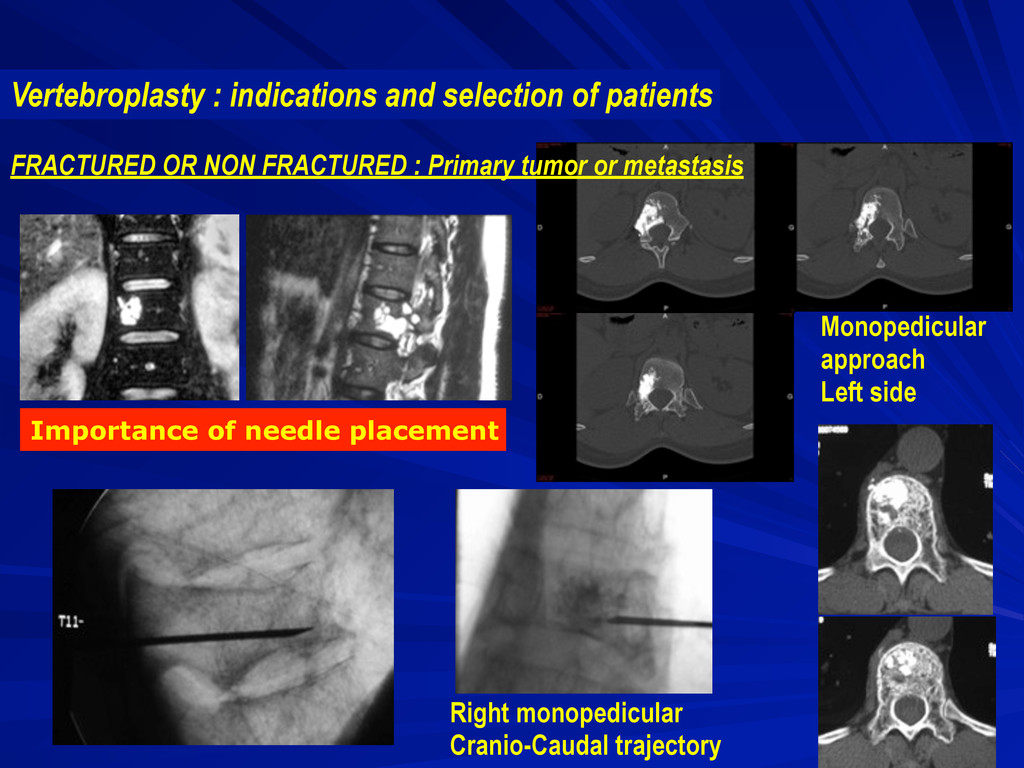
global vertebral body pathology (i.e. traumatic or osteoporotic fracture, or large invasive lesion). « Standard » needle positioning allows full vertebral body filling using classical and safer approach. - specific: in case of focal vertebral lesion. The route of the needle will be planned to reach (tumoral lesion) or to avoid (intraspongious discal herniation) a specific area of the vertebra.
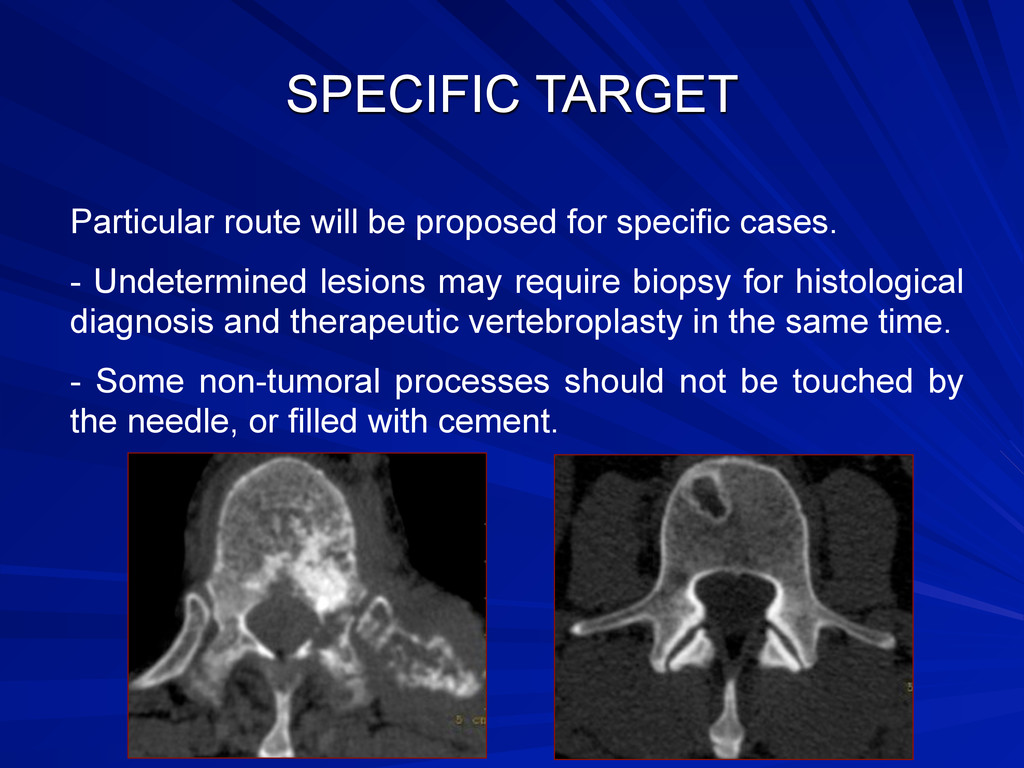
- Undetermined lesions may require biopsy for histological diagnosis and therapeutic vertebroplasty in the same time. - Some non-tumoral processes should not be touched by the needle, or filled with cement.
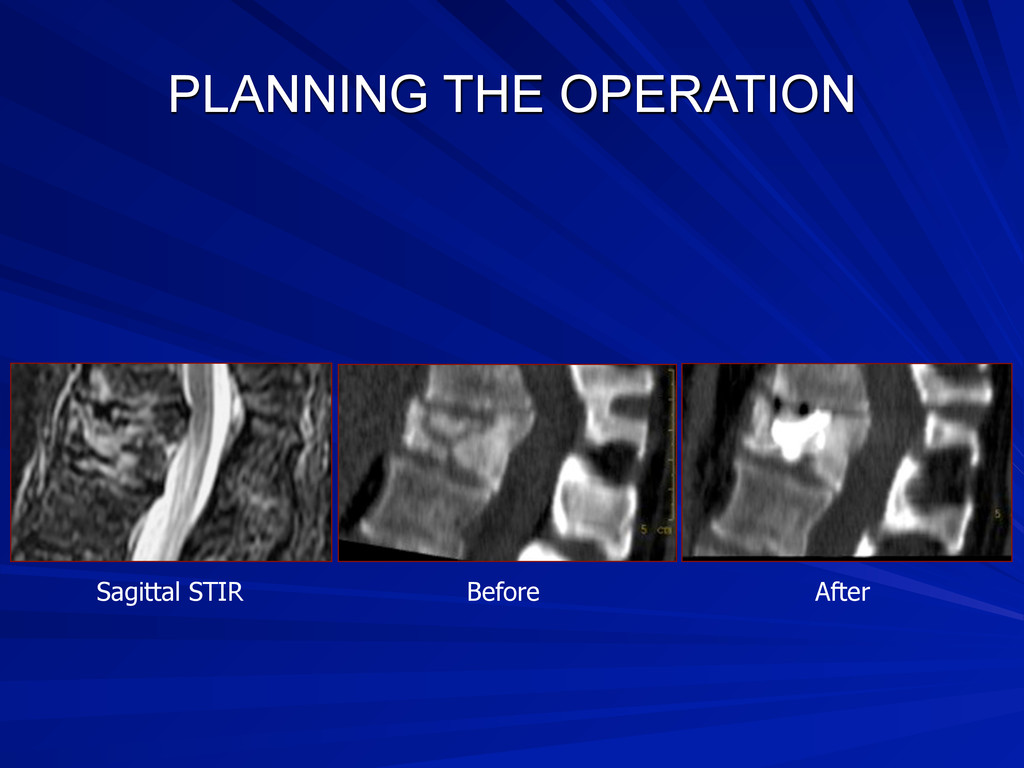
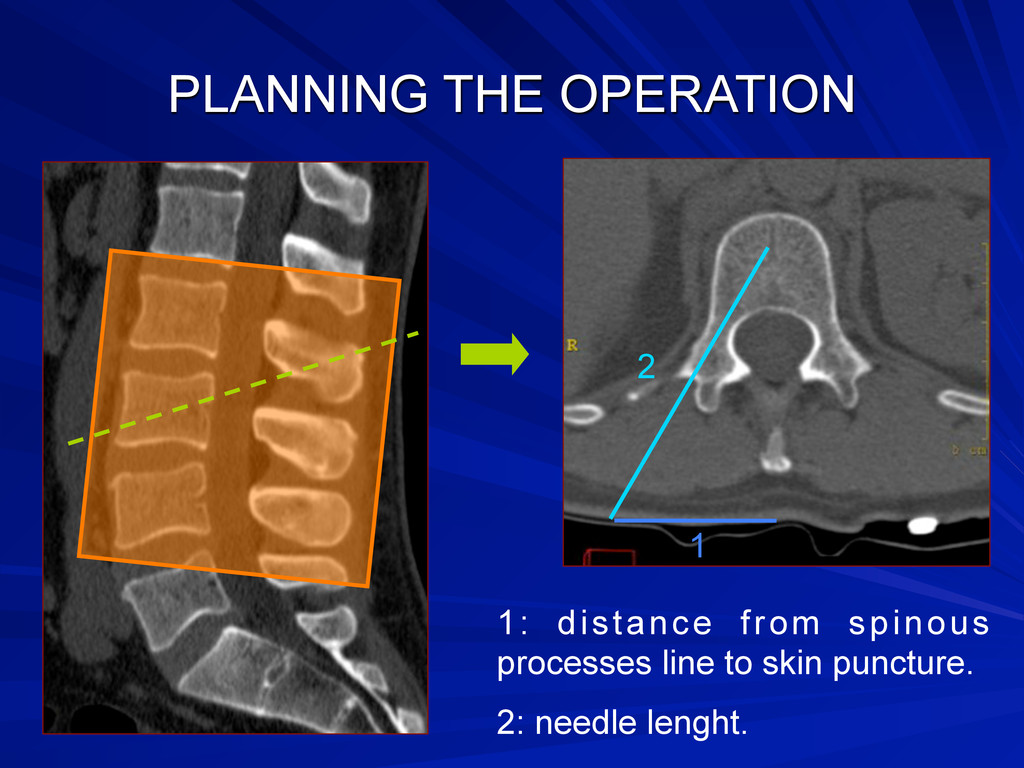
