ICD-10 (And what to do if it won’t) Presentation to AAPC – Denver Chapter September 17, 2013 Vincent Bradshaw, PMP, CHTS-IS Disclaimer: This presentation is intended to provide accurate information as well as the presenter’s opinions and interpretations. The information was gathered from various government, commercial l and Internet sources. The topic of this presentation is dynamic and significant changes in the information may have taken place since the presentation was produced. The author has personal interests in consulting, presenting, writing about, and developing systems and software to assist medical providers and healthcare facilities .This presentation is for general educational purposes only and does not constitute business, professional or legal advice. Also, since each situation is different the presenter does not recommend any specific approach or course of action based solely on the information contained herein.
throughout the health system to the more complex ICD-10 diagnosis codes will go forward without any further delays…” – CMS letter to AMA Feb 6, 2013 “There are no plans for any more extensions…” - Farzad Mostashari National Coordinator for Health IT June 17, 2013
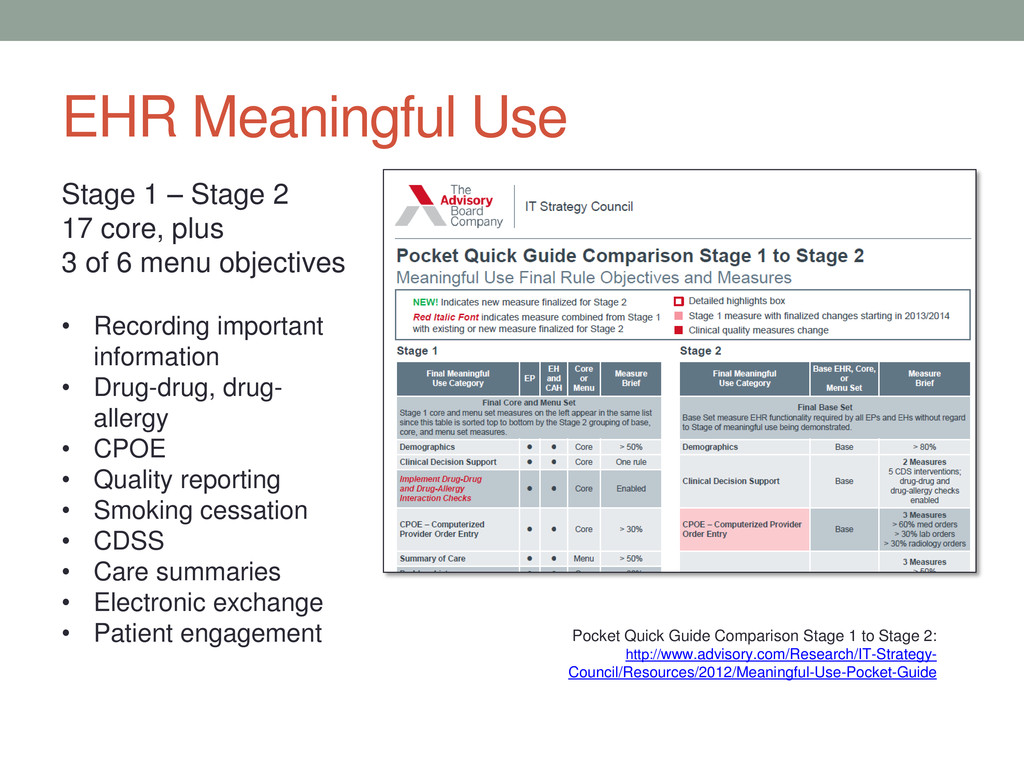
(HIPAA) Omnibus Rules – Sep 23, 2013 • Stage 2 Meaningful Use – 2014 (date depends on date provider certified for Stage 1) • HIE • Patient Engagement • Health Insurance Exchanges – PPACA uncertainty • ACOs, consolidation, outcomes-based reimbursement, clinical quality, value based purchasing EHR dissatisfaction - 31% of respondents said they are dissatisfied enough with their EHR to consider making a change, and 18% said they are looking to change systems within the next 12 months. -- Black Book Rankings’ 2013 State of the Ambulatory EHR Market
groups reported that they have not heard from their electronic health record vendor about when ICD-10 software changes or upgrades will be available for their practice. -- MGMA In April 2013 study, 20% of vendors indicated that their ICD-10 compliant products wouldn’t even be ready for beta testing until 2014. -- Workgroup for Electronic Data Interchange (WEDI)
