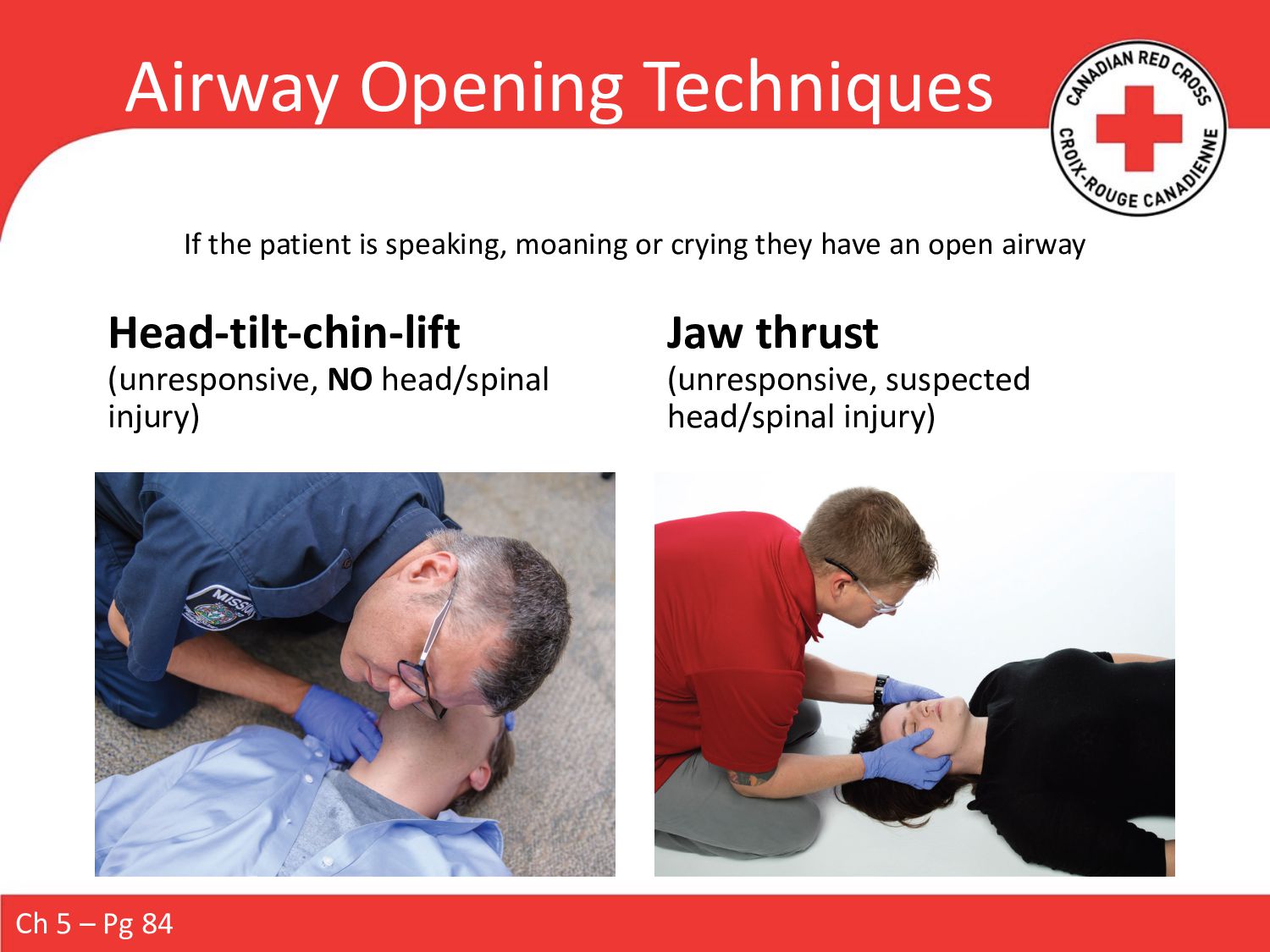
Because oxygen is vital to life, you must always ensure that the patient has an open airway and is breathing effectively. Airway and respiratory problems should be apparent when you check the patient’s ABCs during your primary assessment. A respiratory emergency can occur in two ways: Respiration becomes difficult or ineffective, or respiration stops entirely. A patient who is having difficulty breathing (dyspnea) is in respiratory distress. A patient who has stopped breathing is in respiratory arrest.