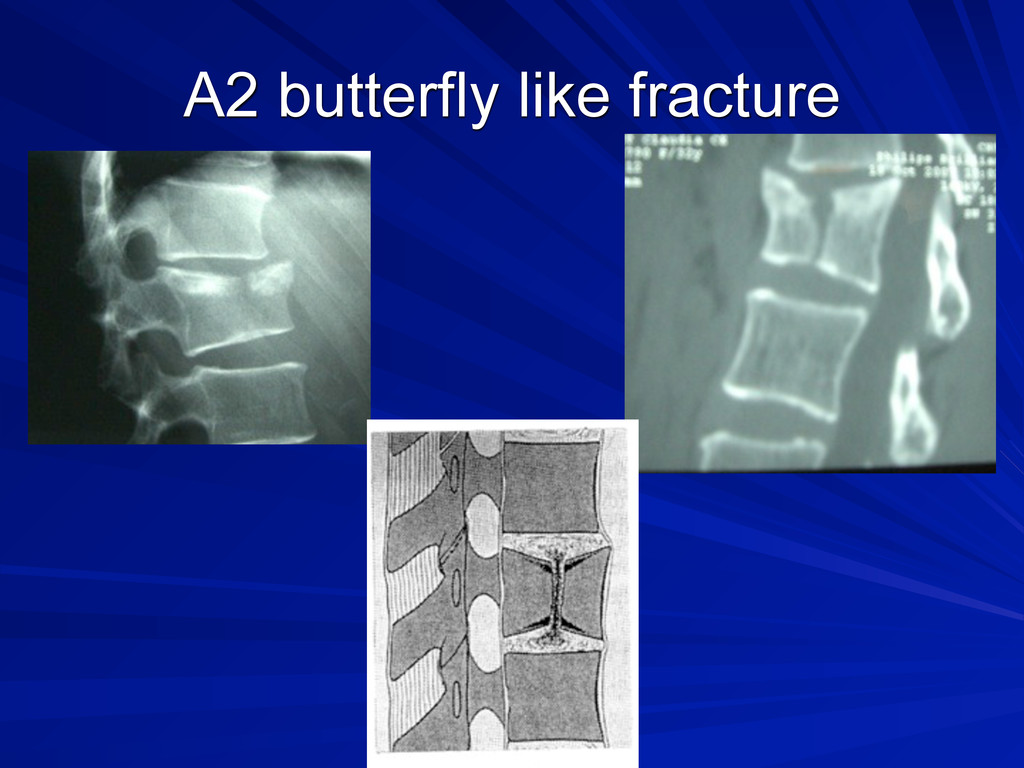
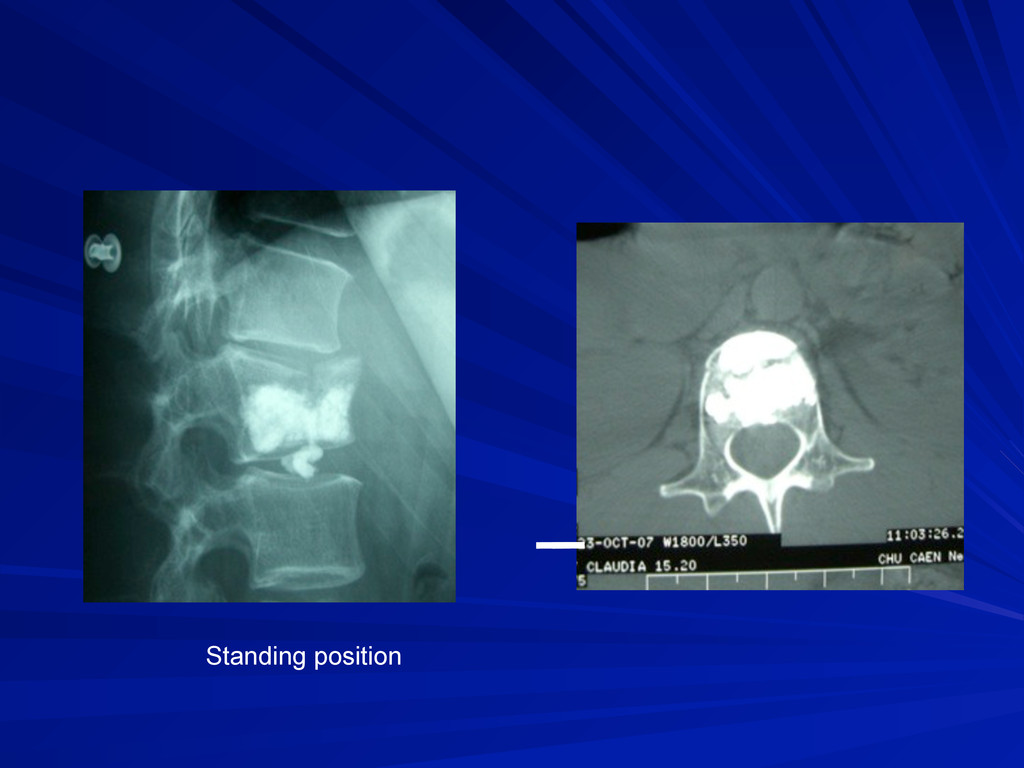
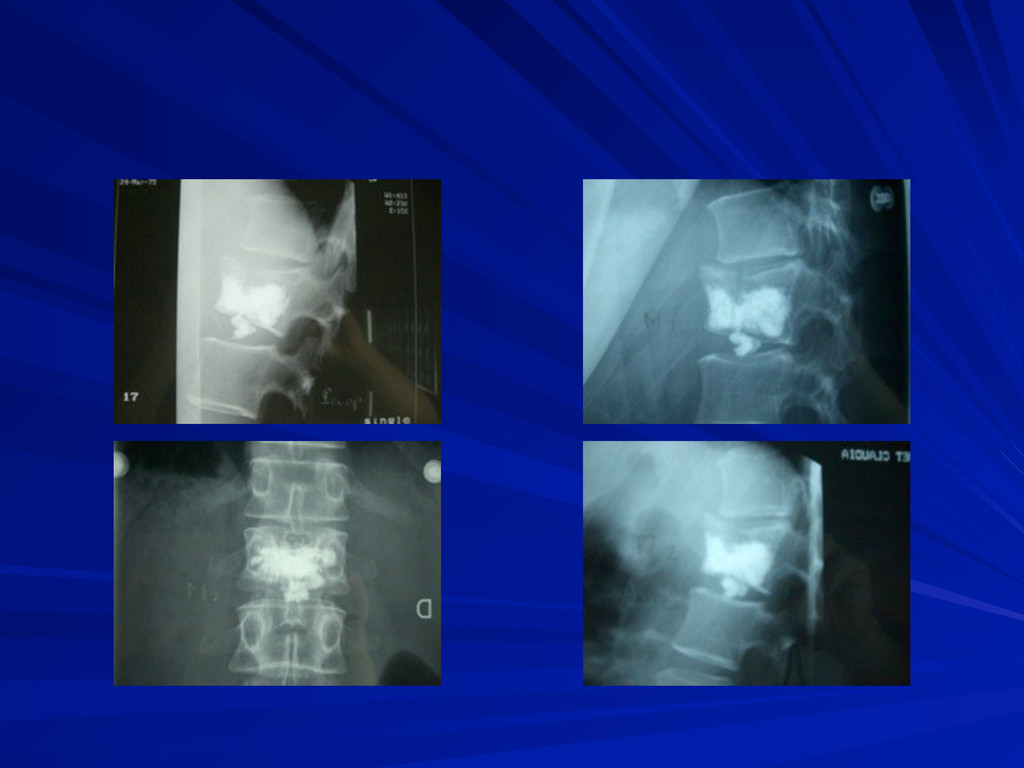
spine, including the two adjacent vertebraes (superior and inferior). - Performed the day before the operation. - Allows: - estimation of kyphosis deformation. - complex fracture visualisation. - distances measurement for percutaneous approach.
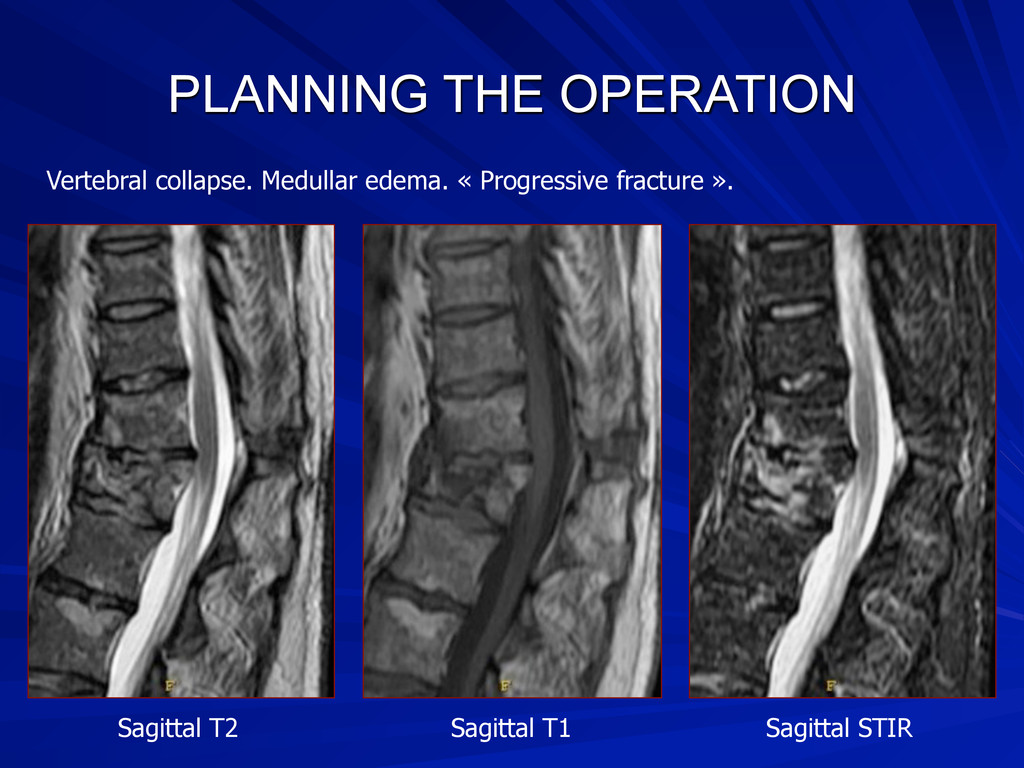
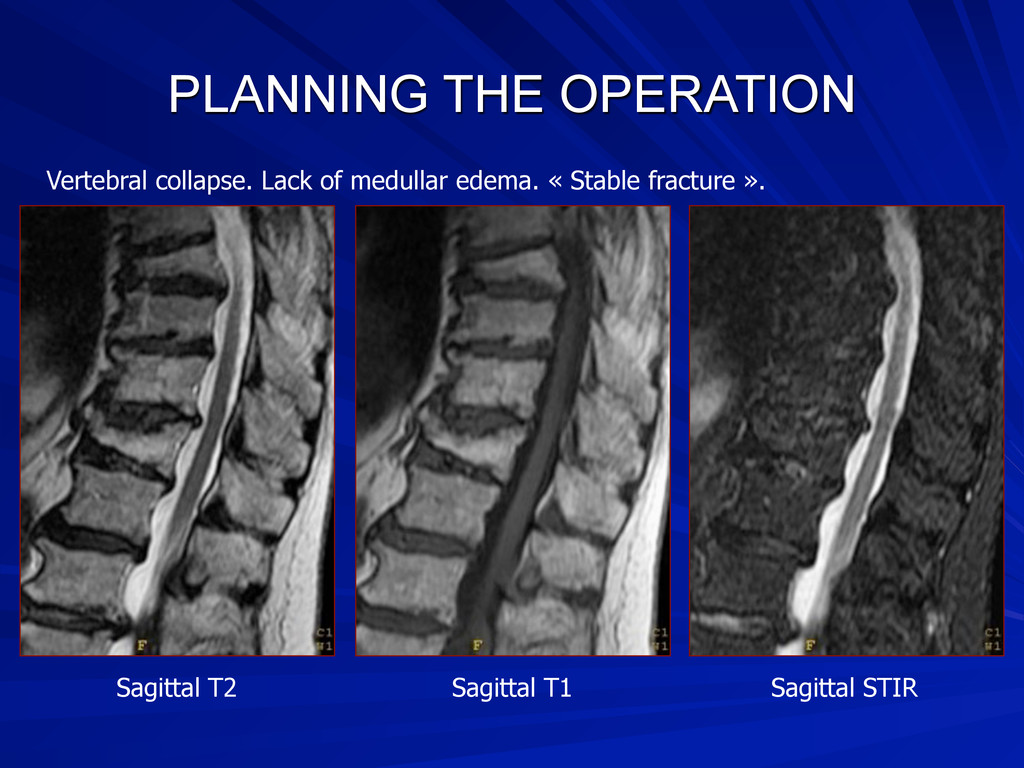
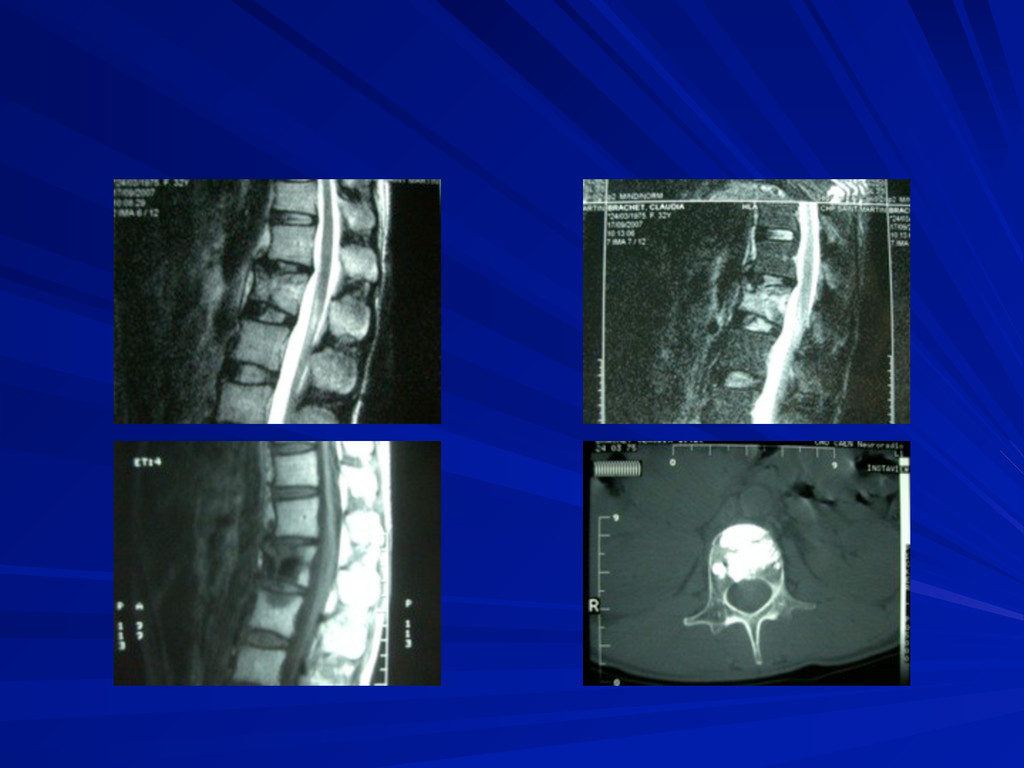
spine. Protocol: sagittal T1, T2, T2 with fat suppression and T1 after IV gadolinium. axial T2 and T1 after IV gadolinium. - Performed during the two weeks before the operation. - Allows: - expecting spine bone marrow oedema. - tumoral extension, possible epiduritis. - spinal cord integrity.