Make sure providers and practice management understand the issues • Learn how your EHR works and how it captures clinical data • Work with your IT people to find out what your EHR and IT vendor’s plans and timetables are for ICD-10 • Check with your major payers and clearing houses to assess their plans and readiness • Prepare a test plan and start it now • Have a back up plan! Chinese character for danger and opportunity
project coordinator • Develop a transition plan • Determine how ICD-10 will affect your organization • Review ICD-10 clinical documentation requirements and EHR templates • Communicate the plan, timeline, changes and new processes • Set up a conversion budget • Communicate with vendors, payers, billing and IT staff
EHR incentives collected by 4,024 (79%) hospitals and (305,778) 76% EPs • Approx. 550 EHR vendors • 31% of providers dissatisfied enough to consider changing EHRs • 23% of patients access doc’s EHRs, 52% said they would like to access them
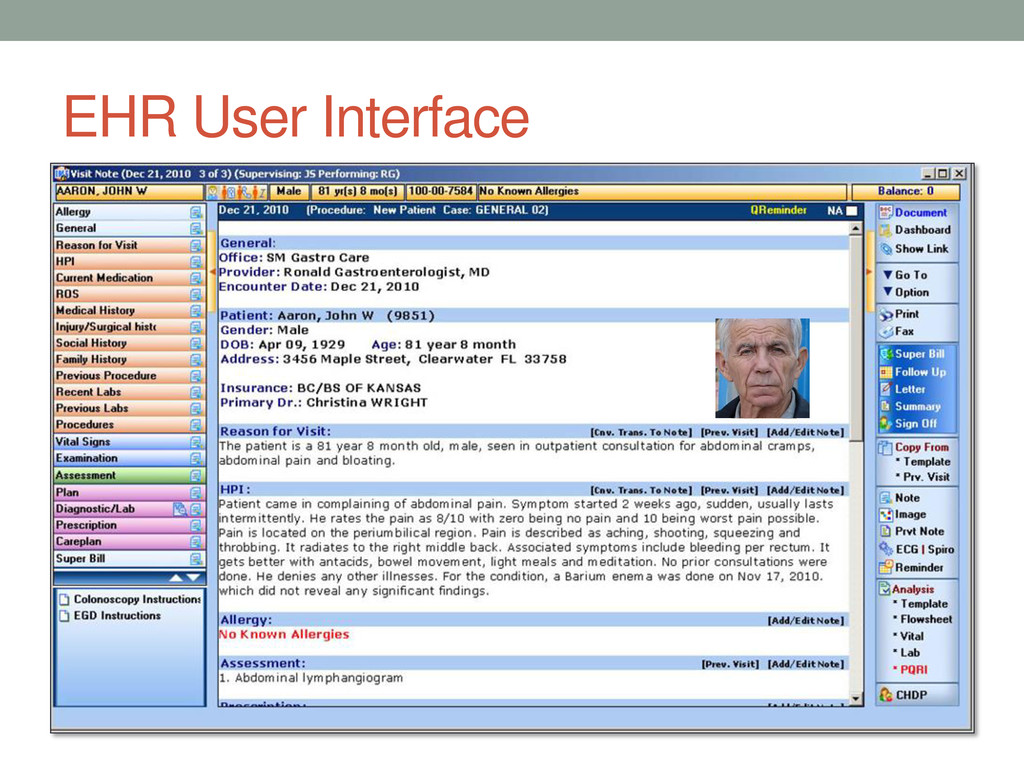
for visit • Allergy • HPI • Current medications • ROS • Medical history • Injury/surgical history • Social history • Family history • Labs (current and prior) • Procedures • Vital signs • Examination • Assessment • Plan • Diagnostic/labs • Prescriptions • Care plan • Superbill • Auditing and management dashboards HL-7 and SNOMED-CT
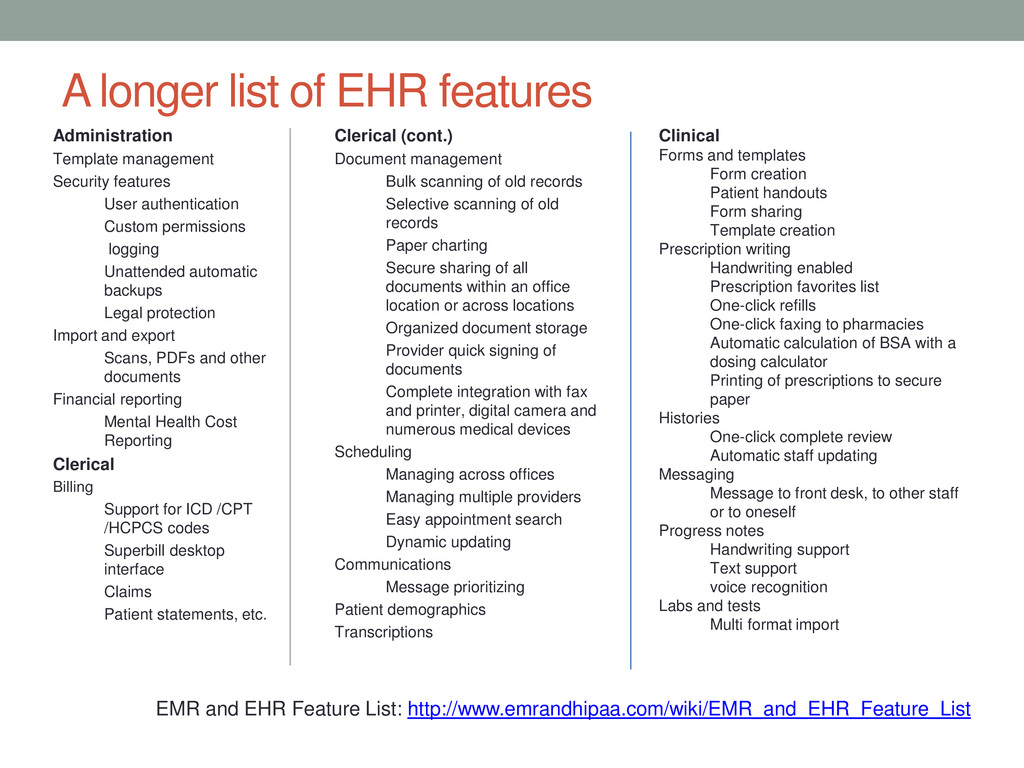
features User authentication Custom permissions logging Unattended automatic backups Legal protection Import and export Scans, PDFs and other documents Financial reporting Mental Health Cost Reporting Clerical Billing Support for ICD /CPT /HCPCS codes Superbill desktop interface Claims Patient statements, etc. Clerical (cont.) Document management Bulk scanning of old records Selective scanning of old records Paper charting Secure sharing of all documents within an office location or across locations Organized document storage Provider quick signing of documents Complete integration with fax and printer, digital camera and numerous medical devices Scheduling Managing across offices Managing multiple providers