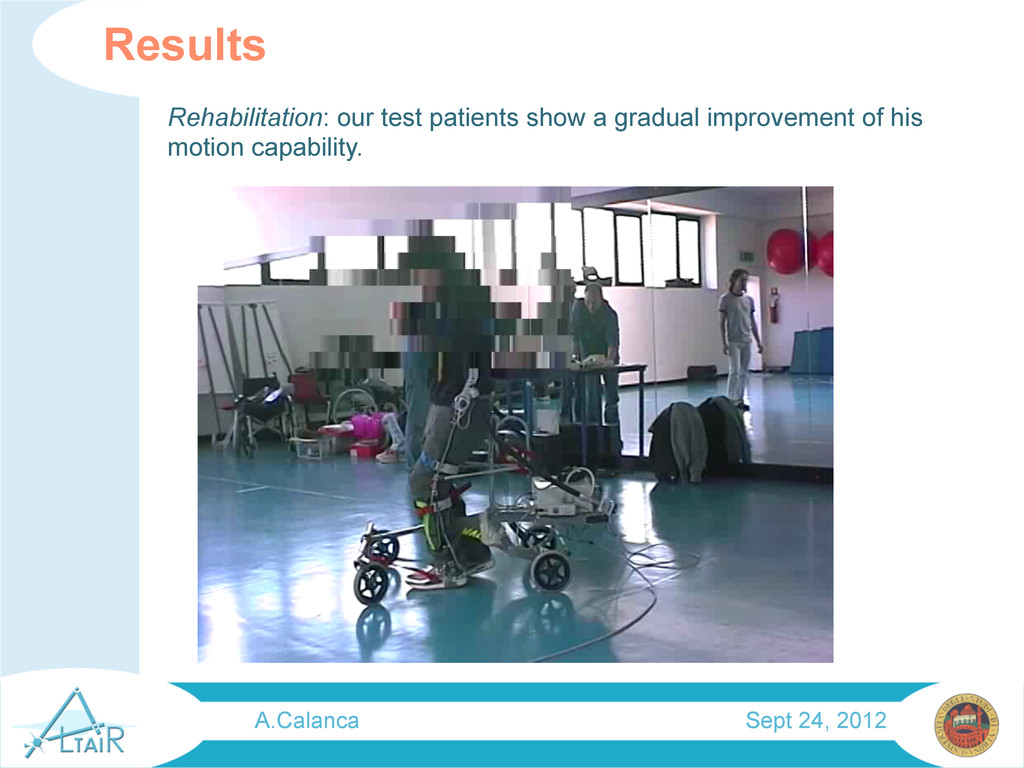
between 0.15 and 0.25%. Precocity of rehabilitation has a fundamental role in prevention of secondary deformity and anomalous motor development [Viurtello1984]. Also recent studies pay great attention on physical therapy applied to young CP patients, focusing on movement based strategy and physical training [Dodd 2002][Damiano 2006]. This kind of treatments are quite expensive because they need the presence of one or more physiotherapists. Orthotic