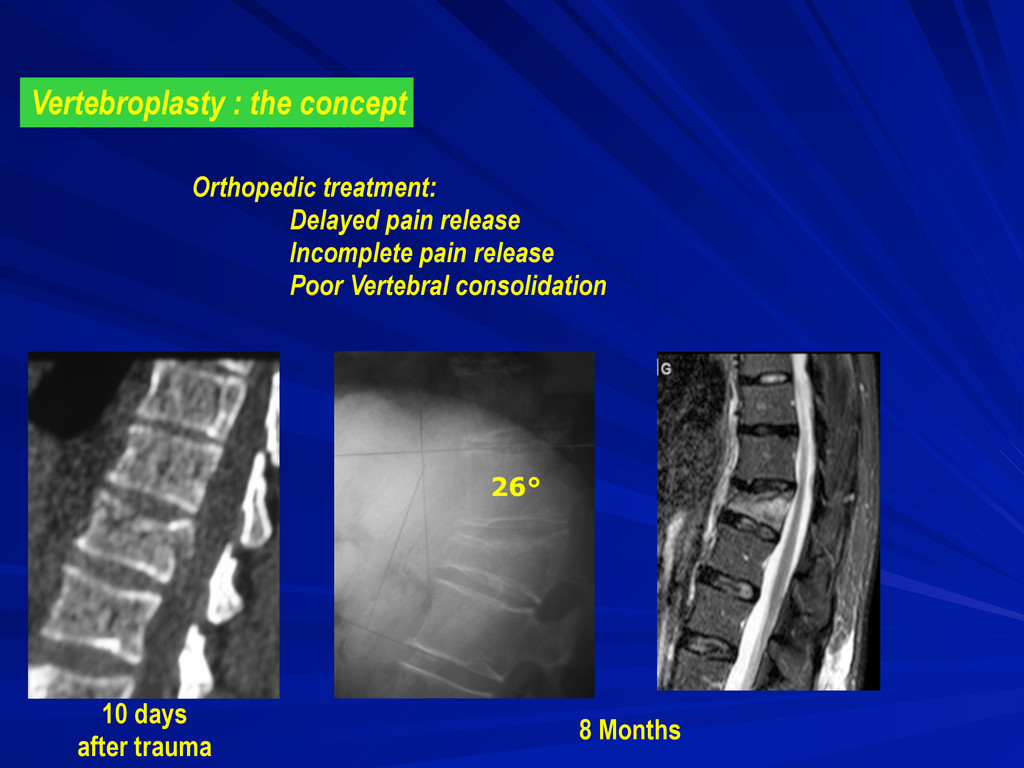
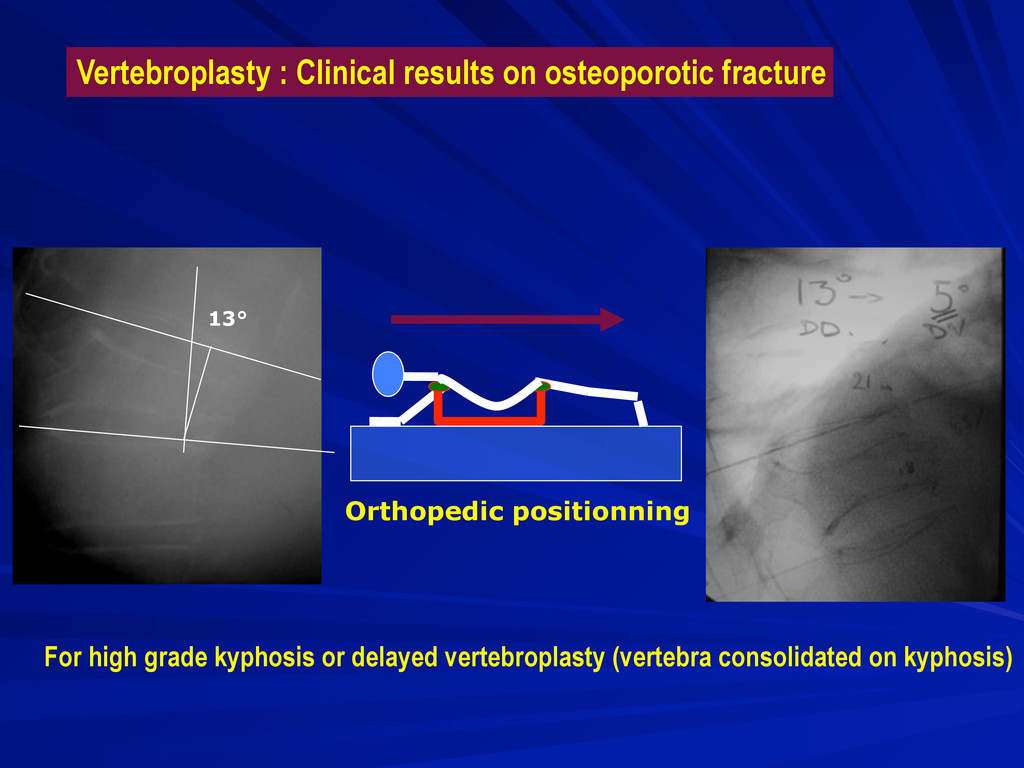
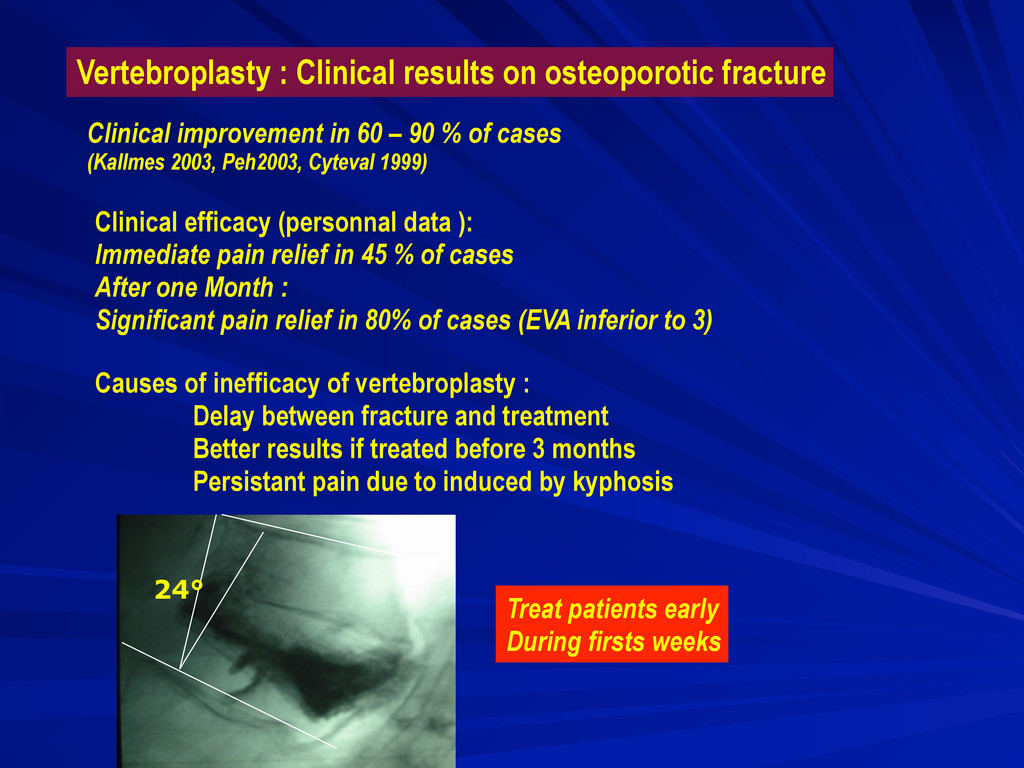
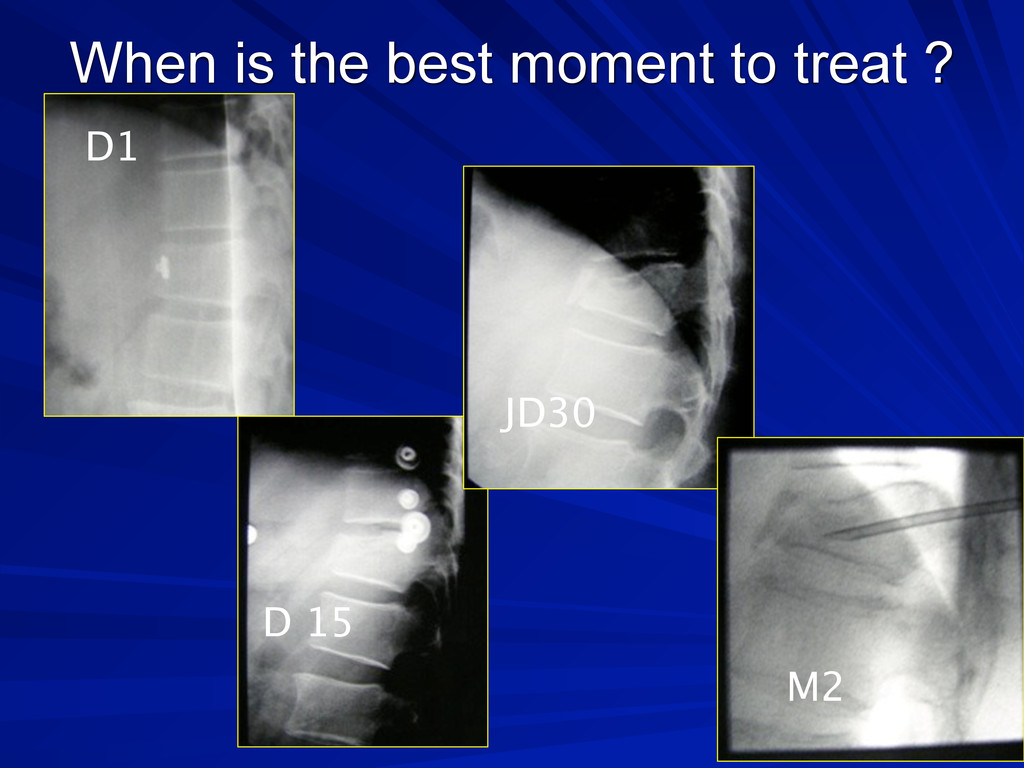
data ): Immediate pain relief in 45 % of cases After one Month : Significant pain relief in 80% of cases (EVA inferior to 3) Causes of inefficacy of vertebroplasty : Delay between fracture and treatment Better results if treated before 3 months Persistant pain due to induced by kyphosis 24° Treat patients early During firsts weeks Clinical improvement in 60 – 90 % of cases (Kallmes 2003, Peh2003, Cyteval 1999)
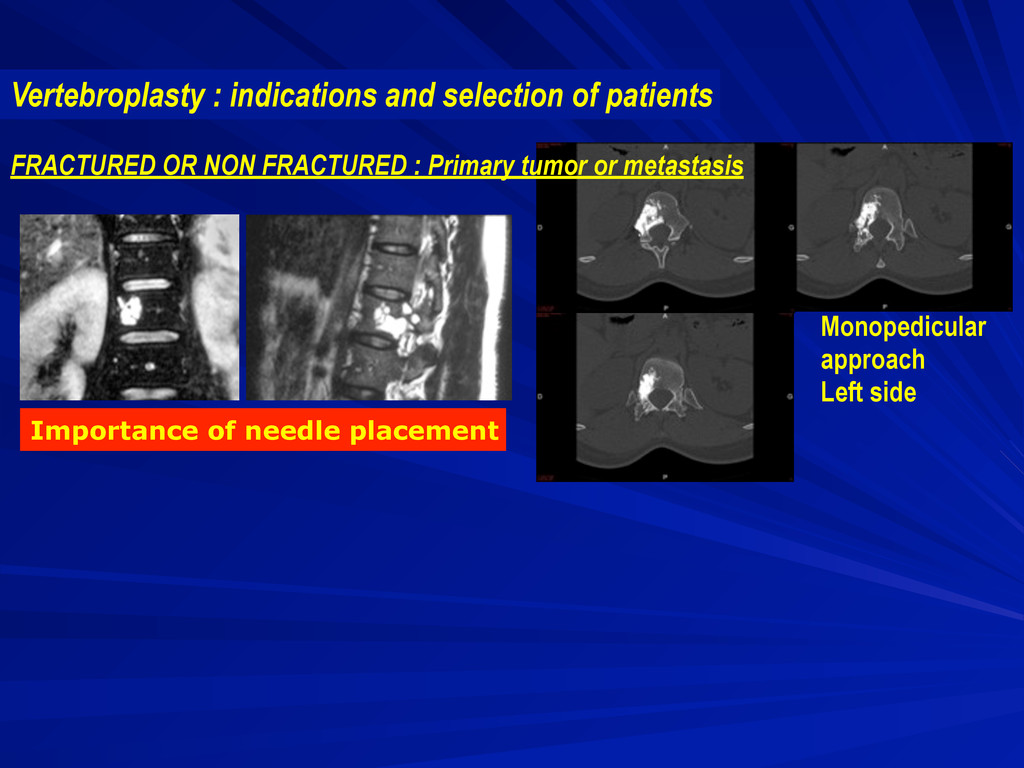
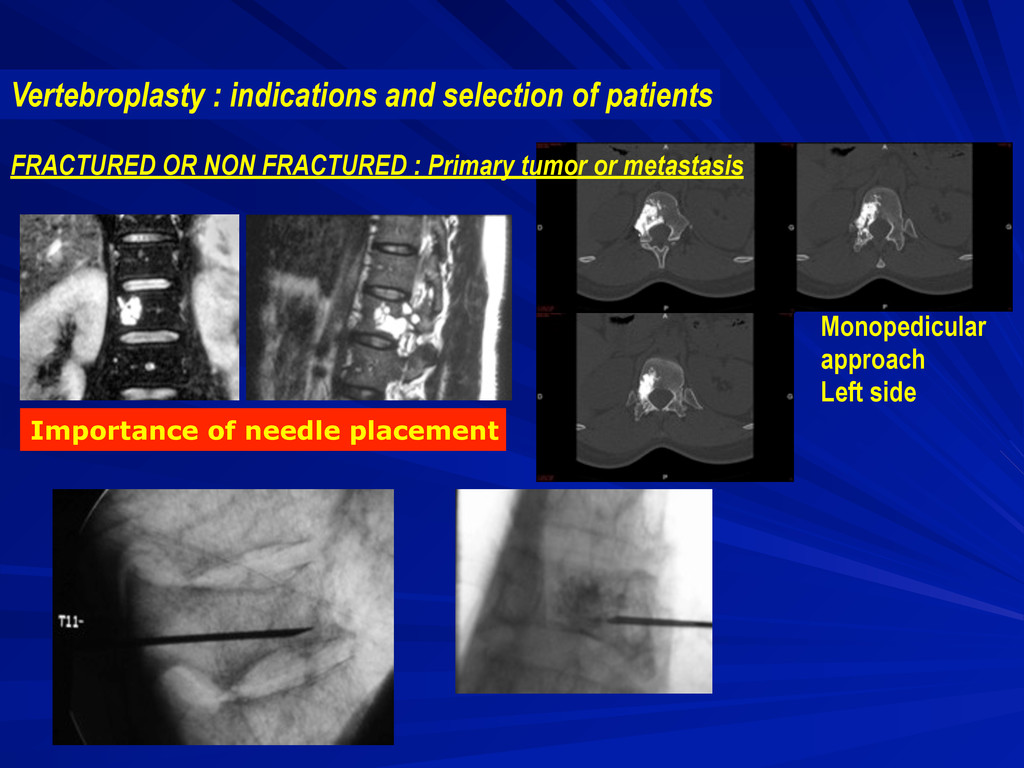
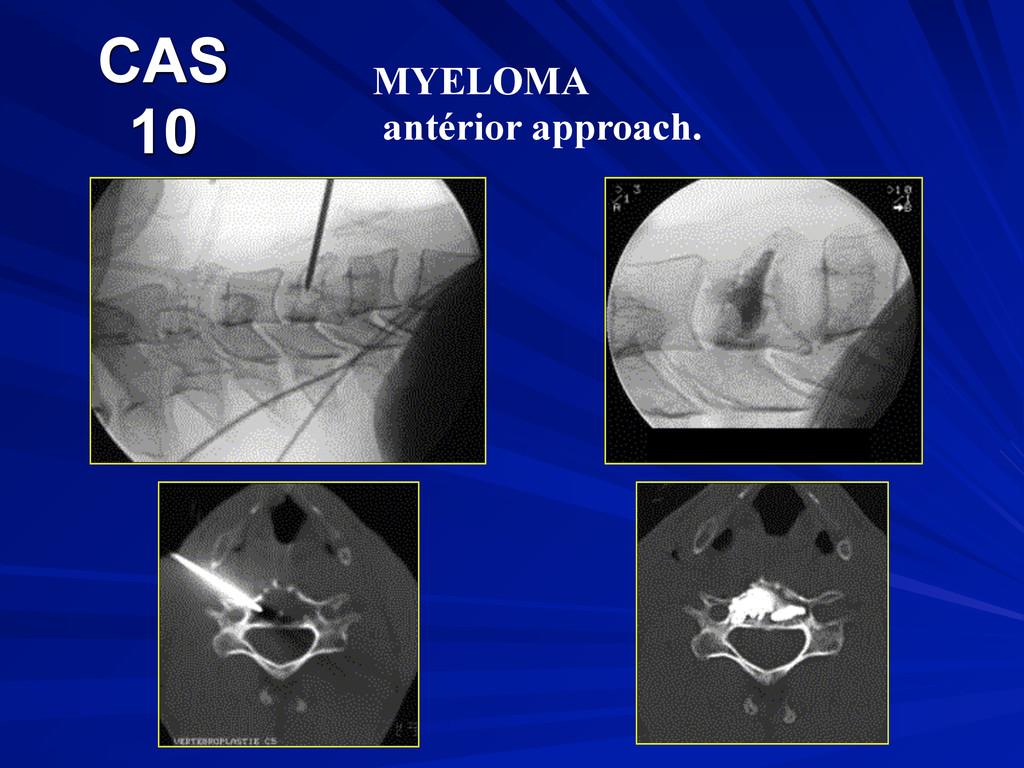
