Your Complete Denture Success and the Important Consultation/Examination Appointment Clarifying the Fundamentals of Complete Denture Fabrication This course will be presented in 5 modules 6 Presenter: M. Leif Stromberg, DDS, MAGD
your success with all tissue-supported edentulous restorations by learning and implementing KEYS to complete denture SUCCESS. • Traditionally fabricated tissue-supported complete dentures. • Digitally fabricated tissue-supported complete dentures. • Implant-retained removable tissue-supported complete dentures, e.g., overdentures with snap-on Locator Attachments. These Keys will increase your success with the following
presenter declares that neither he nor his immediate family have a financial interest that would create a conflict of interest that would influence or restrict his independent judgment with regard to the content of this course.
dentistry in Dallas, Texas. 2. Eight months after graduation, I began studying occlusal reconstruction with Dr. L. D. Pankey. 3. I also studied denture fabrication with leaders in that area of dentistry. 4. I studied with one of the complete denture masters, Dr. Earl Pound. His techniques helped me very much. 5. I successfully implemented Dr. Pound’s techniques into my practice and later taught and wrote a textbook on Dr. Pound’s advanced complete denture systems. 6. I have developed a system for fabricating complete dentures successfully and e ff ectively, and I look forward to sharing this system with you and helping you with your complete denture services. Dr. Leif Stromberg - I want to share my story with you brie y: 14
and implement these Keys to predictability and success with complete dentures. Also, Centric Lab is ready to help you, so please ask us if we can help you. • Centric Lab has helped me on my journey through the years. • I hope we can bring greater pleasure to your life.
1 — PARTICIPANTS WILL BE ABLE TO DISCUSS: 1. It is very important that all denture fabrication steps be done competently by the dentist, dental assistant, and dental lab technician to create well- made complete dentures that (1) are stable, (2) have good occlusal vertical dimension, retention, and esthetics (relative to the patient’s anatomy), and (3) all posterior teeth contact evenly in centric relation occlusion. 2. Sometimes, denture fabrication results are adequate, and the patient still rejects the dentures. 3. FUNDAMENTAL components of the consultation/examination appointment for the edentulous patient and how to decide if you want to treat or refer the case. 16
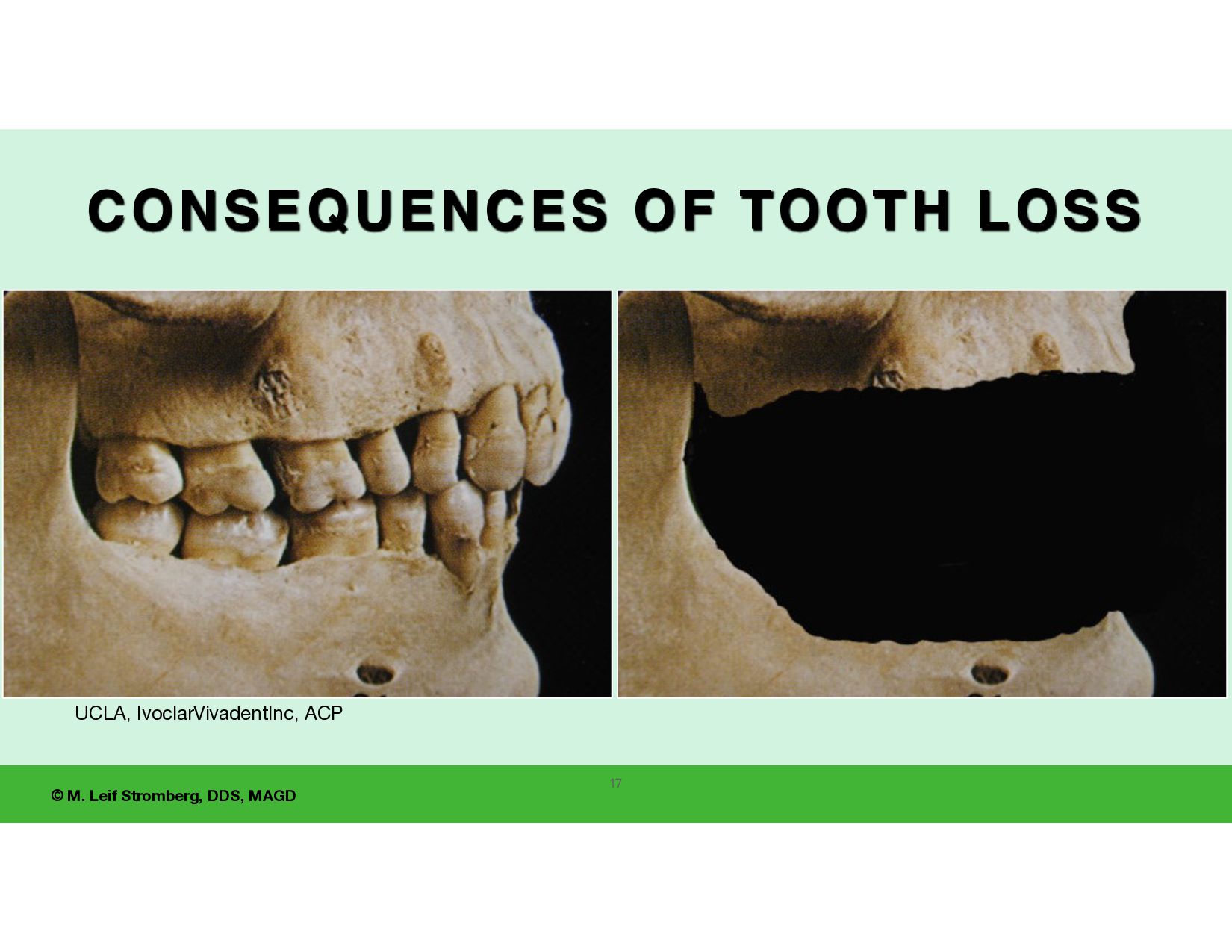
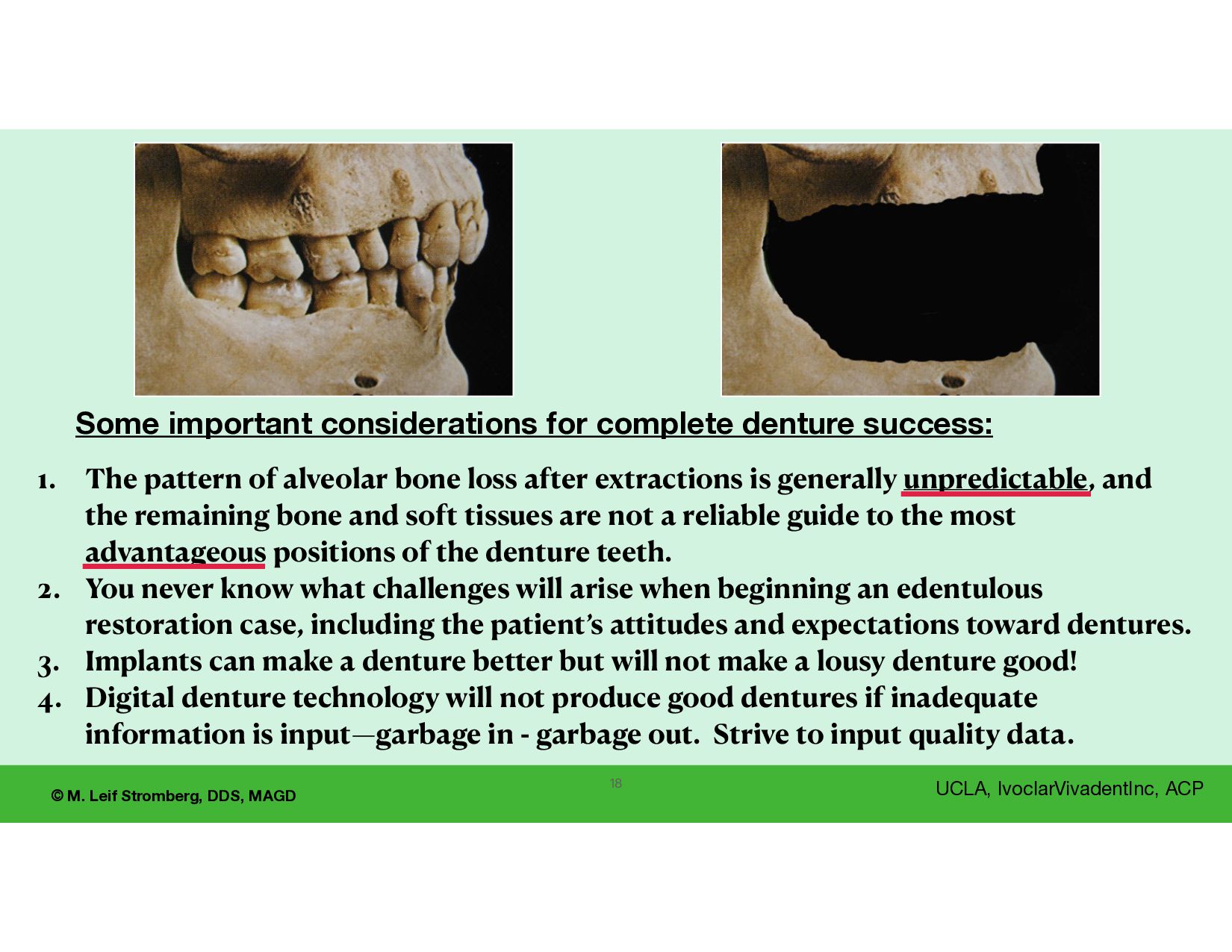
1. The pattern of alveolar bone loss after extractions is generally unpredictable, and the remaining bone and soft tissues are not a reliable guide to the most advantageous positions of the denture teeth. 2. You never know what challenges will arise when beginning an edentulous restoration case, including the patient’s attitudes and expectations toward dentures. 3. Implants can make a denture better but will not make a lousy denture good! 4. Digital denture technology will not produce good dentures if inadequate information is input—garbage in - garbage out. Strive to input quality data. Some important considerations for complete denture success:
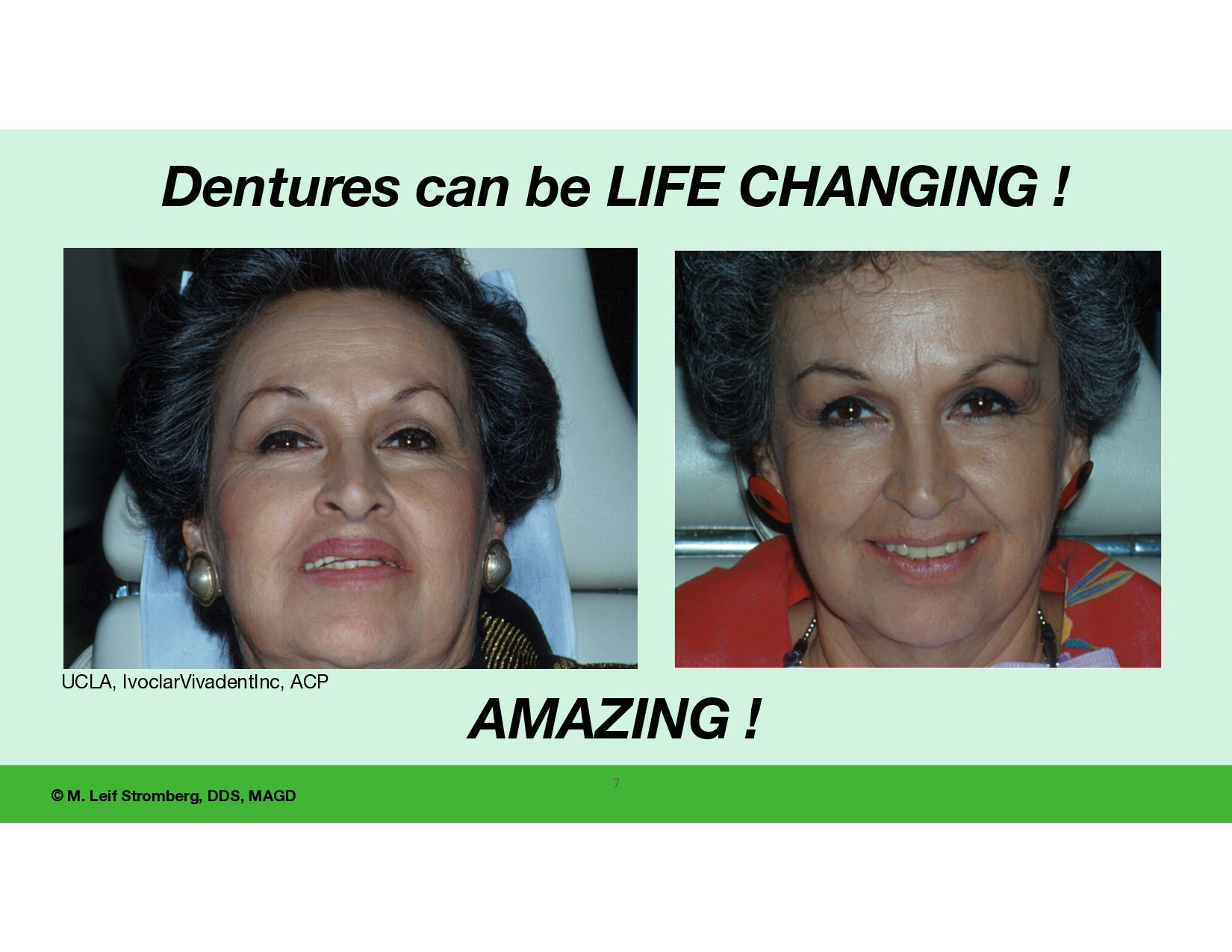
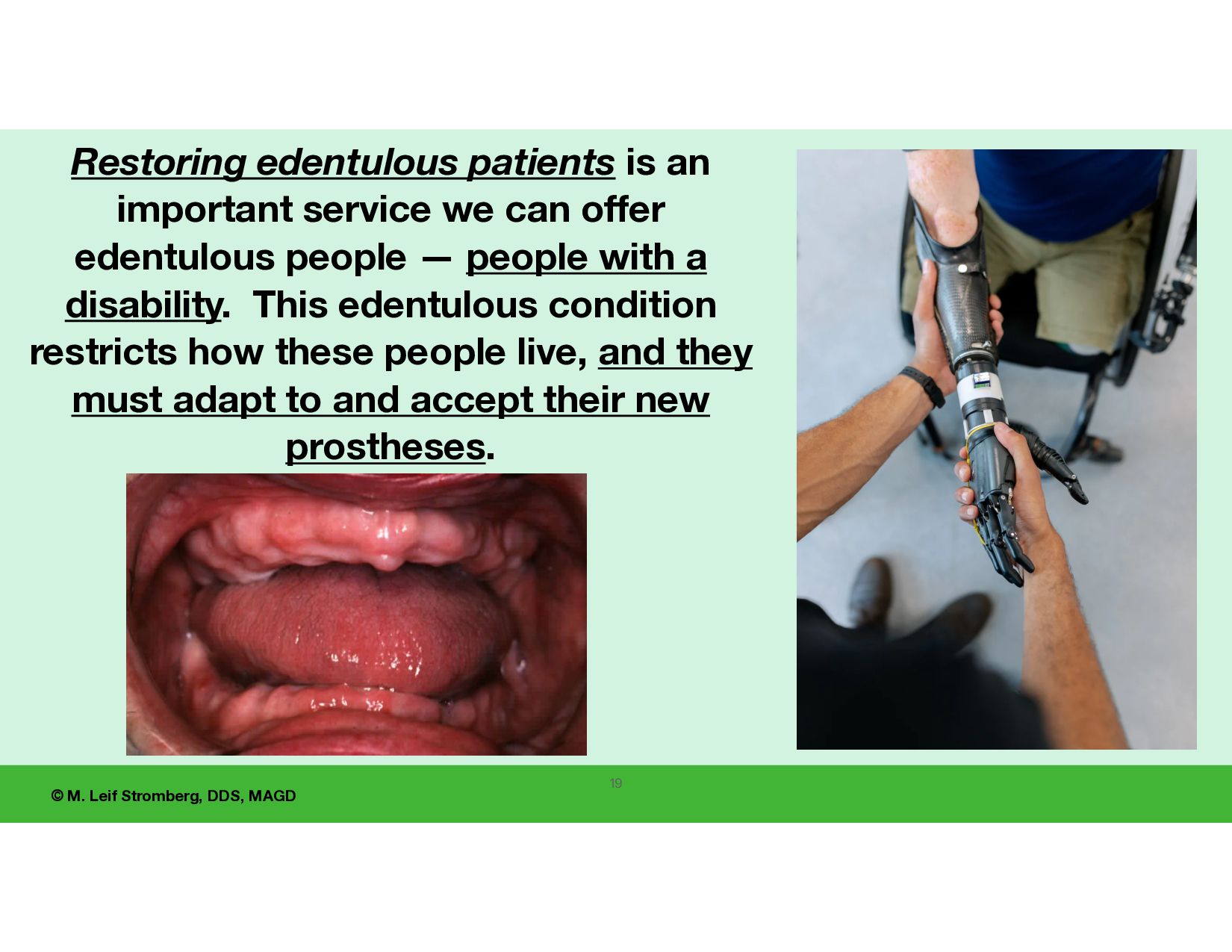
is an important service we can offer edentulous people — people with a disability. This edentulous condition restricts how these people live, and they must adapt to and accept their new prostheses.