systems try to help this treatment relieving physiotherapist of part of work. A.Calanca Sept 24, 2012
have an unique layer of mixed rubber and fibers that improves muscle safety and long lasting in respect with classical McKibben. Disadvantages: non-linear behaviour, control issue. McKibben Pneumatic Artificial Muscles • Intrinsic safety and compliance • High power to weight ratio • High forces • Low cost • Supply via small high pressure air bottle. A.Calanca Sept 24, 2012
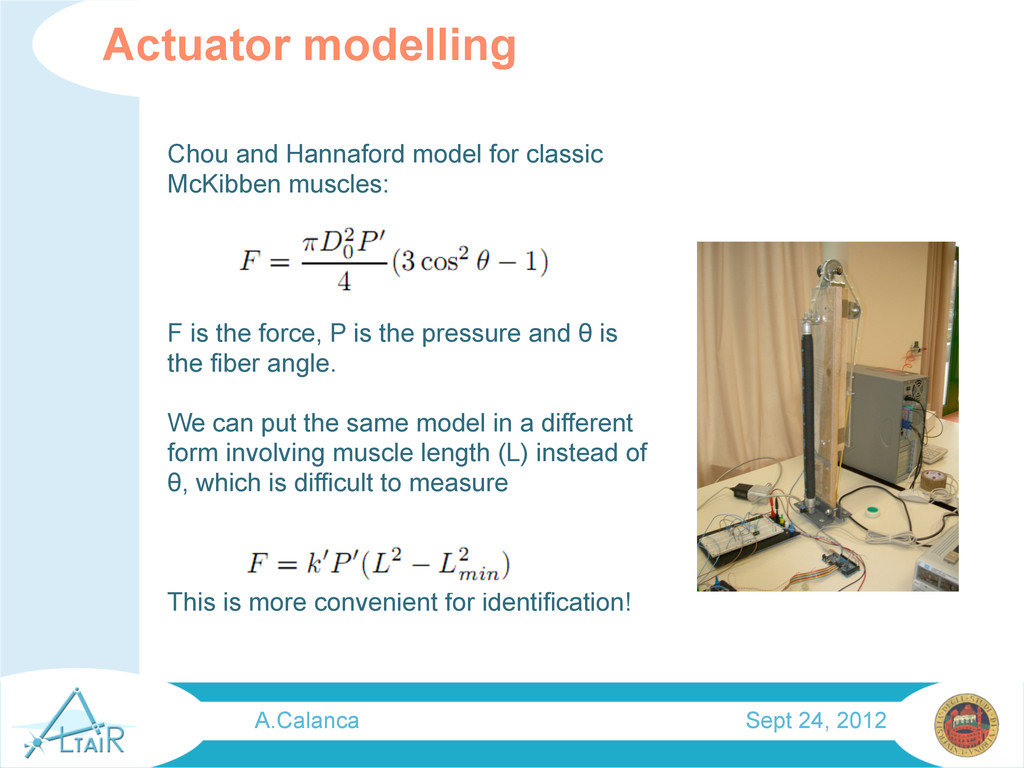
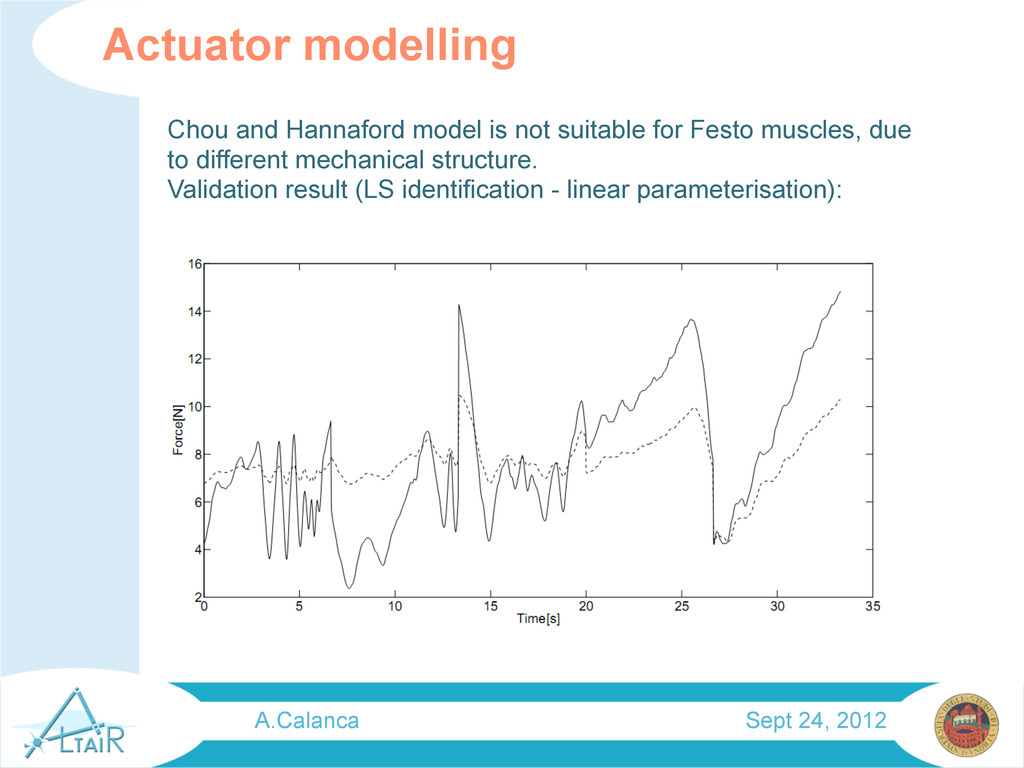
the force, P is the pressure and θ is the fiber angle. We can put the same model in a different form involving muscle length (L) instead of θ, which is difficult to measure This is more convenient for identification! Actuator modelling A.Calanca Sept 24, 2012
input, 5 middle, 1 output) Training Data collected from test bed experiments at different pressure levels and different force frequencies. Pressure and