Easy appointment search Dynamic updating Communications Message prioritizing Patient demographics Transcriptions Clinical Forms and templates Form creation Patient handouts Form sharing Template creation Prescription writing Handwriting enabled Prescription favorites list One-click refills One-click faxing to pharmacies Automatic calculation of BSA with a dosing calculator Printing of prescriptions to secure paper Histories One-click complete review Automatic staff updating Messaging Message to front desk, to other staff or to oneself Progress notes Handwriting support Text support voice recognition Labs and tests Multi format import EMR and EHR Feature List: http://www.emrandhipaa.com/wiki/EMR_and_EHR_Feature_List
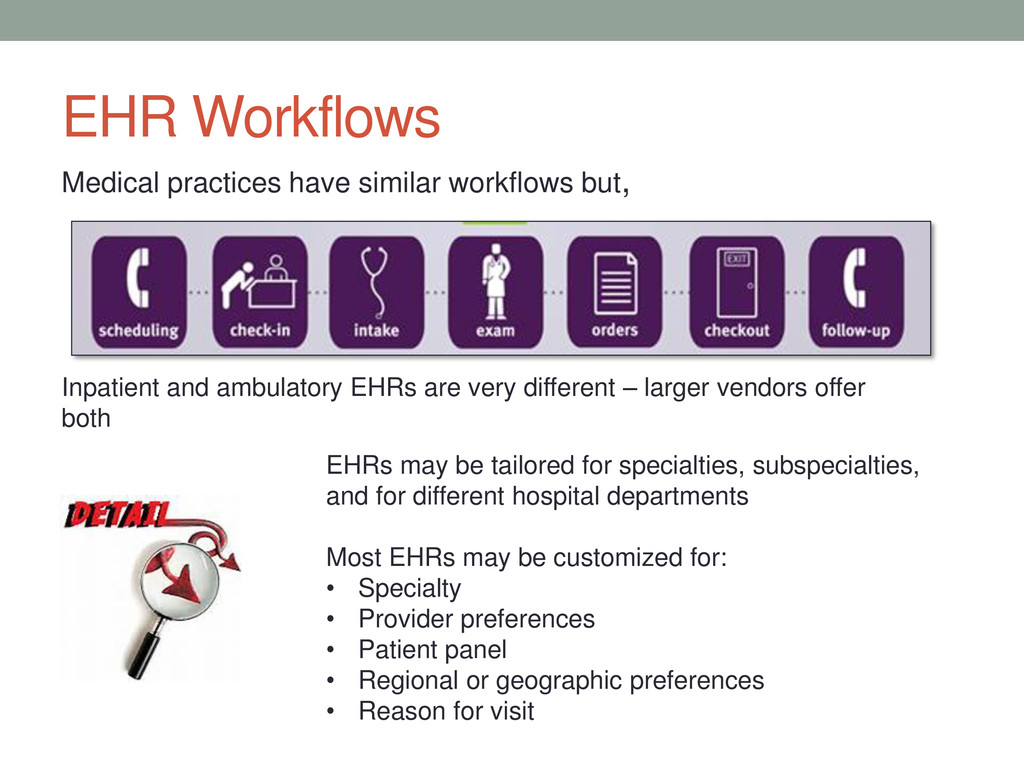
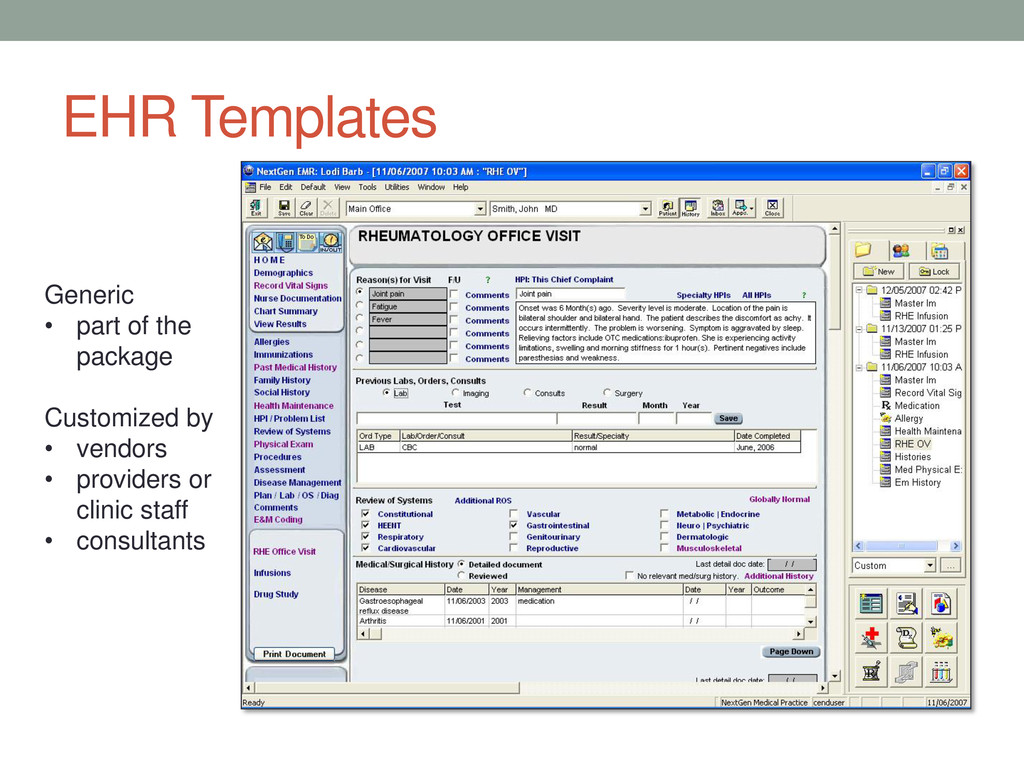
be tailored for specialties, subspecialties, and for different hospital departments Most EHRs may be customized for: • Specialty • Provider preferences • Patient panel • Regional or geographic preferences • Reason for visit Inpatient and ambulatory EHRs are very different – larger vendors offer both
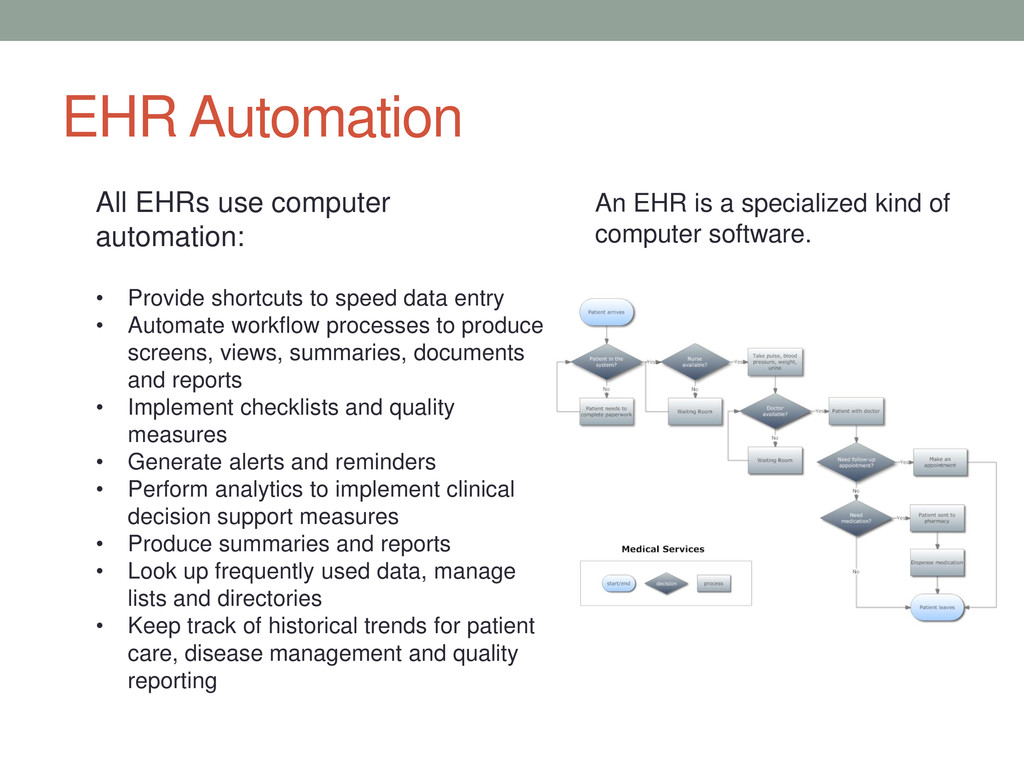
to speed data entry • Automate workflow processes to produce screens, views, summaries, documents and reports • Implement checklists and quality measures • Generate alerts and reminders • Perform analytics to implement clinical decision support measures • Produce summaries and reports • Look up frequently used data, manage lists and directories • Keep track of historical trends for patient care, disease management and quality reporting An EHR is a specialized kind of computer software.
If misused, they also make it easier to make mistakes and harder to detect them. • Templates created by technology vendors often use the same verbiage • Templates can raise suspicions of fraud • Templates and other shortcuts discussed later can increase the probability of medical error, lawsuits, regulatory action, claim denials and revenue recovery • Usability: Does your EHR work well on portable devices?