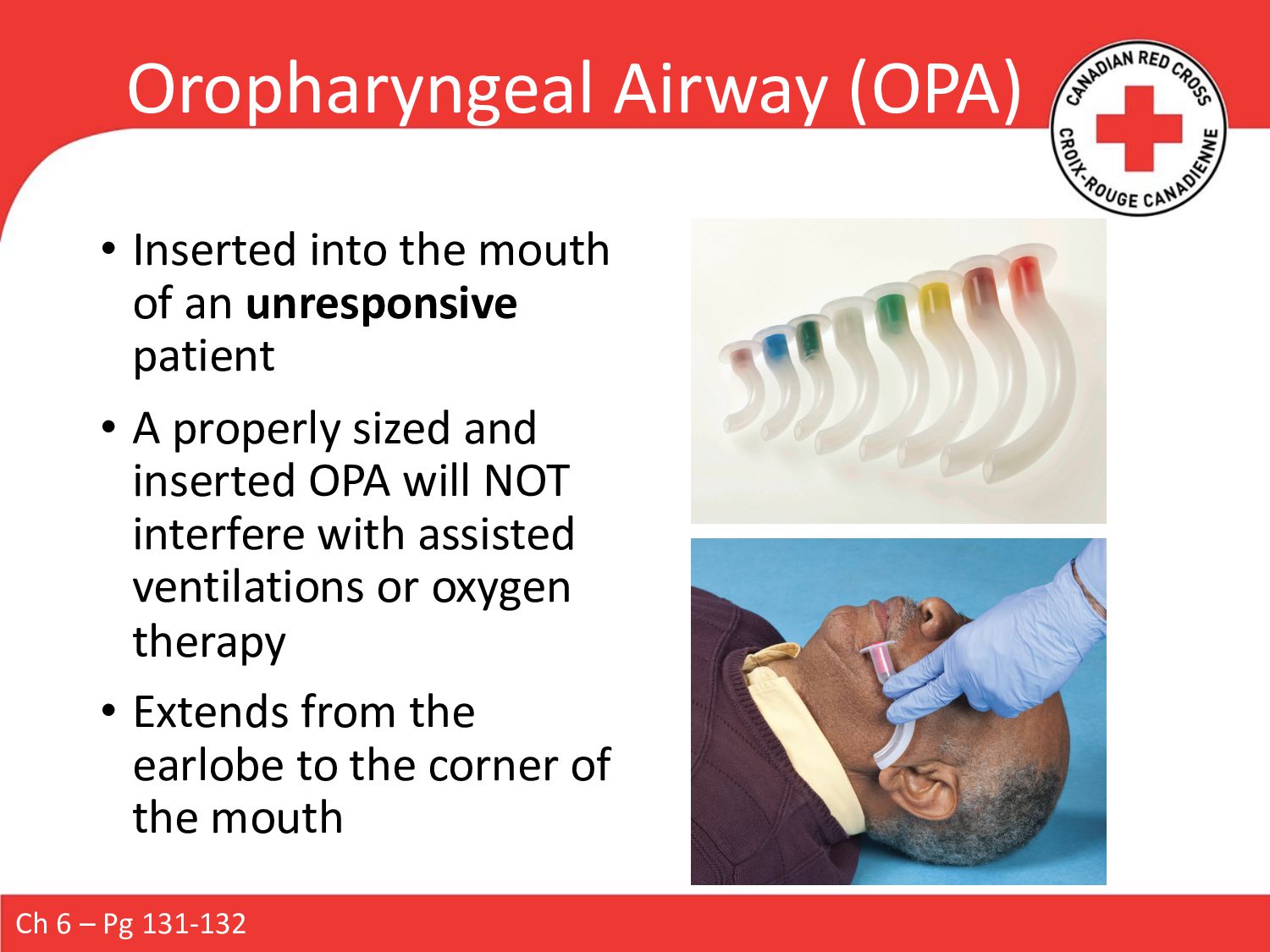
Airway management and ventilation can contribute significantly to the survival and recovery of a seriously ill or injured patient. A number of devices can help you maintain an open airway, perform ventilations, and/or increase the oxygen concentration in a patient’s bloodstream. In addition, some of these devices limit the potential for infection.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}