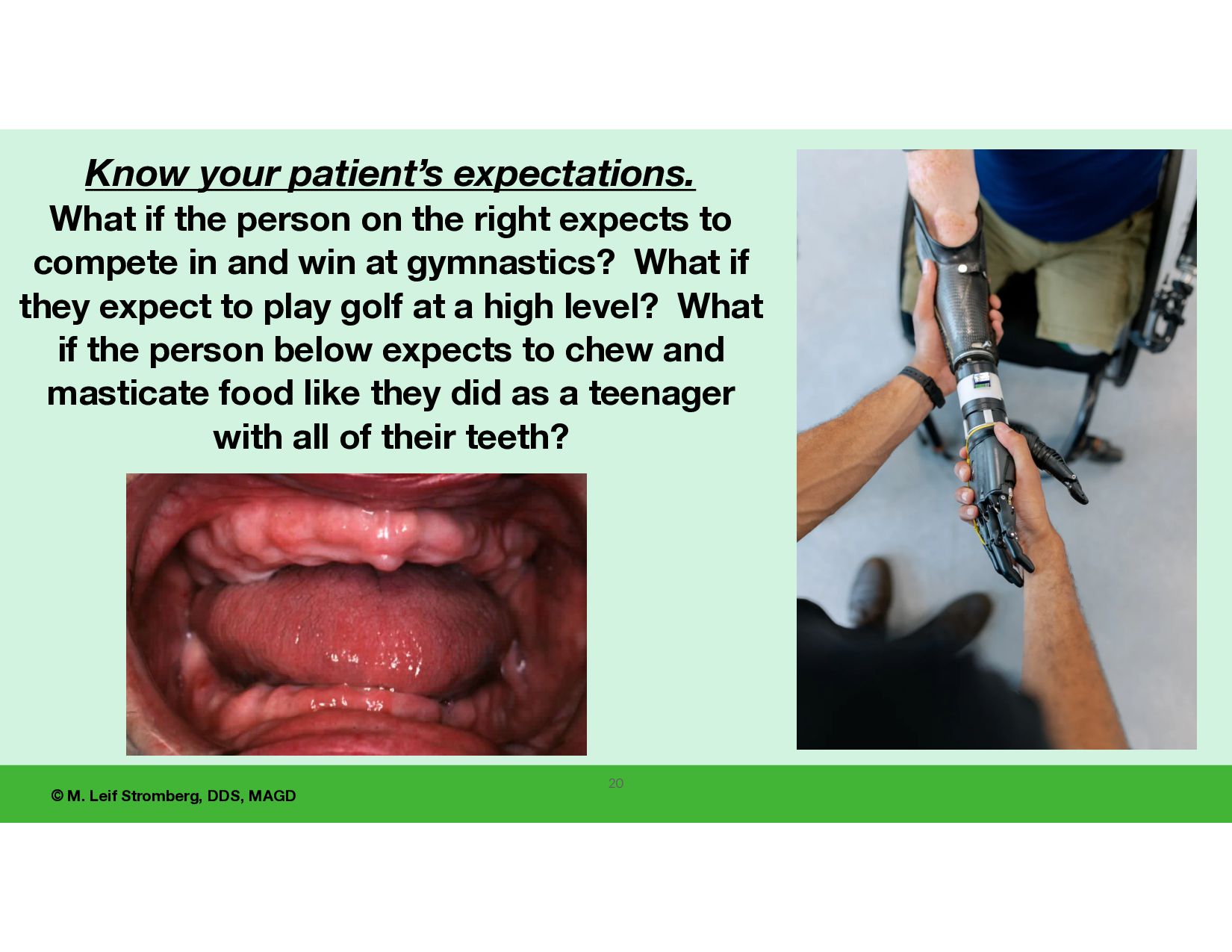
expectations. What if the person on the right expects to compete in and win at gymnastics? What if they expect to play golf at a high level? What if the person below expects to chew and masticate food like they did as a teenager with all of their teeth?
the dentist and team to 1. Understand and accept the limitations and unpredictability of the denture fabrication process. 2. Let fear and anger go. 3. Become more e ff ective and successful in treating edentulous patients (and I will show you a better way). 22
to fabricate complete dentures unpredictably and unsuccessfully. I will show you a much better way !! Key Point! 23 I hope to motivate and encourage you to continue learning and growing. UCLA, IvoclarVivadentInc, ACP
your success with all tissue-supported edentulous restorations by learning and implementing KEYS, FUNDAMENTALS to complete denture SUCCESS. This program teaches the fundamentals of complete denture fabrication. Being on a path to learning a sport, such as tennis or football, fi rst, the fundamentals are taught by the COACH, are learned and implemented by the athlete before adding advanced techniques. … The same goes for denture fabrication.
of complete denture fabrication have been learned and incorporated into practice, 1. many more advanced techniques can be added to your denture service to improve predictability, esthetics, phonetics, occlusion, retention, comfort, TMD treatment, and dental implant services. 2. Also, many steps can be delegated to dental assistants and laboratory technicians.
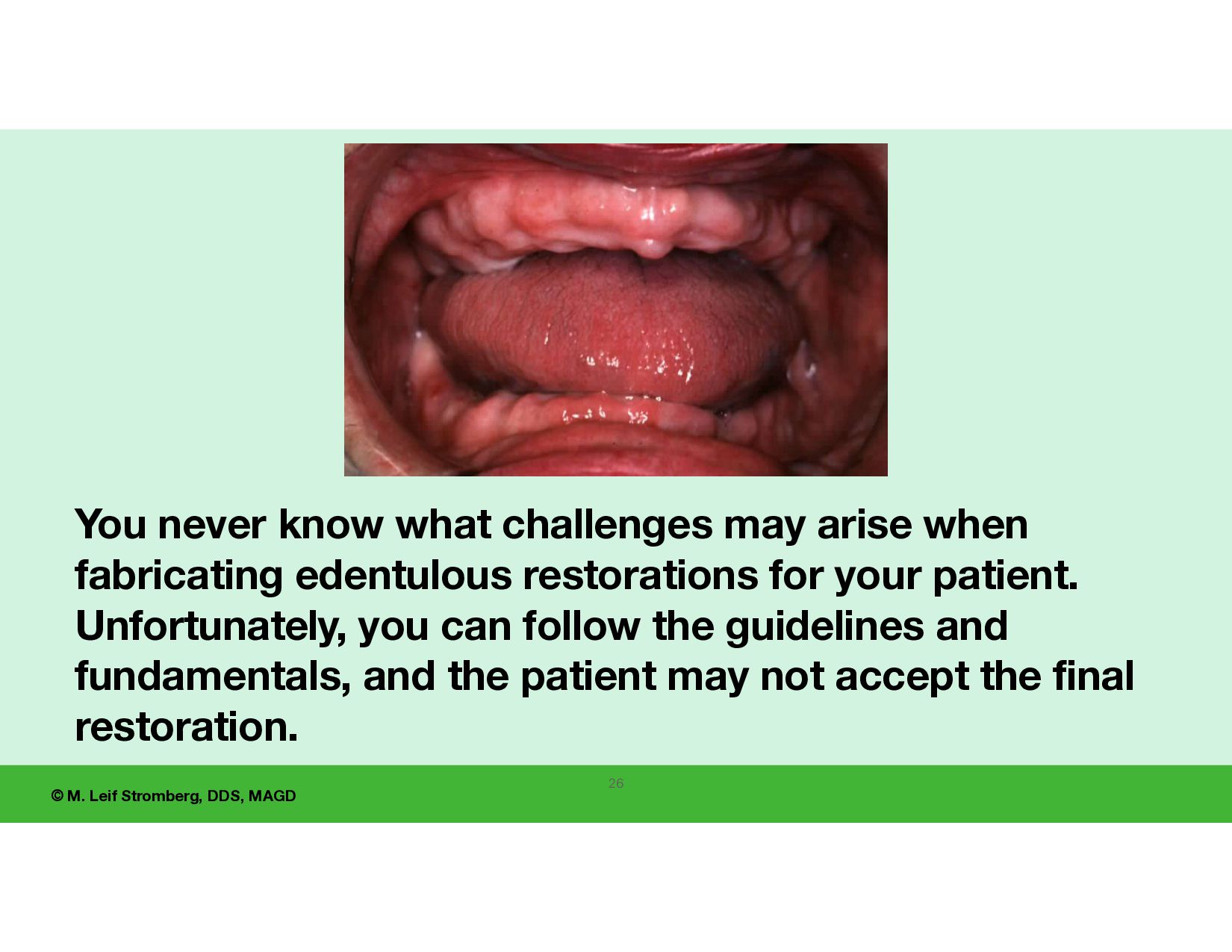
challenges may arise when fabricating edentulous restorations for your patient. Unfortunately, you can follow the guidelines and fundamentals, and the patient may not accept the final restoration. 26
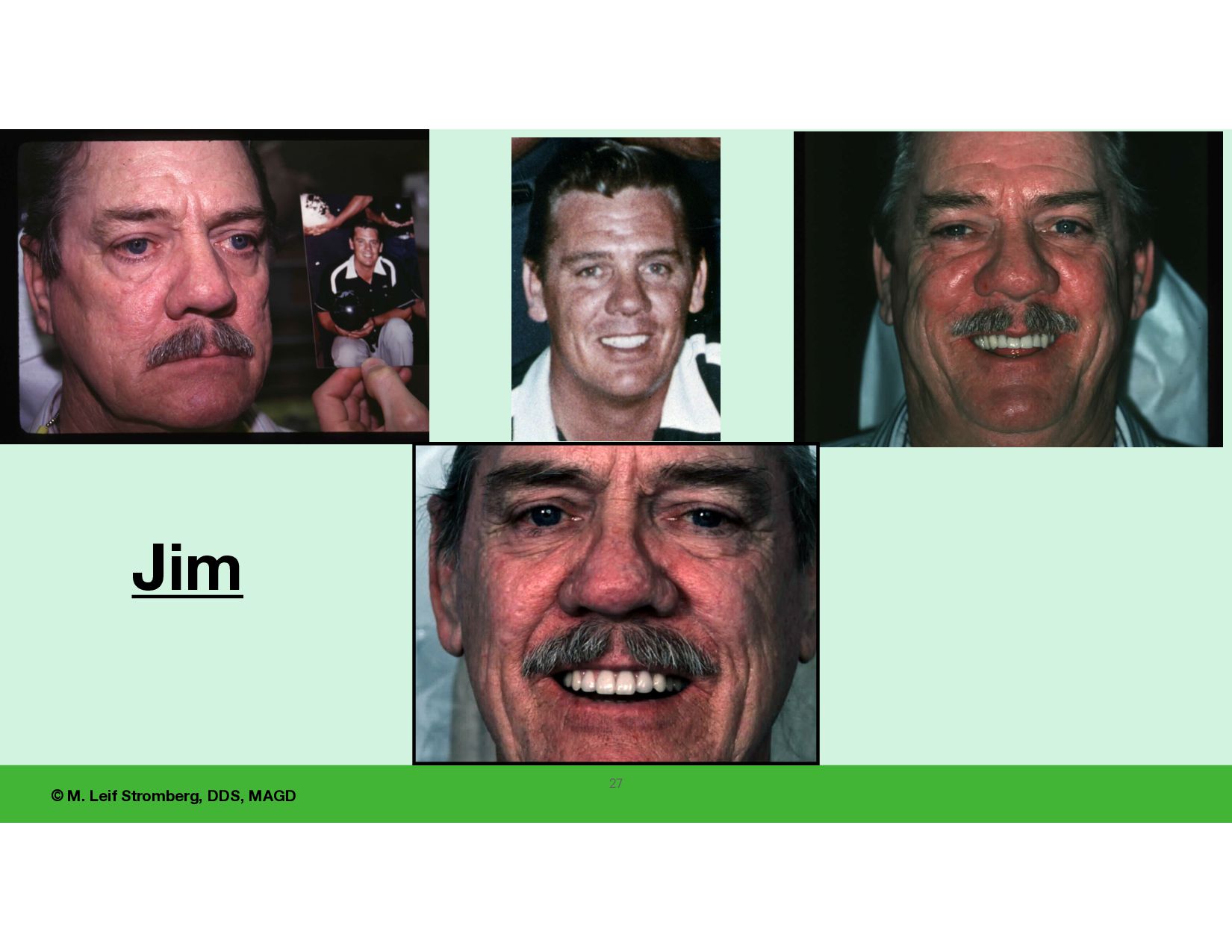
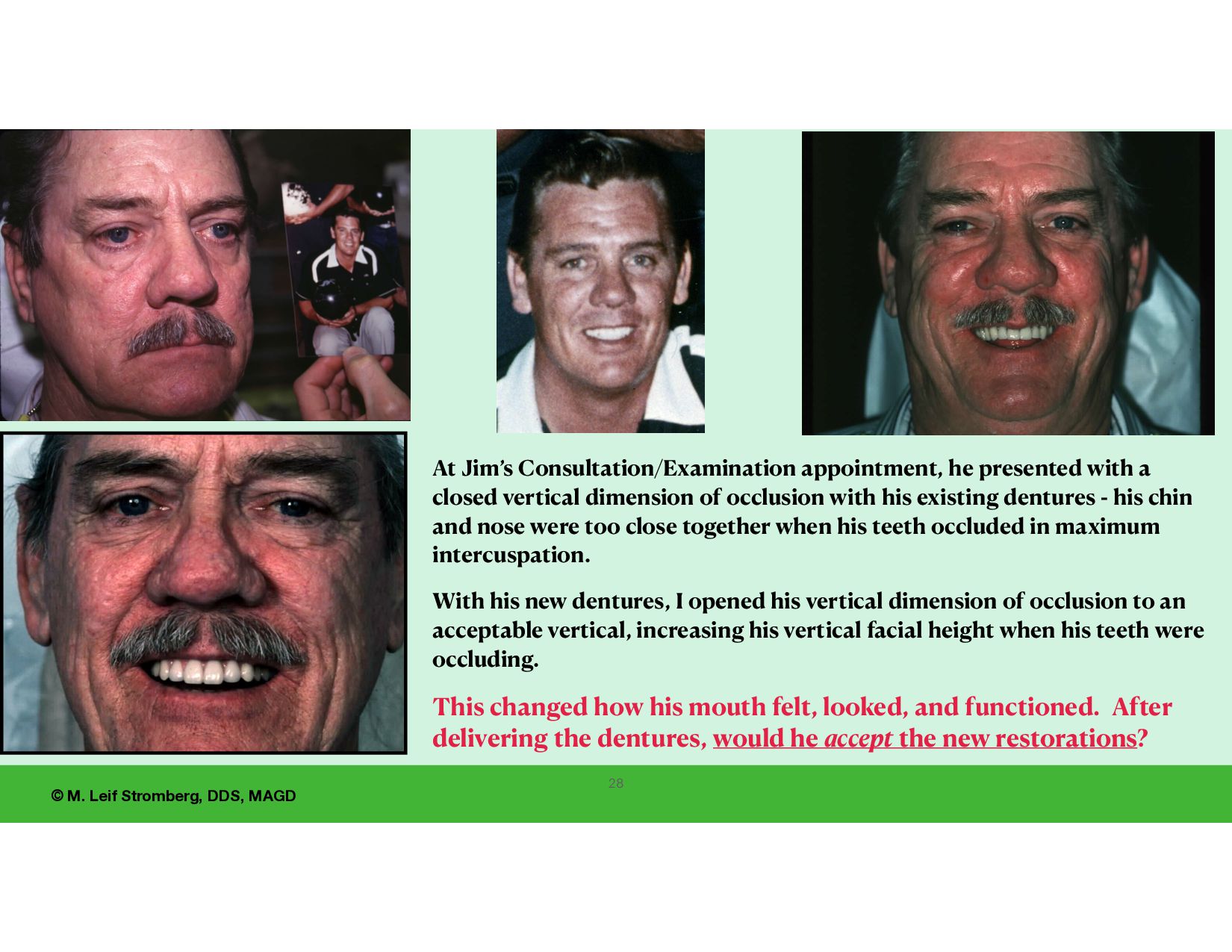
appointment, he presented with a closed vertical dimension of occlusion with his existing dentures - his chin and nose were too close together when his teeth occluded in maximum intercuspation. With his new dentures, I opened his vertical dimension of occlusion to an acceptable vertical, increasing his vertical facial height when his teeth were occluding. This changed how his mouth felt, looked, and functioned. After delivering the dentures, would he accept the new restorations?
Pound Denture Study Group The study club members were all fabricating dentures using the conventional linear denture technique and having the same problems we have today.
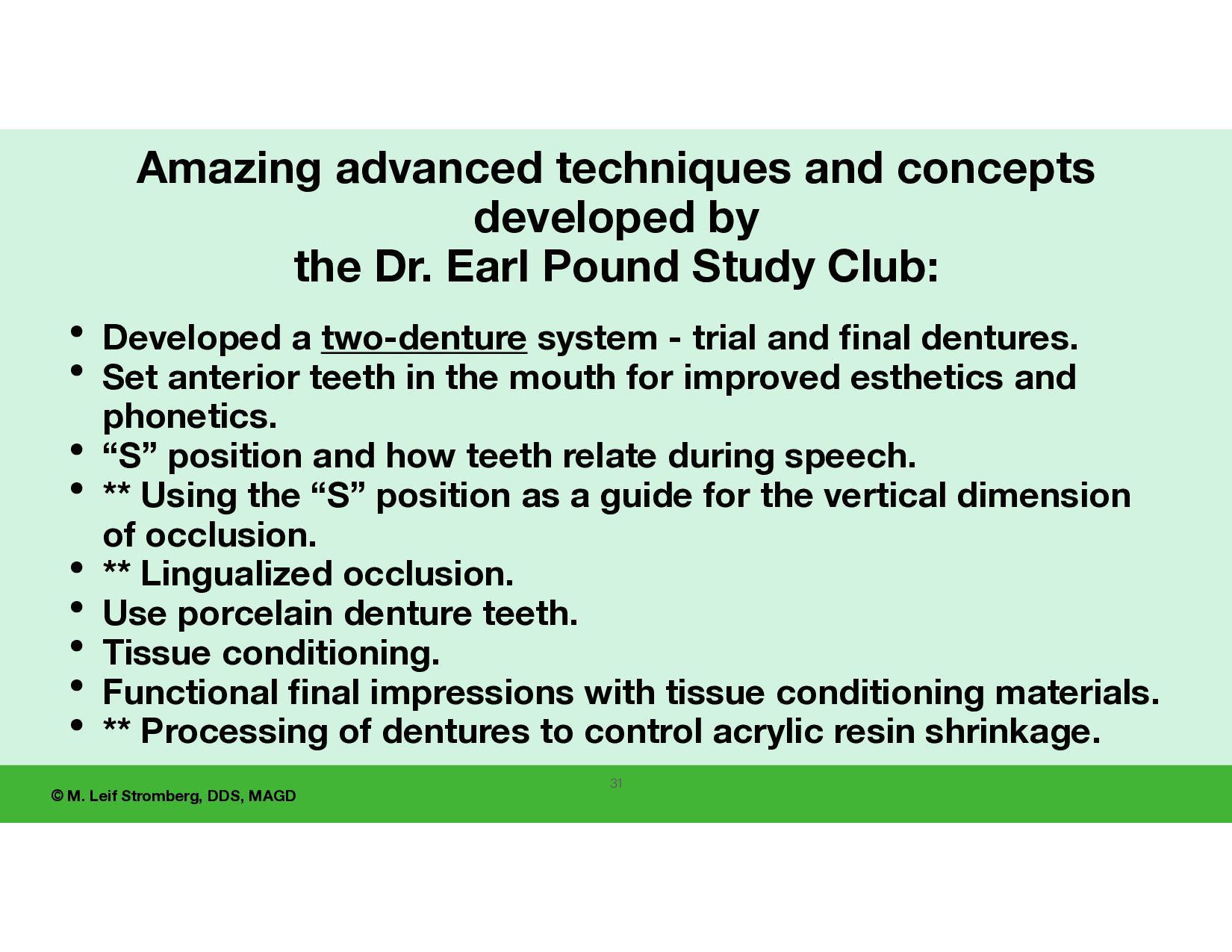
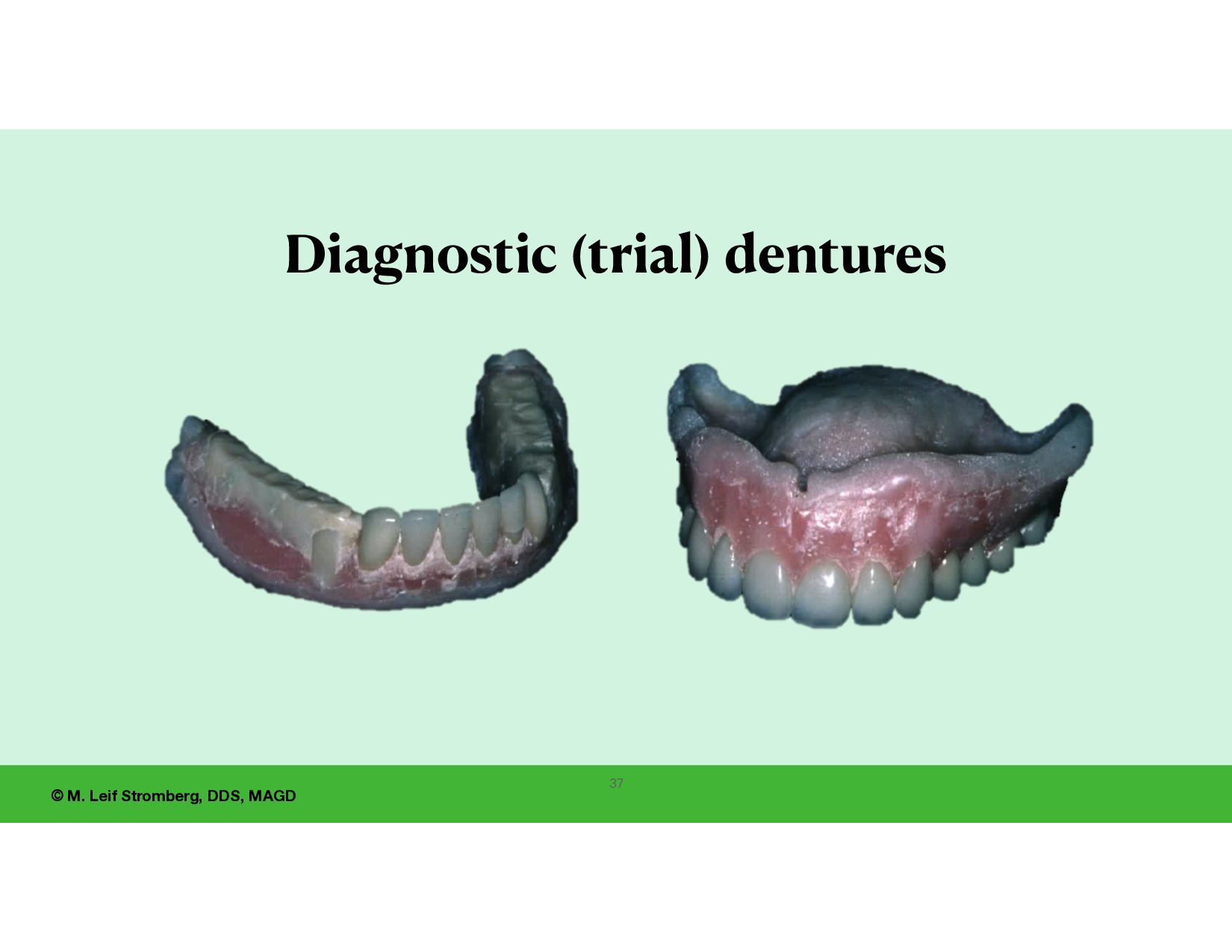
and concepts developed by the Dr. Earl Pound Study Club: • Developed a two-denture system - trial and nal dentures. • Set anterior teeth in the mouth for improved esthetics and phonetics. • “S” position and how teeth relate during speech. • ** Using the “S” position as a guide for the vertical dimension of occlusion. • ** Lingualized occlusion. • Use porcelain denture teeth. • Tissue conditioning. • Functional fi nal impressions with tissue conditioning materials. • ** Processing of dentures to control acrylic resin shrinkage.