provide sufficient documentation: “CMS does not prohibit the use of templates to facilitate record-keeping. CMS also does not endorse or approve any particular templates. A physician/LCMP may choose any template to assist in documenting medical information. Some templates provide limited options and/or space for the collection of information such as by using “check boxes,” predefined answers, limited space to enter information, etc. CMS discourages the use of such templates. Claim review experience shows that that limited space templates often fail to capture sufficient detailed clinical information to demonstrate that all coverage and coding requirements are met. Physician/LCMPs should be aware that templates designed to gather selected information focused primarily for reimbursement purposes are often insufficient to demonstrate that all coverage and coding requirements are met. This is often because these documents generally do not provide sufficient information to adequately show that the medical necessity criteria for the item/service are met. If a physician/LCMP chooses to use a template during the patient visit, CMS encourages them to select one that allows for a full and complete collection of information to demonstrate that the applicable coverage and coding criteria are met. “ (emphasis added) --CMS Transmittal 438, superseded by Transmittal 455
provide sufficient information to determine: • Laterality • Encounter type (initial, subsequent, sequela, routine healing, delayed healing, etc.) • Anatomic details • Severity, Stage • Disease relationships • Body part • Approach • Device ICD-9-CM Pressure ulcer codes - 9 location codes (707.00 – 707.09) Show broad location, but not depth (stage) ICD-10-CM Pressure ulcer codes - 150 codes Show more specific location as well as depth, including: L89.131 – Pressure ulcer of right lower back, stage 1 L89.132 – Pressure ulcer of right lower back, stage 2 L89.133 – Pressure ulcer of right lower back, stage 3 L89.134 – Pressure ulcer of right lower back, stage 4 L89.139 – Pressure ulcer of right lower back, unspecified stage ICD-9-CM Angioplasty - 1 code (39.50) ICD-10-PCS Angioplasty codes - 854 codes Specifying body part, approach, and