muscle length as input, force as target Control System A.Calanca Sept 24, 2012
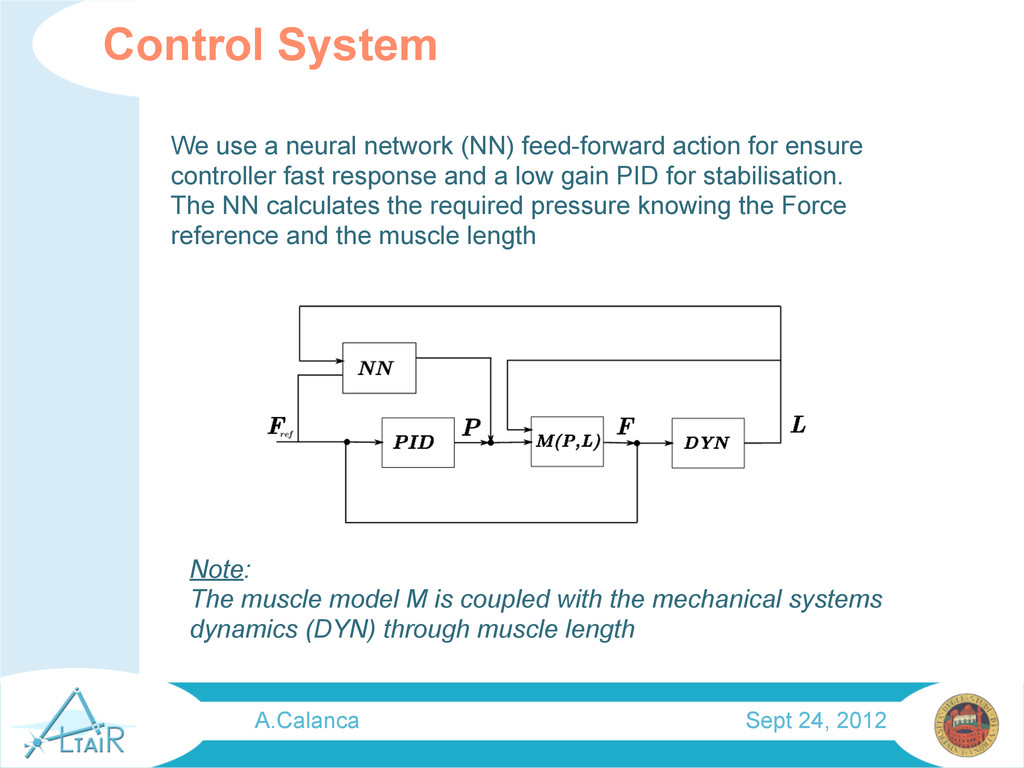
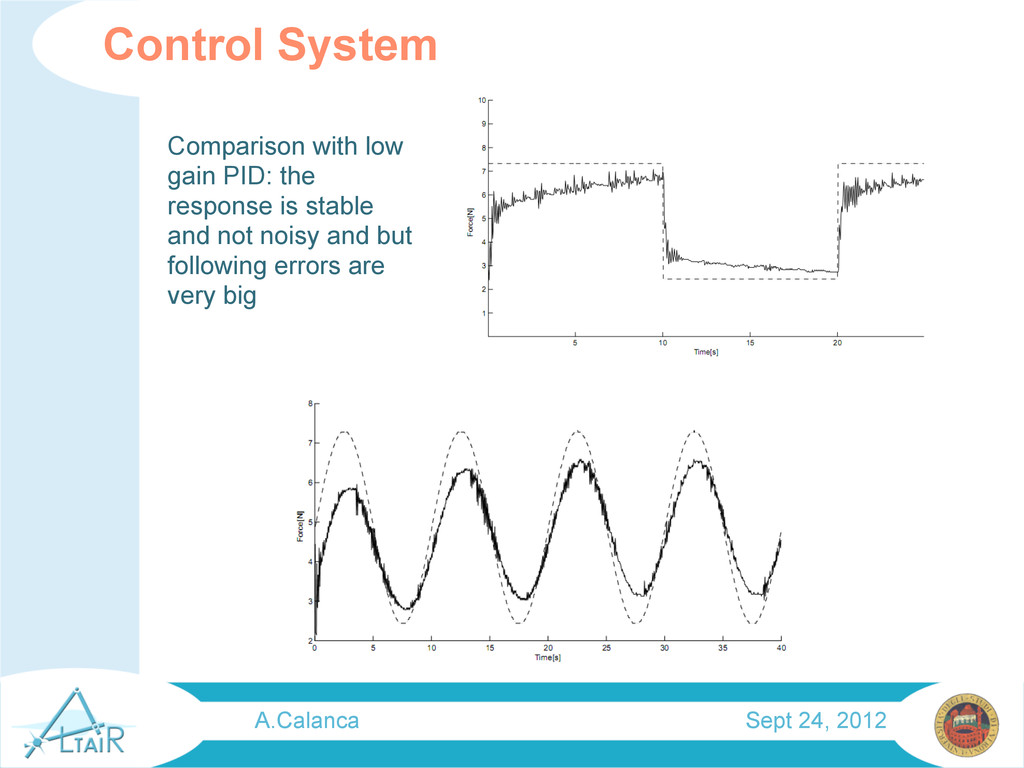
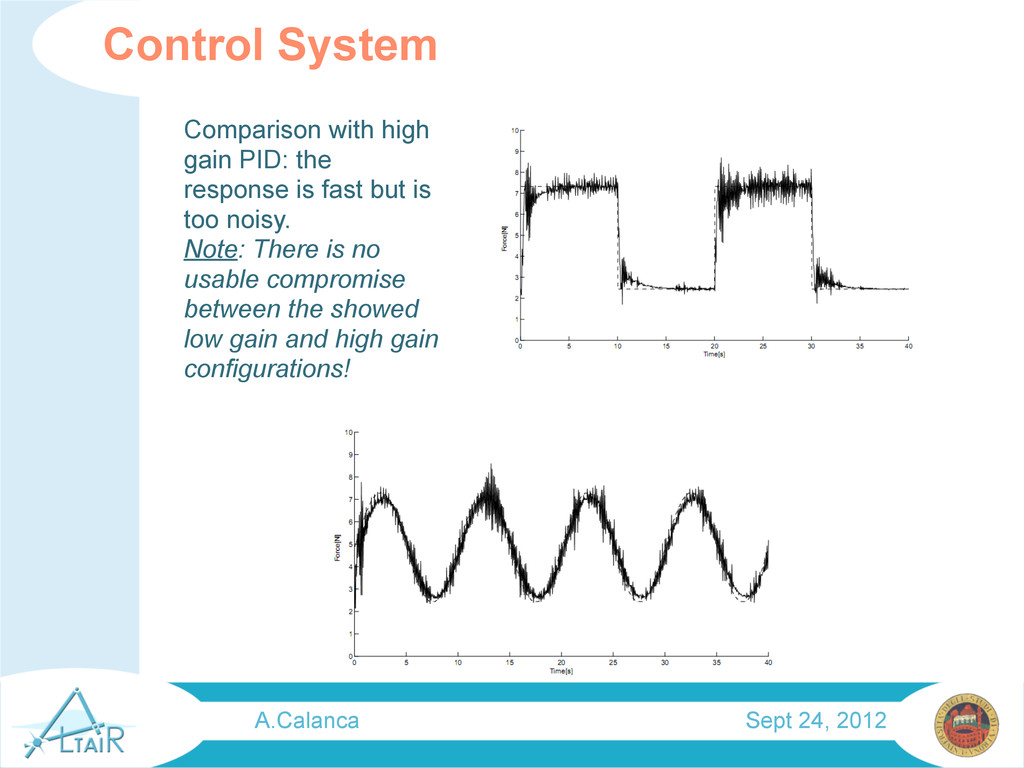
controller fast response and a low gain PID for stabilisation. The NN calculates the required pressure knowing the Force reference and the muscle length Control System Note: The muscle model M is coupled with the mechanical systems dynamics (DYN) through muscle length A.Calanca Sept 24, 2012