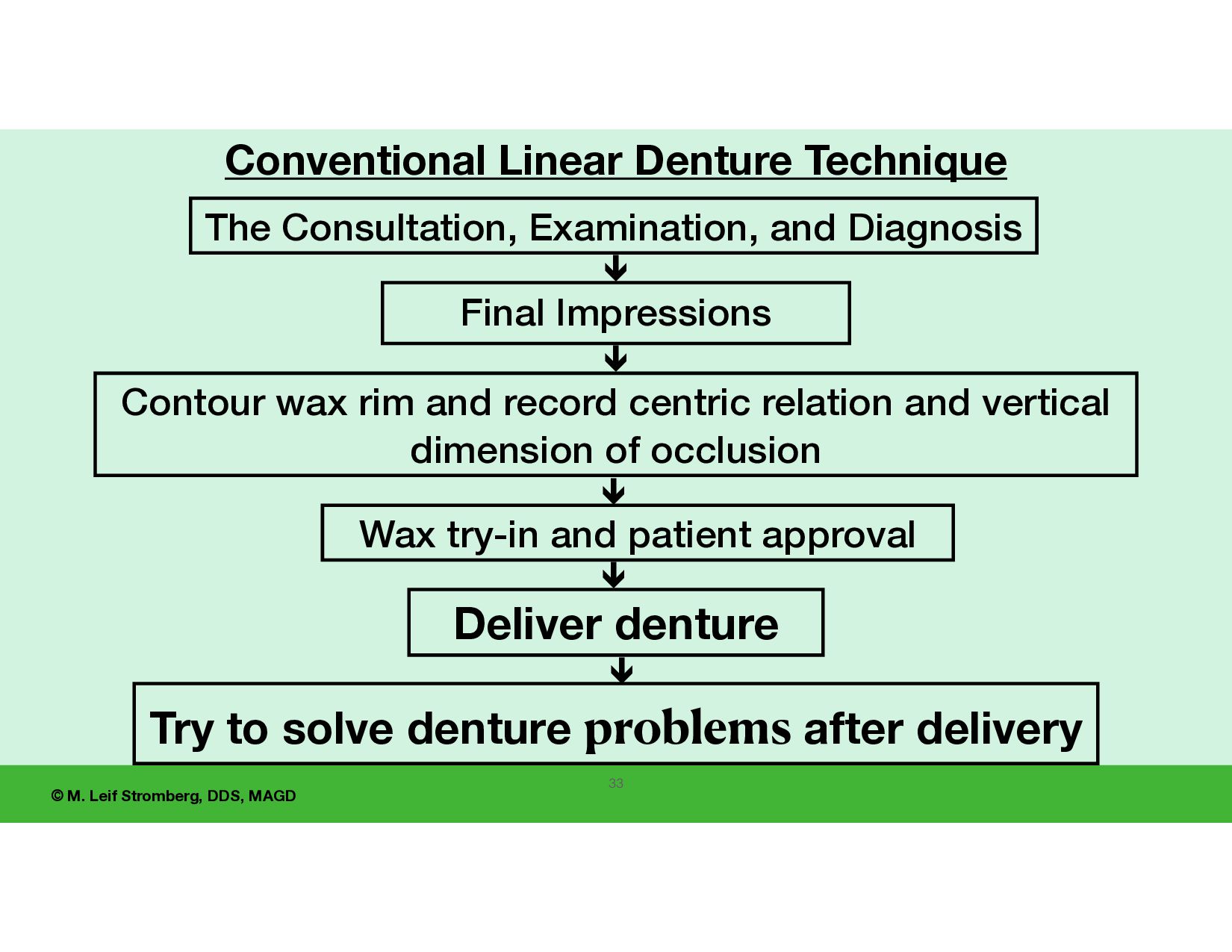
Final Impressions ê Contour wax rim and record centric relation and vertical dimension of occlusion ê Wax try-in and patient approval ê Deliver denture Try to solve denture problems after delivery ê ê The Consultation, Examination, and Diagnosis 33
• Vertical Dimension of Occlusion • Temporomandibular Disorder (TMD) - pain or joint shifts, unstable • Occlusion/Bite • Unhealthy Tissues • Sore areas of tissues under the denture base • Biting cheeks and lips • Comfort, retention, stability • Function Problems - unpredictability Try to solve denture problems after delivery. 34
Design and Technique • Diagnostic (trial) denture • Set anterior teeth in the mouth • Tissue conditioning material • Functional impression • Address problems after delivery of the diagnostic (trial) denture •Aesthetics •Phonetics •Vertical Dimension of Occlusion •TM Disorder •Occlusion/Bite •Unhealthy Tissues •Sore Areas of Tissues under the denture base •Biting cheeks and lips •Comfort, Retention, Stability •Function 36
properly, su ciently, well, but not perfectly. Using the Conventional Linear Denture Technique, if all of the denture fabrication steps are done competently, there will be fewer problems after the delivery of the dentures and greater success.
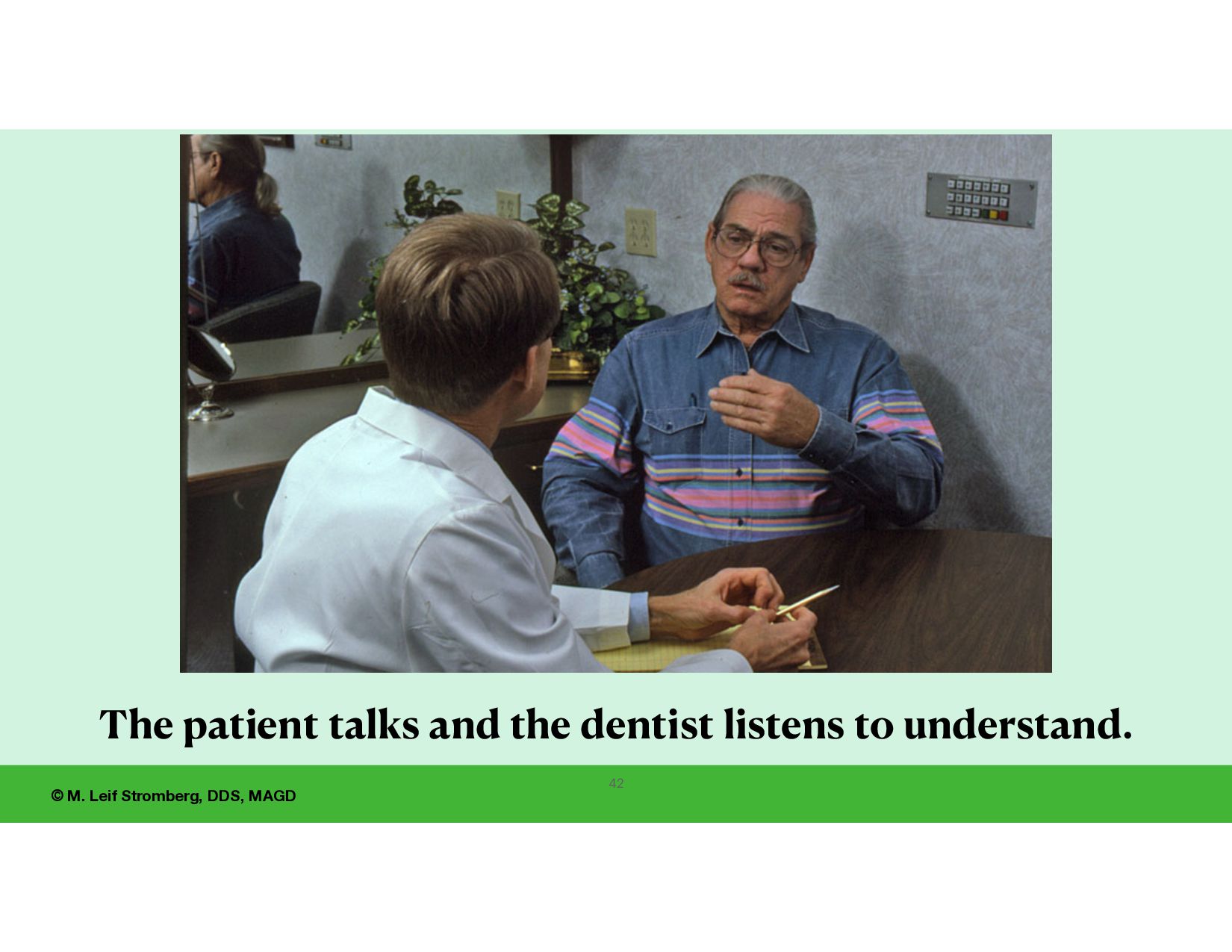
consultation, a pre-clinical interview, before the visual clinical examination. • For increased predictability and success, never treat a stranger. And treat folks you enjoy being with.
the dentist can make with the new patient is to ask: “How can I help you?” Then listen. • Ask your patient to describe the conditions with their existing dentures (esthetics, comfort, retention, function), and discuss their likes and dislikes with past dentures. • Listen with the intent to understand. • Ask about and understand your patient’s wants and expectations with new dentures. 41
wants and expectations. • Show concern, be concerned. • Give feedback so that your patient feels understood. This is important for building trust. • And turn a stranger into a friend. Listen actively and compassionately with curiosity and concern — what is on your patient’s mind? Hopefully, you will gain an understanding of your patient that will help your denture service be more predictable and successful for this patient. 43
understand that the denture problems are theirs, not yours. Say: “I am glad to help you with your denture problems.” or “Can I do a clinical examination to understand your denture problems better?