device, including: 047K04Z – Dilation of right femoral artery with drug-eluting intraluminal device, open approach 047K0DZ – Dilation of right femoral artery with intraluminal device, open approach 047K0ZZ – Dilation of right femoral artery, open approach 047K34Z – Dilation of right femoral artery with drug-eluting intraluminal device, percutaneous approach
in the background. They are used to perform calculations, move data around to different locations, pull in data from external sources, and automate repetitive functions. All EHRs use scripts… • Scripts are generally embedded in the system • Generally speaking only the programmer knows what it actually does • Many EHR basic features are based on scripts • Incorrect or outdated scripts can introduce errors, add unrelated information or reach faulty conclusions • EHR scripts are frequently used to generate or populate physician notes, create CCDs, patient care instructions and other documentation • Used in many outpatient EHRs to determine which E&M code applies to a particular visit
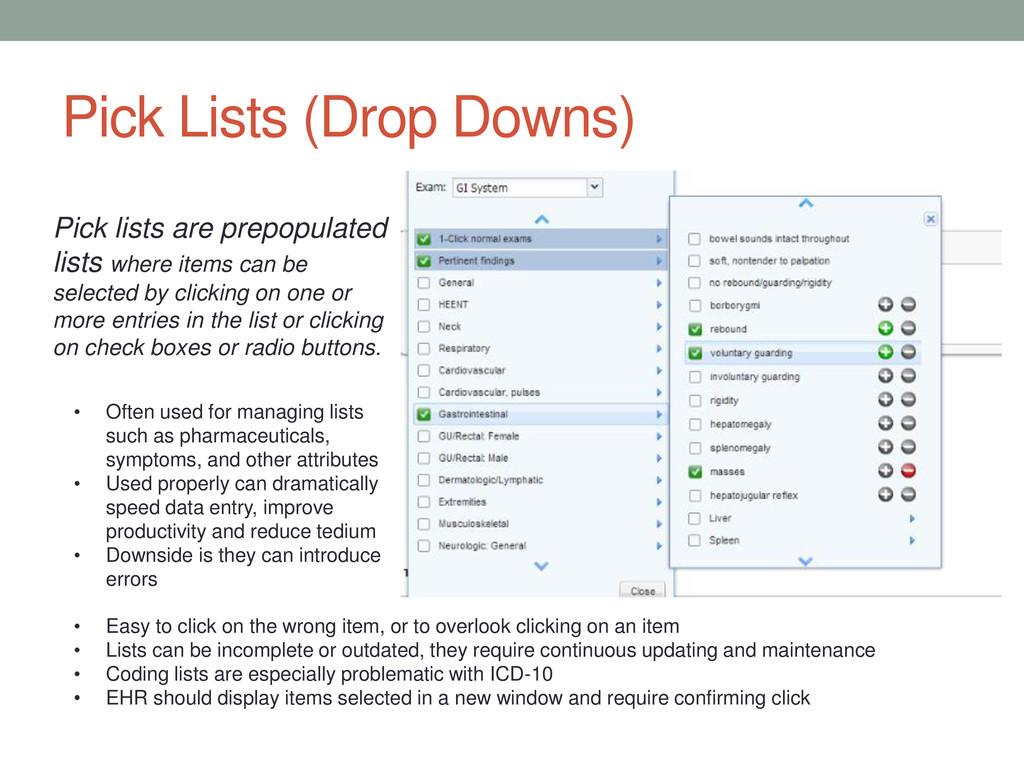
by clicking on one or more entries in the list or clicking on check boxes or radio buttons. • Often used for managing lists such as pharmaceuticals, symptoms, and other attributes • Used properly can dramatically speed data entry, improve productivity and reduce tedium • Downside is they can introduce errors • Easy to click on the wrong item, or to overlook clicking on an item • Lists can be incomplete or outdated, they require continuous updating and maintenance • Coding lists are especially problematic with ICD-10 • EHR should display items selected in a new window and require confirming click Pick Lists (Drop Downs)
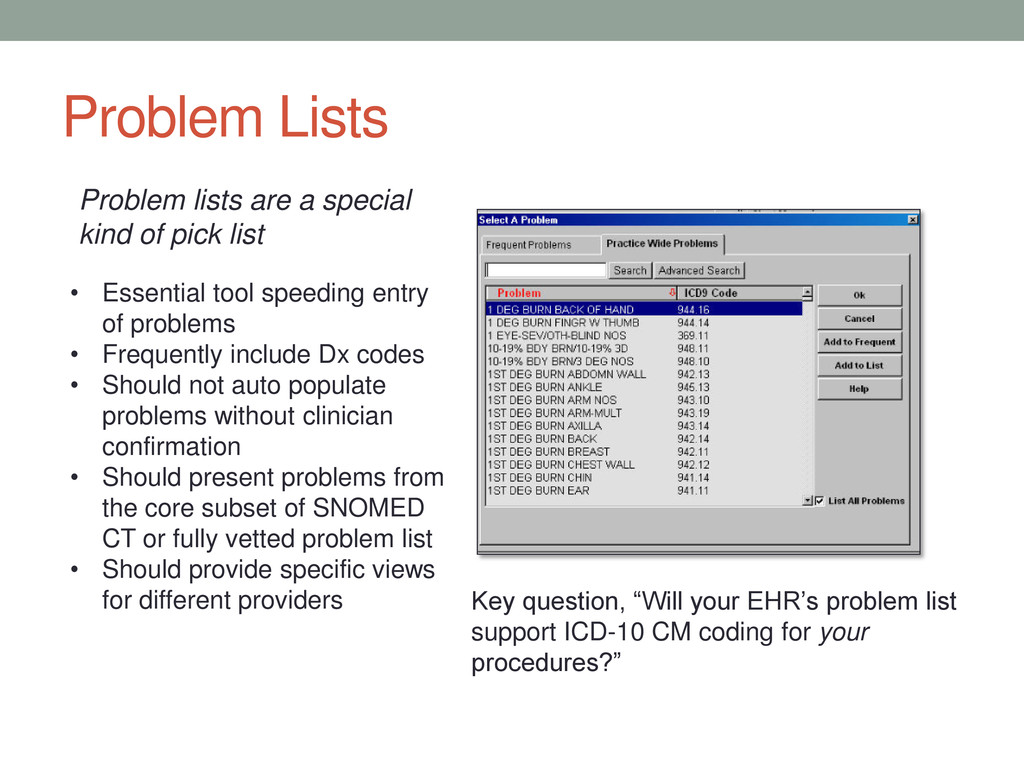
Frequently include Dx codes • Should not auto populate problems without clinician confirmation • Should present problems from the core subset of SNOMED CT or fully vetted problem list • Should provide specific views for different providers Problem lists are a special kind of pick list Key question, “Will your EHR’s problem list support ICD-10 CM coding for your procedures?”
