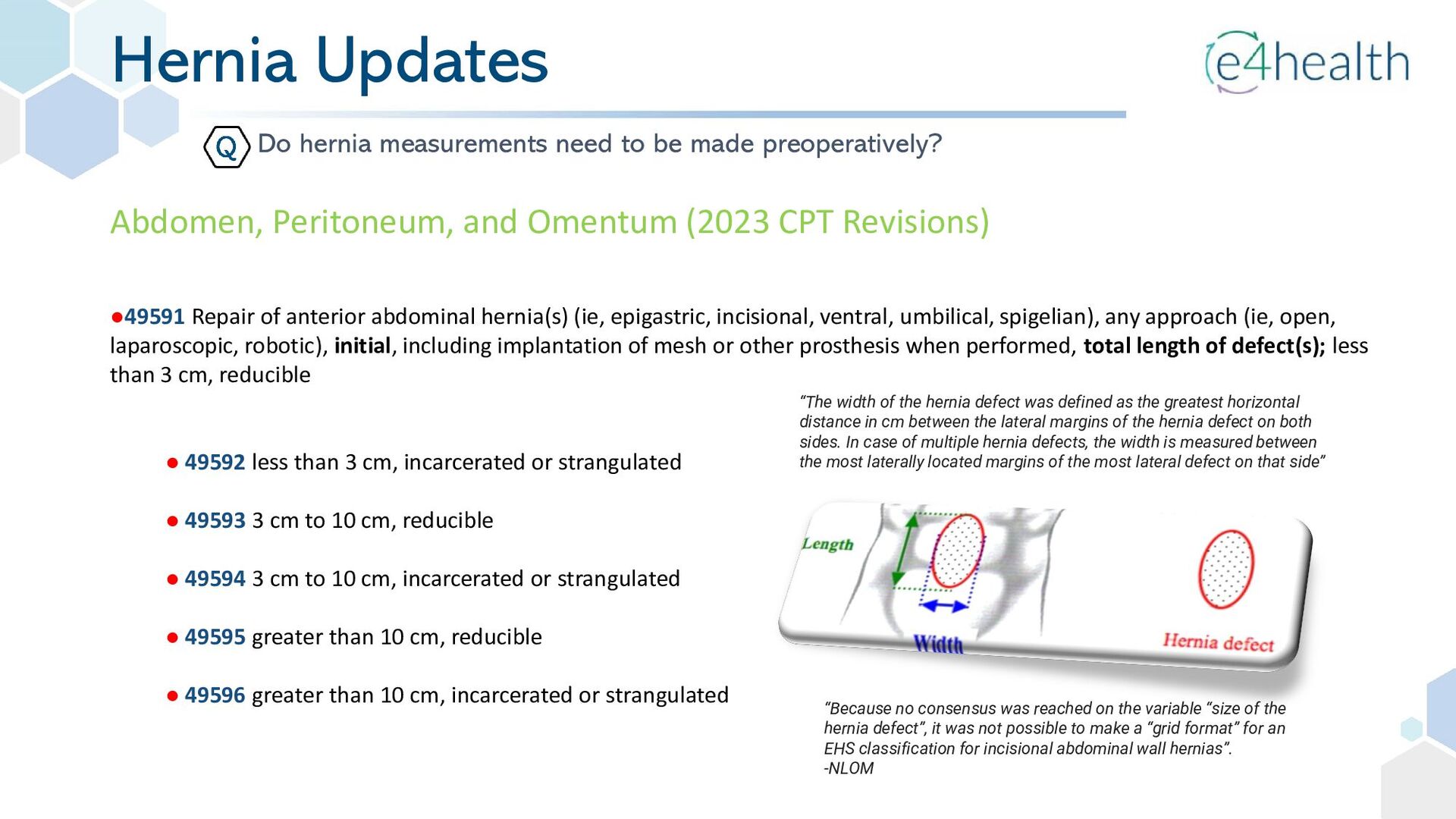
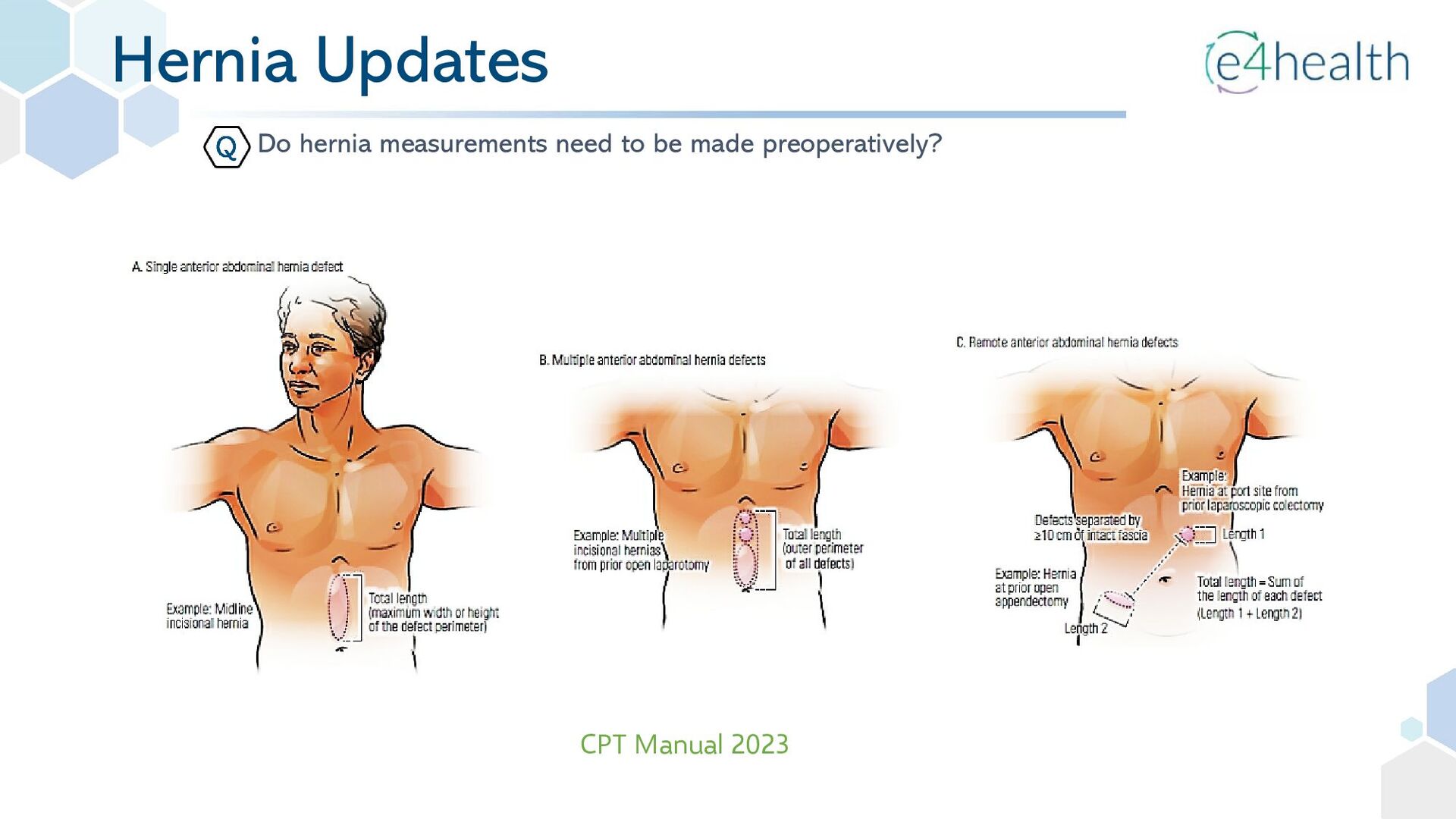
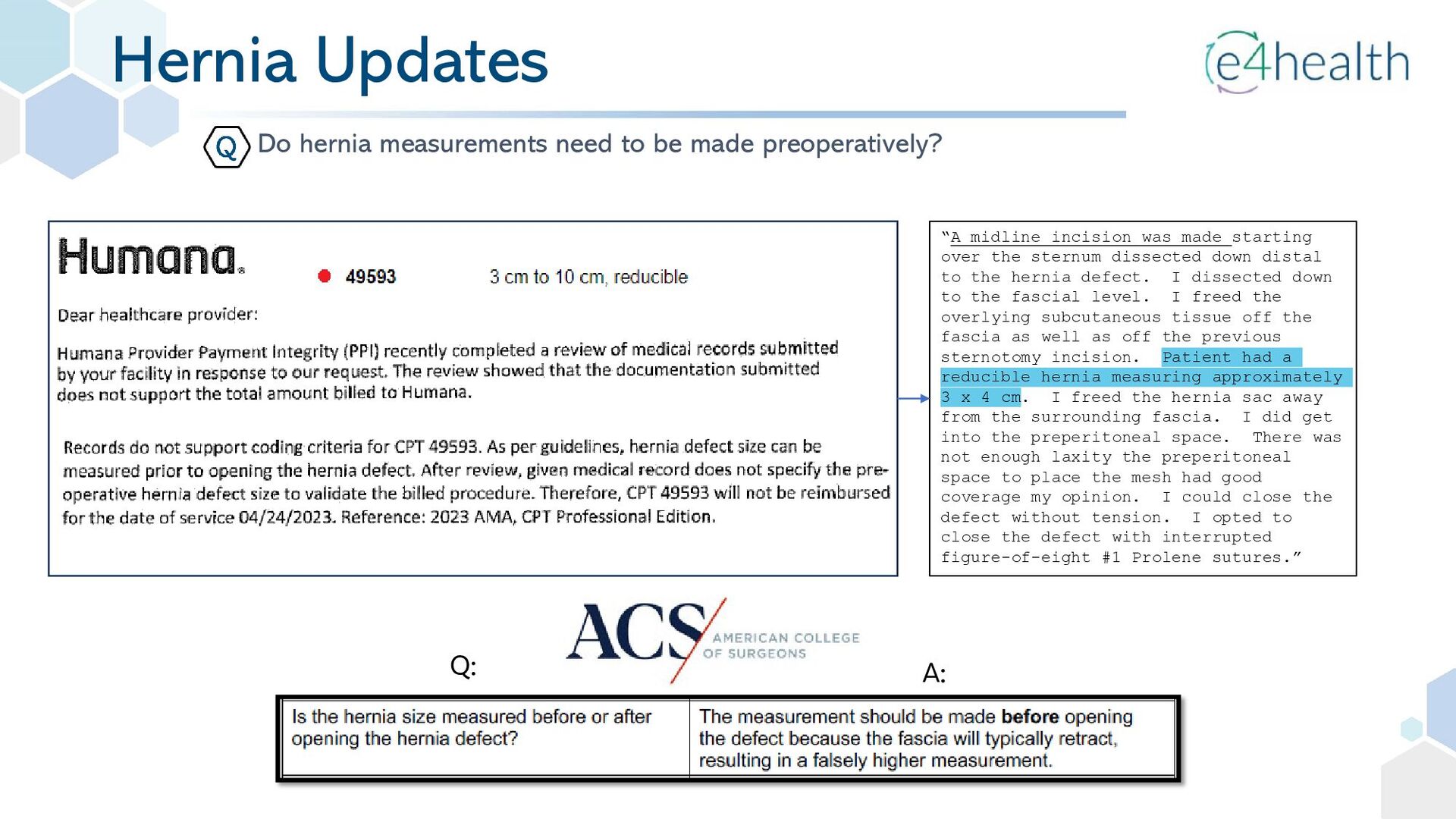
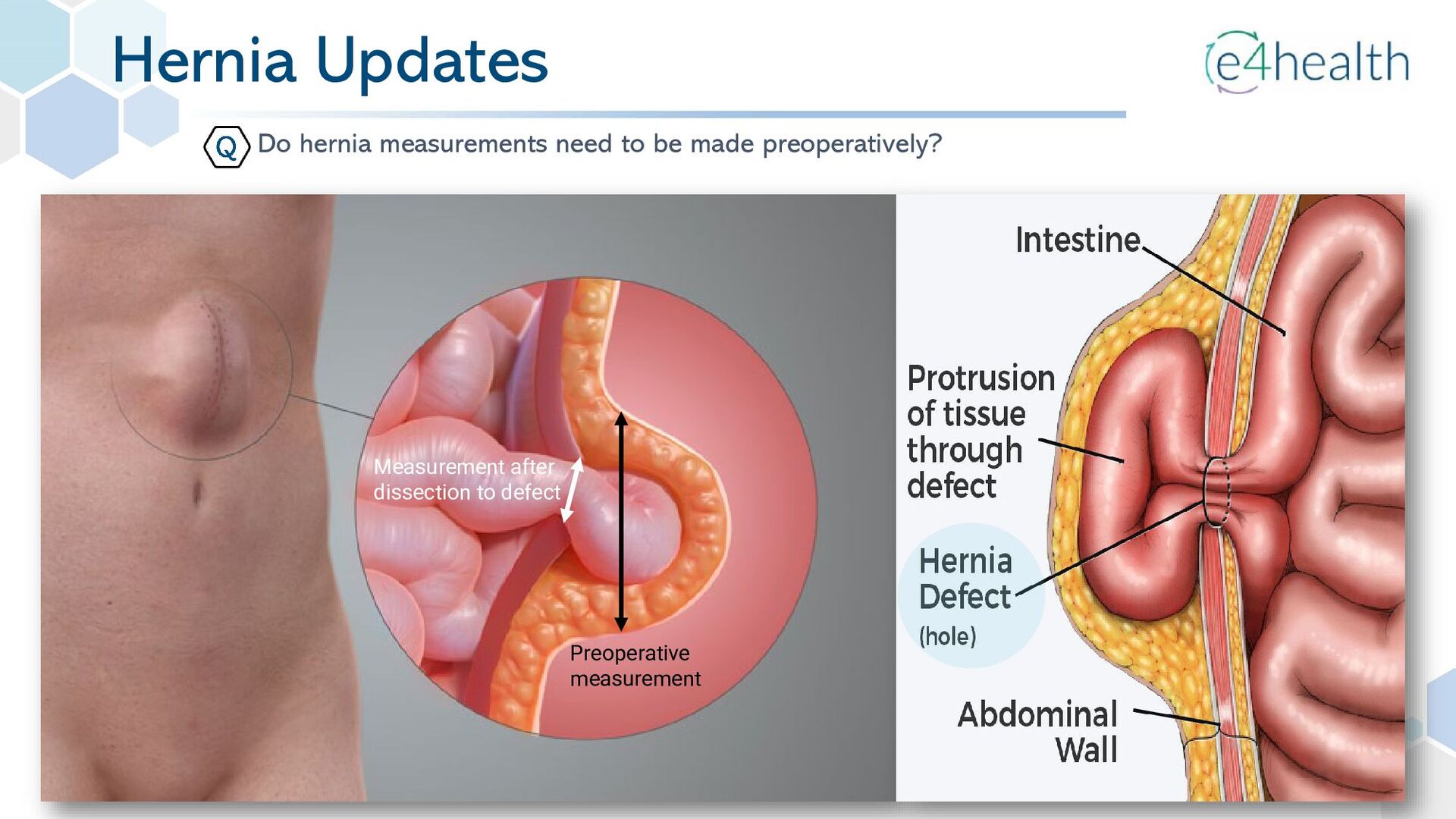
•49591 Repair of anterior abdominal hernia(s) (ie, epigastric, incisional, ventral, umbilical, spigelian), any approach (ie, open, laparoscopic, robotic), initial, including implantation of mesh or other prosthesis when performed, total length of defect(s); less than 3 cm, reducible • 49592 less than 3 cm, incarcerated or strangulated • 49593 3 cm to 10 cm, reducible • 49594 3 cm to 10 cm, incarcerated or strangulated • 49595 greater than 10 cm, reducible • 49596 greater than 10 cm, incarcerated or strangulated Abdomen, Peritoneum, and Omentum (2023 CPT Revisions) “The width of the hernia defect was defined as the greatest horizontal distance in cm between the lateral margins of the hernia defect on both sides. In case of multiple hernia defects, the width is measured between the most laterally located margins of the most lateral defect on that side” “Because no consensus was reached on the variable “size of the hernia defect”, it was not possible to make a “grid format” for an EHS classification for incisional abdominal wall hernias”. -NLOM
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}