the patient’s stomatognathic conditions (mouth and jaws) regarding the level of health, pathology, and structural conditions. 2. Can you treat the case predictably, successfully, and e ff ectively (pro fi tably)? Do you want to treat this patient? 3. Identify conditions that may take extra time to address and treat (and possibly be unable to “solve”). 4. For a patient with conditions such as “poor” alveolar ridges or large tori, you may choose only to treat them if dental implants are placed for retention and support. All options should be discussed, but you might o er only to treat the case if the patient has implants placed. 5. There is nothing wrong with referring patients to colleagues. 46
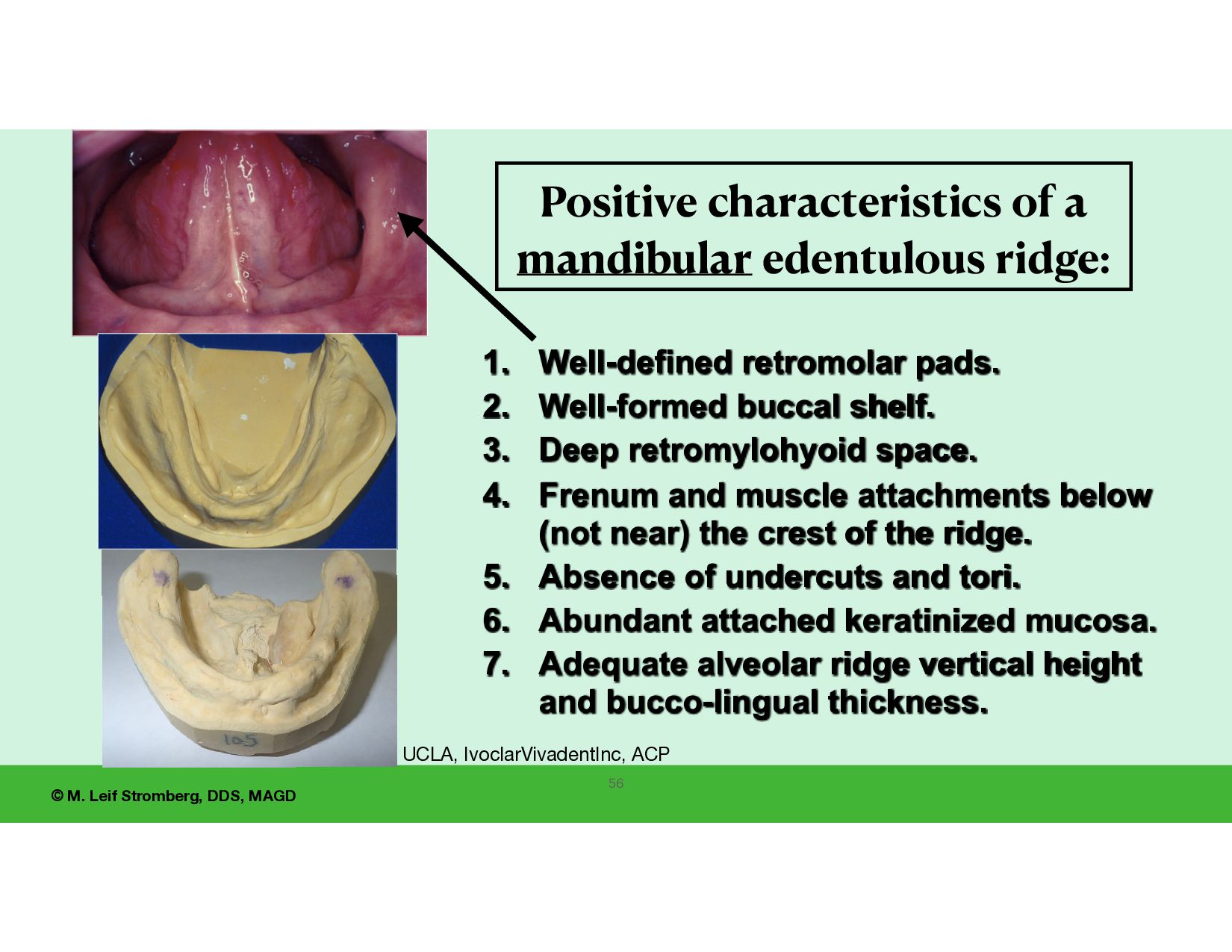
• the form of the edentulous alveolar ridges, tuberosities, and retromolar pads, • mobility of soft tissues of the alveolar ridges, and • the health of the denture-bearing areas. Remember that the patient’s attitude and adaptability are very important regarding predictability and success with tissue-supported complete dentures. Have an examination form so the examination is organized, e cient, and complete - and highlight areas of concern. Report ndings verbally for the assistant to record so the patient hears the ndings. Important Oral Anatomic Features to evaluate regarding predictability and success of tissue-supported complete dentures. 47
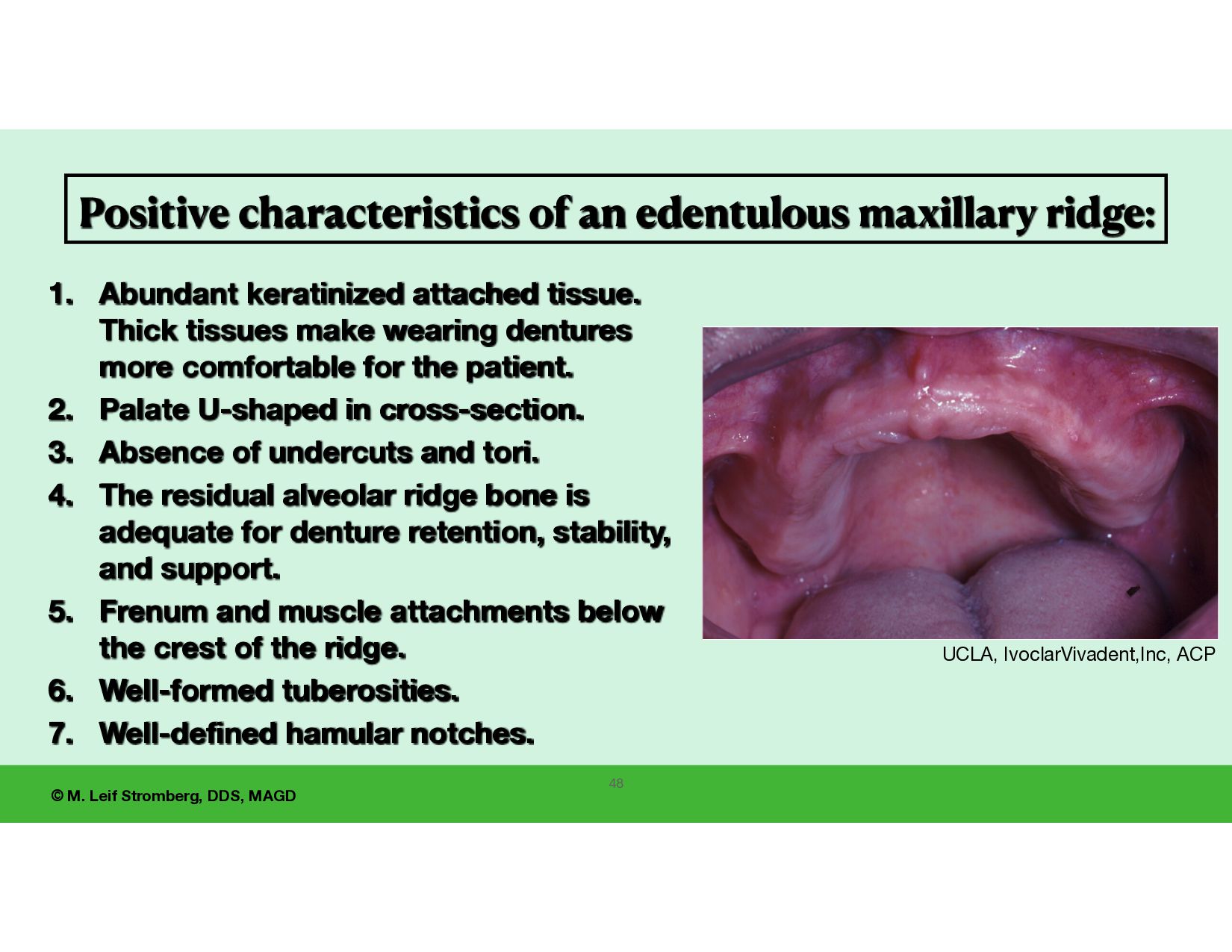
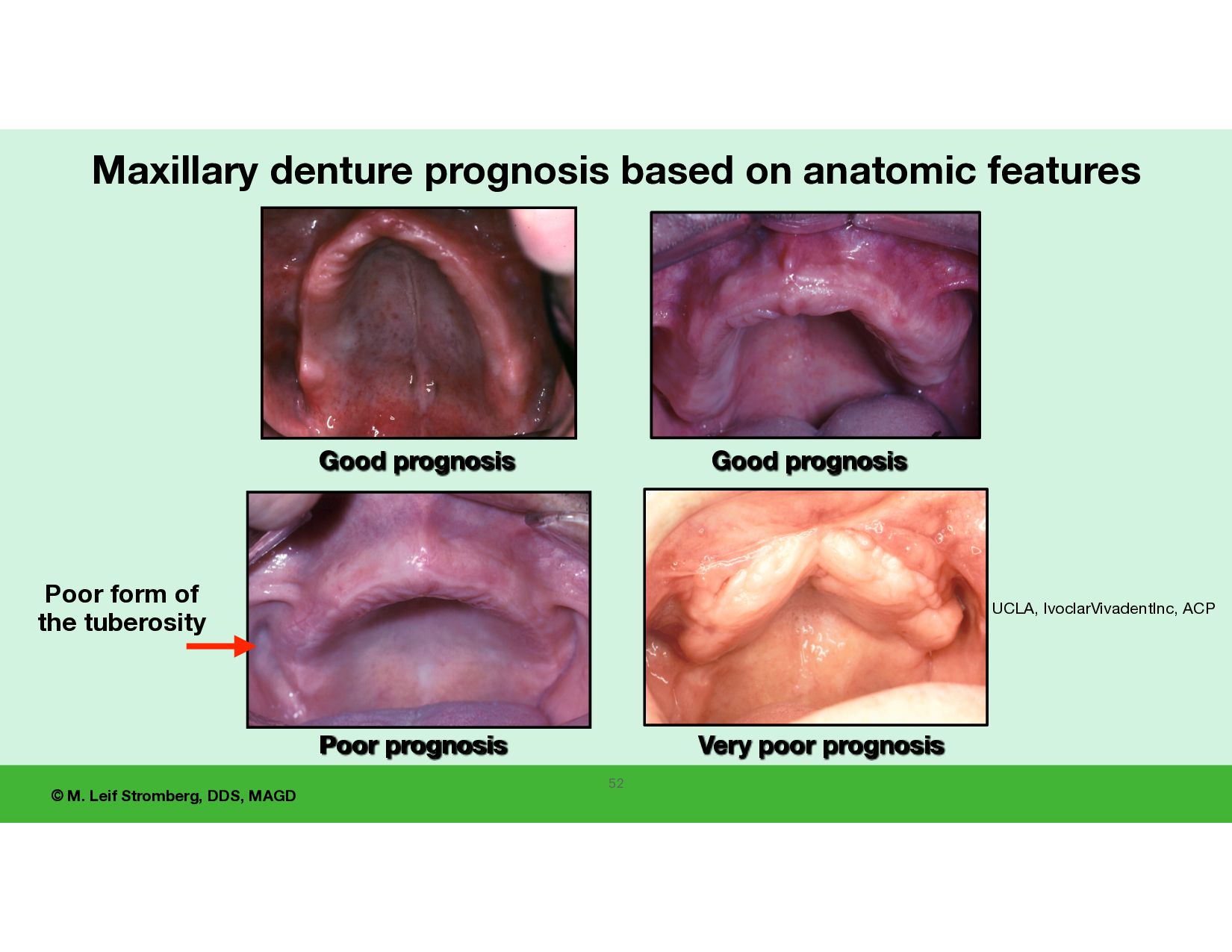
edentulous maxillary ridge: 1. Abundant keratinized attached tissue. Thick tissues make wearing dentures more comfortable for the patient. 2. Palate U-shaped in cross-section. 3. Absence of undercuts and tori. 4. The residual alveolar ridge bone is adequate for denture retention, stability, and support. 5. Frenum and muscle attachments below the crest of the ridge. 6. Well-formed tuberosities. 7. Well-defined hamular notches. UCLA, IvoclarVivadent,Inc, ACP 48
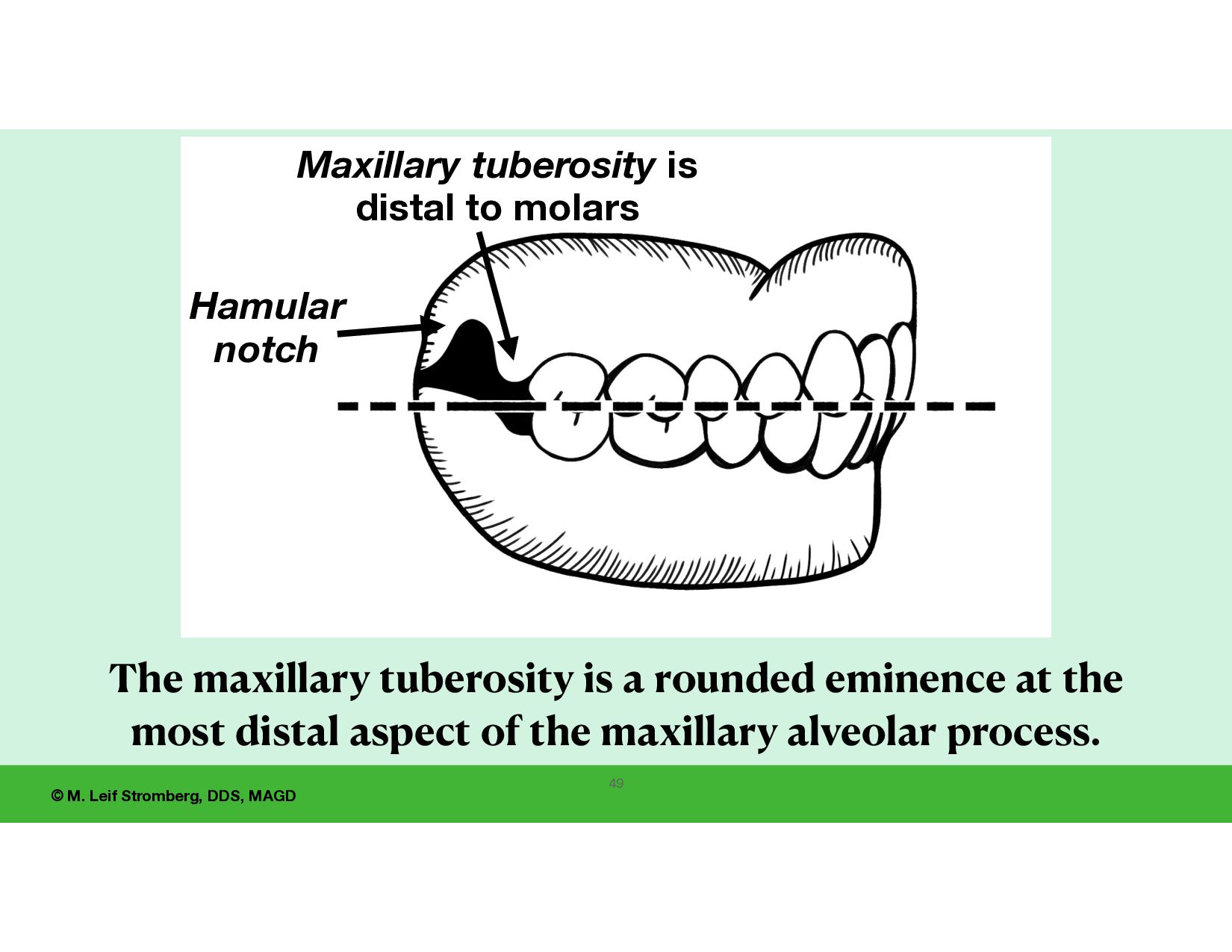
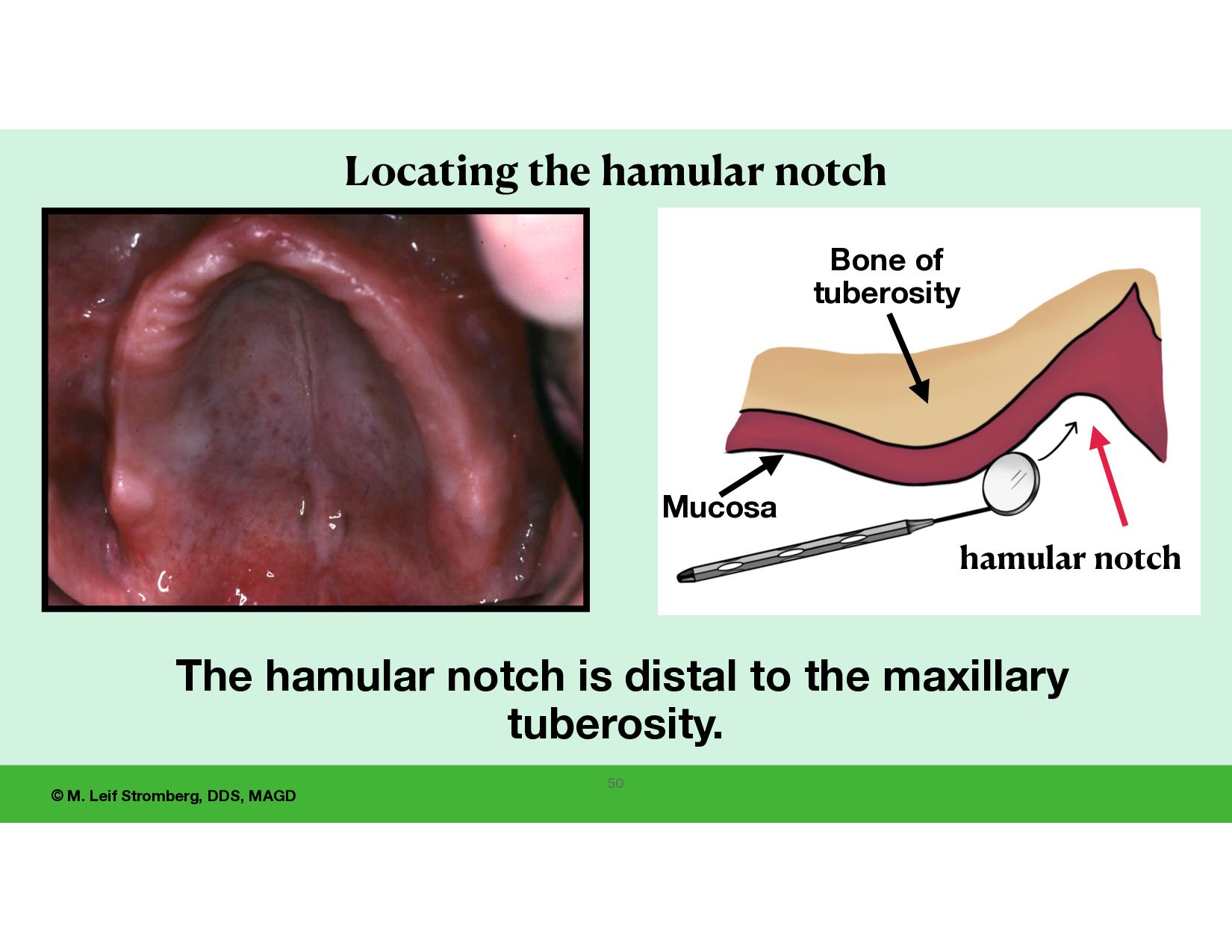
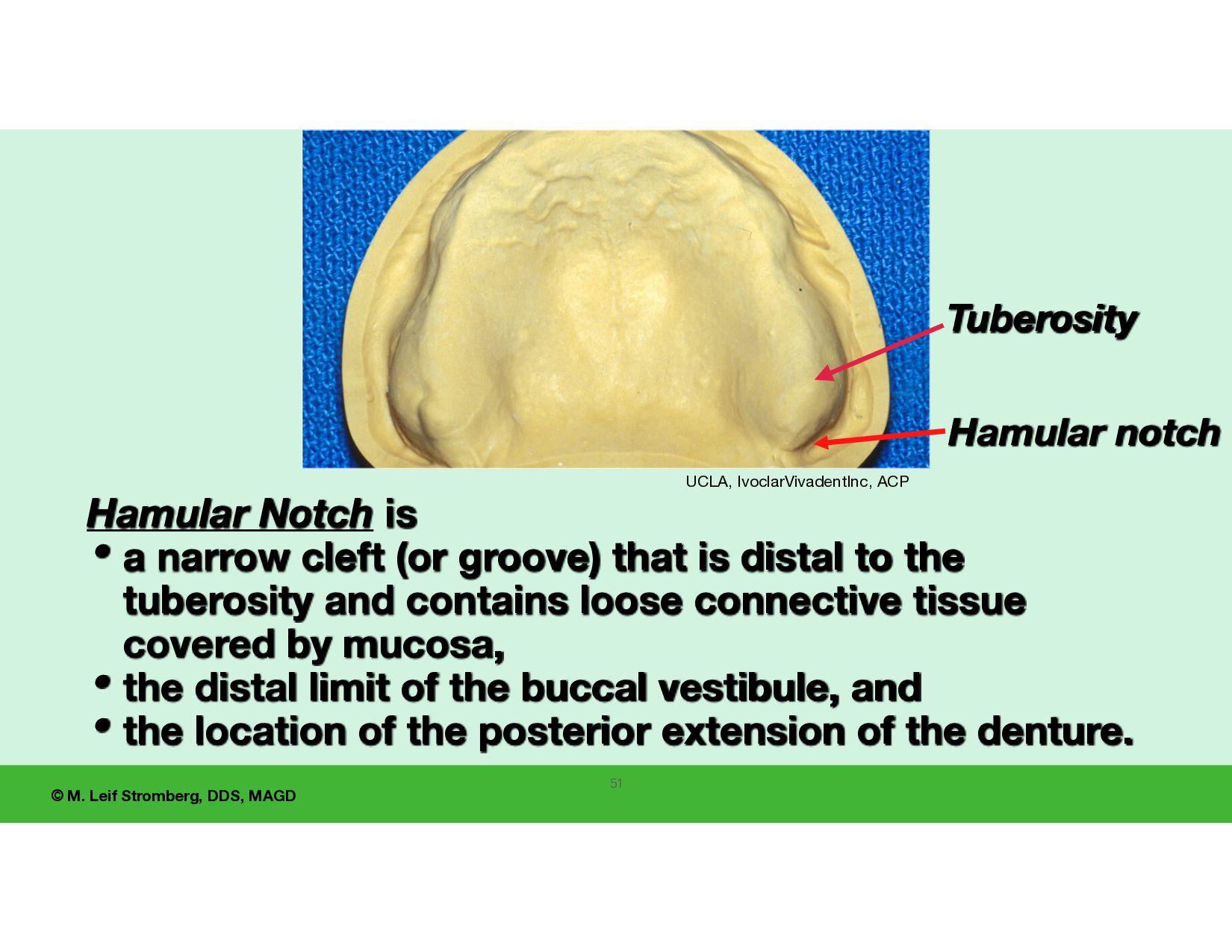
is • a narrow cleft (or groove) that is distal to the tuberosity and contains loose connective tissue covered by mucosa, • the distal limit of the buccal vestibule, and • the location of the posterior extension of the denture. UCLA, IvoclarVivadentInc, ACP Tuberosity 51
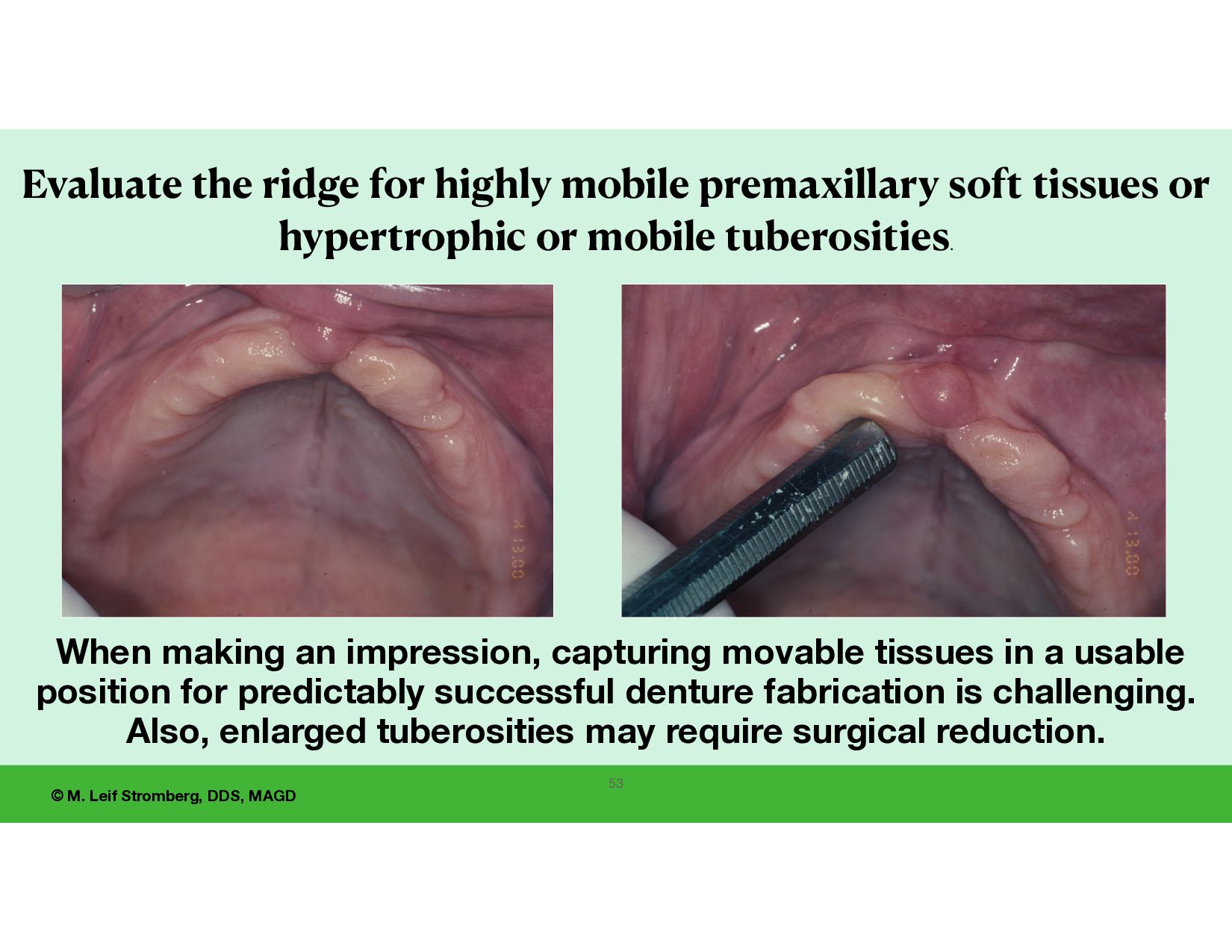
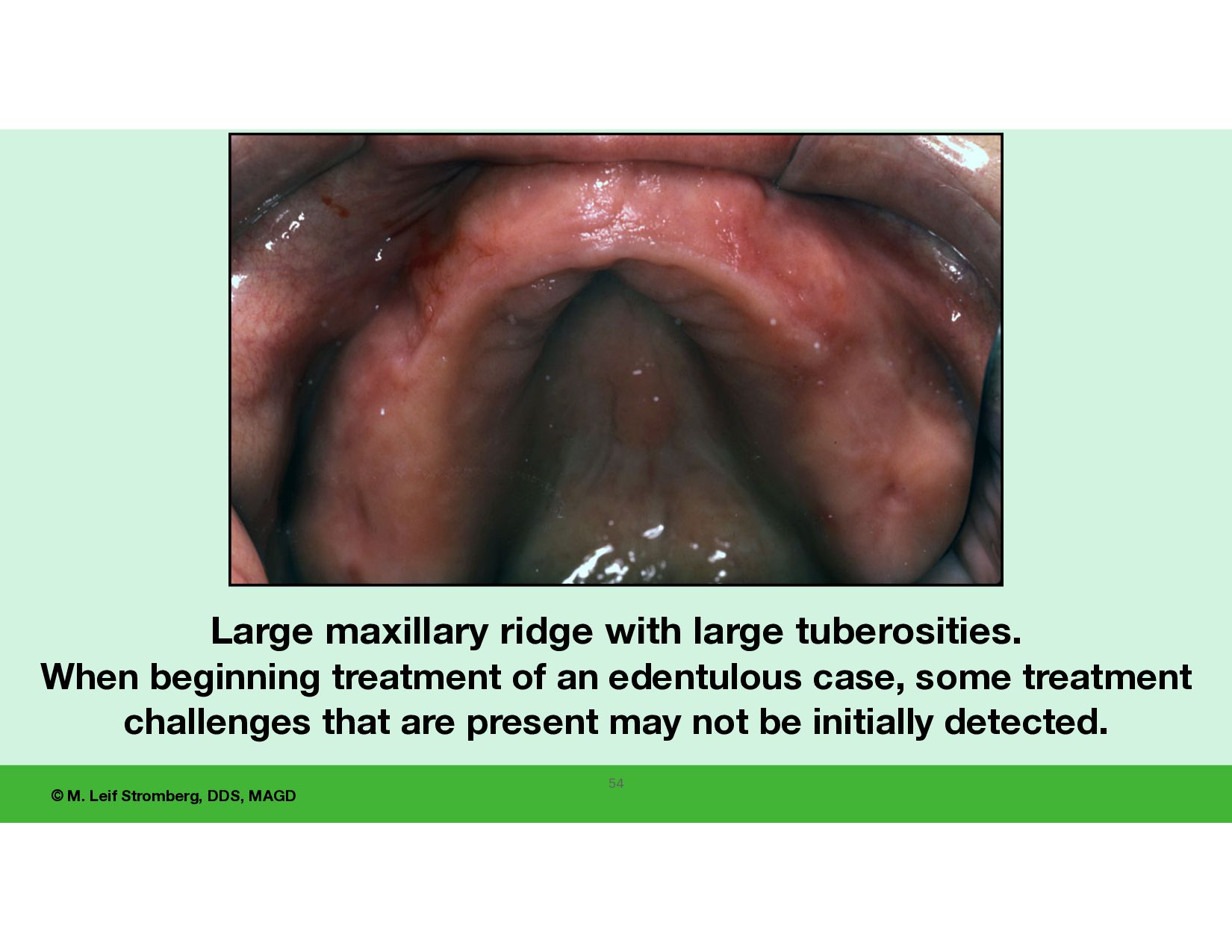
capturing movable tissues in a usable position for predictably successful denture fabrication is challenging. Also, enlarged tuberosities may require surgical reduction. 53 Evaluate the ridge for highly mobile premaxillary soft tissues or hypertrophic or mobile tuberosities.