document HPI based on the patient's description that day. Never copy from a previous visit. • Double-check all diagnoses. Some EHRs copy all diagnoses listed in the problem list. • If another physician's interpretation or consultation is copied, should remember that he or she already has billed for that work. • Copying and pasting of text from another person's note without attribution is plagiarism and may constitute billing fraud. • Avoid repetitive copying and pasting of laboratory results and radiology reports. • Avoid wholesale inclusion of information readily available elsewhere in the EHR. • Copying and pasting other elements of the history, physical examination or formulations is risky, as errors in editing may jeopardize the credibility of the entire note. Copies only selected portions of a prior record to then be pasted into a new encounter
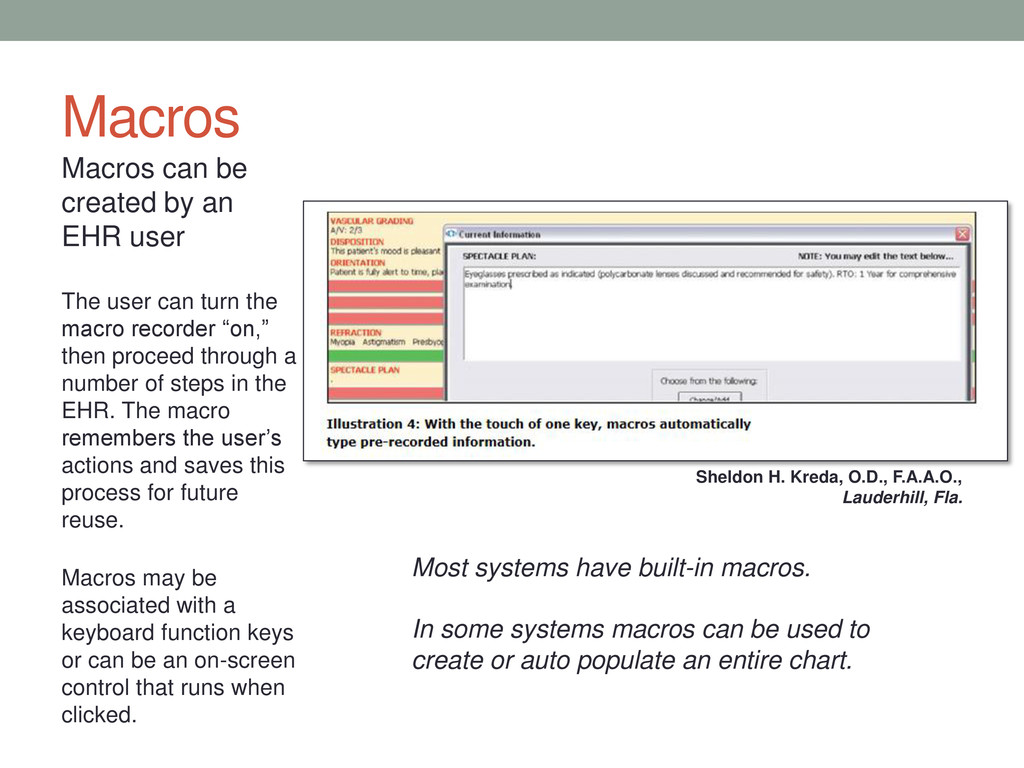
user can turn the macro recorder “on,” then proceed through a number of steps in the EHR. The macro remembers the user’s actions and saves this process for future reuse. Macros may be associated with a keyboard function keys or can be an on-screen control that runs when clicked. Most systems have built-in macros. In some systems macros can be used to create or auto populate an entire chart. Sheldon H. Kreda, O.D., F.A.A.O., Lauderhill, Fla.
information before all of it can be digested and understood • Copy forward is inappropriate for a patient’s ROS, medical history and physical examination findings • Can offer a benefit in bringing forward a patient’s problem or medication list – but doctor must check and sign-off • If copy forward is being used, the EHR at a minimum should require a second click to verify the copied information is correct “Copying forward a previous review of systems without reviewing changes in the patient’s status, for example, is noncompliant and potentially fraudulent…If you bring the information forward with a single- click, the machine is doing the thinking, not the doctor,” says Stephen Levinson, MD. EHR finds the last note entered and literally copies every field forward into a new note.
• Can provoke auditors looking for potential fraud • Can propagate hidden mistakes to multiple encounters or even transfer it from one patient’s chart to others Best advice, is don’t use cloning… But if your providers insist on cloning records, they should adhere to consistent rules: • Never clone from one patient’s record to a different patient’s record • Make sure cloned ROS is medically necessary for current visit • Provider must carefully review and edit any information carried forward from a prior visit At least 2 Medicare Administrative Contractors (MAC) have announced they will recoup payments for Medicare claims if an audit uncovers cloned documentation.
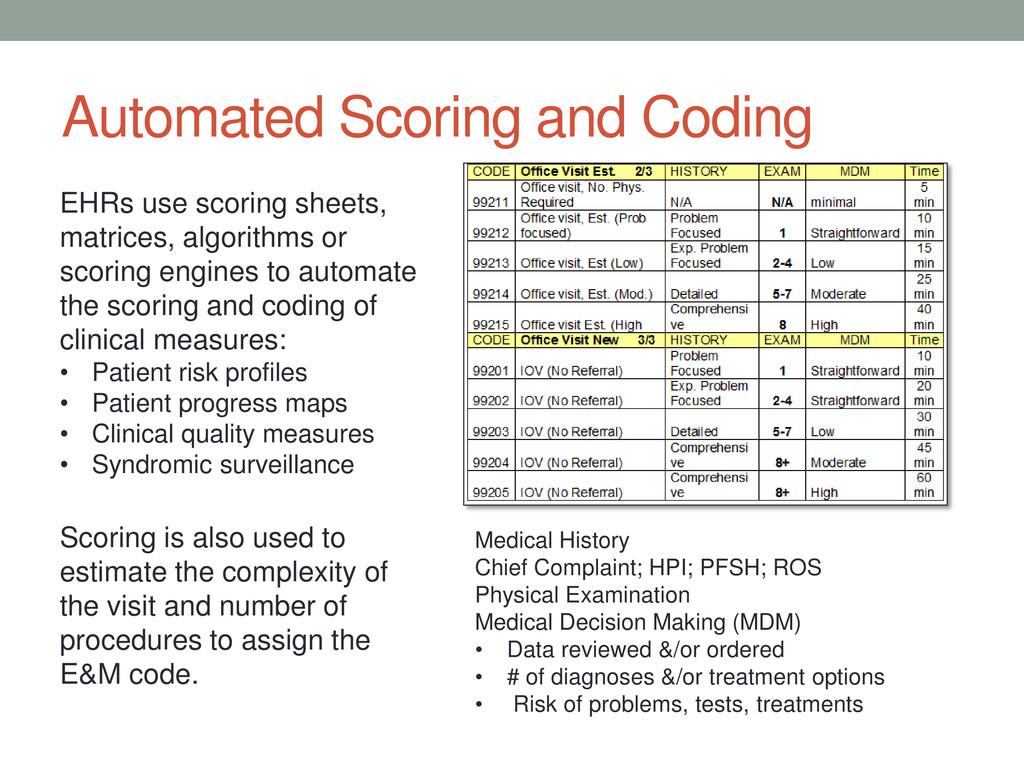
or scoring engines to automate the scoring and coding of clinical measures: Medical History Chief Complaint; HPI; PFSH; ROS Physical Examination Medical Decision Making (MDM) • Data reviewed &/or ordered • # of diagnoses &/or treatment options • Risk of problems, tests, treatments Nature of the presenting problem (NPP) Counseling Coordination of Care Time Scoring is also used to estimate the complexity of the visit and number of procedures to assign the E&M code. • Patient risk profiles • Patient progress maps • Clinical quality measures • Syndromic surveillance Prescription drug monitoring Immunization data Reporting health statistics
to stay: automation and analytics are essential components of EHRs: • Automation brings promise of faster, less costly, higher quality care • Analytics promise quicker identification of disease, better reporting of health trends, patients more engaged in their care, and improved outcomes The providers and practice team are still responsible for: • Care provided patients • Compliance with good medical practices, laws and regulations • Accuracy of billing and claims • Health and survival of the business Automation and analytics turn over much of the process thinking to programmers and system administrators: • Automating a bad process is a faster way to a bad ending– GIGO • System designers and vendors are subject to many competing demands • Software code and data systems, even if well designed, become outdated or corrupted over time if not maintained properly
Pre-auths - state forms, HMOs, workers comp Prescription monitoring – narcotics Benefits eligibility Claims status, resubmissions, appeals Disability, return to work documentation Immunization logs - pediatrics Evidence of medical necessity for wheel chairs, oxygen, etc.