perform biopsy before vertebroplasty Vertebroplasty can be done in the same time Multiple myeloma Breast, lung or kydney cancer Vertebroplasty : indications and selection of patients
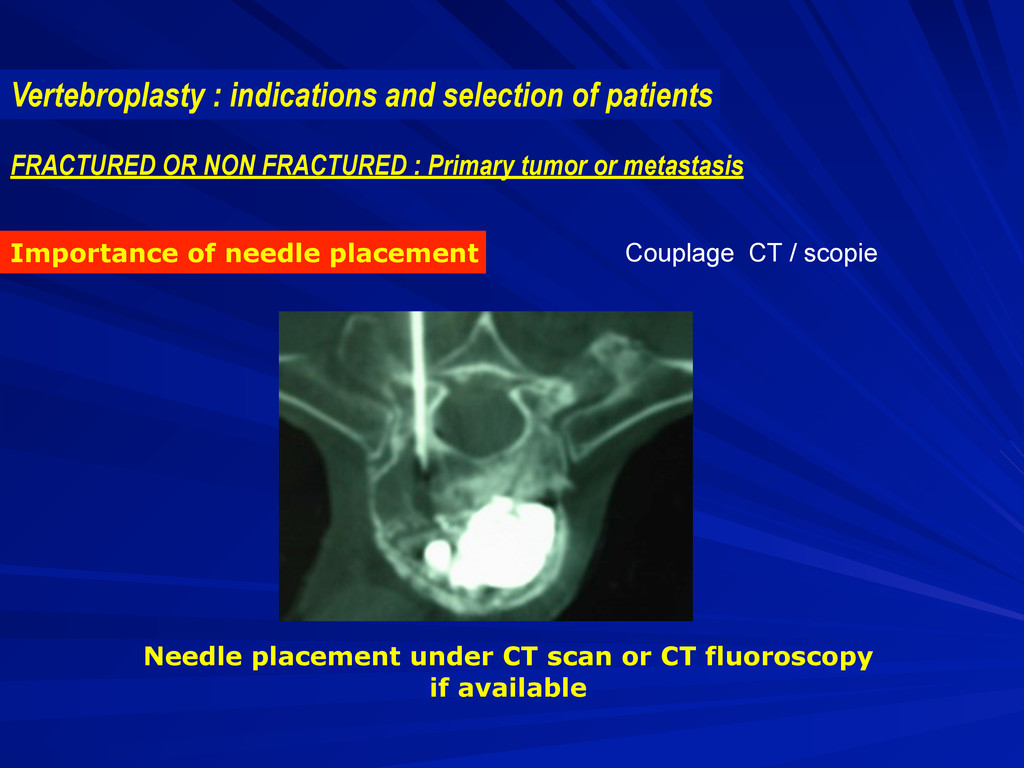
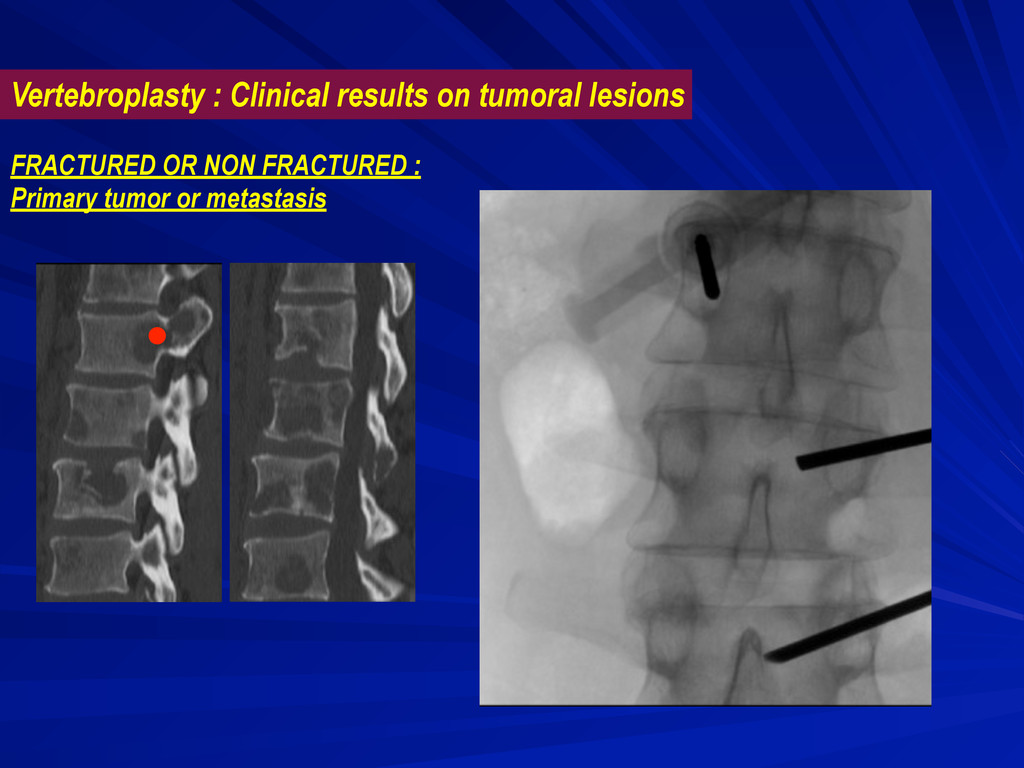
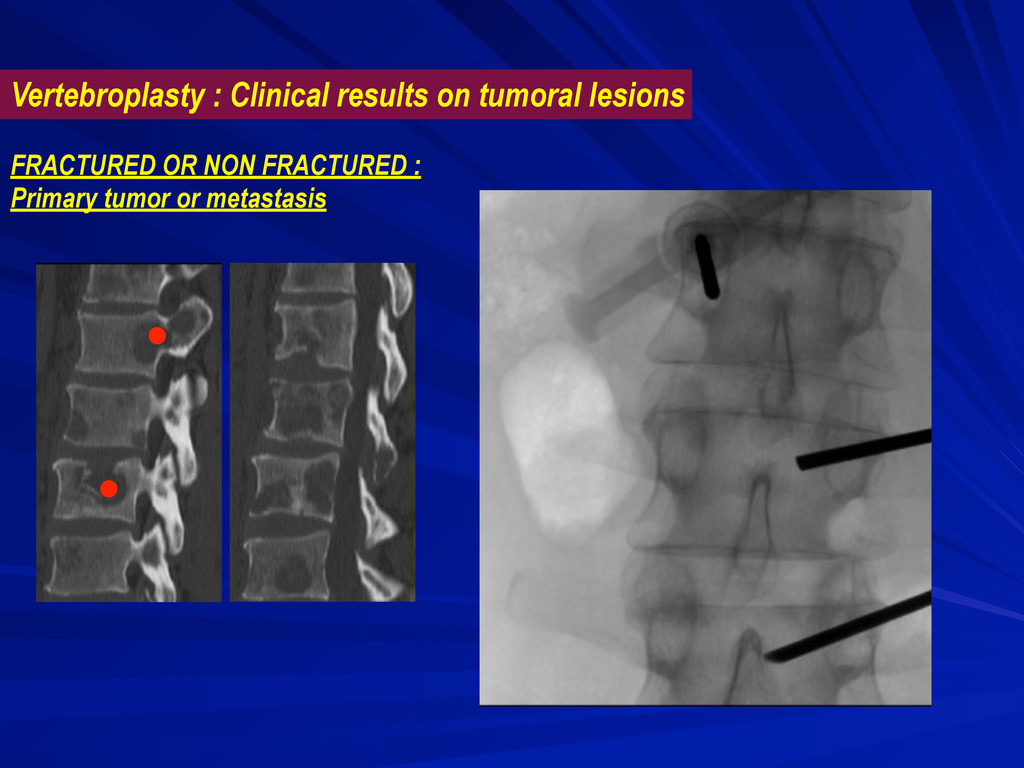
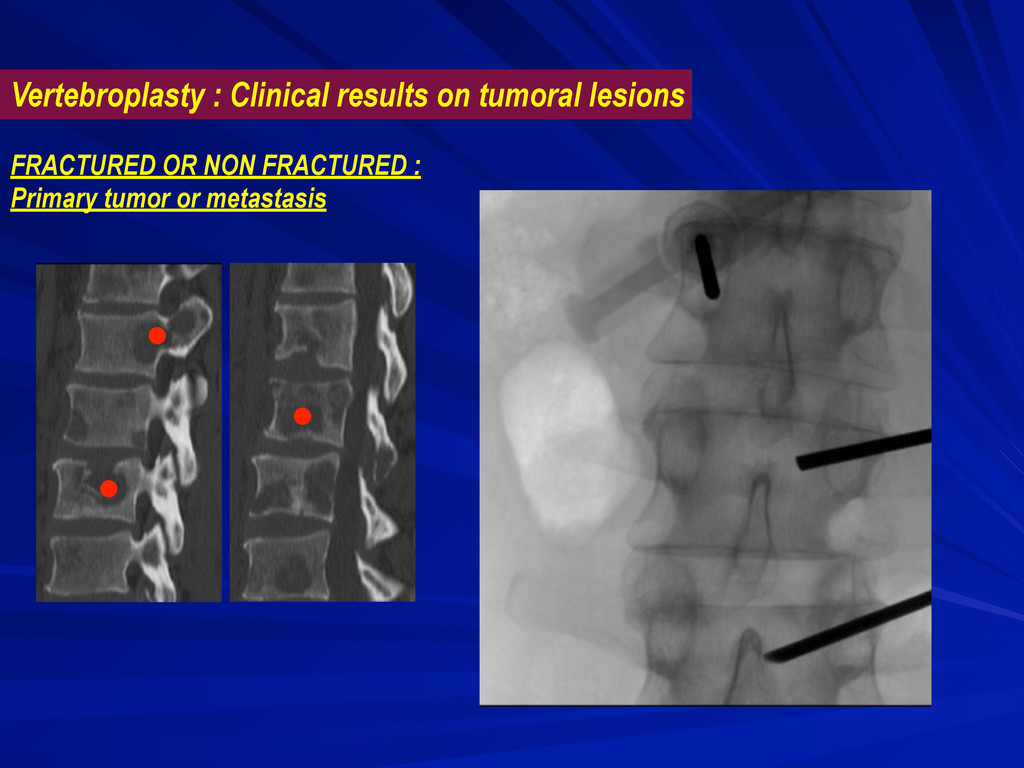
CT fluoroscopy if available FRACTURED OR NON FRACTURED : Primary tumor or metastasis Vertebroplasty : indications and selection of patients Couplage CT / scopie
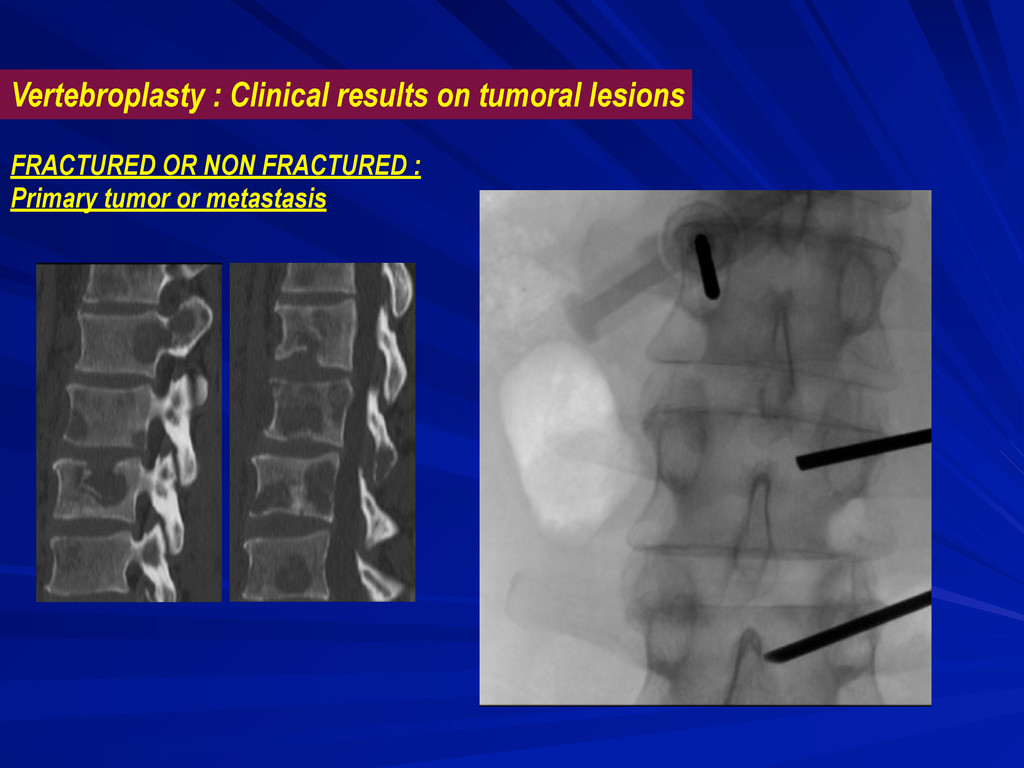
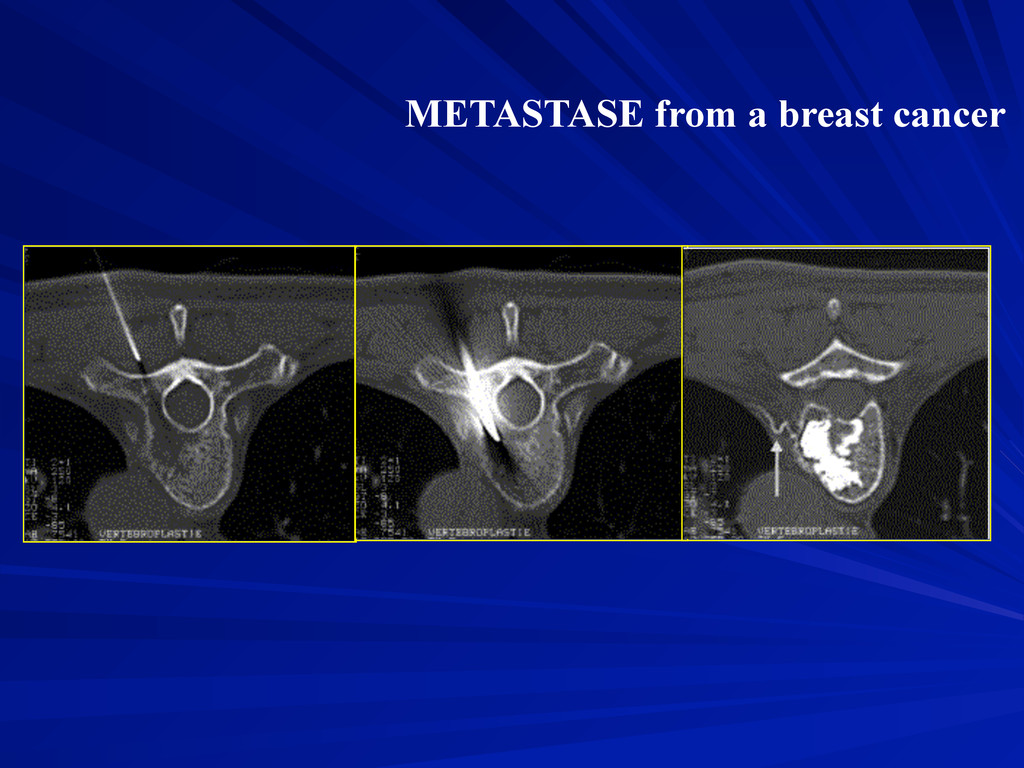
pain and on quality of life 60 to 90 % of significant pain release Weill in Radiology 1996 (241-247) ; Kaemmerlen NEJM 1989 (121-128) FRACTURED OR NON FRACTURED : Primary tumor or metastasis Significant increasing of Karnoffsky index Significant decrease in analgesics and morphinic demand