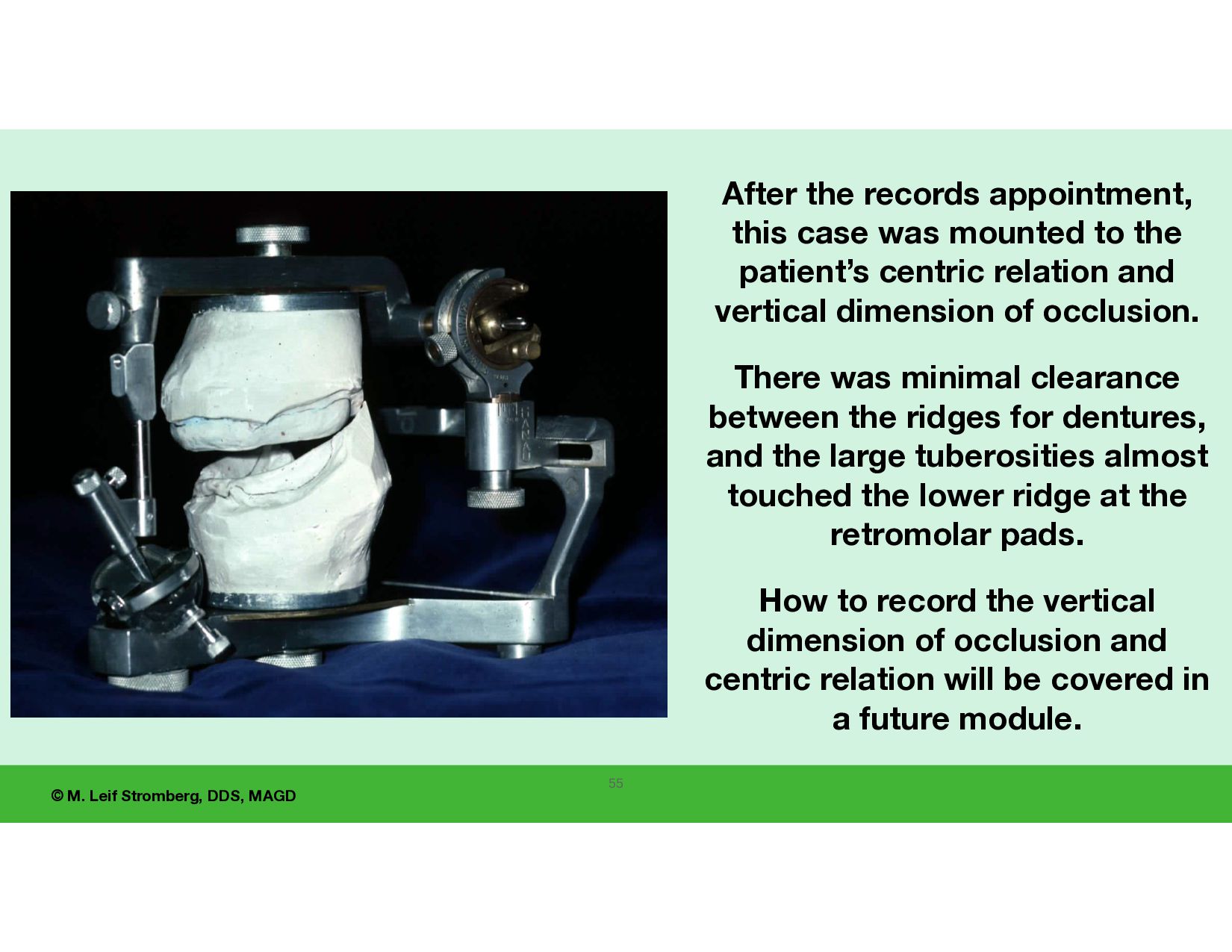
appointment, this case was mounted to the patient’s centric relation and vertical dimension of occlusion. There was minimal clearance between the ridges for dentures, and the large tuberosities almost touched the lower ridge at the retromolar pads. How to record the vertical dimension of occlusion and centric relation will be covered in a future module.
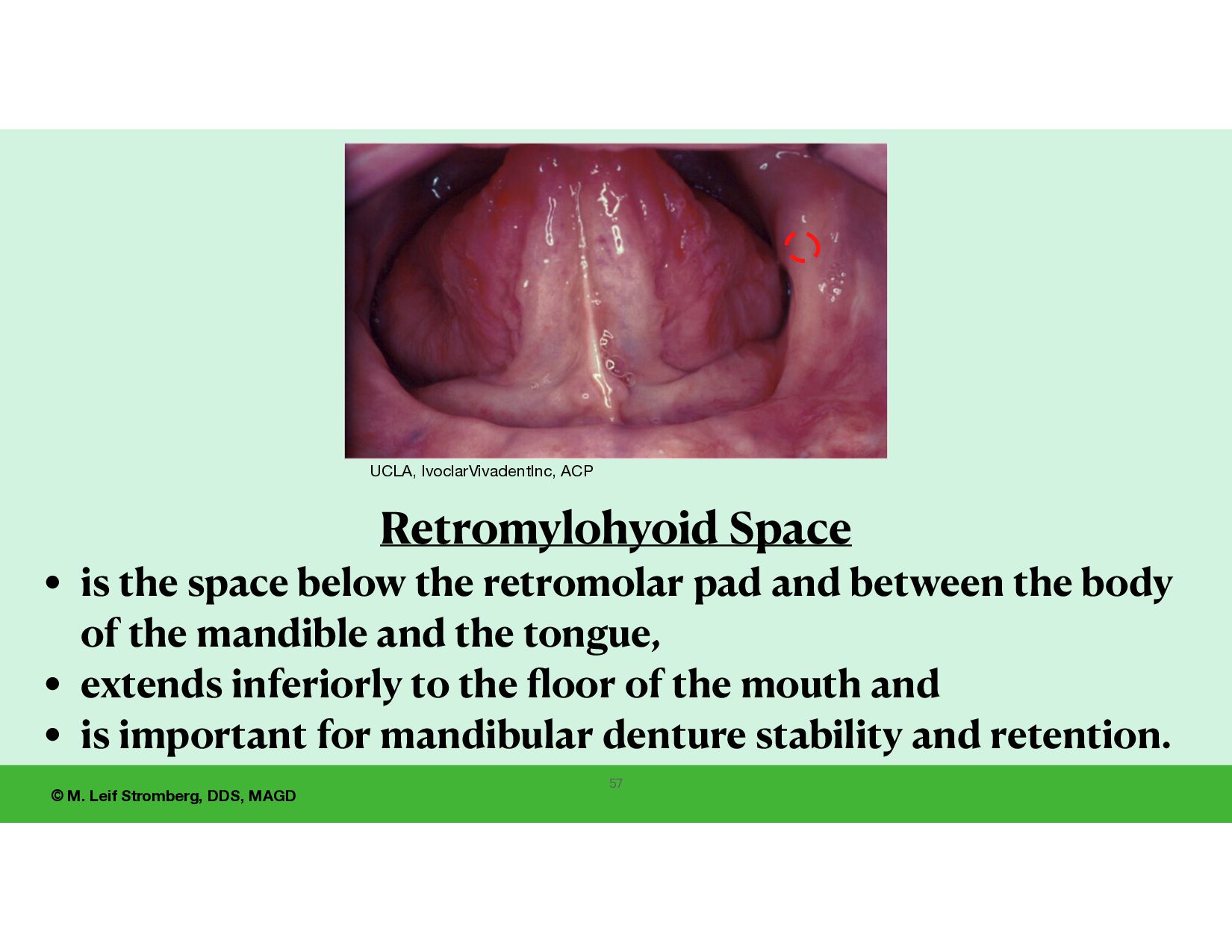
is the space below the retromolar pad and between the body of the mandible and the tongue, • extends inferiorly to the fl oor of the mouth and • is important for mandibular denture stability and retention. UCLA, IvoclarVivadentInc, ACP
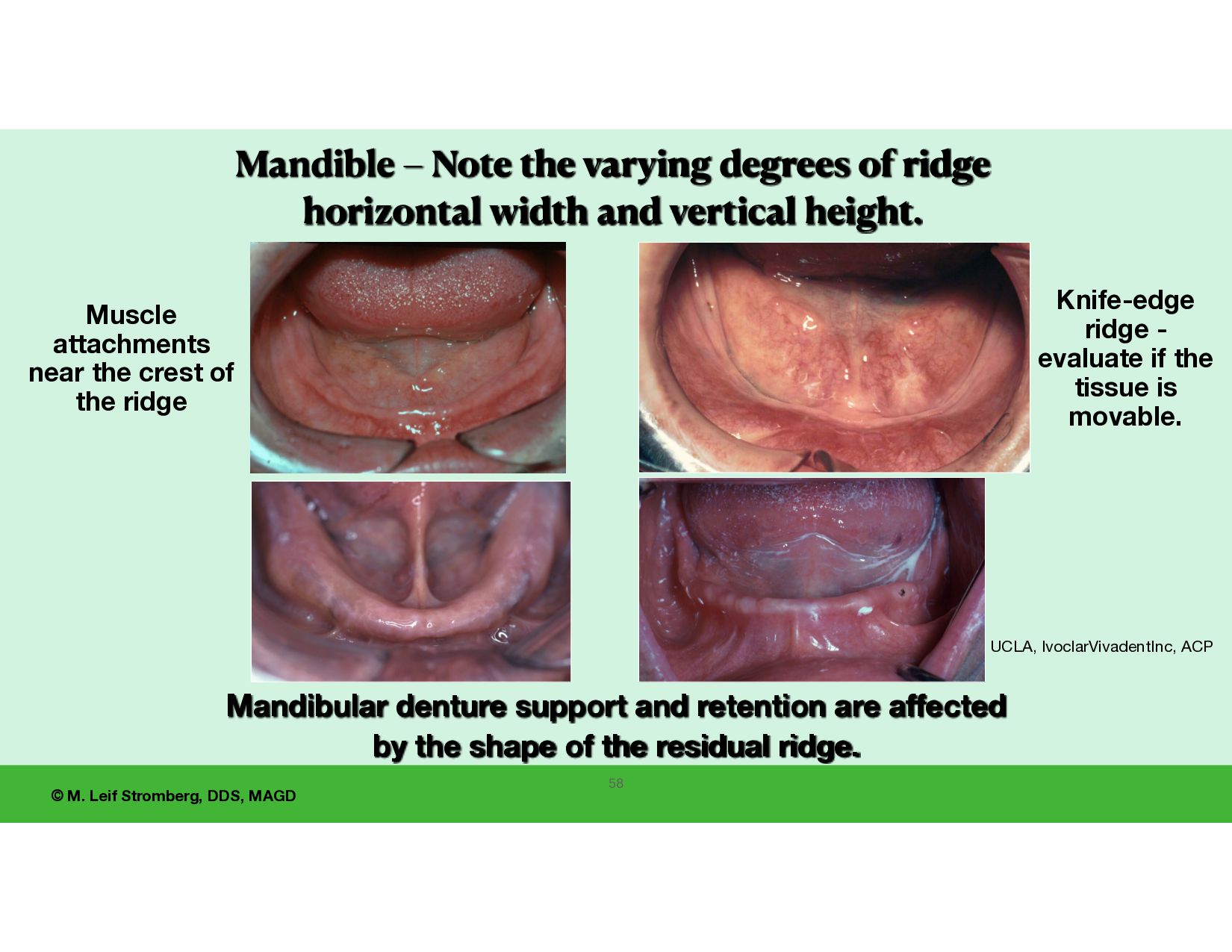
varying degrees of ridge horizontal width and vertical height. Knife-edge ridge - evaluate if the tissue is movable. Muscle attachments near the crest of the ridge UCLA, IvoclarVivadentInc, ACP Mandibular denture support and retention are affected by the shape of the residual ridge. 58
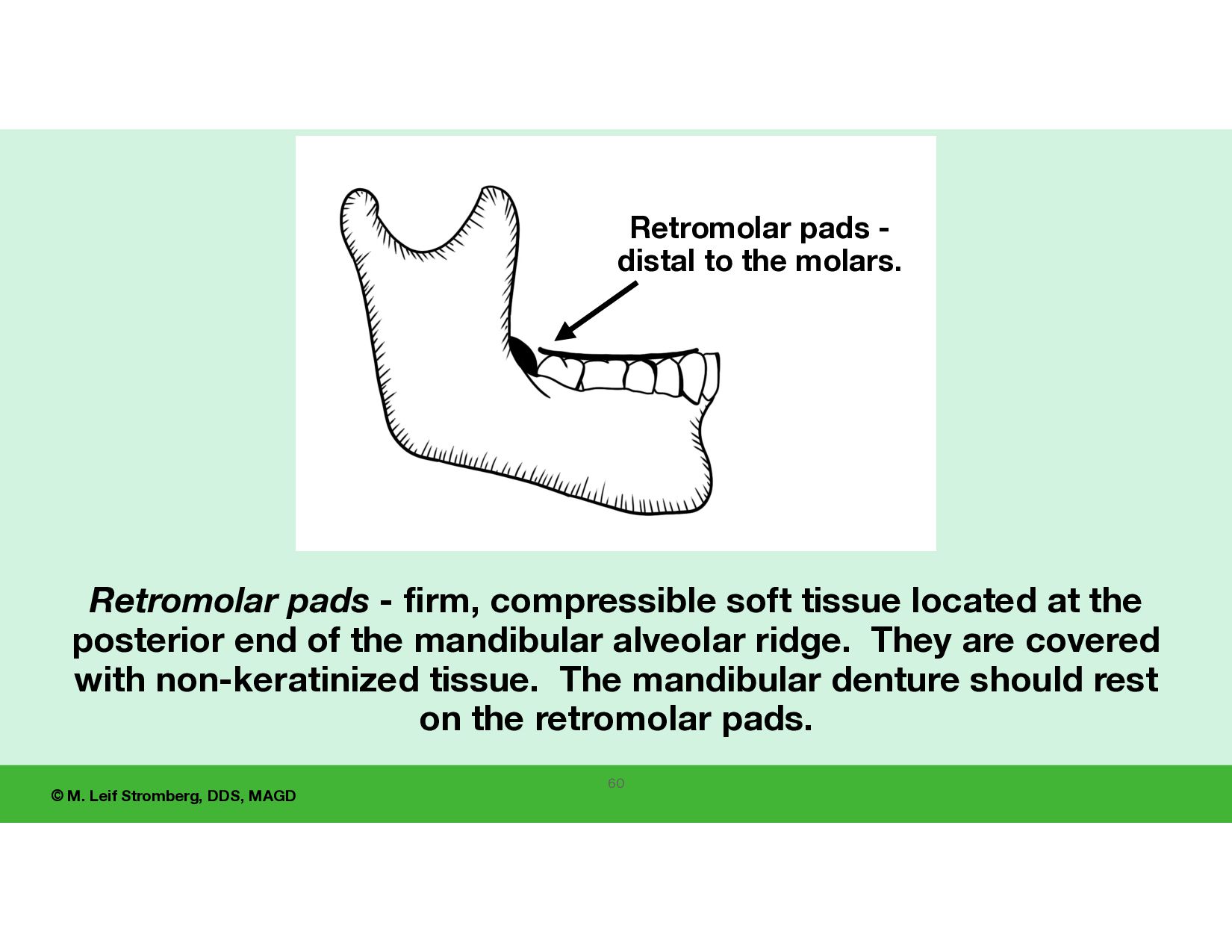
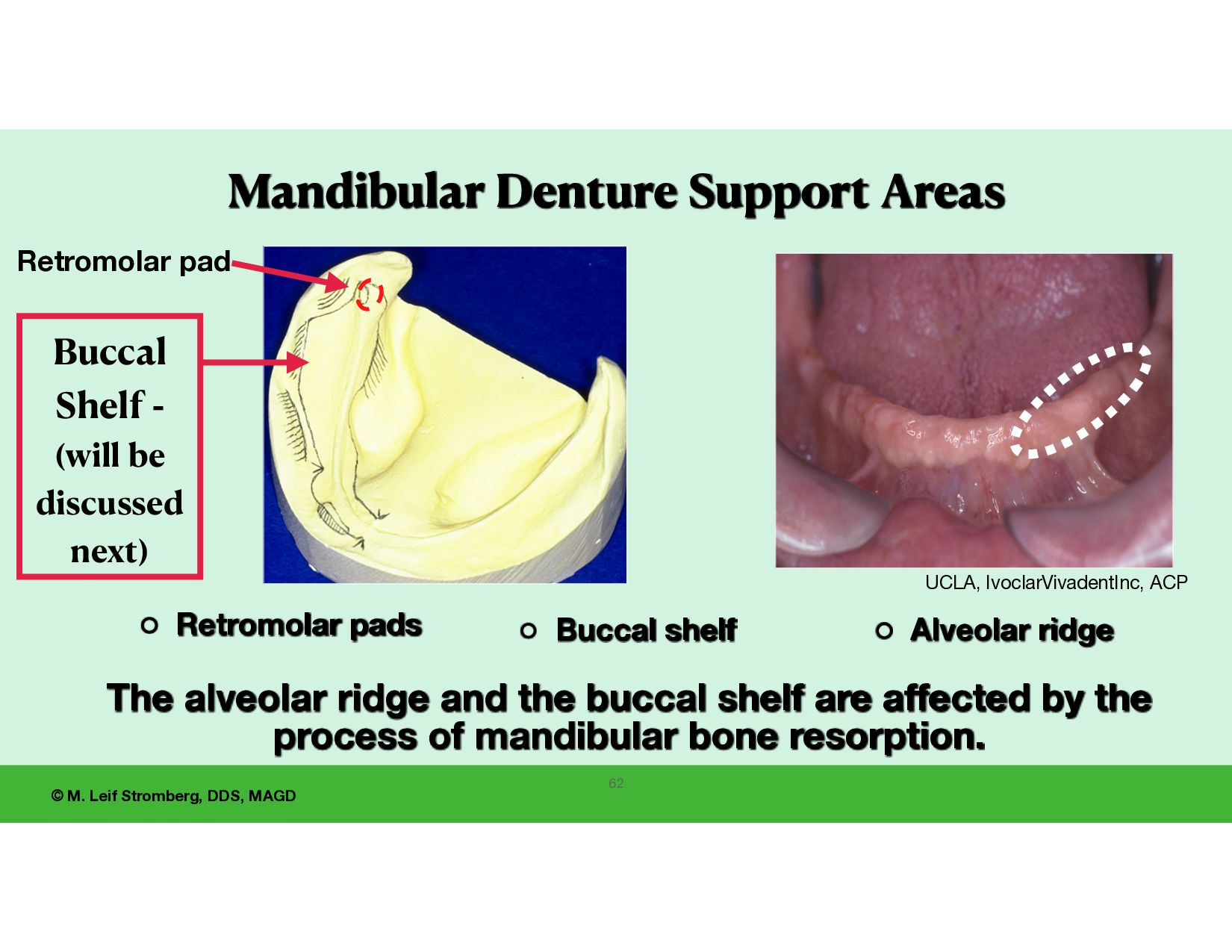
to the molars. Retromolar pads - firm, compressible soft tissue located at the posterior end of the mandibular alveolar ridge. They are covered with non-keratinized tissue. The mandibular denture should rest on the retromolar pads. 60
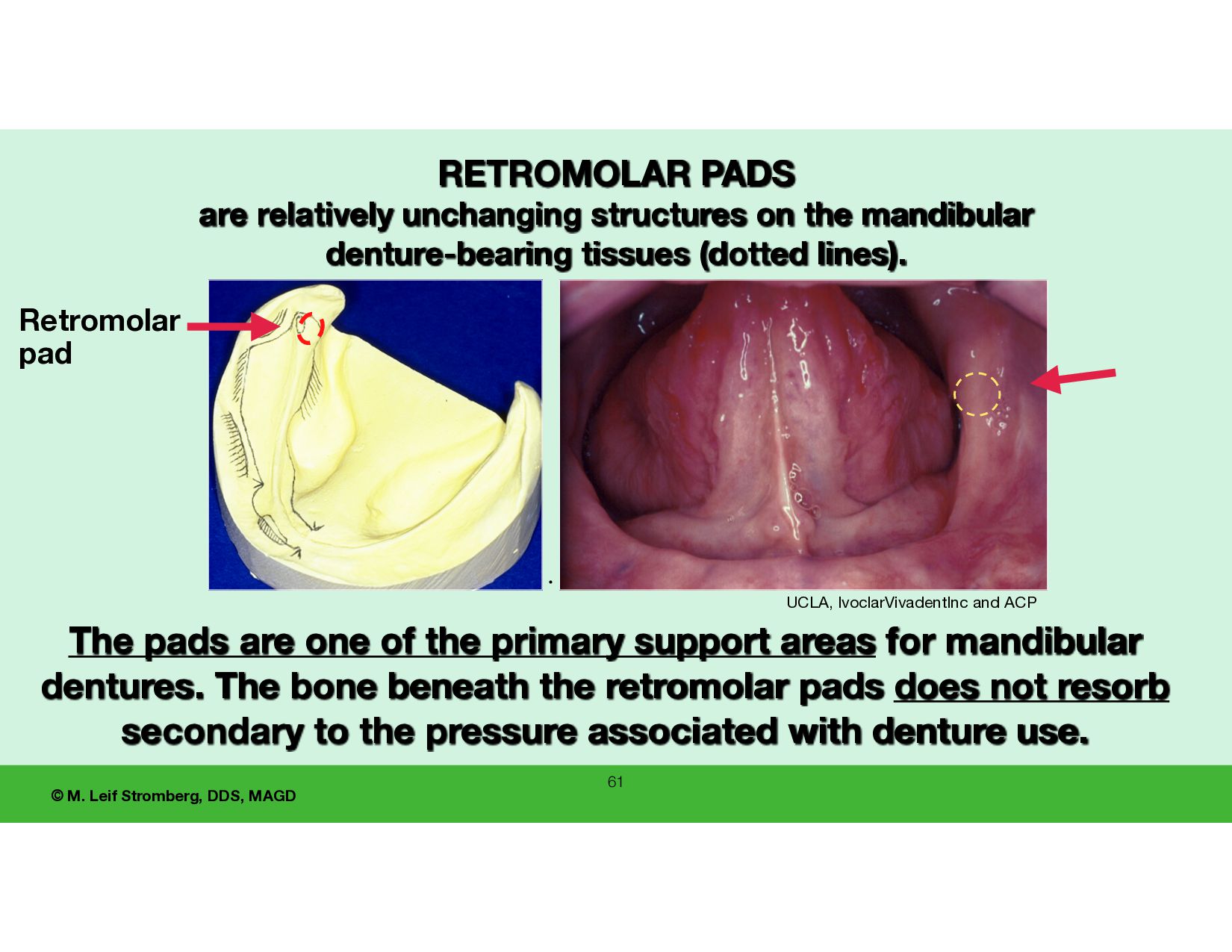
