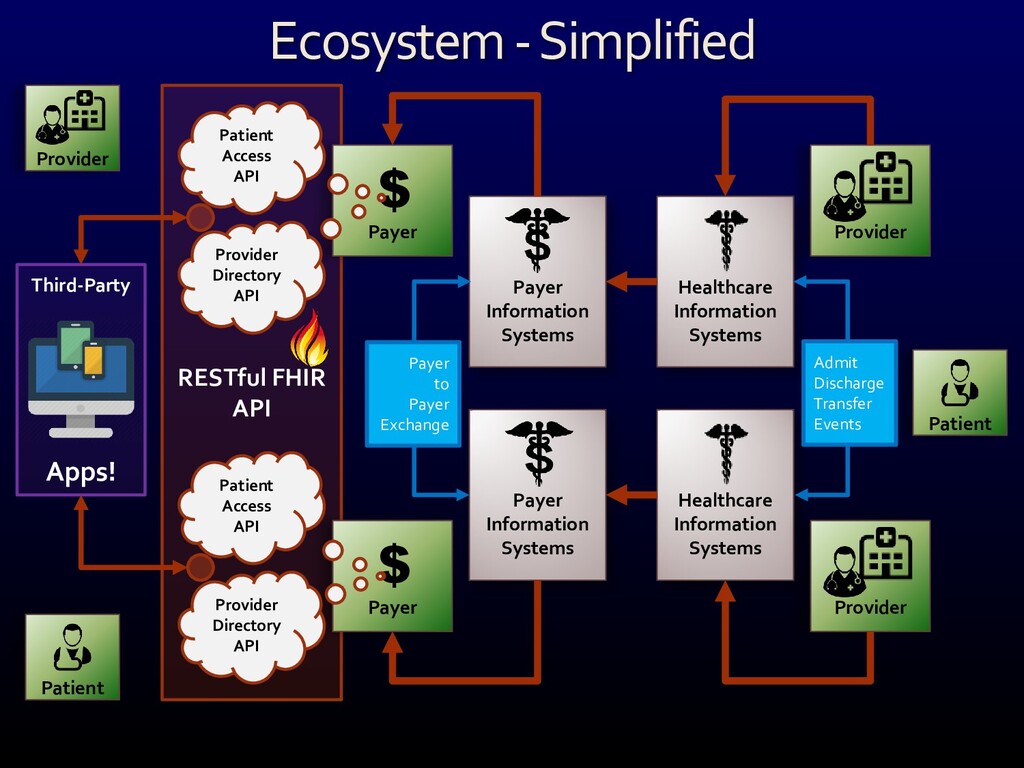
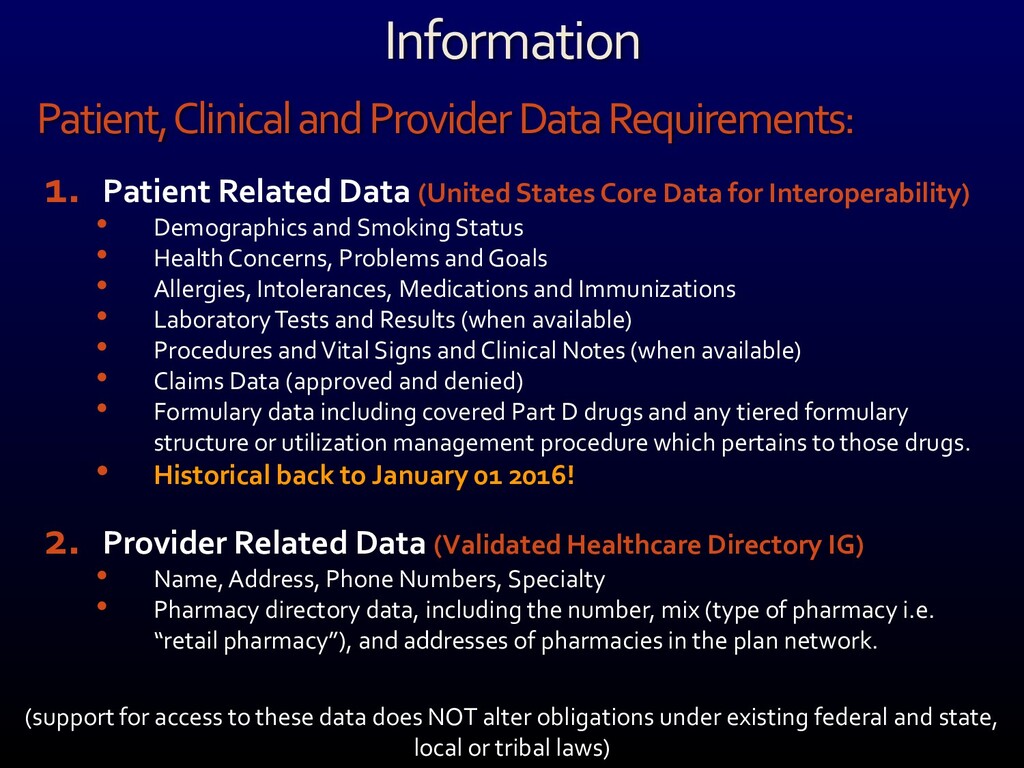
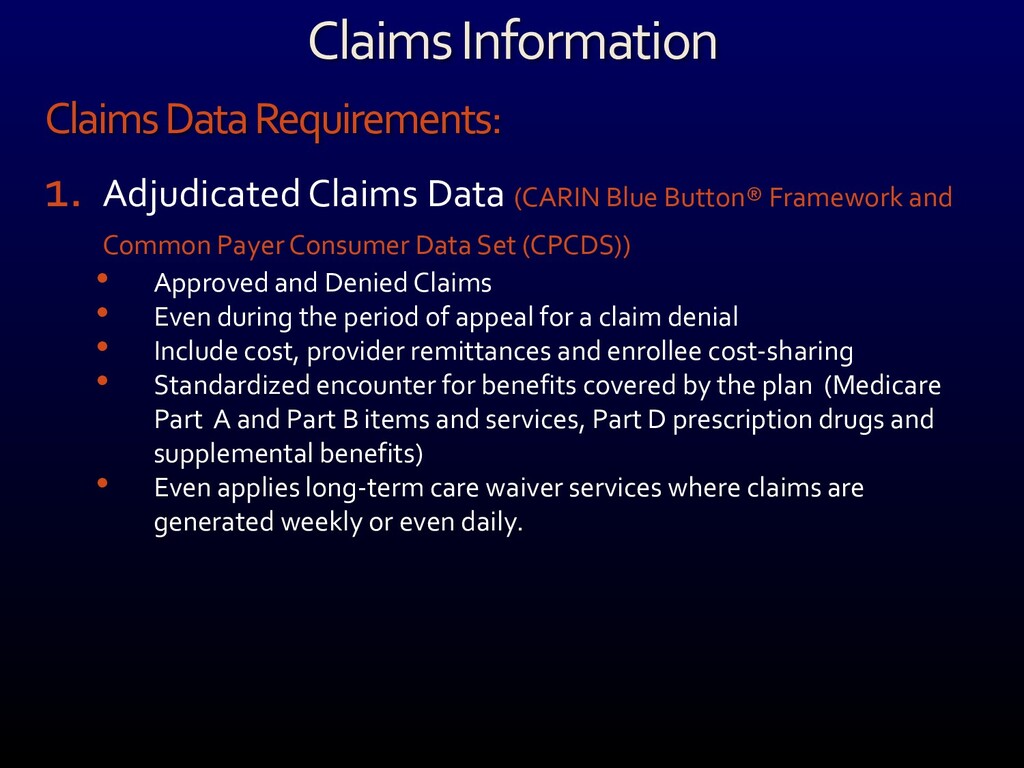
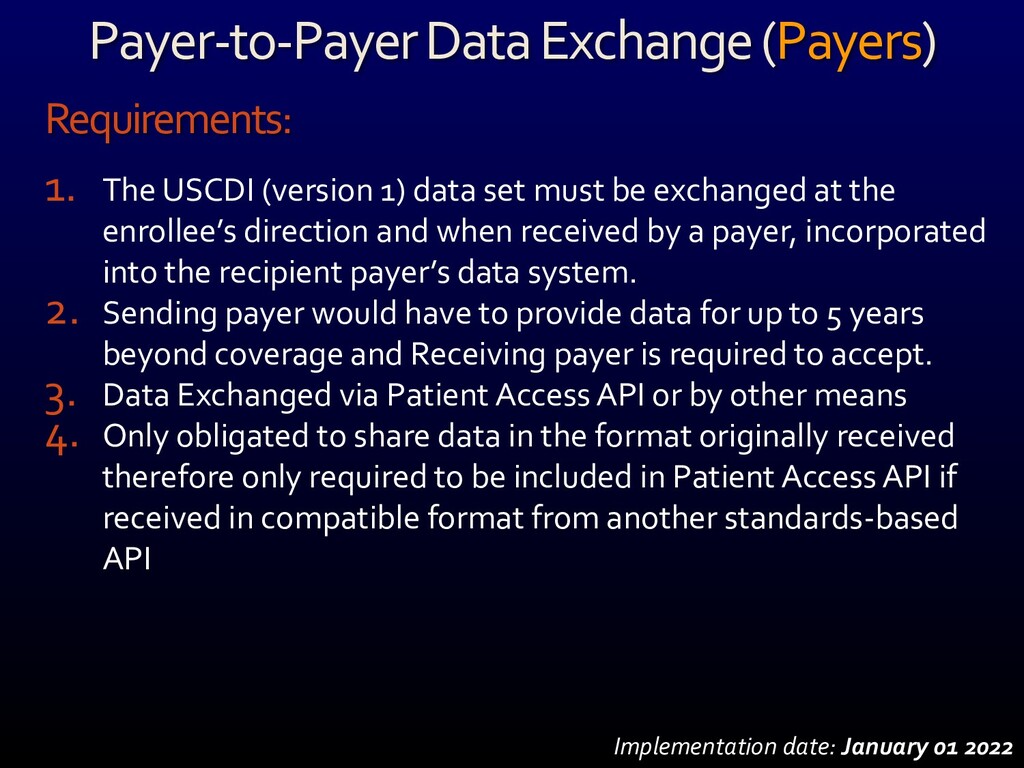
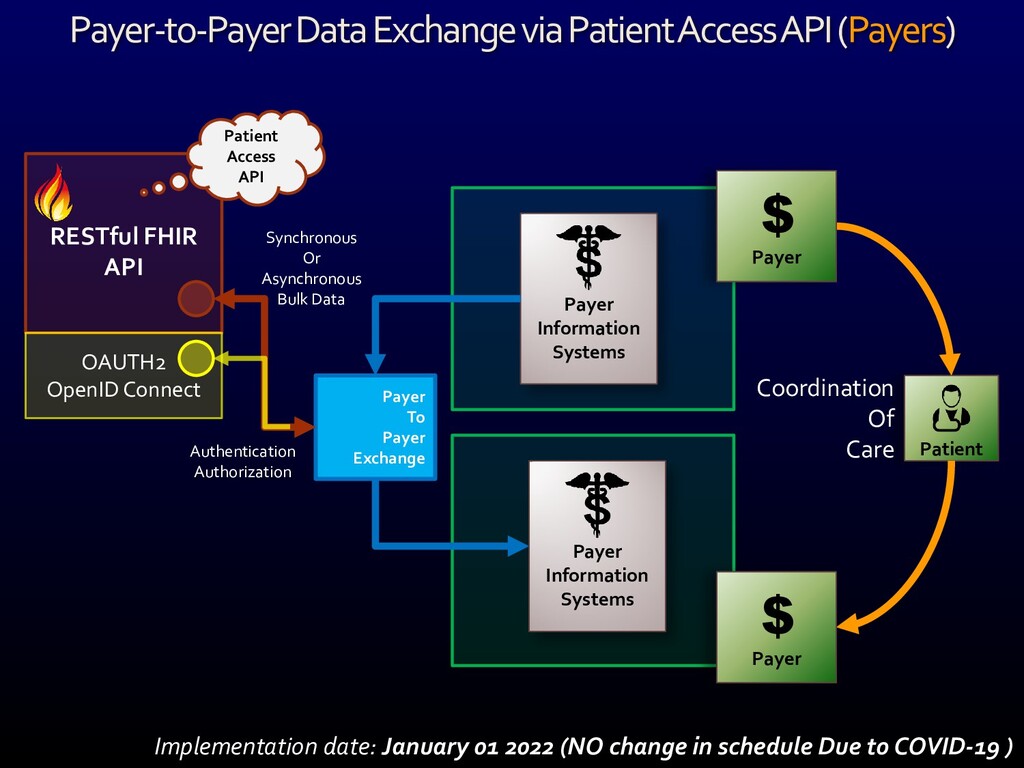