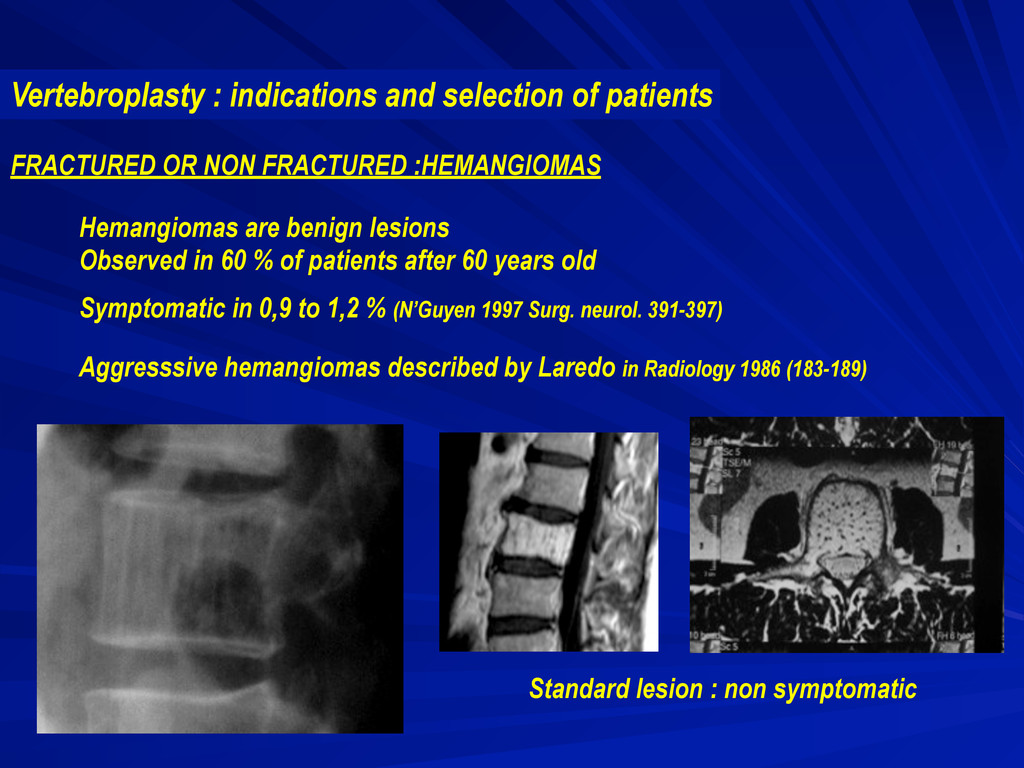
after 60 years old Symptomatic in 0,9 to 1,2 % (N’Guyen 1997 Surg. neurol. 391-397) Aggresssive hemangiomas described by Laredo in Radiology 1986 (183-189) FRACTURED OR NON FRACTURED :HEMANGIOMAS Vertebroplasty : indications and selection of patients Standard lesion : non symptomatic
mean f.u. : 37 months Pain release in 15/16 patients 56% totally asymptomatic at f.u. 31 % slightly symptomatic but no need for chronic use of antalgics 16 symptomatic and 3 preventive vertebroplasty 3 patients treated preventively did not develop symptoms or fractures after treatment Vertebroplasty : Clinical results on aggressive hemangiomas
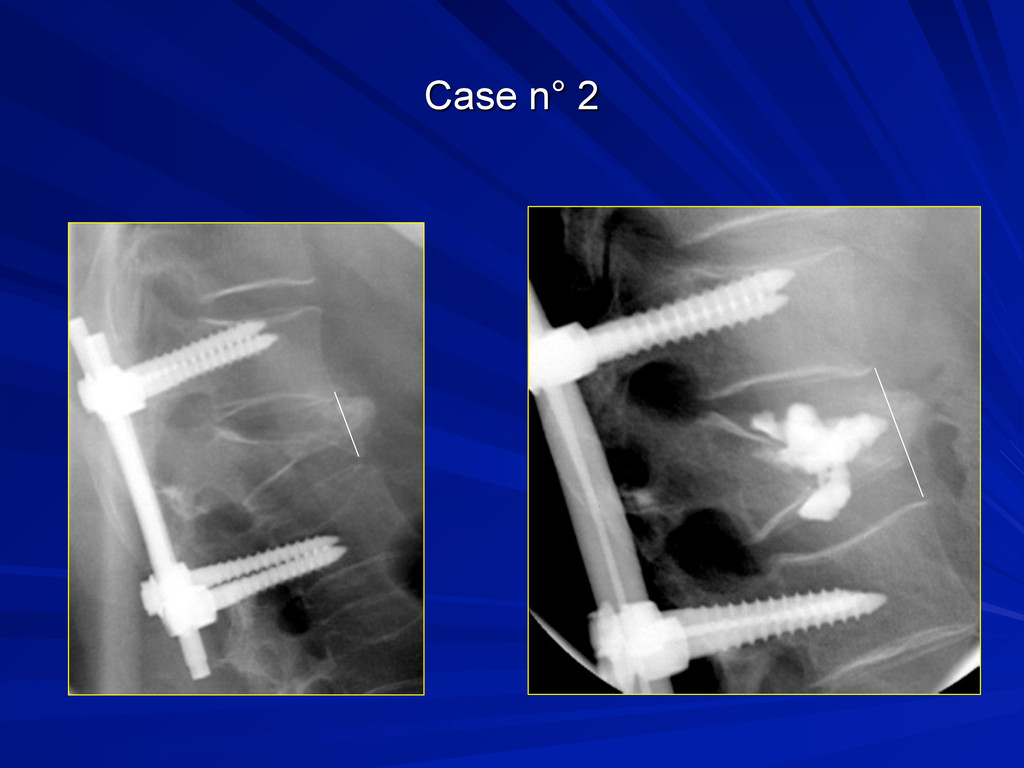
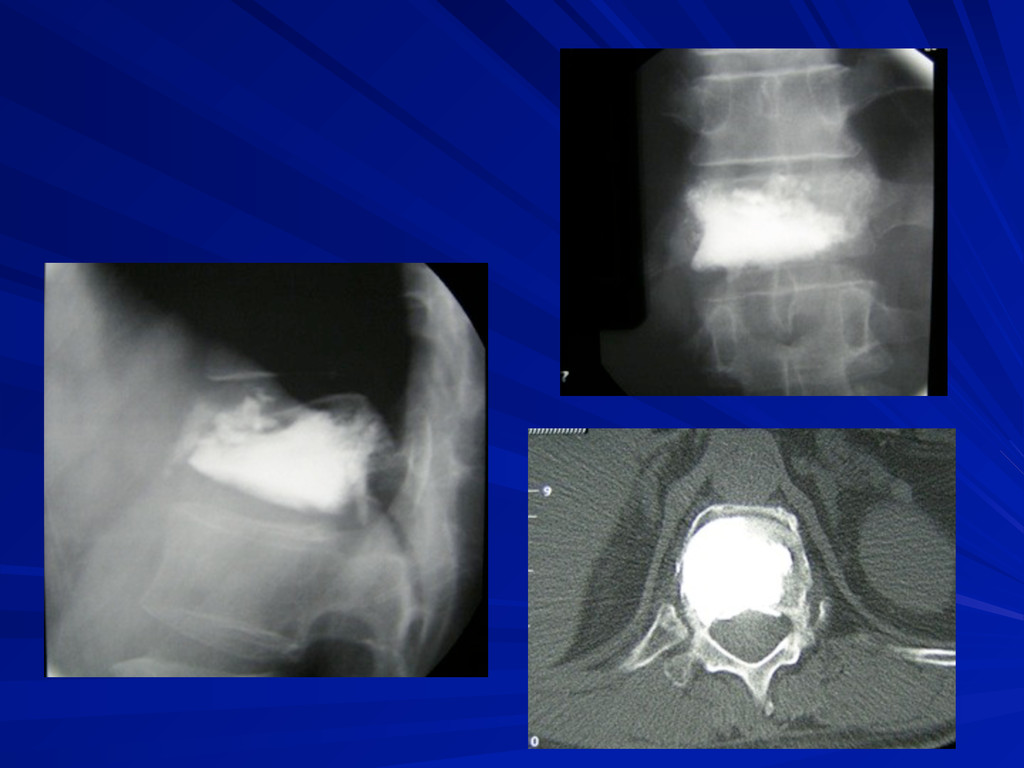
