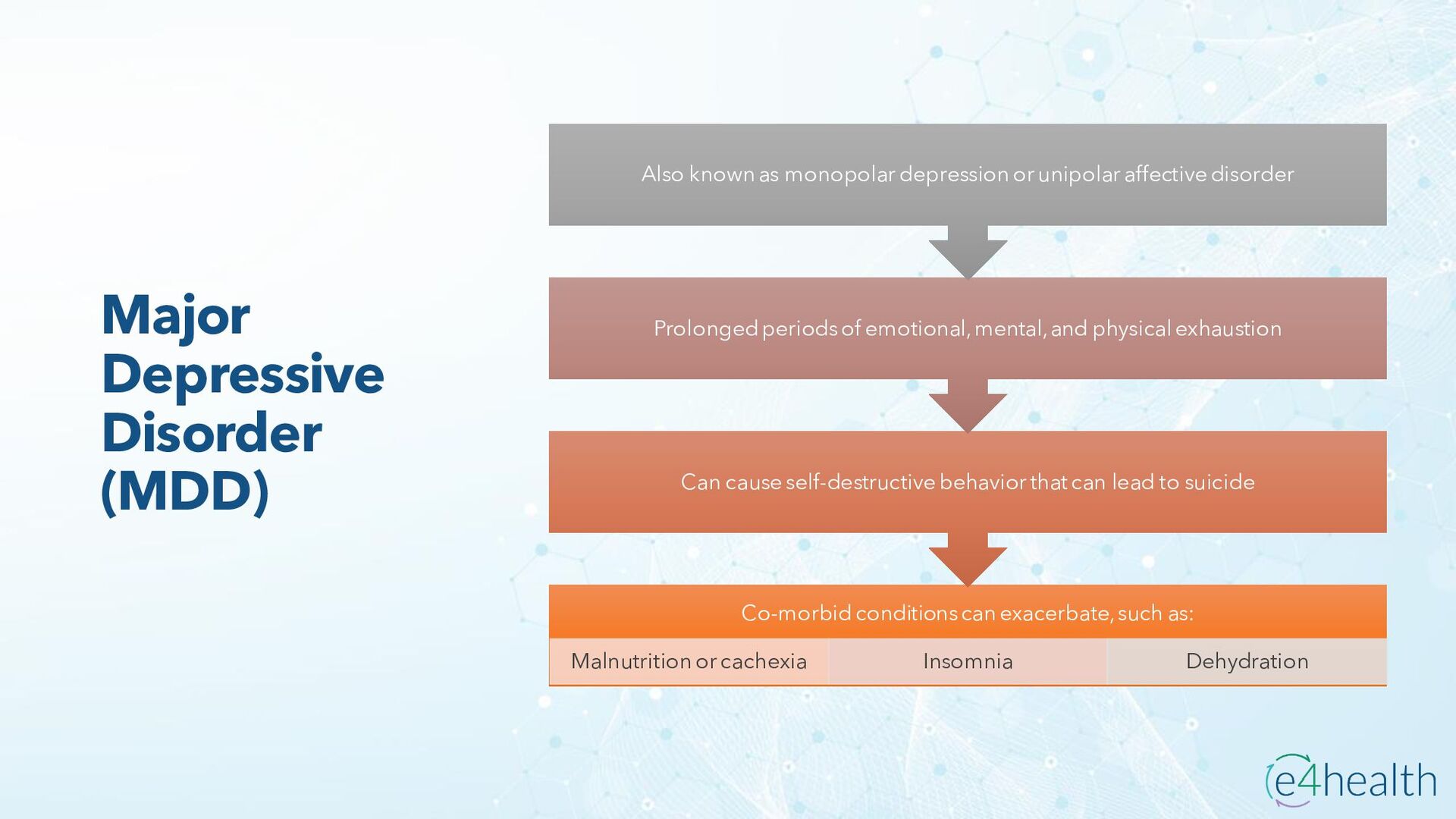
9-10 • A code has been created to identify depression (unspecified) and the narrative at category F32 was revised from Major depress ive disorder, single episode to "Depressive episode." This retitling brings back the WHO ICD-10 category title, and also brings the title into better alignment with all of what has been included in the category. The new code follows: • F32.A Depression, unspecified • Depression is a common mental health disorder. Approximately 30% of patients report symptoms of depression to their primary care providers; however, fewer than 10% of these patients have major depression. Although depression can begin at almost any age, it typically develops during a person's mid-teens, 20s, or 30s. When untreated, an episode of depression may last from 6 months to two years or more, and episodes tend to recur several times over a lifetime. • The exact etiology of depression is unclear; however, risk factors may include heredity, certain physical disorders, emotionally distressing events, changes in hormone levels, and side effects of certain drugs. • Symptoms of depression vary, and typically develop gradually over days or weeks. Symptoms may include anxiety, feelings of loneliness, irritability, sadness, poor concentration, poor hygiene, and loss of interest in activities that were once enjoyed. Some people have poor appetite while others overeat. Some become withdrawn, have difficulty sleeping or sleep more than usual, and some have thoughts of death and suicide. • Previously in ICD-10-CM, the default for Depression not otherwise specified (NOS) was code F32.9, Major depressive disorder, single episode, unspecified. However, this code did not separately capture the actual occurrence of depression not further specified, and statistically inflated the incidence of major depressive disorder.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}