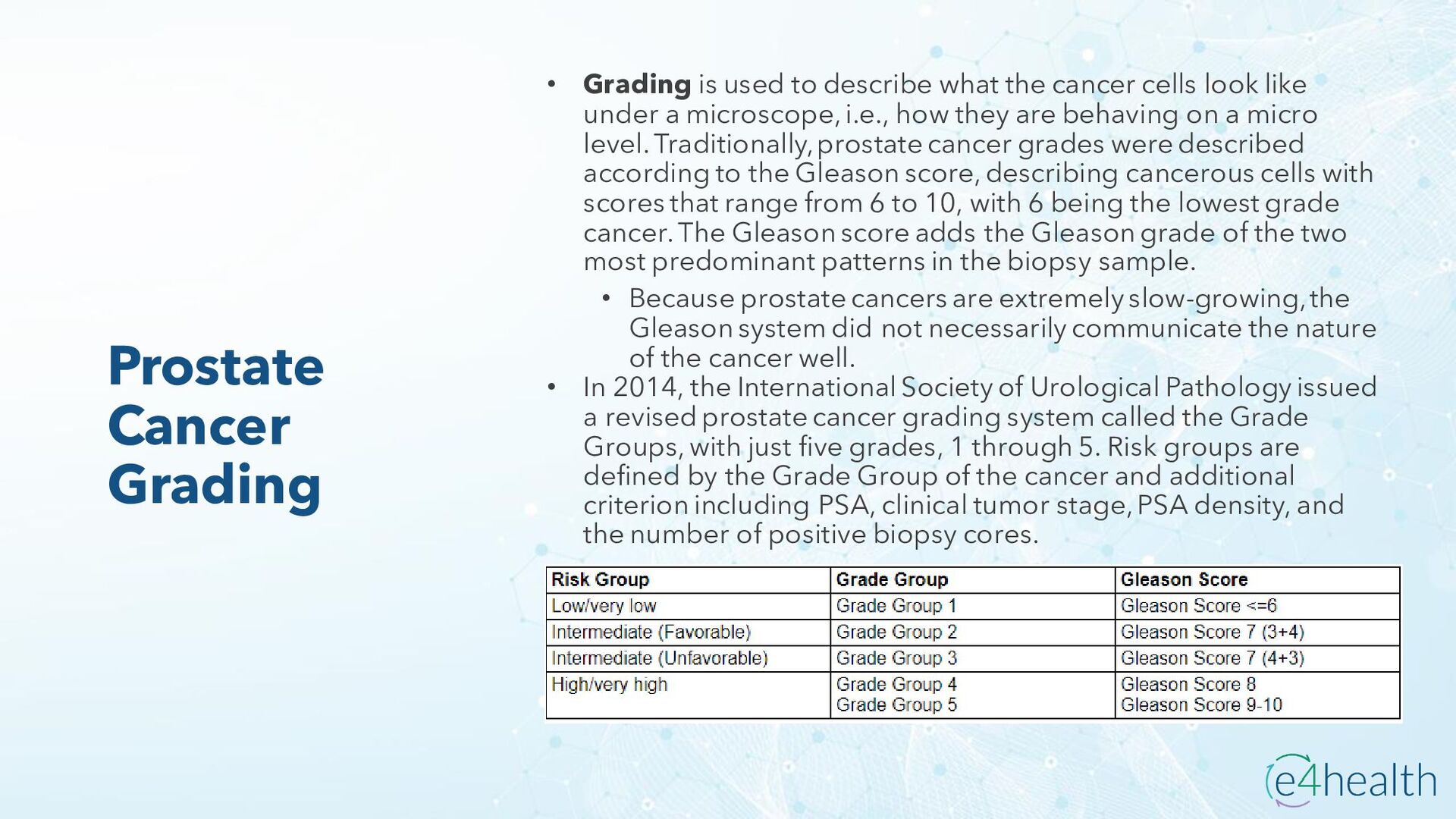
the cancer cells look like under a microscope, i.e., how they are behaving on a micro level. Traditionally, prostate cancer grades were described according to the Gleason score, describing cancerous cells with scores that range from 6 to 10, with 6 being the lowest grade cancer. The Gleason score adds the Gleason grade of the two most predominant patterns in the biopsy sample. • Because prostate cancers are extremely slow-growing, the Gleason system did not necessarily communicate the nature of the cancer well. • In 2014, the International Society of Urological Pathology issued a revised prostate cancer grading system called the Grade Groups, with just five grades, 1 through 5. Risk groups are defined by the Grade Group of the cancer and additional criterion including PSA, clinical tumor stage, PSA density, and the number of positive biopsy cores.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}