How is it doing today? ICD-9 coding accuracy CPT – HCPCS coding accuracy Any 5010 issues? Reliability? Easy to use? HIPAA compliance? Data security and backup? Vendor support? Vendor certification status? Cost to maintain, expand? Check your contract – are you and the vendor in compliance? Are you one of the 31 percenters?
good vendor contact Make sure your IT support is on board Use a checklist Ask detailed, pointed questions - insist on specific answers Document every discussion and communication Ask them their timeline for ICD-10 compliance. Where will they be at end of 2013? Get a firm commitment of when you can begin ICD-10 testing Make sure new EHR releases comply with Meaningful Use 2 What training will the vendor provide and when? Physicians and clinical staff Coding strategies and clinical documentation. Are there any additional costs or hardware associated with the ICD-10 upgrade?
ICD-10 release simplify your transition? • How will functionality of the upgraded system compare with your current system? • Will your implementation require a complete system conversion? • How much time will it take to upgrade your system? • Is the upgrade the vendor’s own software or does it involve third parties? • Are their any hidden costs? • How much time will training take? • What is the timeframe for implementation? • What testing will vendor do before they release the upgrade? • What testing will vendor do after the install the upgrade? • What guarantees do they offer, and are they in writing? If you like the vendor’s answers to your first questions…
to test your coding processes and knowledge • Focus on procedures that produce the greatest revenue (Good time to get your finance people in the loop) • Pareto’s Law • Most important CPT • Most important DRGs “Take a sample of claims that have already been adjudicated successfully and paid and try to assign an ICD-10 code to that claim based on the existing documentation. During the next year, it is a good exercise to say “What would that ICD-10 code be?” -- Robert M. Tennant, MA Senior Policy Advisor at the Medical Group Management Association (MGMA) • Verify crosswalks for your key procedures – don’t blindly rely on GEMs • Educate your providers on what they need to do to support the documentation requirements for ICD-10 (CM and/or PCS)
Internal Testing: how the information flows within the provider system, as well as ensuring that ICD-10 codes are processed correctly from beginning to end External Testing: how transactions are sent and received between external trading partners, such as payers, clearinghouses, billing services, etc. through channels already in use Revenue Impact Assessment: ensures the processing of data, either CPT/HCPCS or ICD-10, does not negatively impact revenue generation, and that there are no vast differences in the revenue generated between ICD-9 and ICD-10 data End-to-End Business Process Testing: making sure the full spectrum works together and meets the expectations of everyone involved (from doctors and patients to billing services and clearinghouses)
the conversion, potential impacts on patient care and revenue generation Clinical documentation improvement testing and validation: because ICD-10 will require more documentation, this validates the appropriateness of, identifies deficiencies in, and recommends improvements to the EHR templates, views and records, not just to support coding but improve patient care Verification and Validation: set up separate tools, (e.g., spreadsheets, tracking logs) to monitor revenue flow and claims before, during and after conversion Perform verification audits of actual claims until you are sure everything is working
out of things that can go wrong. • Think outside the box: Identify alternative ways to code and submit claims without relying on the EHR to generate the codes or provide all the documentation: o Electronic or manual check lists for each patient visit to ensure necessary information is captured o Maybe back up paper checklists and temporary charts • Use all available resources : Train front desk and other support staff on coding basics to have them ready to help out in a pinch • Bring in more troops: Identify staffing agencies or contractors who can provide qualified coding specialists, data analysts, EHR experts, etc. Check your schedule: Sept-Oct 2014 might not be the best time to schedule vacations?