relatively unchanging structures on the mandibular denture-bearing tissues (dotted lines). • The pads are one of the primary support areas for mandibular dentures. The bone beneath the retromolar pads does not resorb secondary to the pressure associated with denture use. UCLA, IvoclarVivadentInc and ACP Retromolar pad
Retromolar pad Buccal Shelf - (will be discussed next) Retromolar pads Buccal shelf Alveolar ridge The alveolar ridge and the buccal shelf are affected by the process of mandibular bone resorption. UCLA, IvoclarVivadentInc, ACP 62
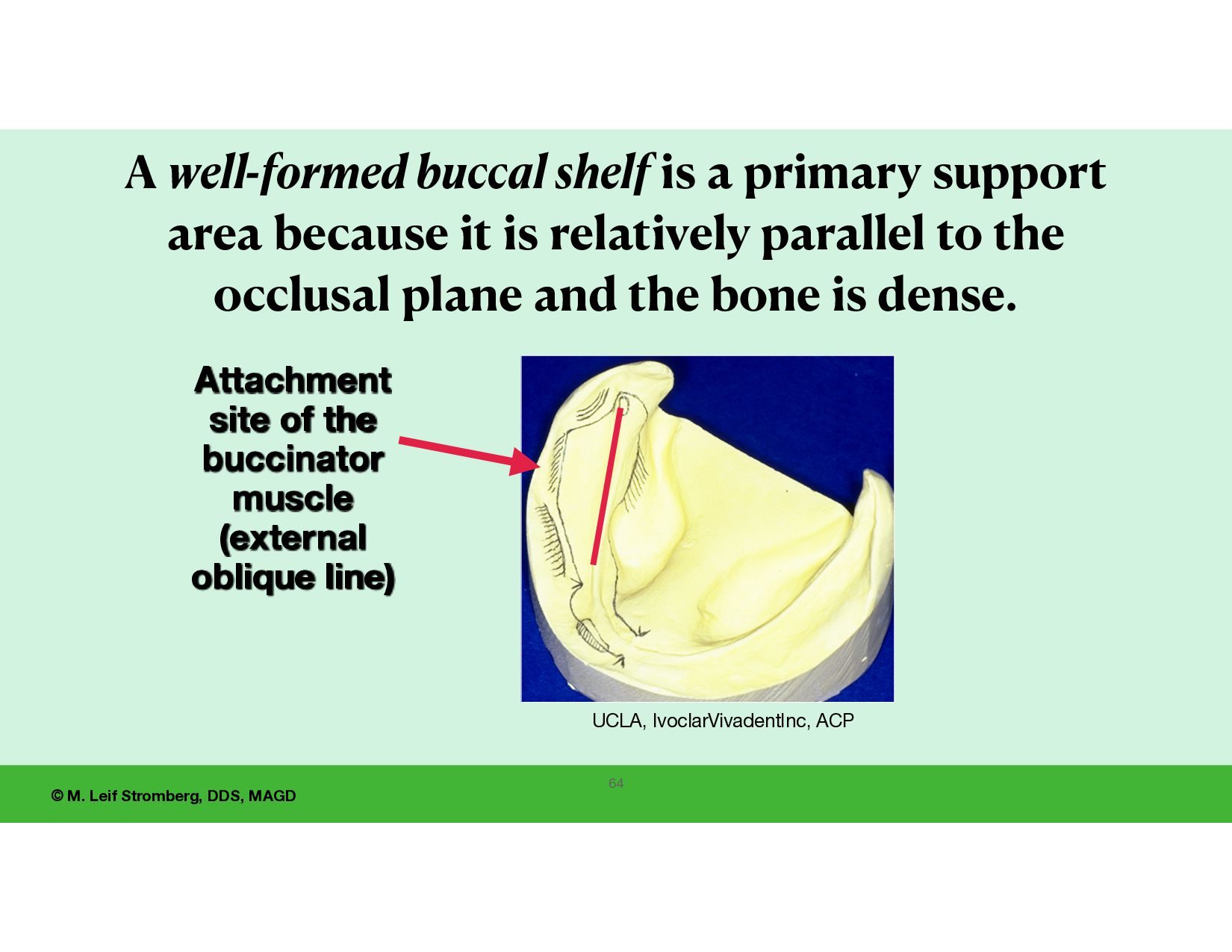
buccinator muscle (external oblique line) A well-formed buccal shelf is a primary support area because it is relatively parallel to the occlusal plane and the bone is dense. UCLA, IvoclarVivadentInc, ACP 64
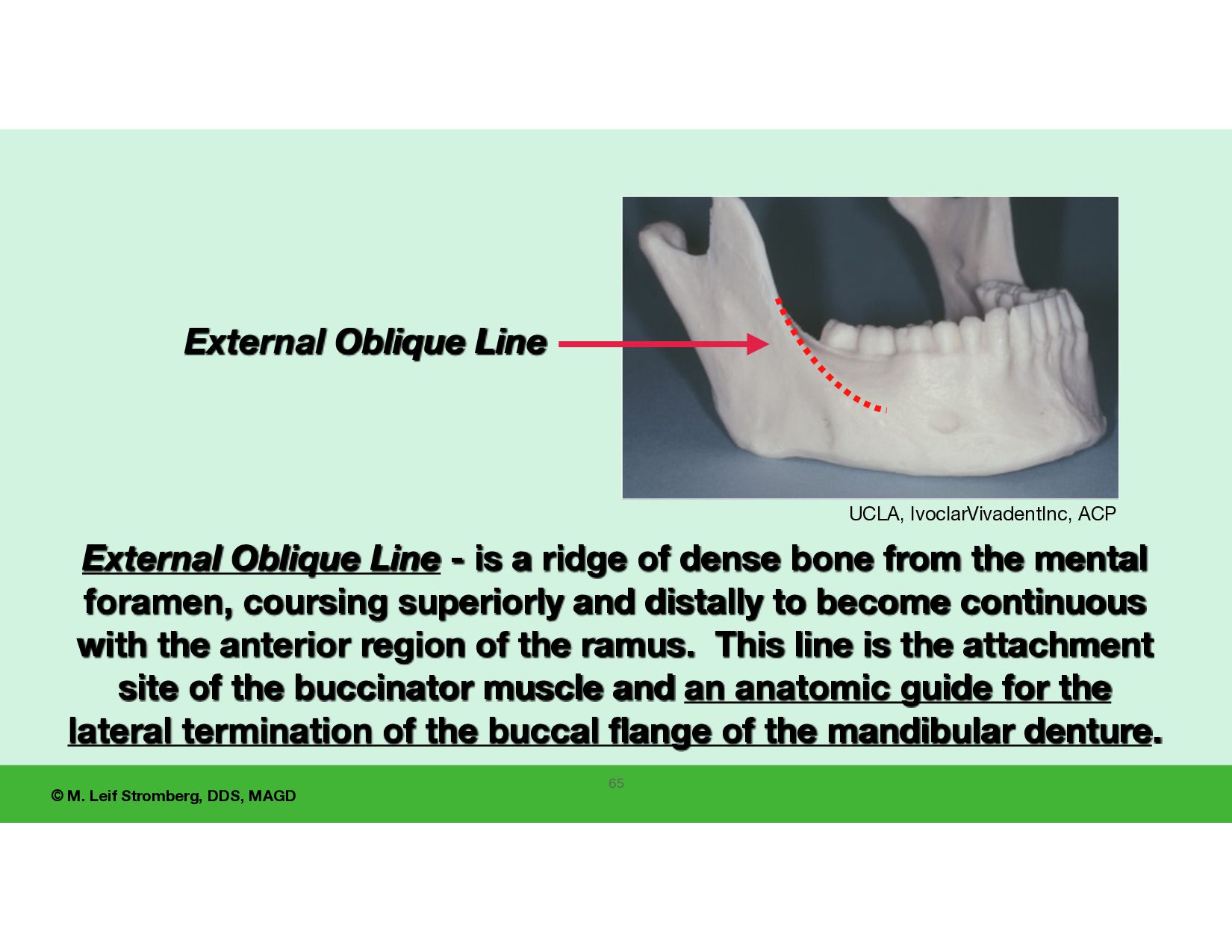
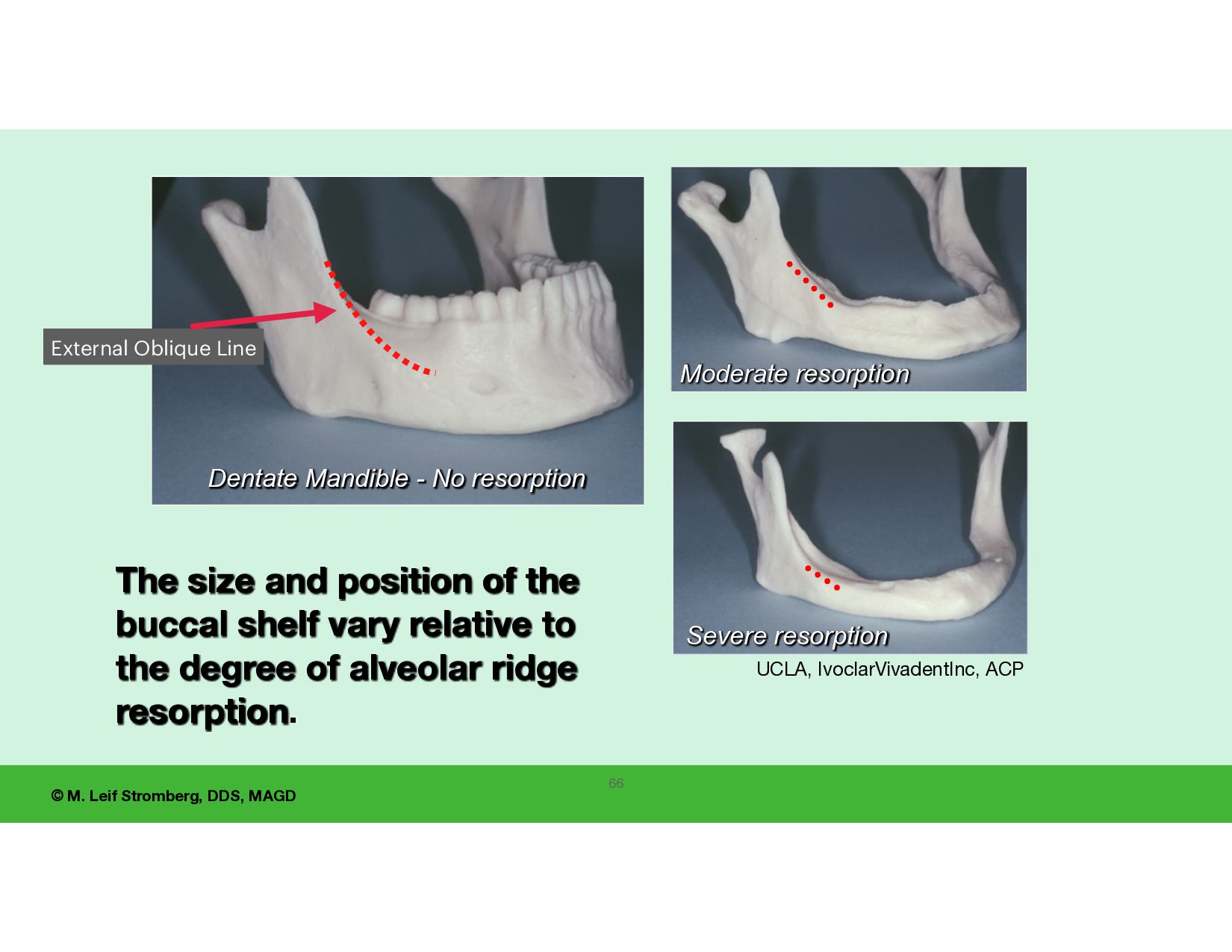
- is a ridge of dense bone from the mental foramen, coursing superiorly and distally to become continuous with the anterior region of the ramus. This line is the attachment site of the buccinator muscle and an anatomic guide for the lateral termination of the buccal flange of the mandibular denture. UCLA, IvoclarVivadentInc, ACP External Oblique Line
resorption The size and position of the buccal shelf vary relative to the degree of alveolar ridge resorption. UCLA, IvoclarVivadentInc, ACP Dentate Mandible - No resorption External Oblique Line
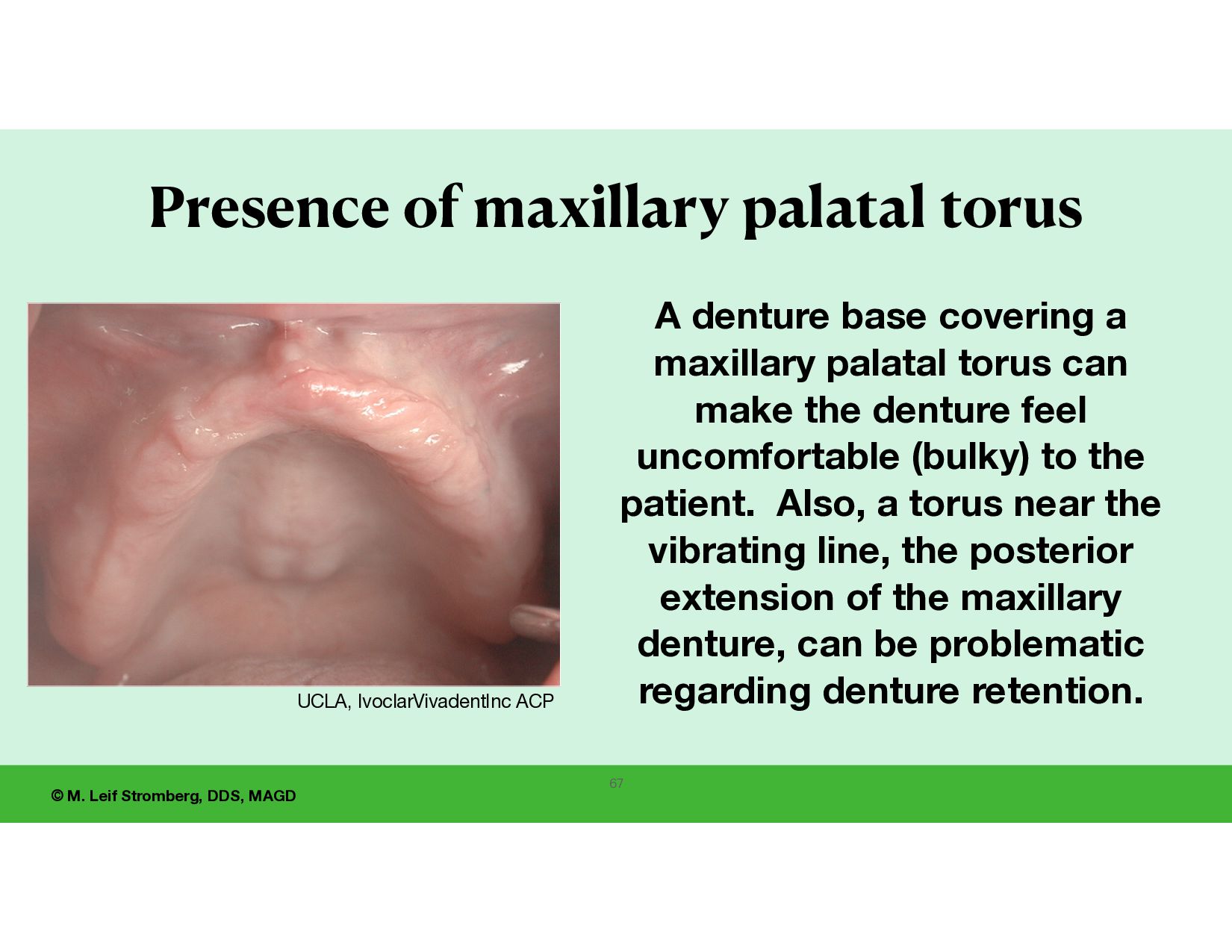