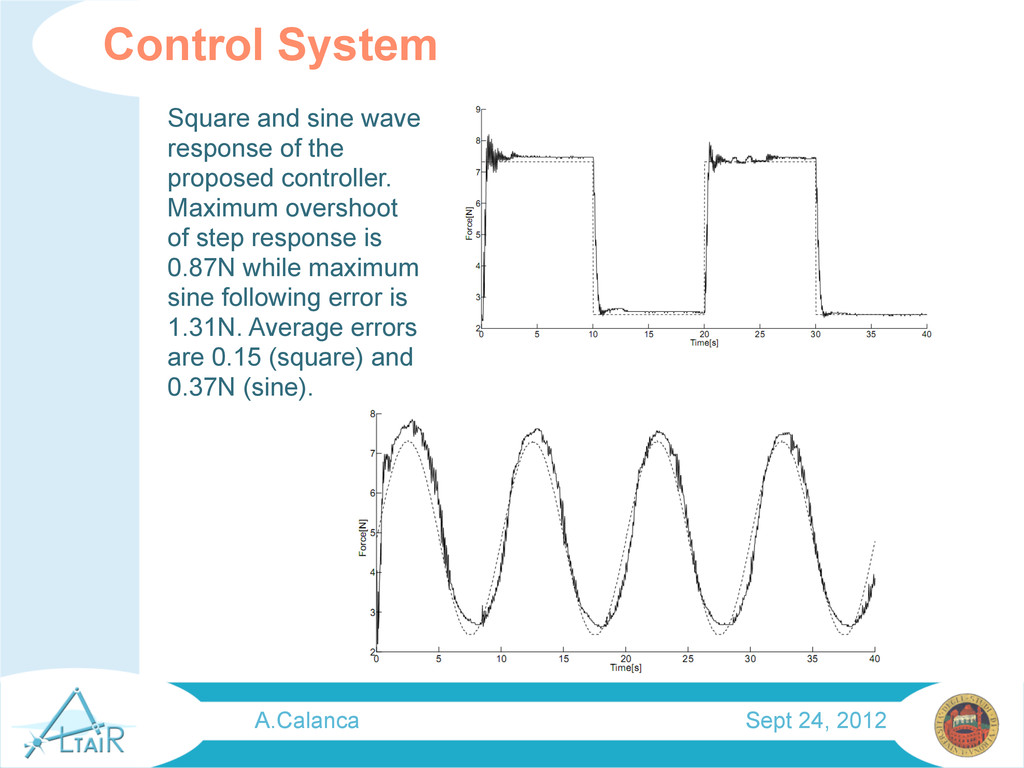
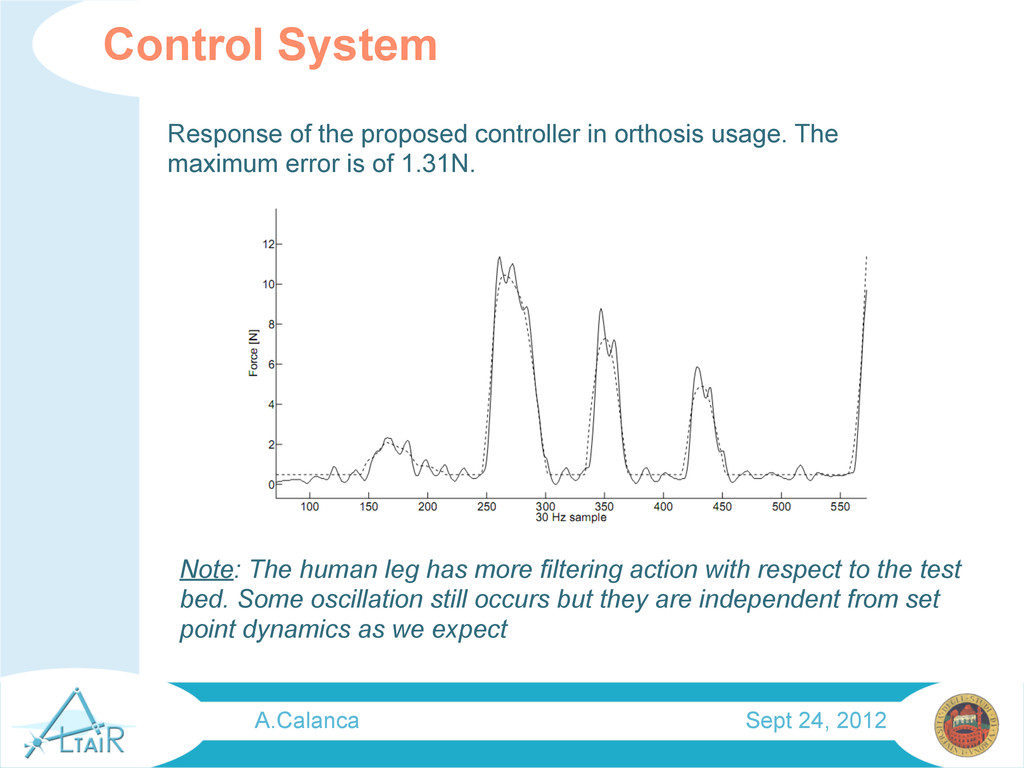
controller. Maximum overshoot of step response is 0.87N while maximum sine following error is 1.31N. Average errors are 0.15 (square) and 0.37N (sine). A.Calanca Sept 24, 2012
The maximum error is of 1.31N. Note: The human leg has more filtering action with respect to the test bed. Some oscillation still occurs but they are independent from set point dynamics as we expect A.Calanca Sept 24, 2012