Market “Black Book Rankings:” http://www.blackbookrankings.com/healthcare/rankings-ambulatory-physician-emr.php Appropriate Documentation in an EHR: Use of Information That Is Not Generated During the Encounter for Which the Claim is Submitted: Copying/Importing/Scripts/Templates: https://www.aamc.org/download/253812/data/appropriatedocumentationinanehr.pdf A Wholistic Approach to ICD-10 Testing for Healthcare Providers: http://www.qualitestgroup.com/ICD-10-Testing- White-Paper: An Appropriate Use of Copy Forward, with a Caveat: http://journal.ahima.org/2008/06/04/an-appropriate-use-of- copy-forward-with-a-caveat/ Cloned EHR Notes Jeopardize Medicare Payment: http://www.medscape.com/viewarticle/771548 CMS ICD-10 Website: http://www.cms.gov/Medicare/Coding/ICD10/index.html CMS Transmittal 455: http://www.cms.gov/Regulations-and- Guidance/Guidance/Transmittals/Downloads/R455PI.pdf CMS: No more delays with move to ICD-10: http://www.amednews.com/article/20130304/government/130309977/7/ Conquering Coding’s Everest: Compliant E/M Coding & Auditing for Electronic Health Records: http://static.aapc.com/a3c7c3fe-6fa1-4d67-8534-a3c9c8315fa0/e0bdf19e-6a7c-4179-9300- 8acc467f224e/45682476-d260-4da0-8a99-ab676088be44.pdf EHR templates could cost providers reimbursement dollars: http://www.fierceemr.com/story/why-ehr-templates- could-cost-providers-reimbursement/2012-12-13 Emergency cash a must for ICD-10: http://www.healthcareitnews.com/news/emergency-cash-must-move-icd-10 EMR and EHR Feature List: http://www.emrandhipaa.com/wiki/EMR_and_EHR_Feature_List Five things your EMR will never do: http://www.emrandhipaa.com/james/2013/08/15/things-your-emr-will-never-do/ HIMSS ICD-10 Playbook: http://www.himss.org/library/icd-10/playbook?navItemNumber=13480 How to Avoid the Potential Pitfalls of Automated E&M Coding in EHRs: http://www.e-mds.com/news/how-avoid- potential-pitfalls-automated-em-coding-ehrs ICD-10 Coding with Change Documentation: http://www.aapcps.com/news-articles/ICD- 10%20Coding%20Will%20Change%20Documentation.aspx
creep towards readiness: http://ehrintelligence.com/2013/04/12/icd-10- survey-vendors-payers-barely-creep-towards-readiness/ ICD-10-CM/PCS Transition: Planning and Preparation Checklist: http://www.ahima.org/downloads/pdfs/resources/checklist.pdf Is your EMR charting accurately: http://www.emrandhipaa.com/james/2013/08/23/is-your-emr-charting- accurately/?utm_source=feedburner&utm_medium=feed&utm_campaign=Feed%3A+EmrAndHipaa+%28EMR+an d+HIPAA%29 Key Things You Need to Do With Your EHR in Coming Months: http://www.medscape.com/viewarticle/808891 Majority of hospitals, docs have received EHR incentives: Majority of hospitals, docs have received EHR incentives Vital Signs The healthcare business blog from Modern Healthcare http://www.modernhealthcare.com/article/20130729/blog/307299995#ixzz2cSQbVayM?trk=tynt Managing Copy Functionality and Information Integrity in the EHR: http://library.ahima.org/xpedio/groups/public/documents/ahima/bok1_049377.hcsp?dDocName=bok1_049377 MGMA anticipates problems, disruptions with ICD-10: Q&A: http://ehrintelligence.com/2013/07/30/mgma- anticipates-problems-disruptions-with-icd-10-qa/ Mostashari no more icd-10 extensions: http://www.healthcareitnews.com/news/mostashari-no-more-icd-10- extensions?single-page=true Patient access to physician EHRs helps build loyalty: http://www.amednews.com/article/20130820/business/130829999/8/ Pocket Quick Guide Comparison Stage 1 to Stage 2: http://www.advisory.com/Research/IT-Strategy- Council/Resources/2012/Meaningful-Use-Pocket-Guide Problem list guidance in the ehr: http://library.ahima.org/xpedio/groups/public/documents/ahima/bok1_049241.hcsp?dDocName=bok1_049241 Problem List Guidance in the EHR: http://library.ahima.org/xpedio/groups/public/documents/ahima/bok1_049241.hcsp?dDocName=bok1_049241
documentation: http://www.kevinmd.com/blog/2013/01/protect-fraudulent- ehr-documentation.html Providers Behind On ICD-10 Testing: http://www.healthcaretechnologyonline.com/doc/providers-behind-on-icd-10- testing-0001 Readers Write: A Balanced EHR Copy Forward Solution: http://histalk2.com/2013/03/13/readers-write-a-balanced- ehr-copy-forward-solution/ Report: Nearly 50% of EHR Vendors Unresponsive About ICD-10 Implementation: http://www.beckershospitalreview.com/racs-/-icd-9-/-icd-10/report-nearly-50-of-ehr-vendors-unresponsive-about- icd-10-implementation.html Sloppy and paste: http://www.amednews.com/article/20130204/profession/130209993/2/ Stage 1 vs. Stage 2 Comparison Table for Eligible Professionals: https://www.cms.gov/Regulations-and- Guidance/Legislation/EHRIncentivePrograms/downloads/Stage1vsStage2CompTablesforEP.pdf Stage 2 changes may be rude awakening: http://www.healthcareitnews.com/news/stage-2-changes-could-be-rude- awakening Survey: 75% of providers haven’t started ICD-10 testing: http://ehrintelligence.com/2013/08/01/survey-75-of- providers-haven%E2%80%99t-started-icd-10-testing/ The EHR billing controversy: should you worry: http://www.poweryourpractice.com/electronic-health-records/the- ehr-billing-controversy-should-you-worry/ The EHR Honeymoon Is Over: http://www.healthcaretechnologyonline.com/doc/the-ehr-honeymoon-is-over-0001 Top ten ICD-10 readiness questions to ask your vendors: http://ehrintelligence.com/2013/07/10/top-ten-icd-10- readiness-questions-to-ask-your-vendors/ What to expect from EHR vendors during the ICD-10 transition: http://www.icd10watch.com/blog/what-expect-ehr- vendors-during-icd-10-transition When is EHR cloning acceptable?: http://medicaleconomics.modernmedicine.com/medical- economics/news/modernmedicine/modern-medicine-now/when-ehr-cloning-acceptable Why your EHR note may not be accurate: http://www.kevinmd.com/blog/2011/12/ehr-note-accurate.html/ Your EHR Works As Designed, And That’s The Problem: http://healthsystemcio.com/2011/12/28/your-ehr-works- as-designed-and-thats-the-problem/
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}