torus A denture base covering a maxillary palatal torus can make the denture feel uncomfortable (bulky) to the patient. Also, a torus near the vibrating line, the posterior extension of the maxillary denture, can be problematic regarding denture retention. UCLA, IvoclarVivadentInc ACP 67
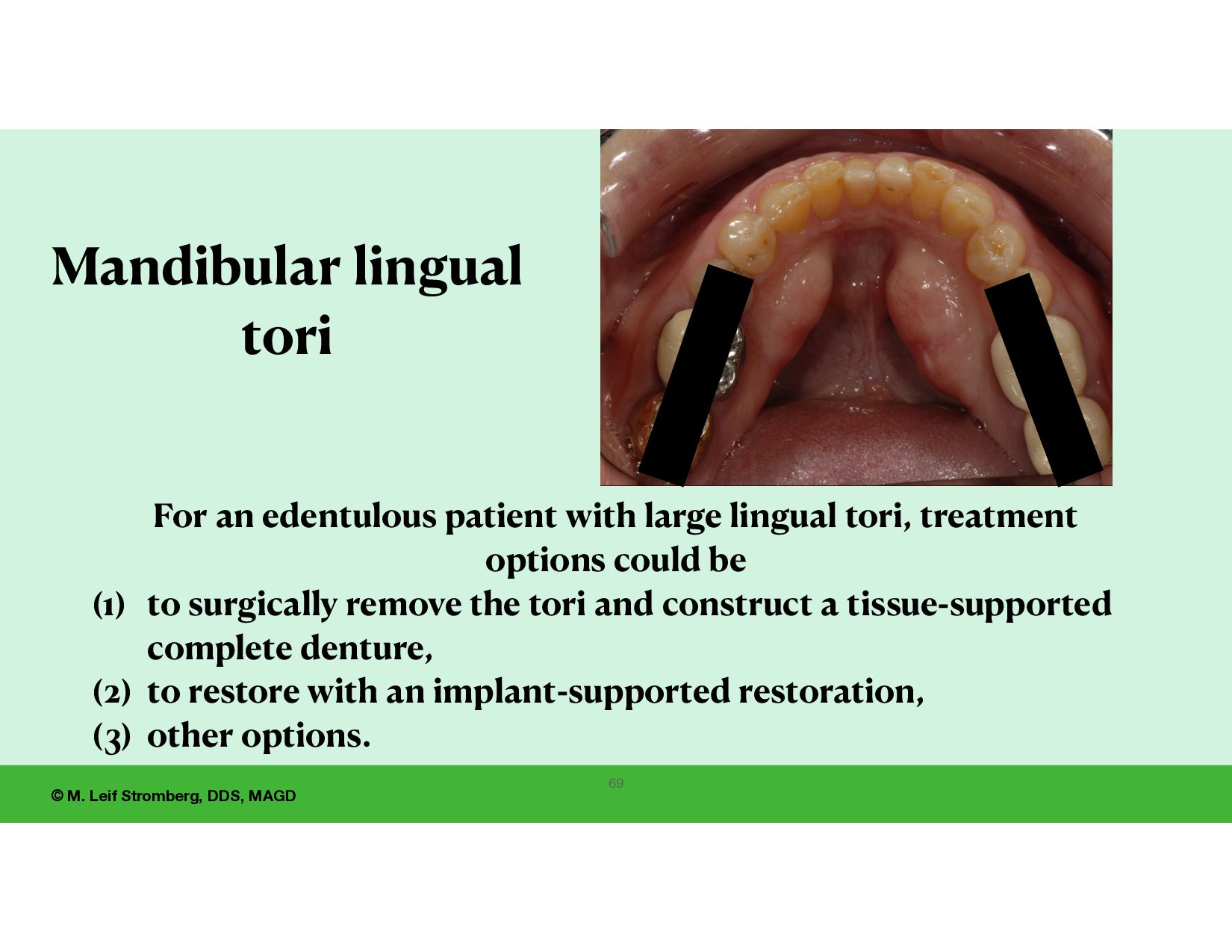
For an edentulous patient with large lingual tori, treatment options could be (1) to surgically remove the tori and construct a tissue-supported complete denture, (2) to restore with an implant-supported restoration, (3) other options.
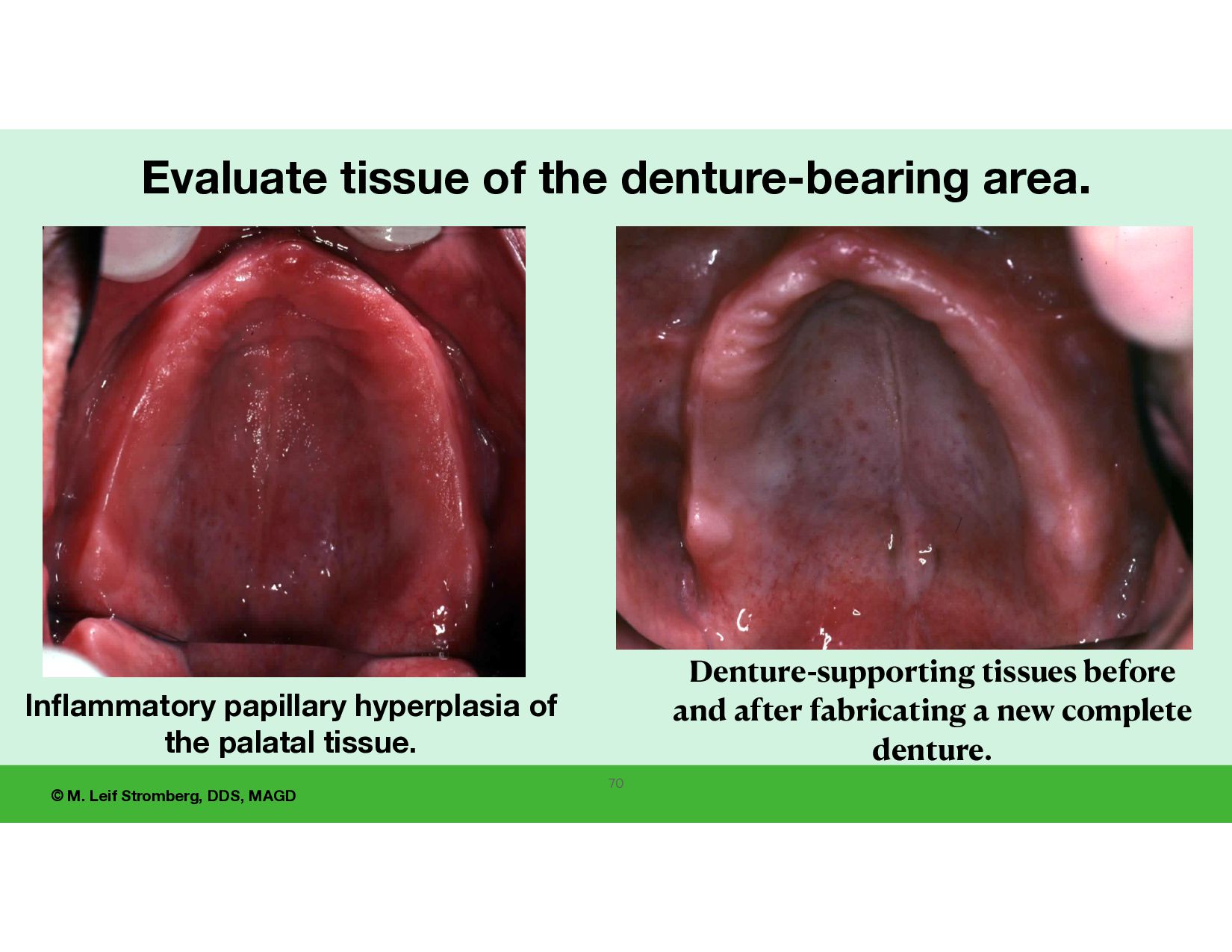
hyperplasia of the palatal tissue. Evaluate tissue of the denture-bearing area. 70 Denture-supporting tissues before and after fabricating a new complete denture.
ill- tting dentures and irritated, in amed, ulcerated denture-supporting tissues? 71 How will this tissue condition be resolved before the fi nal impressions are made?
treatment time. During the clinical examination, evaluate the patient for dry mouth, reduced salivary ow rate. Dry mouth makes wearing dentures more di cult and should be addressed. Rub a gloved nger on tissue-bearing mucosal tissues to evaluate tissue dryness and determine if there is a decrease in the fl ow of mucous saliva. (mucous saliva versus serous, watery saliva)
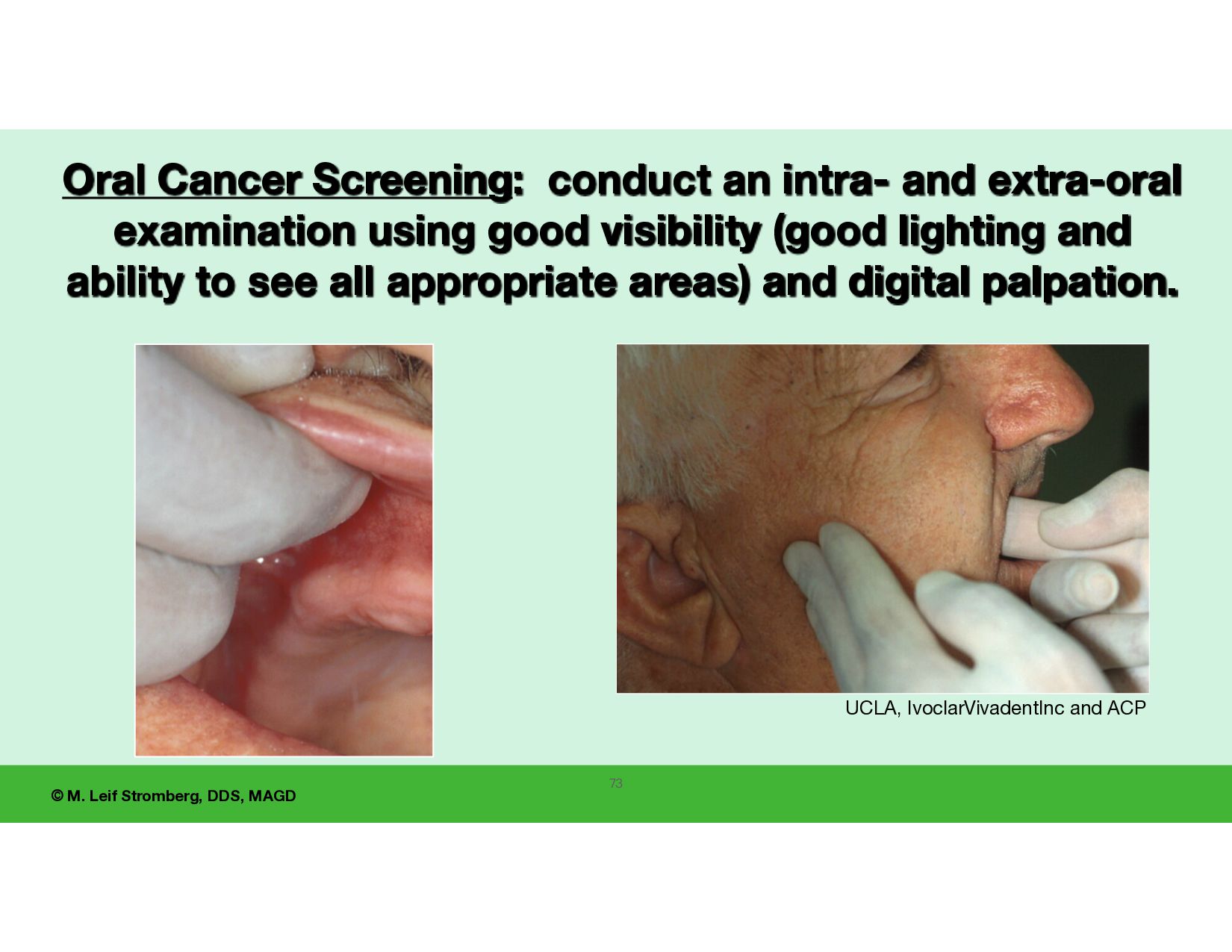
ACP Oral Cancer Screening: conduct an intra- and extra-oral examination using good visibility (good lighting and ability to see all appropriate areas) and digital palpation.