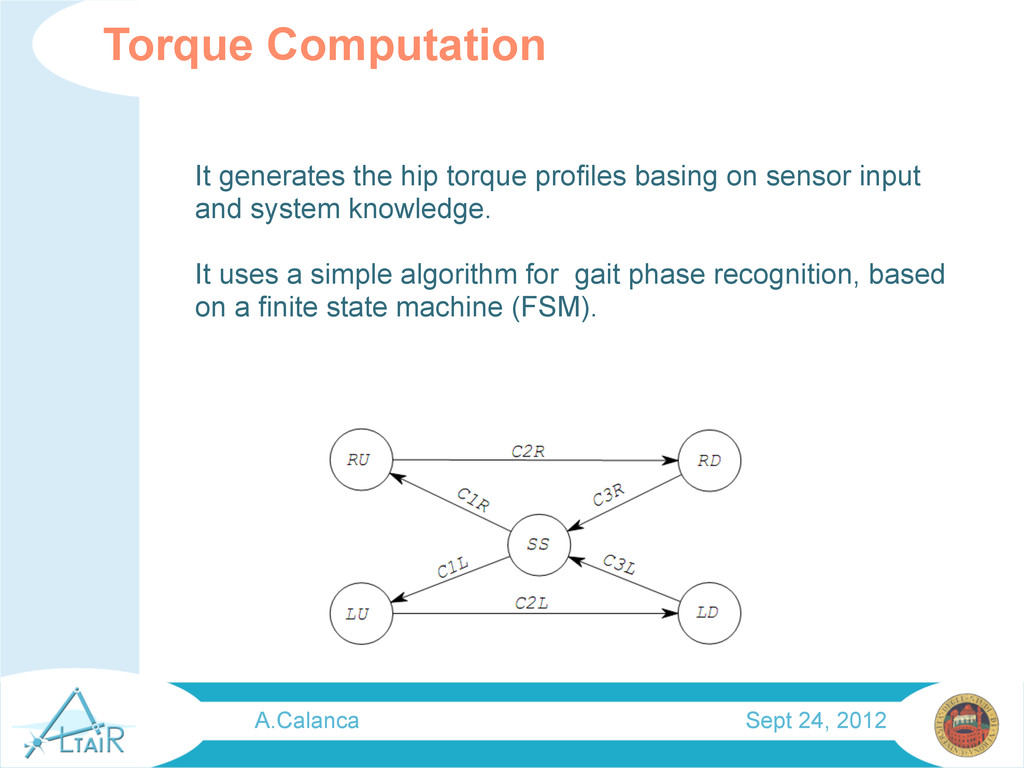
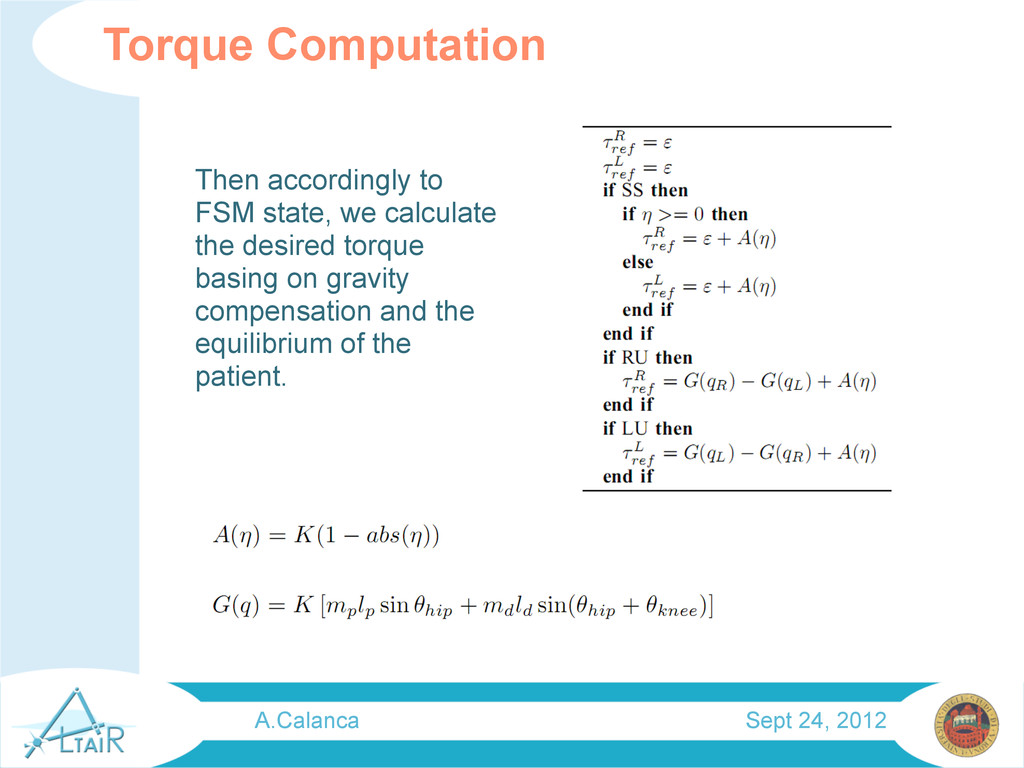
and system knowledge. It uses a simple algorithm for gait phase recognition, based on a finite state machine (FSM). Torque Computation A.Calanca Sept 24, 2012
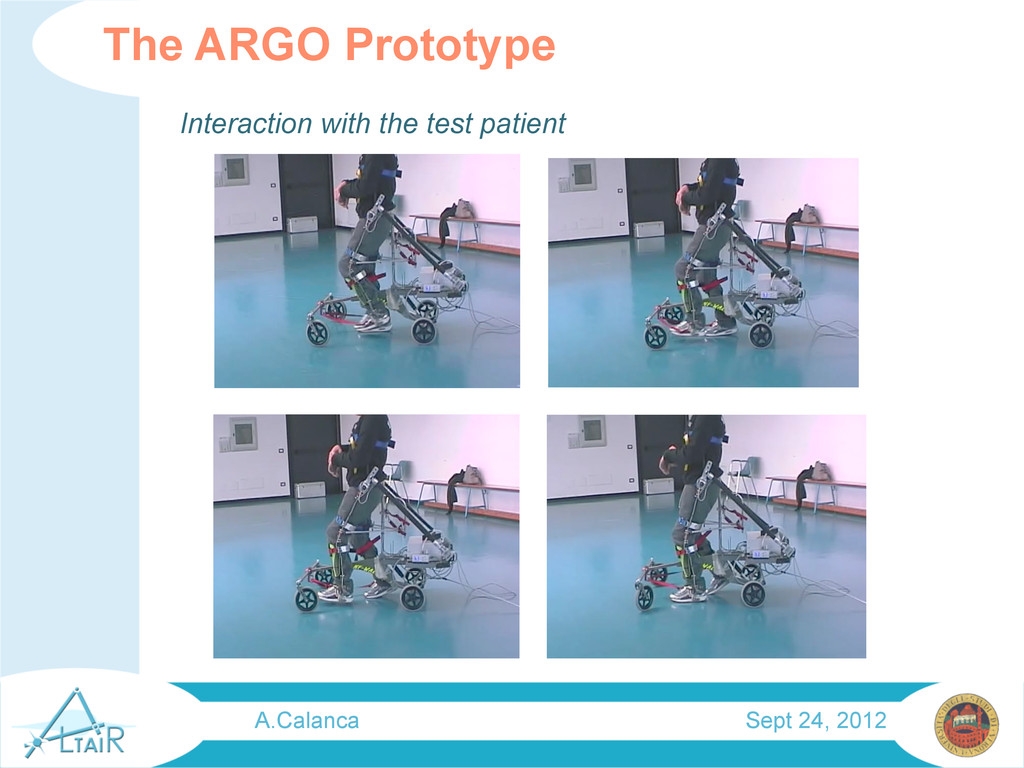
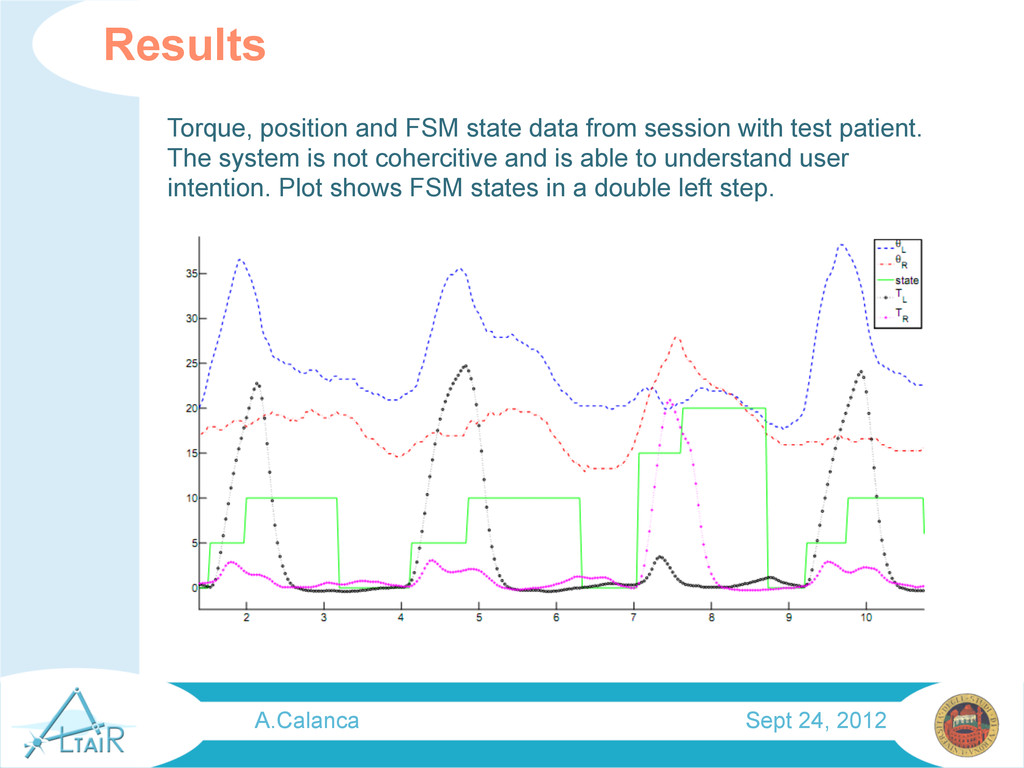
test patient. The system is not cohercitive and is able to understand user intention. Plot shows FSM states in a double left step. A.Calanca Sept 24, 2012