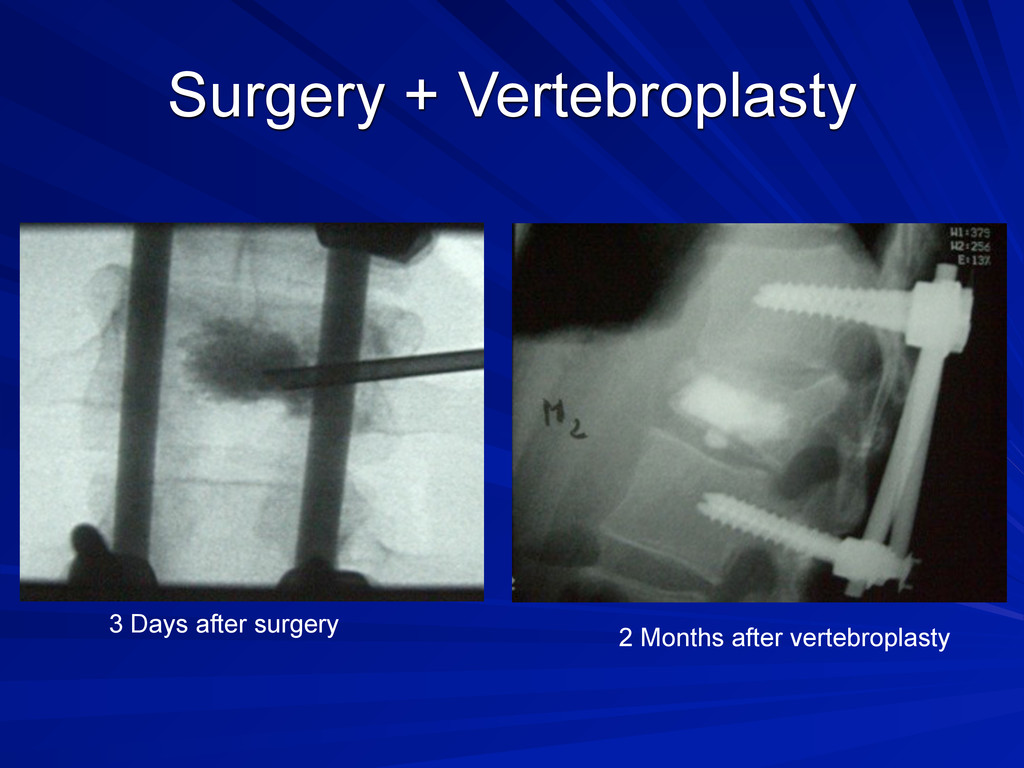
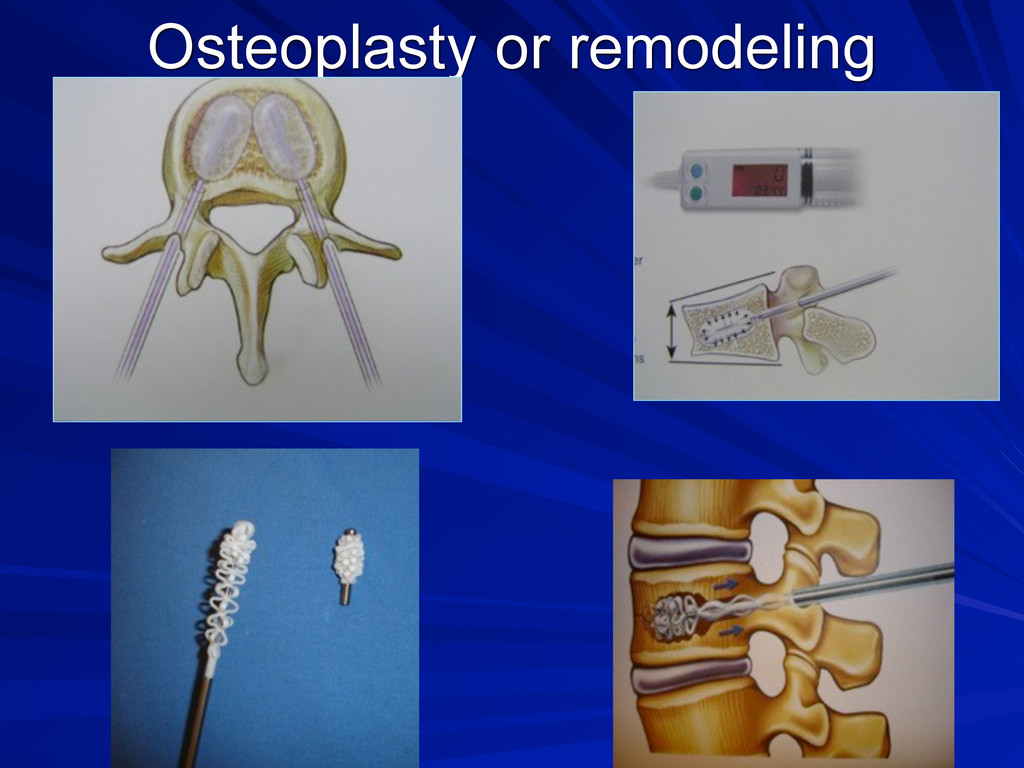
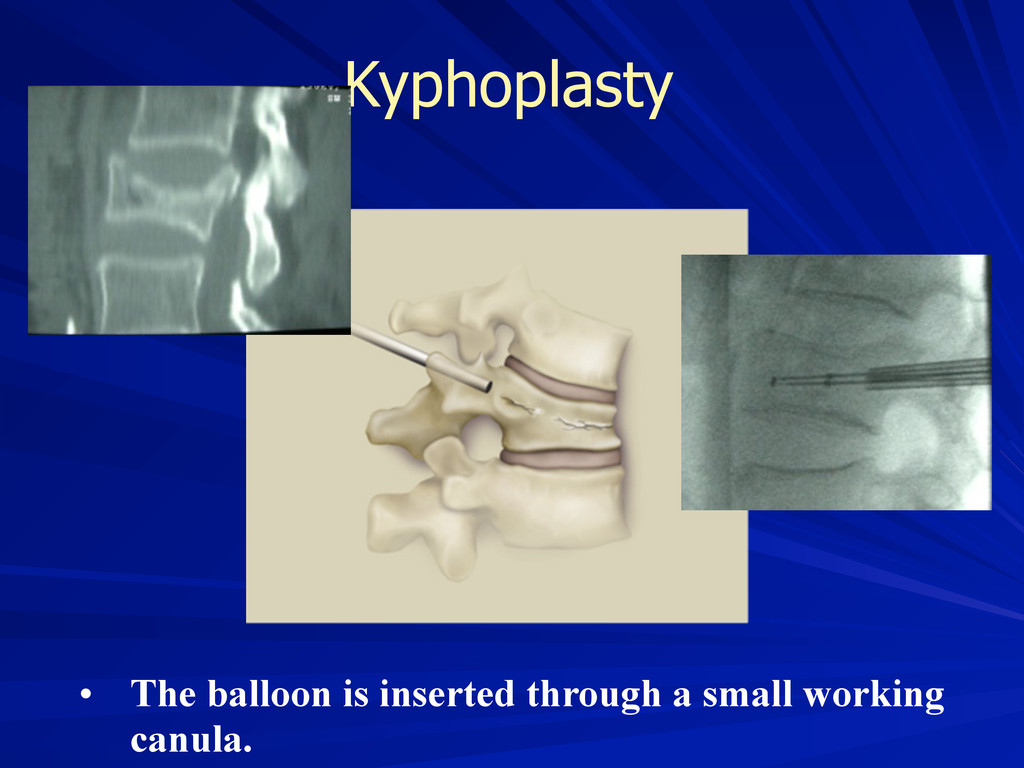
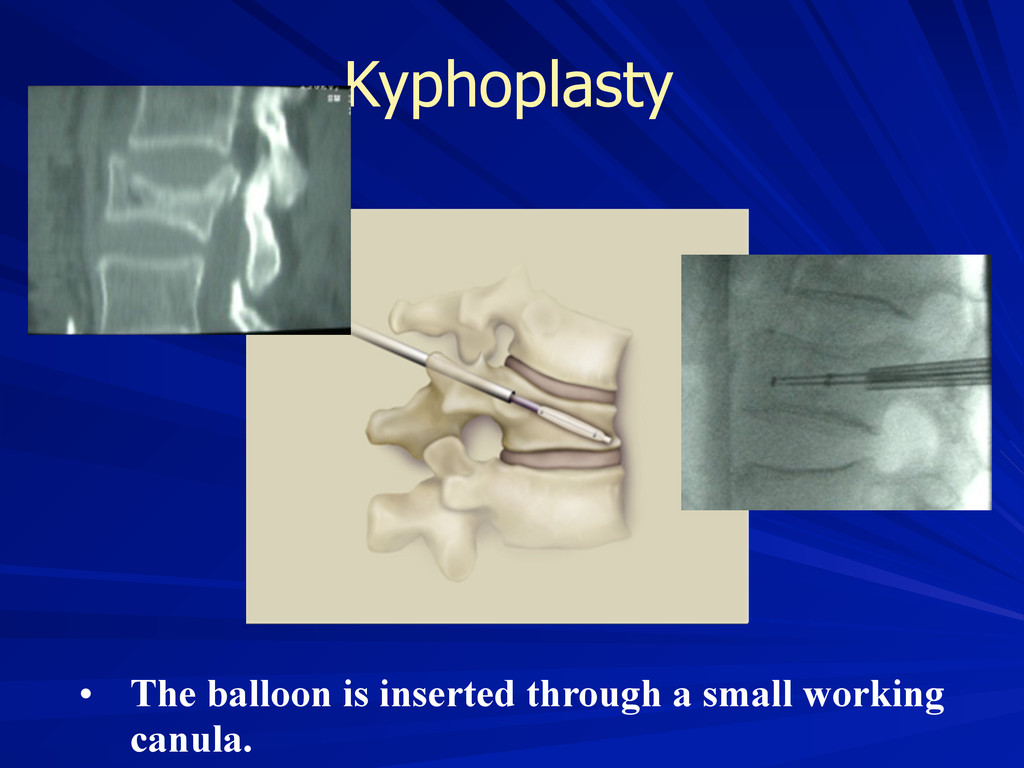
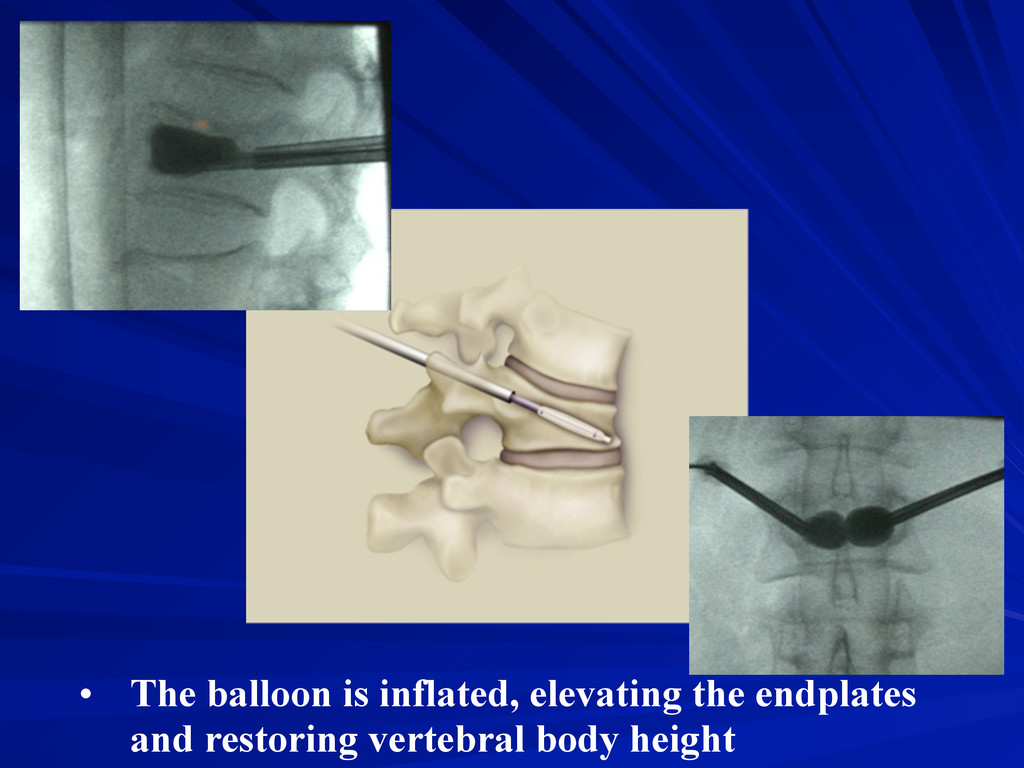
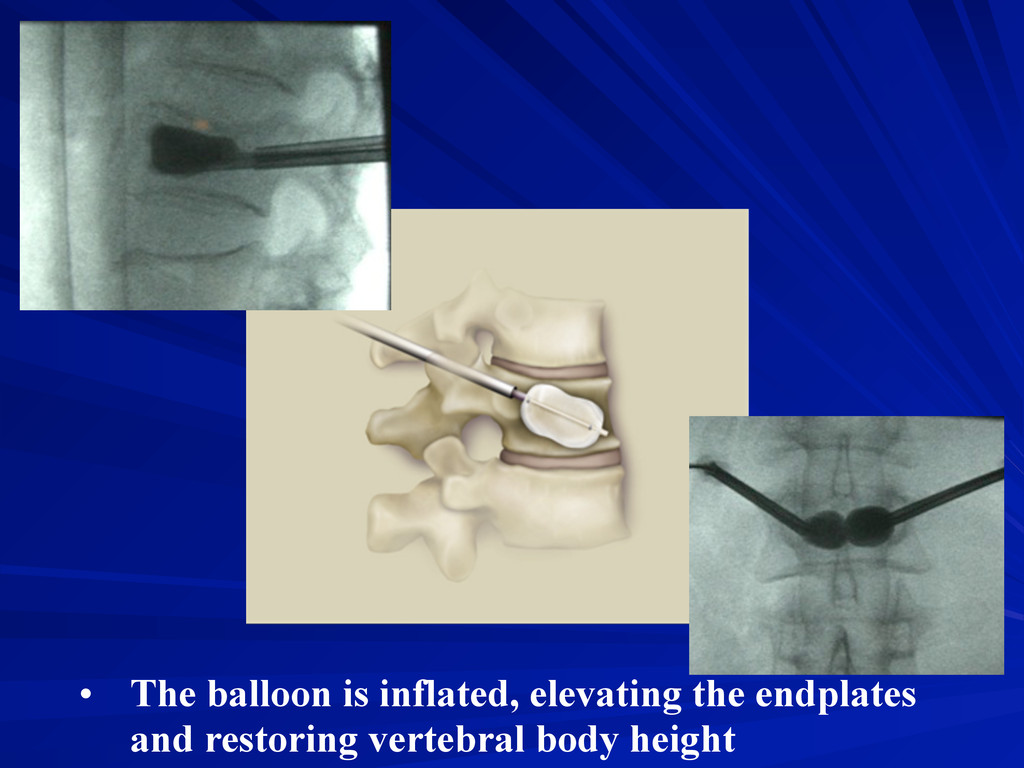
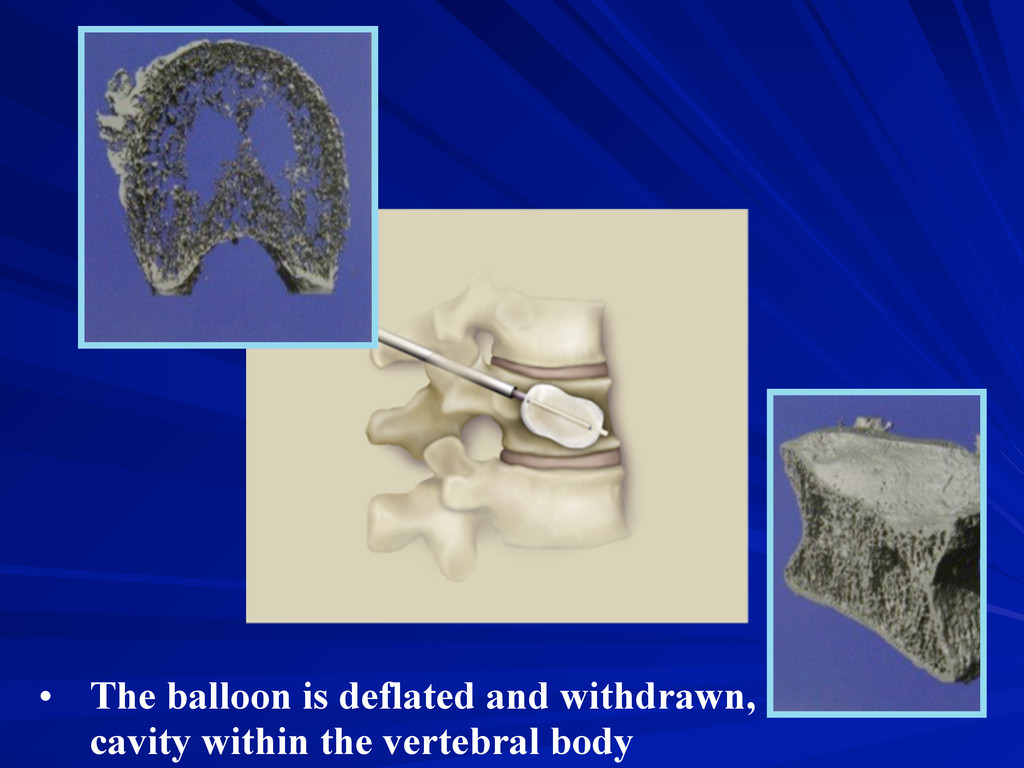
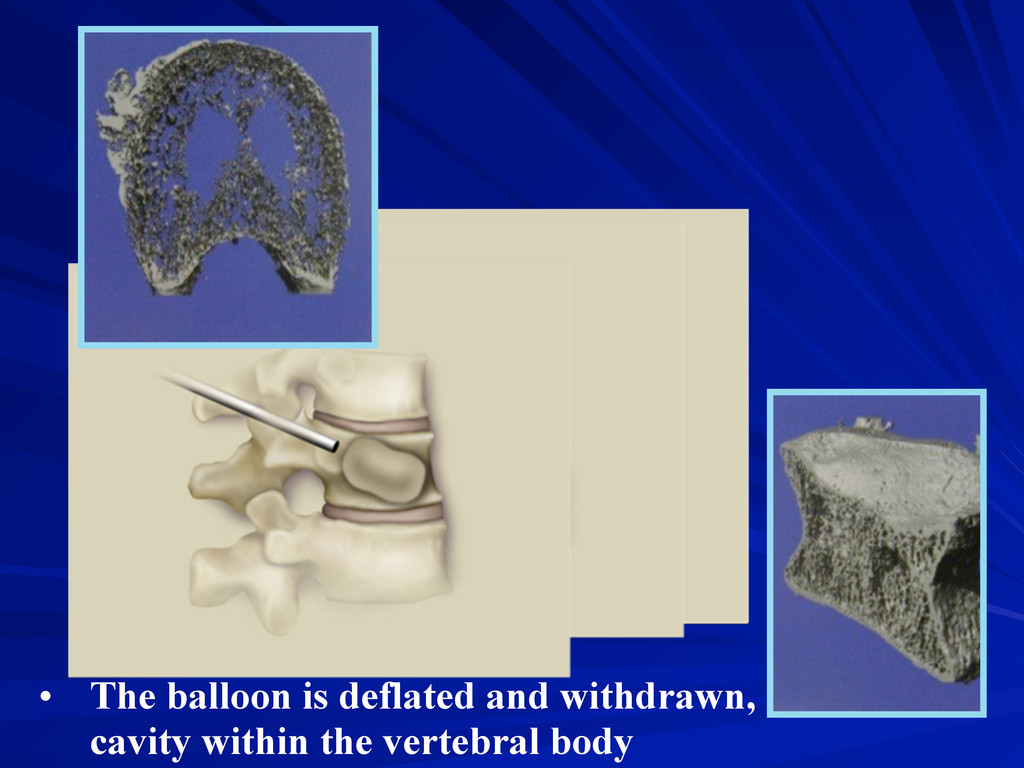
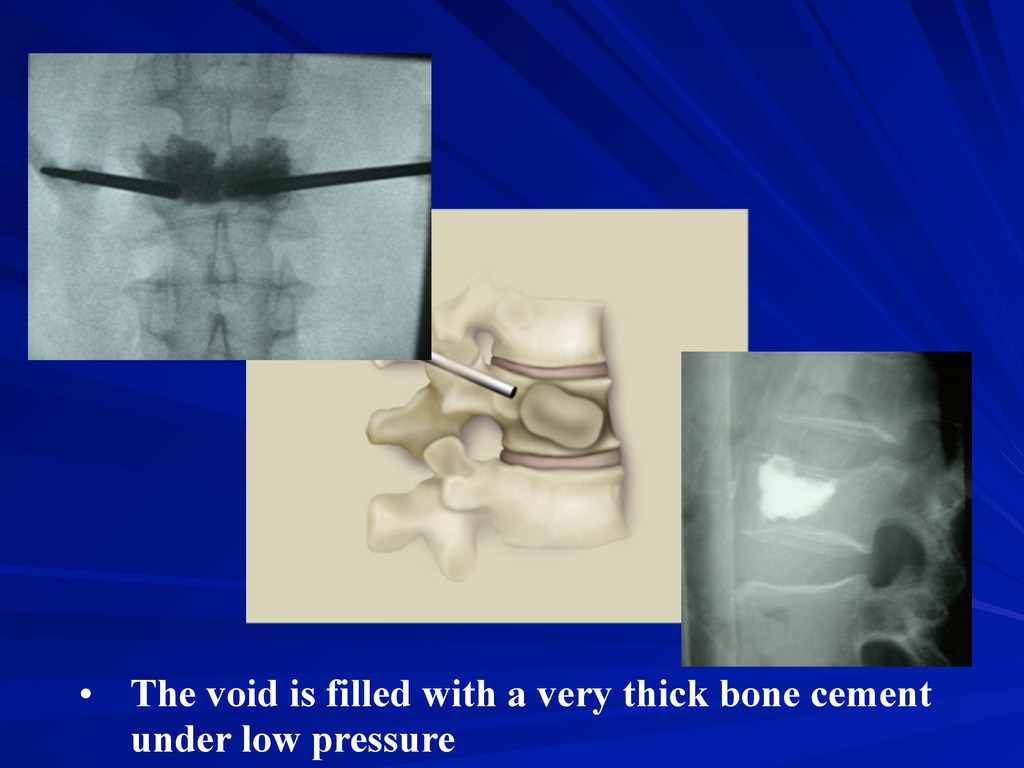
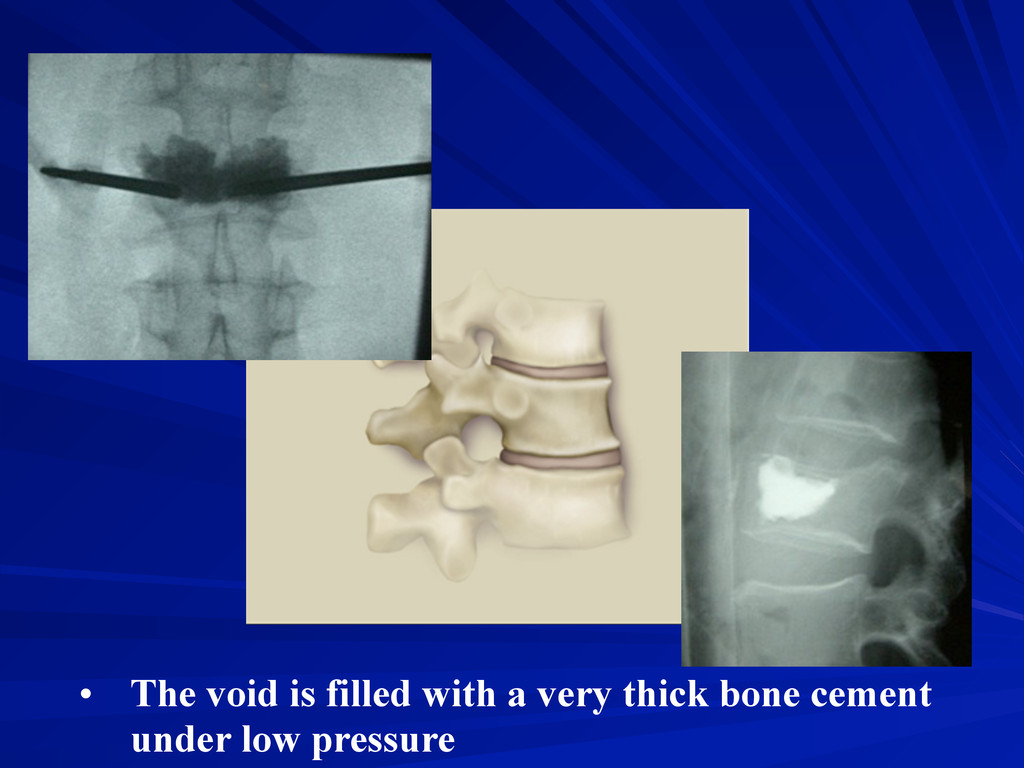
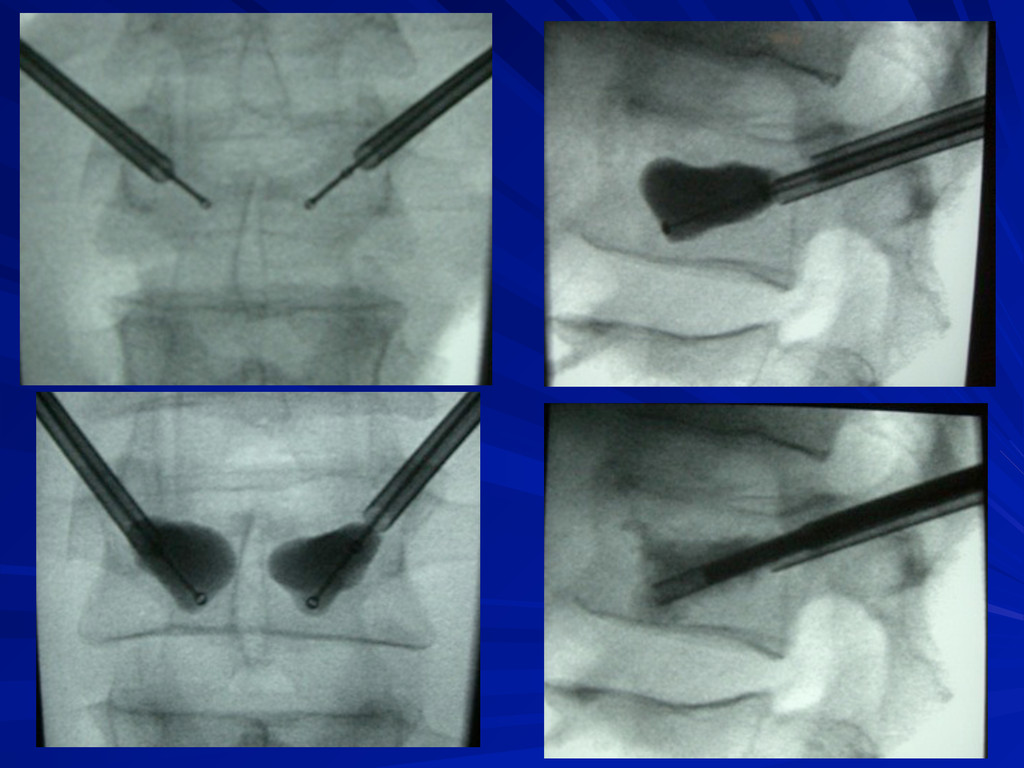
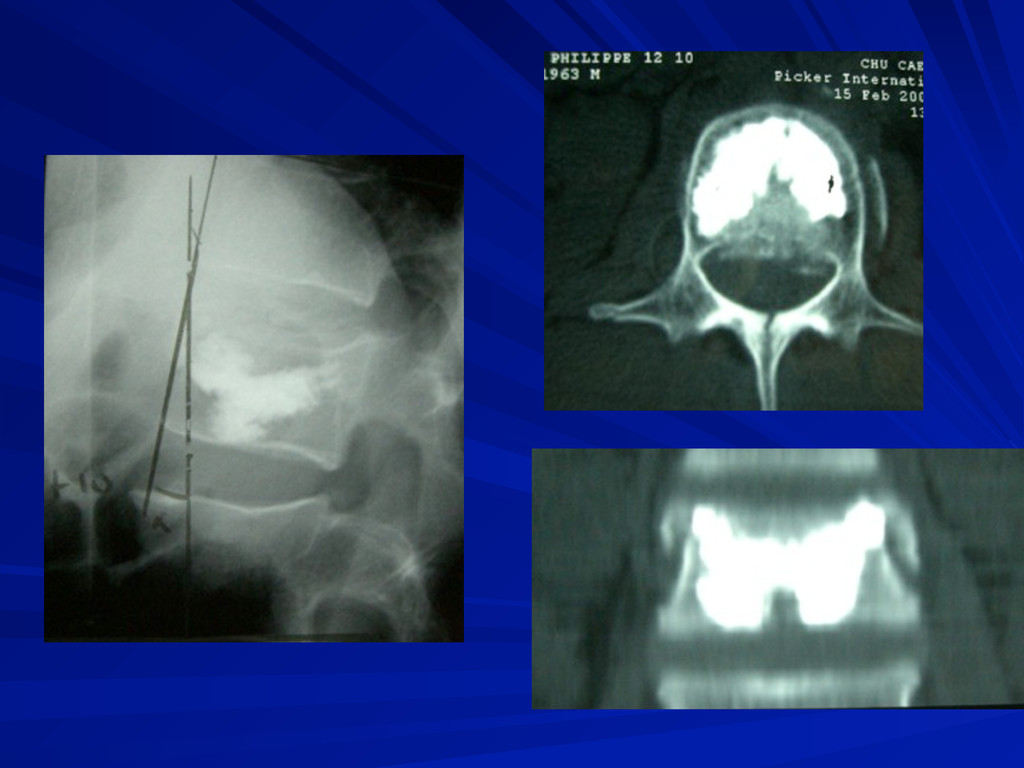
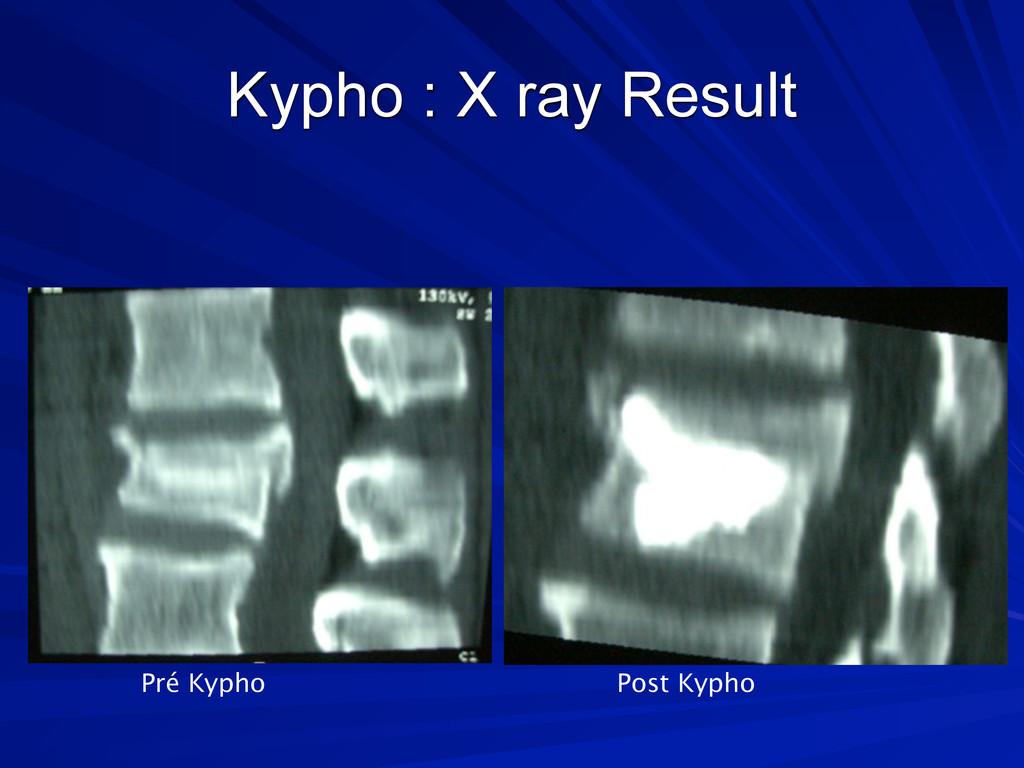
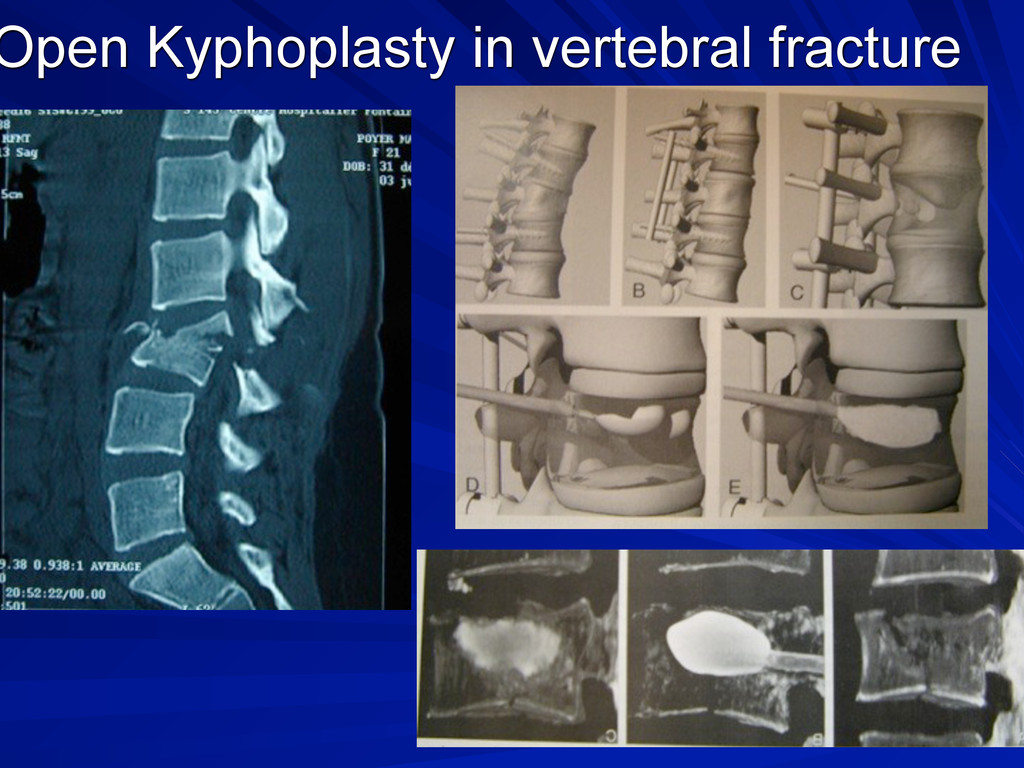
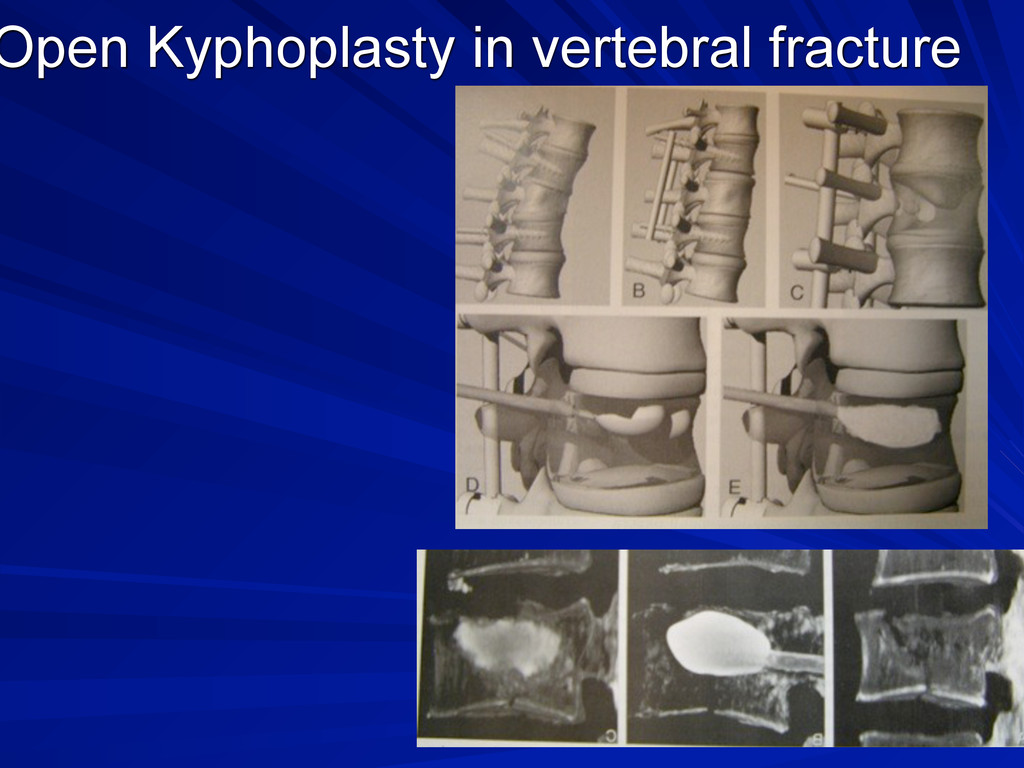
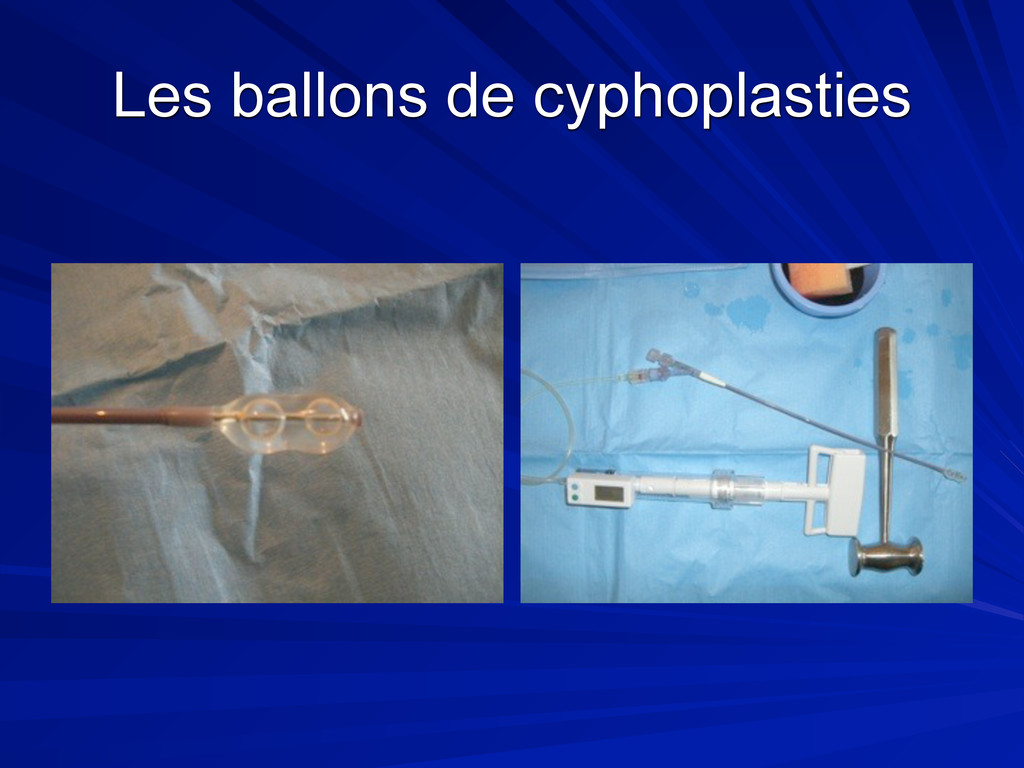