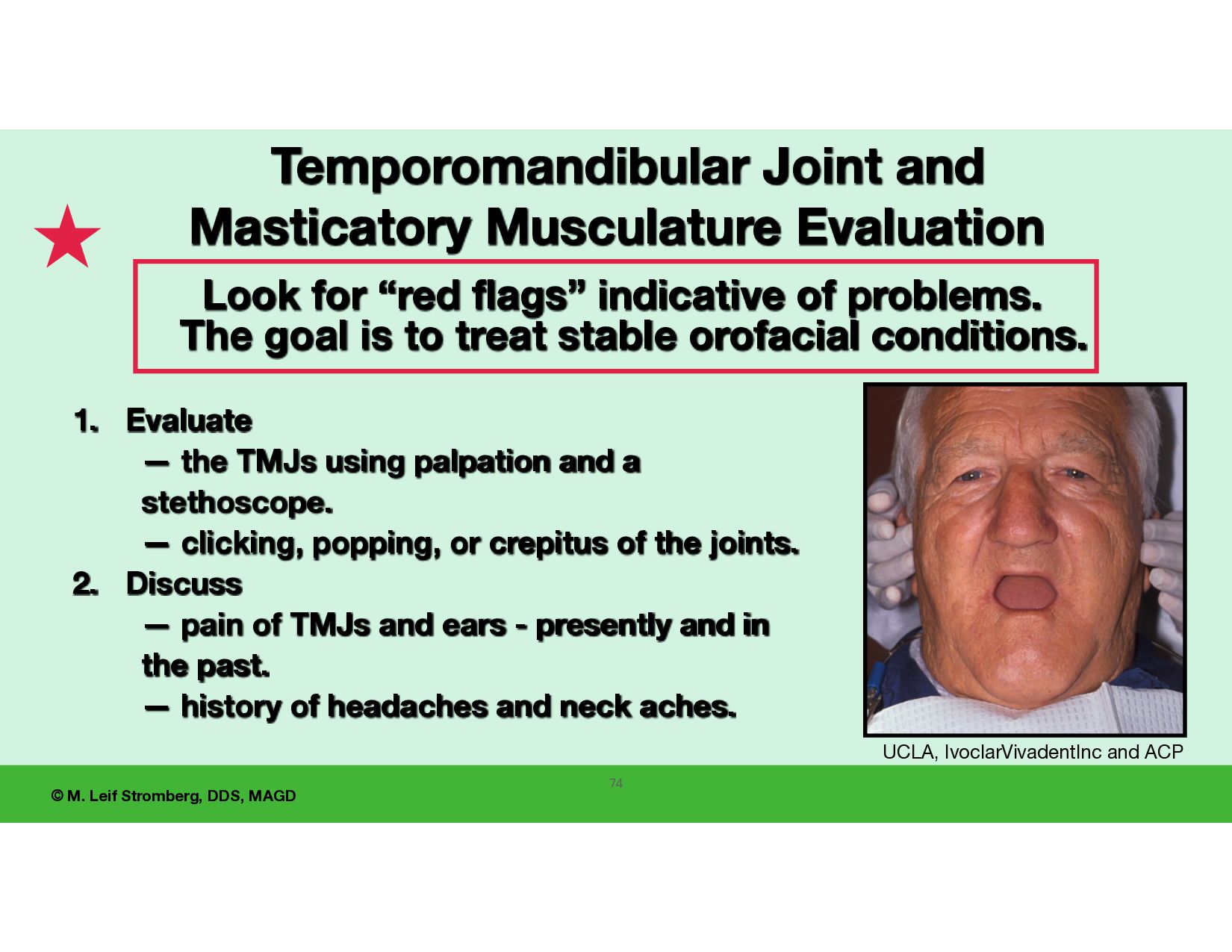
flags” indicative of problems. The goal is to treat stable orofacial conditions. UCLA, IvoclarVivadentInc and ACP Temporomandibular Joint and Masticatory Musculature Evaluation 1. Evaluate — the TMJs using palpation and a stethoscope. — clicking, popping, or crepitus of the joints. 2. Discuss — pain of TMJs and ears - presently and in the past. — history of headaches and neck aches.
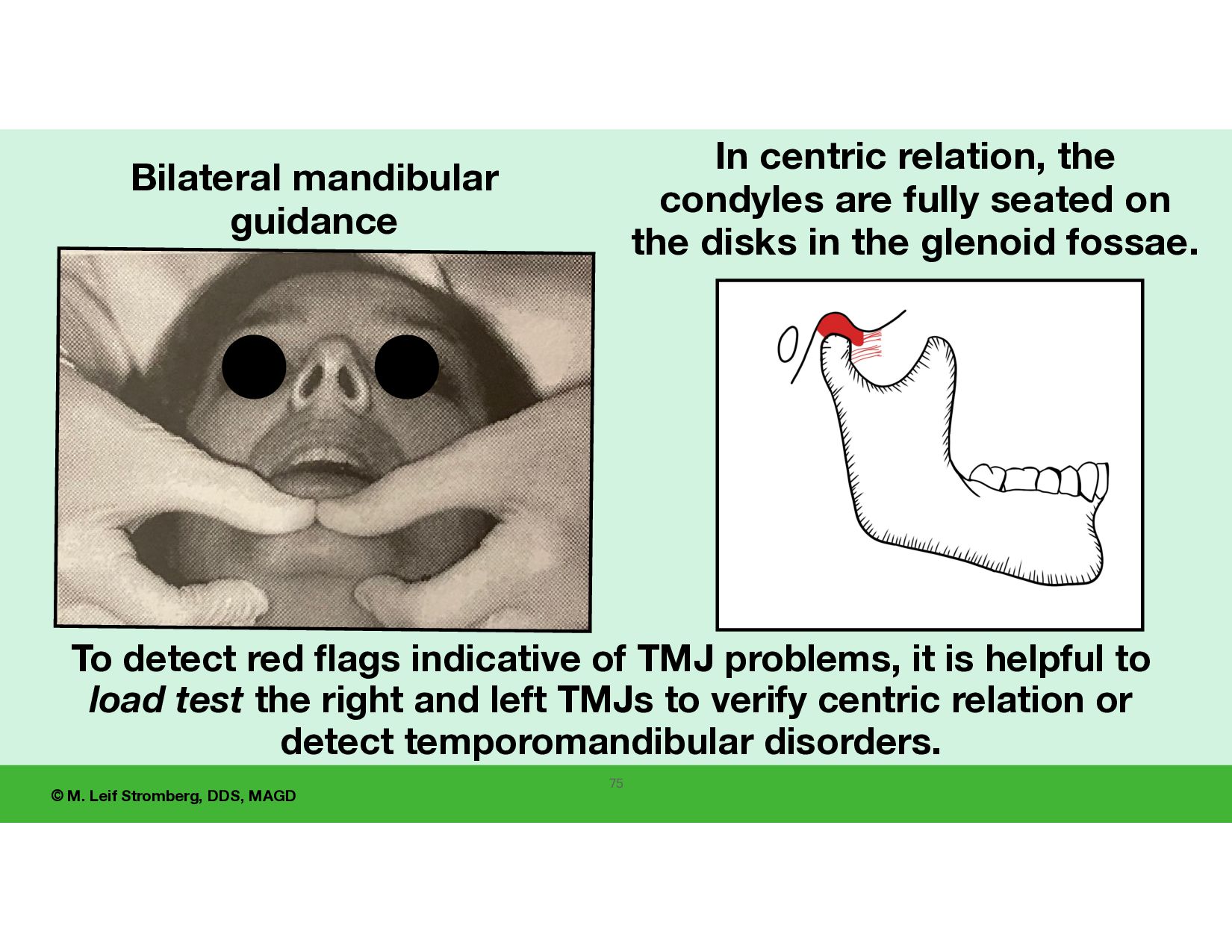
centric relation, the condyles are fully seated on the disks in the glenoid fossae. To detect red flags indicative of TMJ problems, it is helpful to load test the right and left TMJs to verify centric relation or detect temporomandibular disorders. 75
crucial for attempting successful and predictable edentulous restorations. Complete denture failure or the need for many post- delivery adjustments can result from: • a misdiagnosed temporomandibular disorder, • an undetected occlusal-muscle condition, or • treatment to an unstable condylar position. Sometimes, the dentist misplaces blame on the laboratory technician for denture problems resulting from unstable temporomandibular joints.
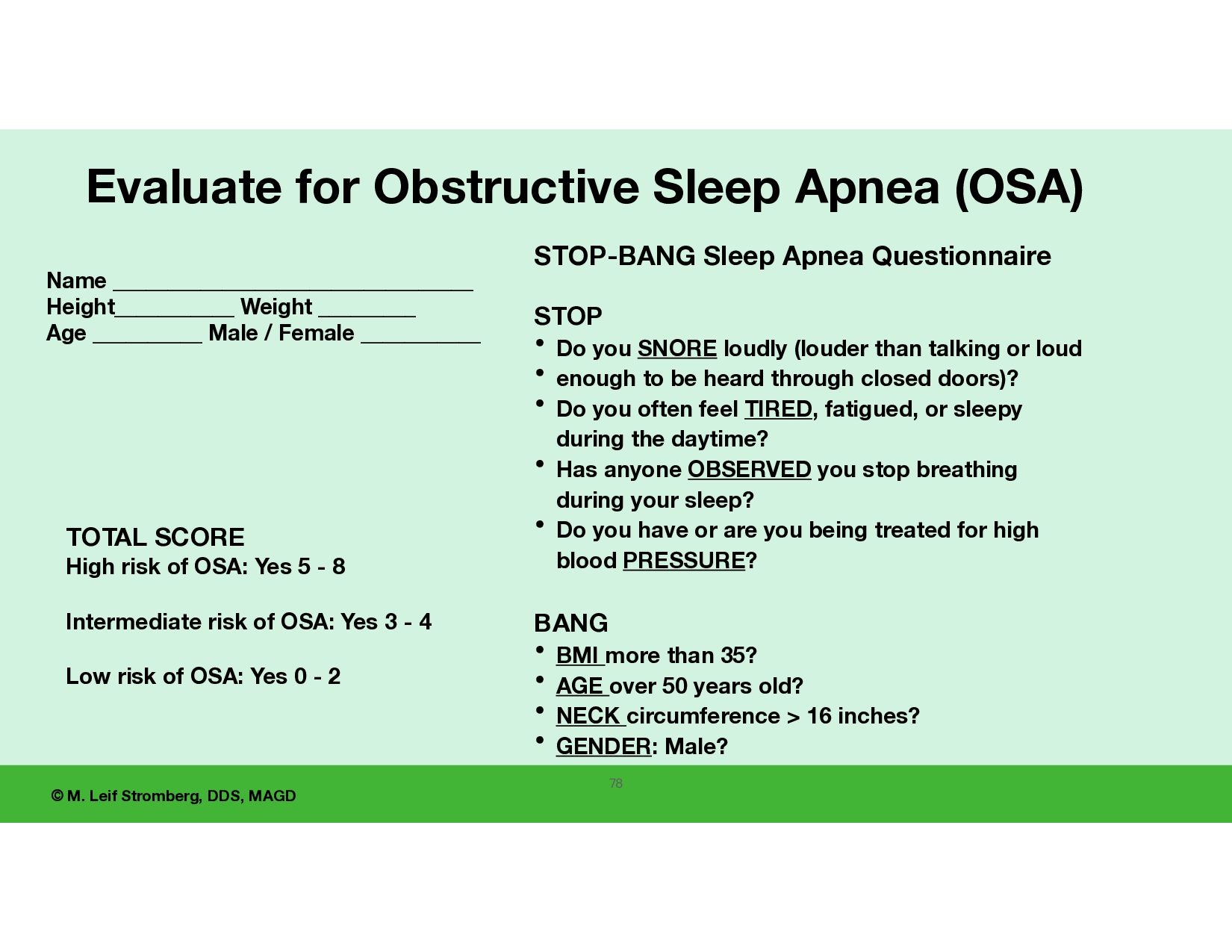
sleep apnea • The STOP-BANG questionnaire and a home pulse oximeter screening can be used. Also, discuss snoring. • The vertical dimension of occlusion of the edentulous restoration can a ff ect the patient’s airway. • To use a CPAP (Continuous Positive Airway Pressure) machine on an edentulous person, implants may be needed for denture support for a seal of the face mask. Consult with the patient’s physician.
STOP • Do you SNORE loudly (louder than talking or loud • enough to be heard through closed doors)? • Do you often feel TIRED, fatigued, or sleepy during the daytime? • Has anyone OBSERVED you stop breathing during your sleep? • Do you have or are you being treated for high blood PRESSURE? BANG • BMI more than 35? • AGE over 50 years old? • NECK circumference > 16 inches? • GENDER: Male? Name _________________________________ Height___________ Weight _________ Age __________ Male / Female ___________ TOTAL SCORE High risk of OSA: Yes 5 - 8 Intermediate risk of OSA: Yes 3 - 4 Low risk of OSA: Yes 0 - 2 Evaluate for Obstructive Sleep Apnea (OSA) 78
a panoramic radiograph or CBCT (Cone-beam computed tomography) image. The dentist or radiologist should carefully evaluate and diagnose any radiographs taken. If the patient is considering placement of dental implants in the future, consider recommending CBCT imaging. 79
patient’s wants, expectations, and needs. • Let the patient know the treatment options, what to expect with the options, the fees of the various options, and your recommended treatment. • Tell the patient what you can possibly improve (e.g., retention, esthetics). Be positive and realistic. 80
the patient’s existing dentures. If you do alter the patient’s existing dentures, have consent from the patient (for altering the denture base, adding tissue conditioning material, placing adhesive and impression material, and/or putting an acrylic table on mandibular posterior teeth to act as an occlusal splint). A ft er adjustments, the dentures may be unwearable by the patient. 82
Include that discussed: • option of no treatment and consequences (not recommended); • option of single-phase and dual-phase denture services, • option of small diameter (less than 3 mm diameter) implants or root form (3mm or more diameter) implants in the maxilla and mandible to retain dentures, • option of all-on-4-6 fi xed (dentist removable) restorations, • option of implants with fi xed bridges. • bene fi ts/advantages, risks/disadvantages, and fees of options. • that a denture can fracture and need repairs or replacement, • teeth can wear, necessitating replacement of teeth or remaking of the denture at additional fees; • that the patient should not self-repair a denture but return to the dentist to evaluate and discuss repair options; • that the ADA recommends: over time, dentures may need relining, rebasing, or replacing. The normal life of dentures is about 5 to 10 years.
to place implants after dentures have been fabricated. • However, the patient may need bone reduction if implants and attachments are placed; • there will be additional costs; • the denture will weaken in the area of implants and attachments, and denture fracture may require repair or remaking the denture; • the patient may need to have the dentures remade after bone reduction when implants and attachments are added. 84
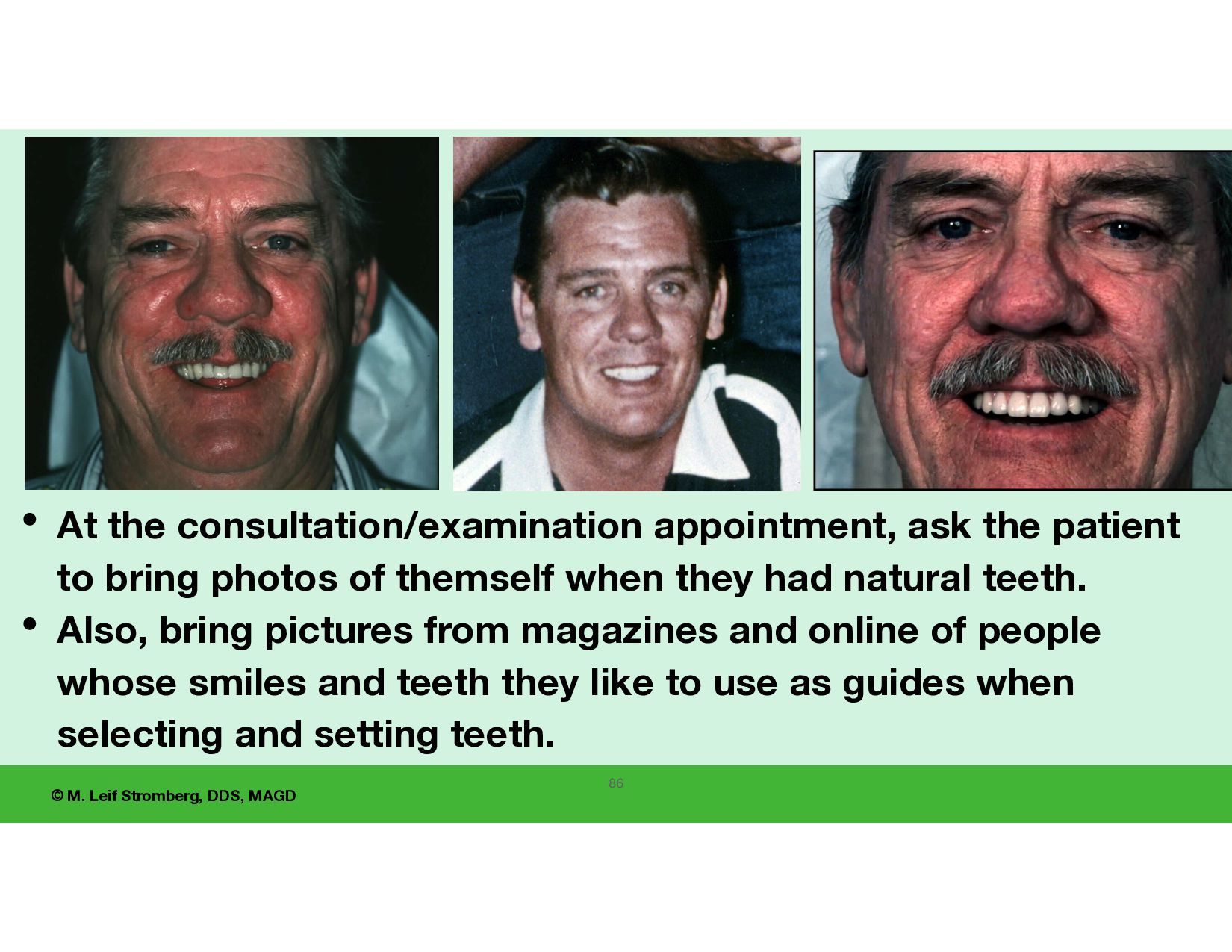
to expect with new tissue-supported dentures. • The patient’s chewing function will be signi cantly reduced from natural teeth. • The restorations will feel “di ff erent” and possibly uncomfortable at the initial placement. • The patient’s speech will be a ff ected. This is normal. • The patient will experience some movement of the dentures in their mouth. • Let the patient know that you will support them in adapting to their new dentures if they have di ffi culty with them. What will you do if the patient does not accept the new dentures after delivery? 85
appointment, ask the patient to bring photos of themself when they had natural teeth. • Also, bring pictures from magazines and online of people whose smiles and teeth they like to use as guides when selecting and setting teeth. 86
fabrication steps being done competently by the dentist, dental assistant, and dental lab technician for complete denture SUCCESS. 2. “Adequate complete dentures”: are stable, have adequate retention, adequate vertical dimension of occlusion and esthetics, and all posterior teeth contact evenly in centric relation occlusion. Sometimes the denture results are adequate, and the patient rejects the new dentures. 3. When beginning to fabricate an edentulous restoration, you never know what challenging conditions may present. 4. FUNDAMENTALS of the edentulous consultation/examination appointment include (a) listening actively and with compassion so the patient feels understood, (b)understanding the patient’s wants and expectations, and (c) evaluating important anatomical intraoral features. 5. Considering the clinical fi ndings and patient expectations, decide if you can treat the case to achieve acceptable results, and do you want to? SYNOPSIS OF MODULE 1: 87
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
![© M. Leif Stromberg, DDS, MAGD 89 CONTACT ME [email protected]](https://files.speakerdeck.com/presentations/9dffa32ffc8941b79425289379f5f629/slide_84.jpg){kind=link}
{kind=link}