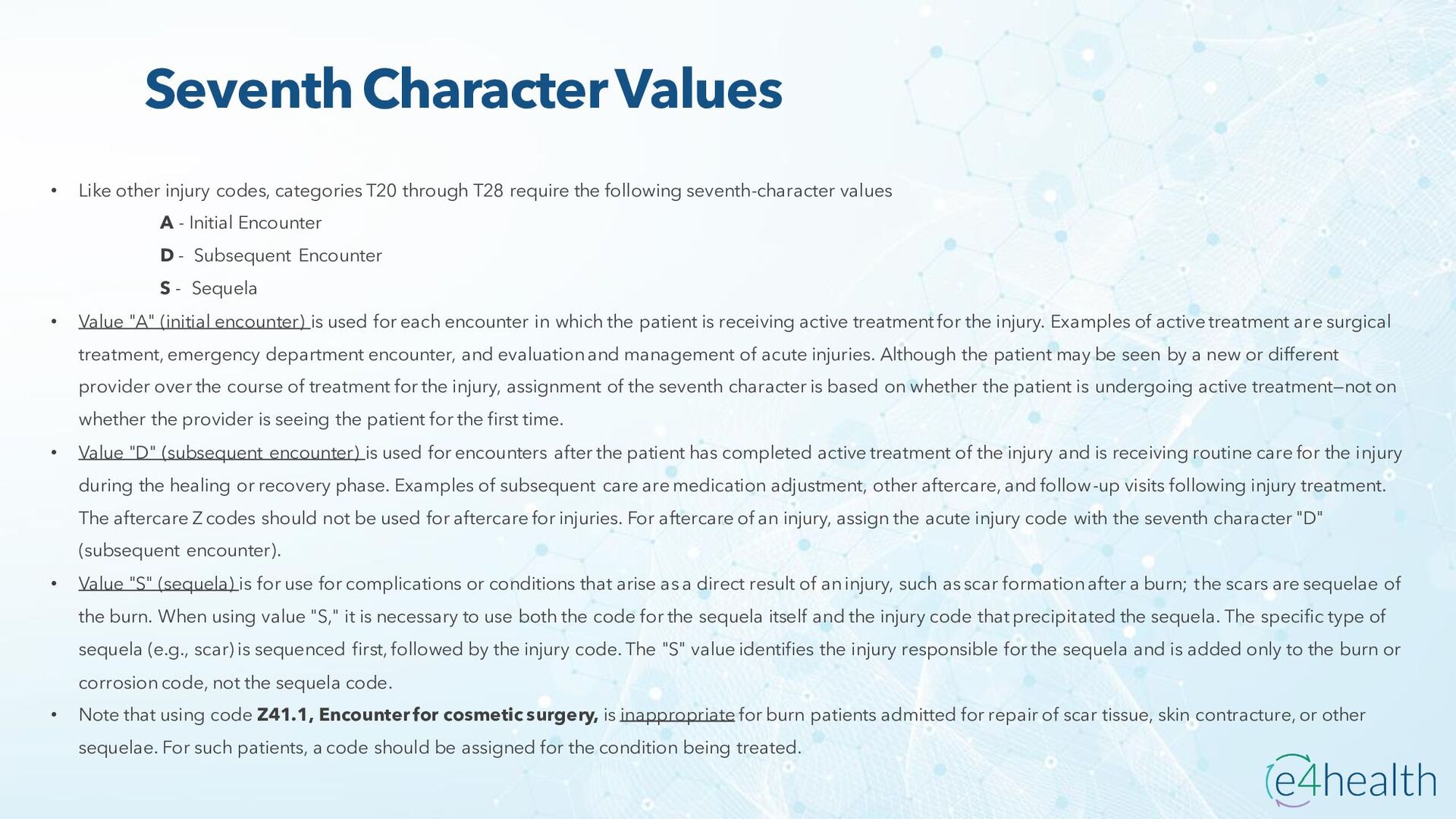
through T28 require the following seventh-character values A - Initial Encounter D - Subsequent Encounter S - Sequela • Value "A" (initial encounter) is used for each encounter in which the patient is receiving active treatment for the injury. Examples of active treatment are surgical treatment, emergency department encounter, and evaluation and management of acute injuries. Although the patient may be seen by a new or different provider over the course of treatment for the injury, assignment of the seventh character is based on whether the patient is undergoing active treatment—not on whether the provider is seeing the patient for the first time. • Value "D" (subsequent encounter) is used for encounters after the patient has completed active treatment of the injury and is receiving routine care for the injury during the healing or recovery phase. Examples of subsequent care are medication adjustment, other aftercare, and follow-up visits following injury treatment. The aftercare Z codes should not be used for aftercare for injuries. For aftercare of an injury, assign the acute injury code with the seventh character "D" (subsequent encounter). • Value "S" (sequela) is for use for complications or conditions that arise as a direct result of an injury, such as scar formation after a burn; the scars are sequelae of the burn. When using value "S," it is necessary to use both the code for the sequela itself and the injury code that precipitated the sequela. The specific type of sequela (e.g., scar) is sequenced first, followed by the injury code. The "S" value identifies the injury responsible for the sequela and is added only to the burn or corrosion code, not the sequela code. • Note that using code Z41.1, Encounter for cosmetic surgery, is inappropriate for burn patients admitted for repair of scar tissue, skin contracture, or other sequelae. For such patients, a code should be assigned for the condition being treated.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}