The Center for Medicare and Medicaid Services (CMS) has published their final “Interoperability and Patient Access Proposed Rule” that intends to “move the health care ecosystem in the direction of interoperability” and to “signal [our] commitment to the vision set out in the 21st Century Cures Act and Executive Order 13813 to improve the quality and accessibility of information that Americans need to make informed health care decisions, including data about health care prices and outcomes, while minimizing reporting burdens on affected health care providers and payers.”
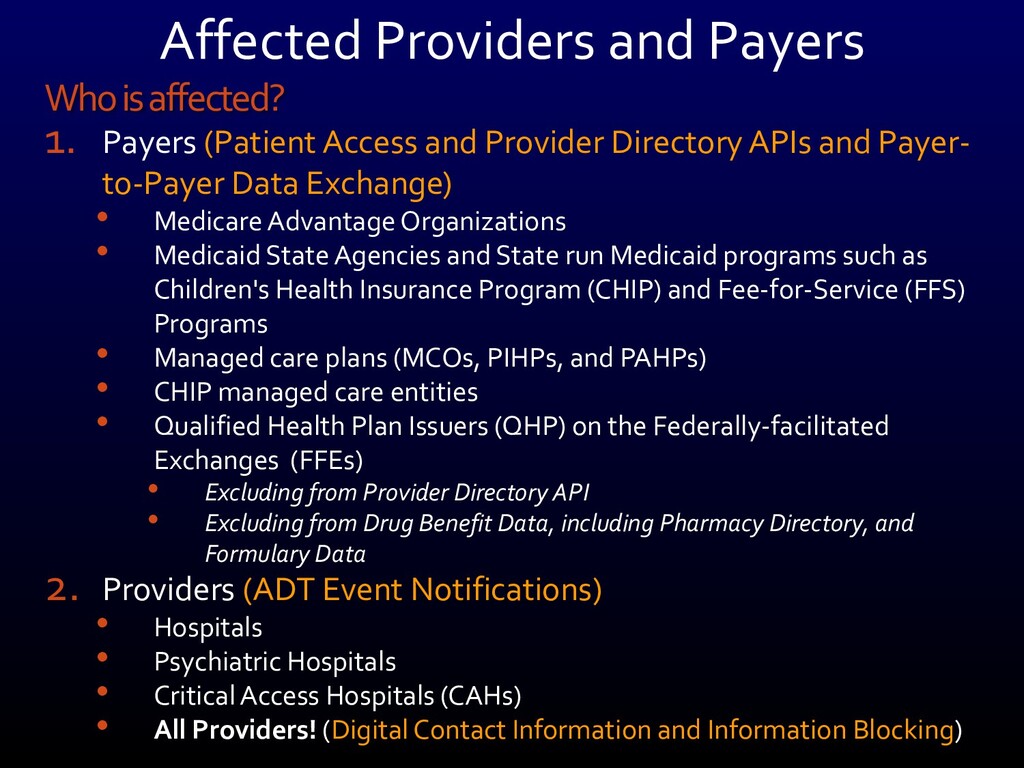
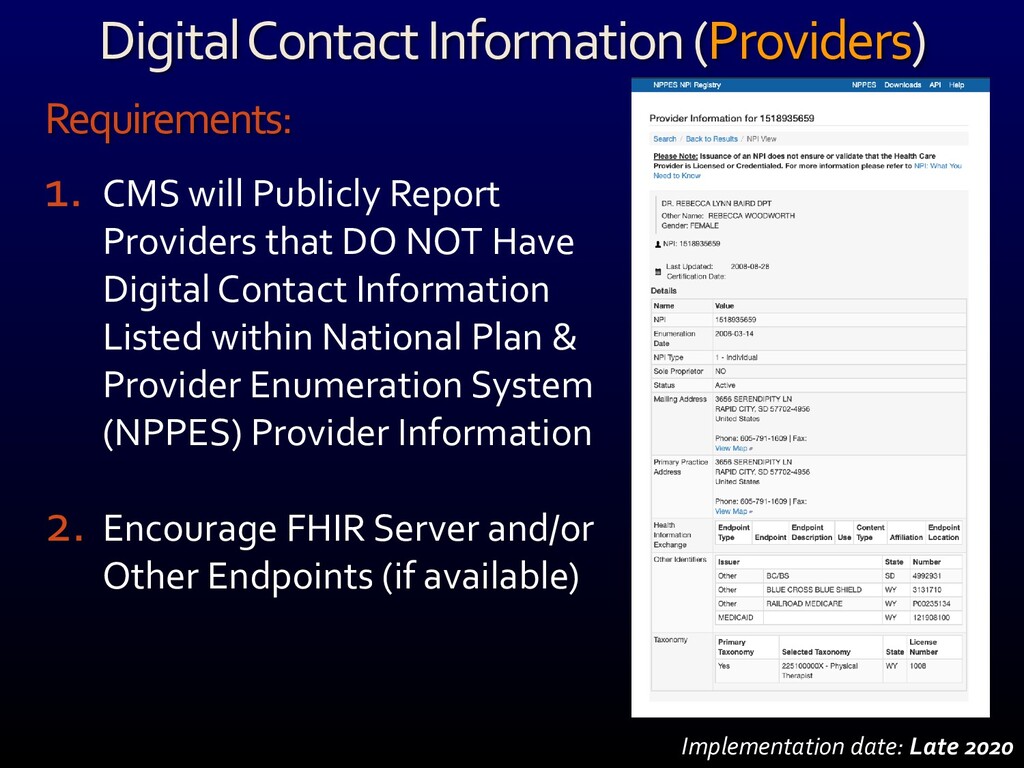
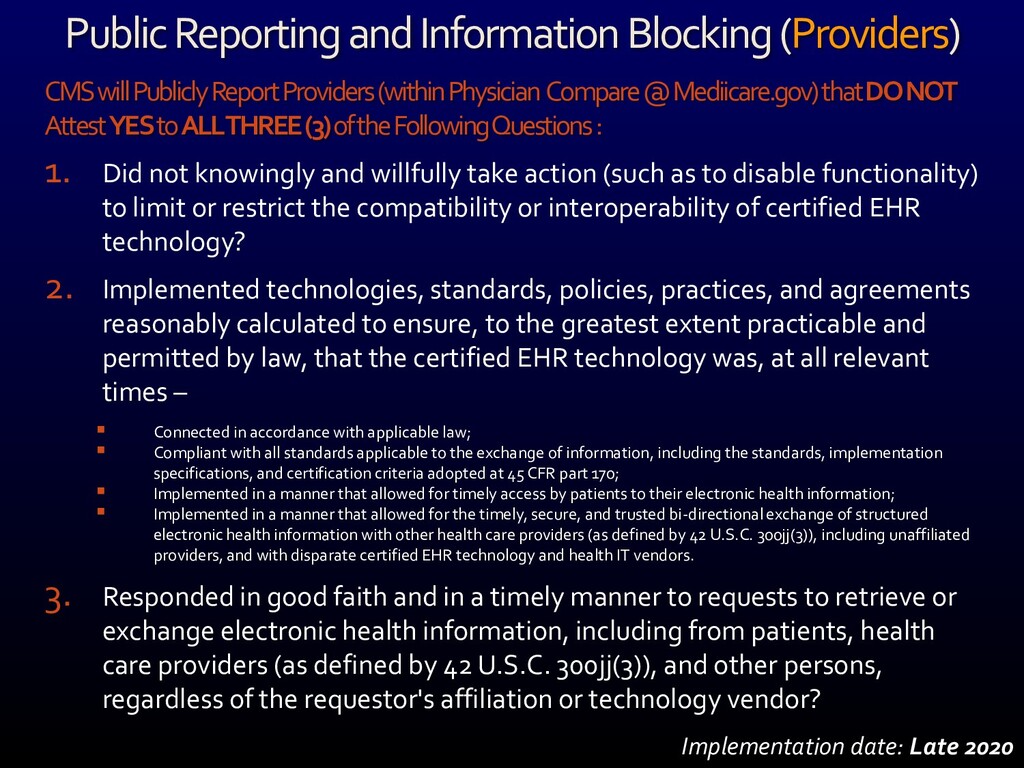
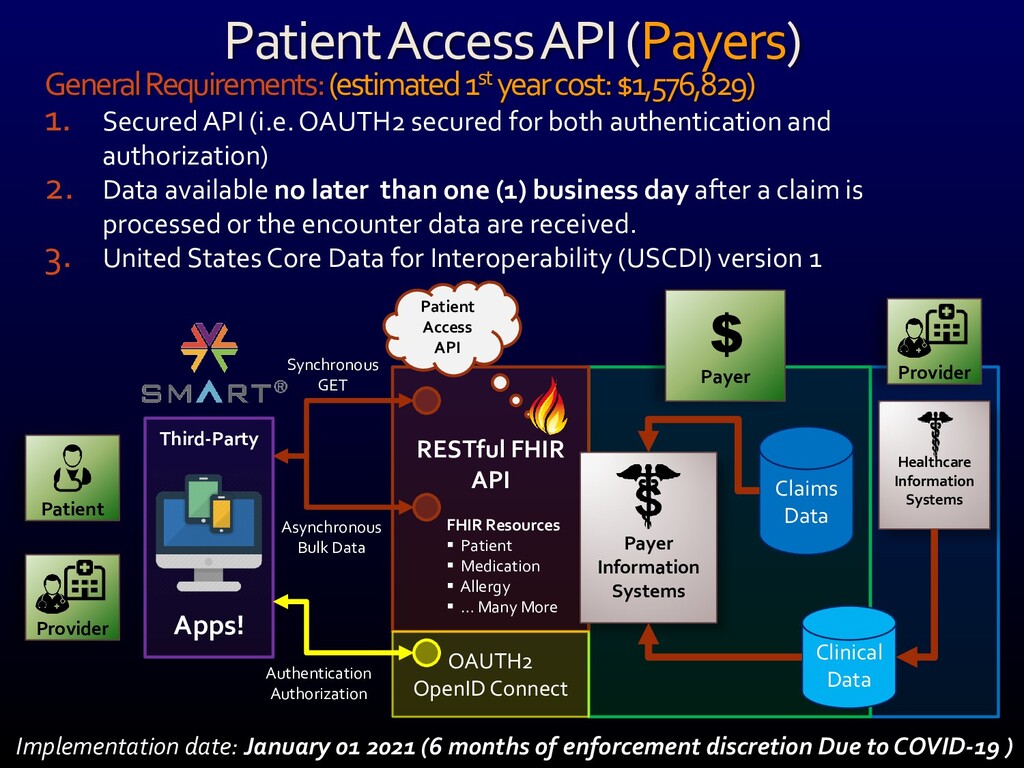