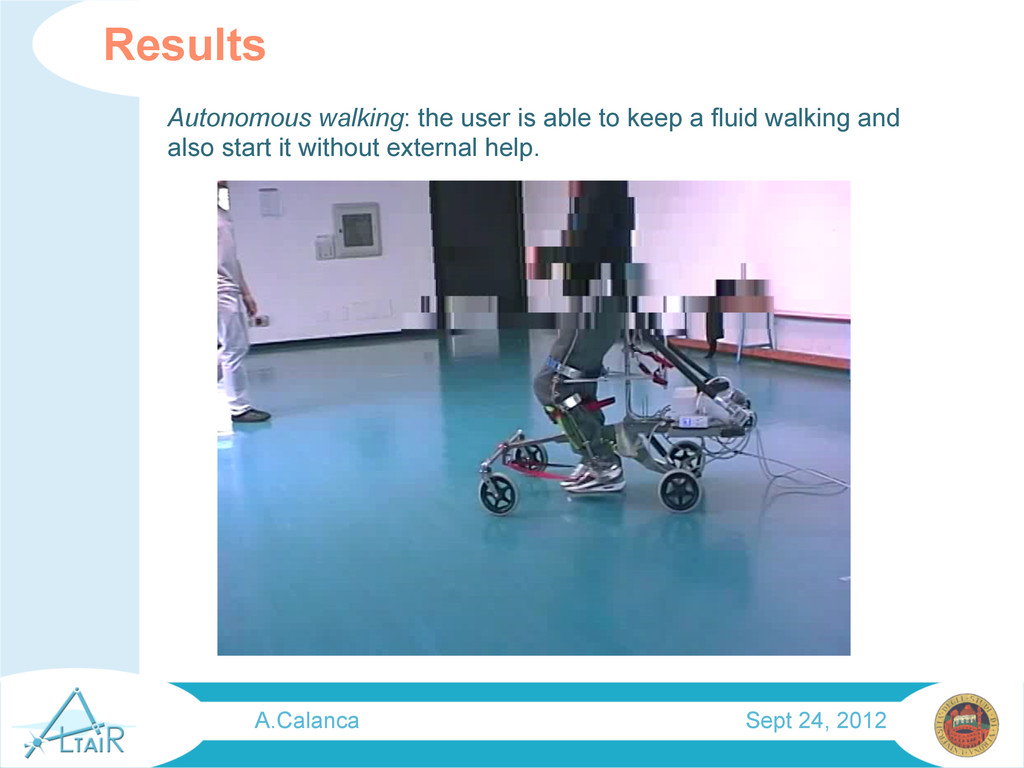
results. He was not only able to walk autonomously but also to improve his capability in passive orthosis usage. This can be due to the interaction with the orthosis that doesn’t make the user passive but follows his action plan. Patient action plan Vs Physiotherapist action plan A.Calanca Sept 24, 2012
CP patient for having more scientific evidence of benefits We propose to investigate if there is an improvement in patient condition. How much is the