possible to inject through standard needle. New cements coming soon…. New indications : Burst Fractures : very promising results from personnal datas. Allows quick walk and prevents from delayed cyphosis Kyphoplasty : Can be used for kyphosis resisting to orthopedic positionning of the patient during vertebropalsty
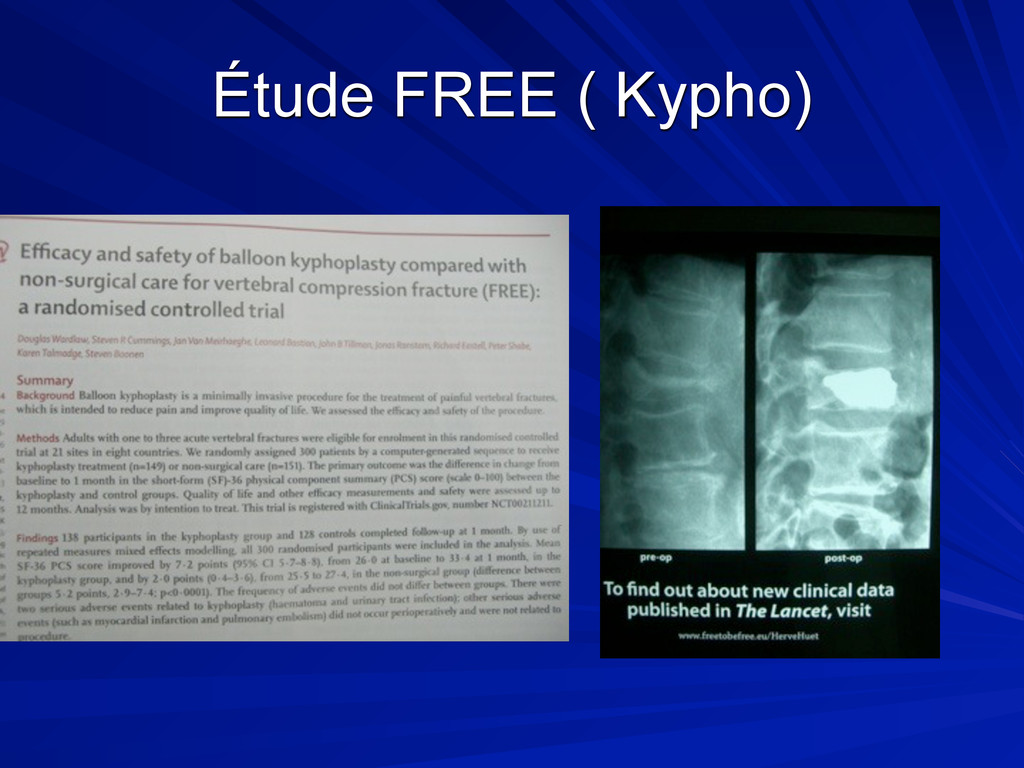
NS à l’amelioration cte groupe V . Tendance inv. ds le groupe placebo Fausse multicentrique IRM non systématique ( fracture récente?) Délai non précisé ( =/= / inclusion ) Cross- over important ++ 13 G.
R. Related Article by Kallmes, D. F. PubMed Citation To the Editor: In the August 6 issue, Kallmes et al.1 report on the Investigational Vertebroplasty Safety and Efficacy Trial (ClinicalTrials.gov number, NCT00068822 [ClinicalTrials.gov] ), and Buchbinder et al.2 report on a randomized trial of vertebroplasty for painful osteoporotic vertebral fractures (Australian New Zealand Clinical Trials Registry number, ACTRN012605000079640). We have serious concerns about both trials, which included patients with a duration of pain of up to 12 months. Vertebroplasty provides internal fixation of nonhealed osteoporotic vertebral fractures. It is well established that fixation of acute fractures elsewhere in the skeleton reduces fracture pain. Internal fixation of healed fractures is clearly . . . [Full Text of this Article] Réponse du 19 nov 2009
ou 2 vertèbres) GHM : 1000 à 4000 Euros …(voir avec dim ..) Kit Kypho =//= de 3500 E Kit ? Vertebro 200 à 600 E Durée d’hospi nécessaire 1 à 2 jours =/=durée pour toucher le GHM
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}