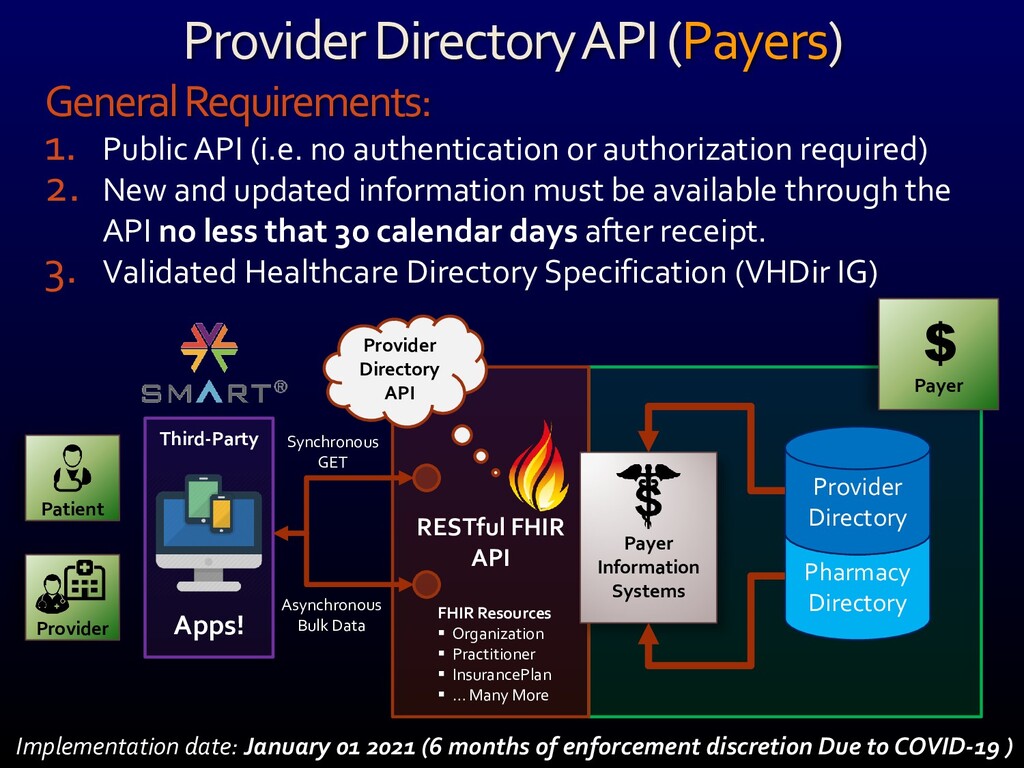
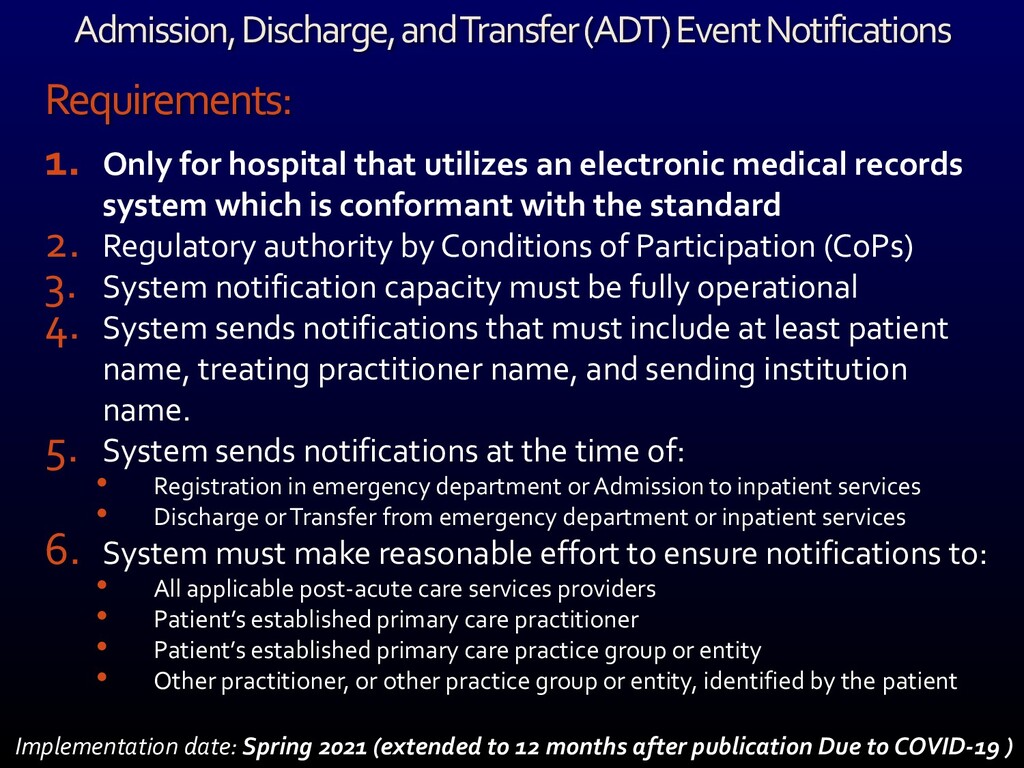
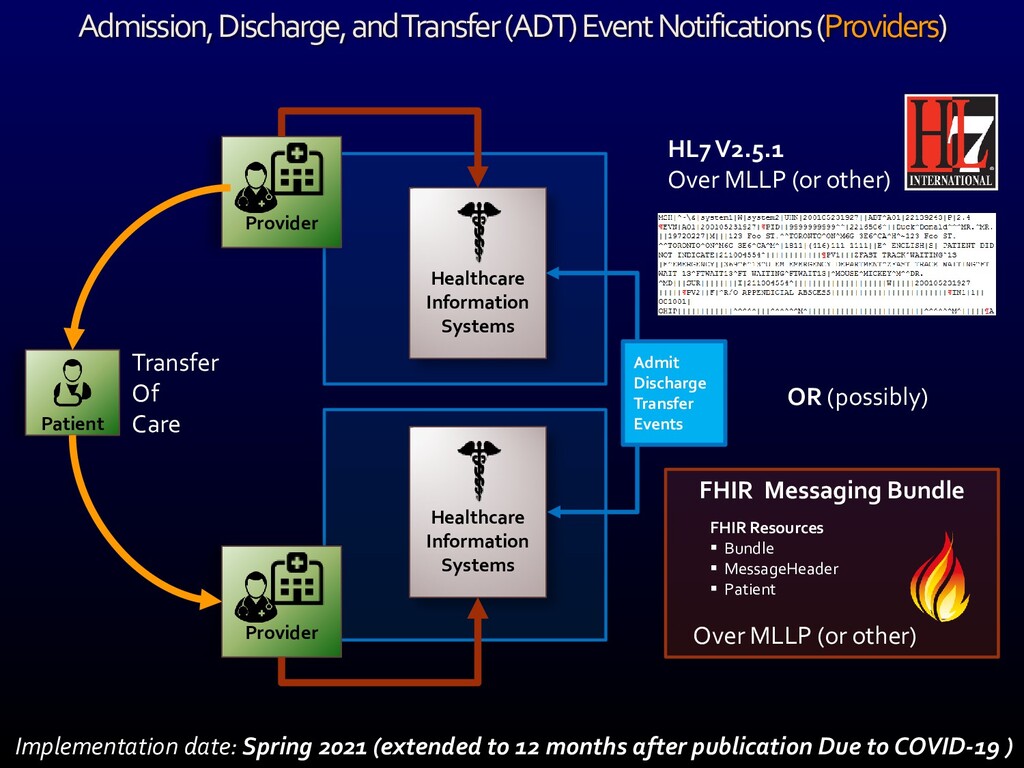
This rule comes with a pretty aggressive schedule of interoperability mandates starting this fall with the registration of digital contact information (including a FHIR API endpoint) and the implementation of a modern admit, discharge and transfer (ADT) event notification scheme as well as a comprehensive attestation to a number of Promoting Interoperability Program requirements.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}