improvement? In wich aspects? Is it dependent from patient initial condition? How? What can be the best way to help patient? Are all still open question.
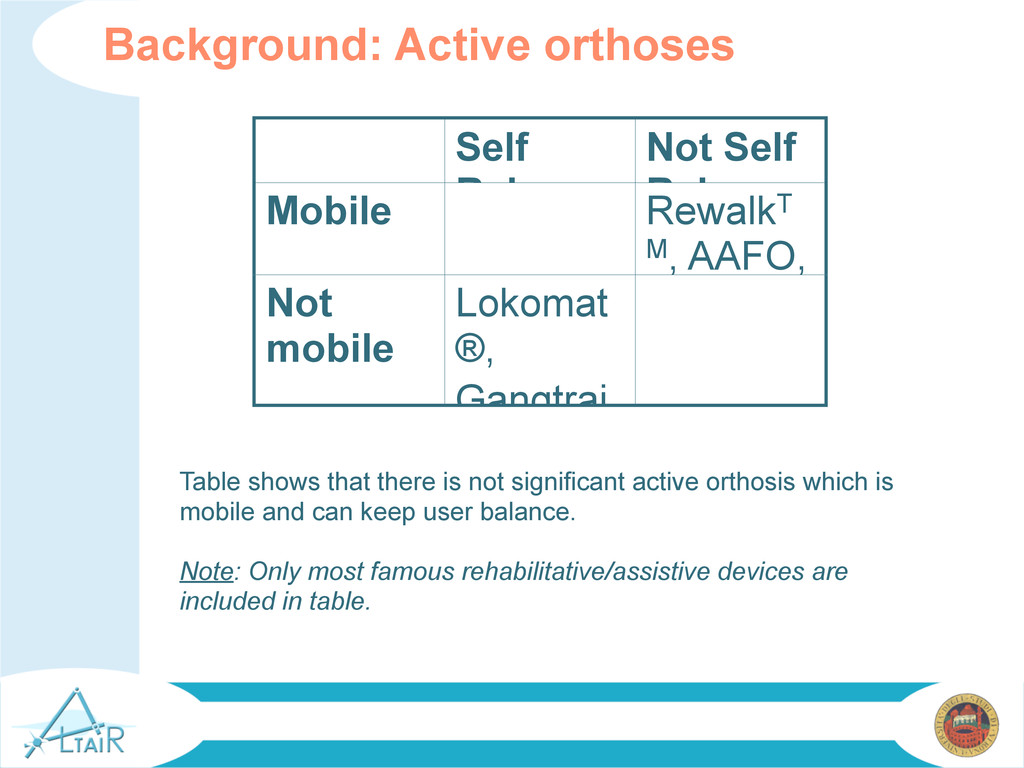
active orthosis which is mobile and can keep user balance. Note: Only most famous rehabilitative/assistive devices are included in table. Self Balance d Not Self Balance d Mobile RewalkT M, AAFO, WWH, HAL Not mobile Lokomat ®, Gangtrai nerTM,
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}