no benefit of PV • Vertos II study found effective pain relief after PV at acceptable costs. Kallmes DF, Comstock BA, Heagerty PJ et al. A randomized trial of vertebroplasty for osteoporotic spinal fractures. N Engl J Med 2009; 361(6):569-579. Buchbinder R, Osborne RH, Ebeling PR et al. A randomized trial of vertebroplasty for painful osteoporotic vertebral fractures. N Engl J Med 2009; 361(6):557-568 Klazen CA, Lohle PN, et al. Lancet. 2010 Sep 25;376(9746):1085-92.
Sham • neelde + cement ↔ neelde + longacting local anesthetic - PMMA - bupivacaina - marcaïne Concluded: - There is no statistically significant difference between patients treated with PV or the Sham procedure. - It is therefore inappropriate to offer this treatment in routine care. 2 Sham studies New Engl J Med
mixed “apples with pears” • statistical en methodologic flaws – included mix subacute + chronic fractures – no control group without intervention – absence of bone edema on MRI as a consistent inclusion criterium , which makes these 2 studies difficult to interpret clinically
referred by the general practitioner for back pain • all patients completed a clinical questionnaire • all patients underwent a physical examination • patients randomised to PV or conservative therapy
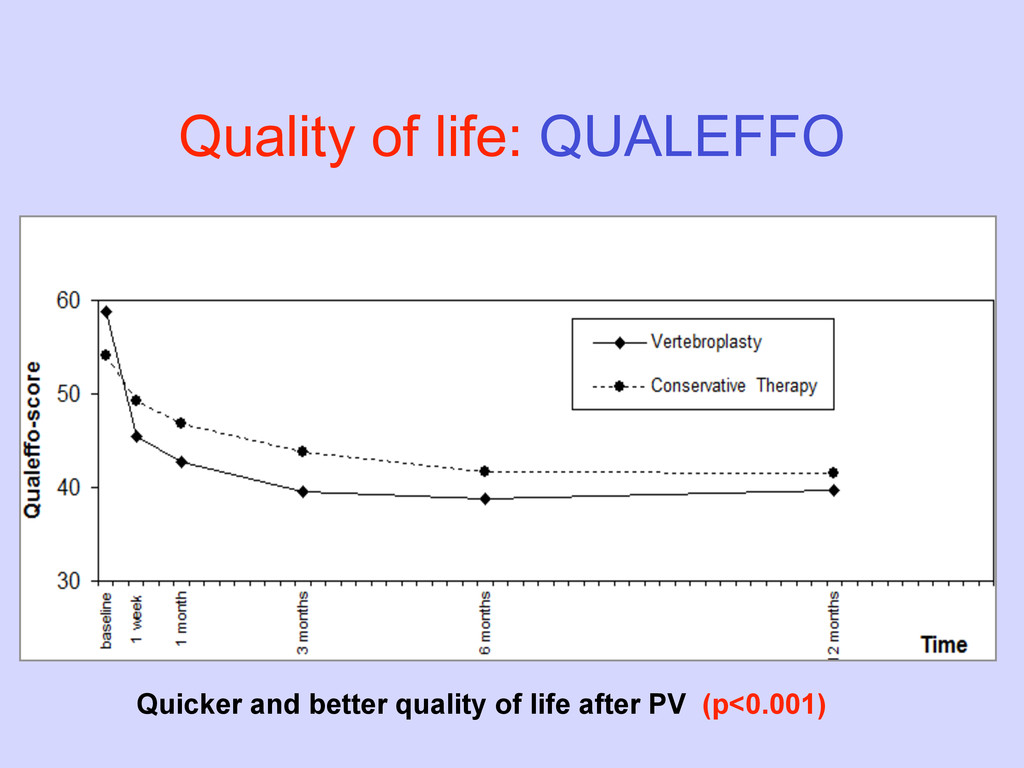
year 2. Secondary endpoint – cost effectiveness 1 month and 1 year – secondary VCFs during 1 year follow up 3. Third endpoint – quality of life (QUALEFFO)
a difference in total costs - at 1 month € 2,474 - at 1 year € 2,450 • However, significant difference in QALYs gained in favor of PV • This results in, cost-effectiveness ratio at 1 year of €22,685 per QALY gained → very much acceptable in the “Western world”
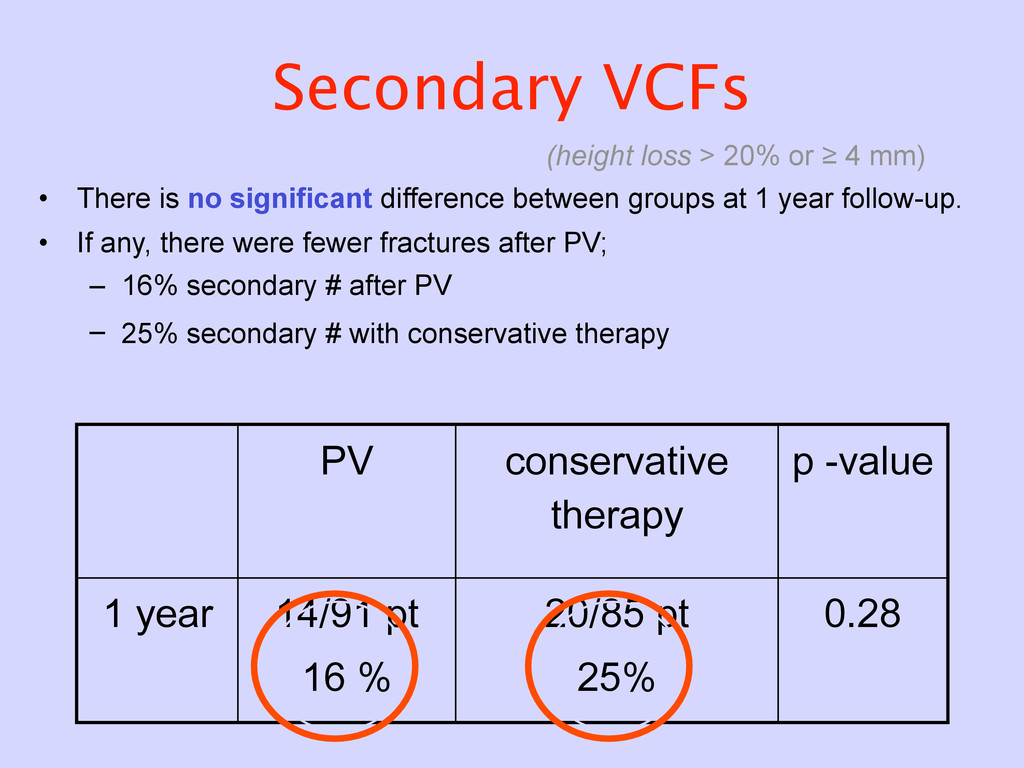
• There is no significant difference between groups at 1 year follow-up. • If any, there were fewer fractures after PV; – 16% secondary # after PV – 25% secondary # with conservative therapy PV conservative therapy p -value 1 year 14/91 pt 16 % 20/85 pt 25% 0.28
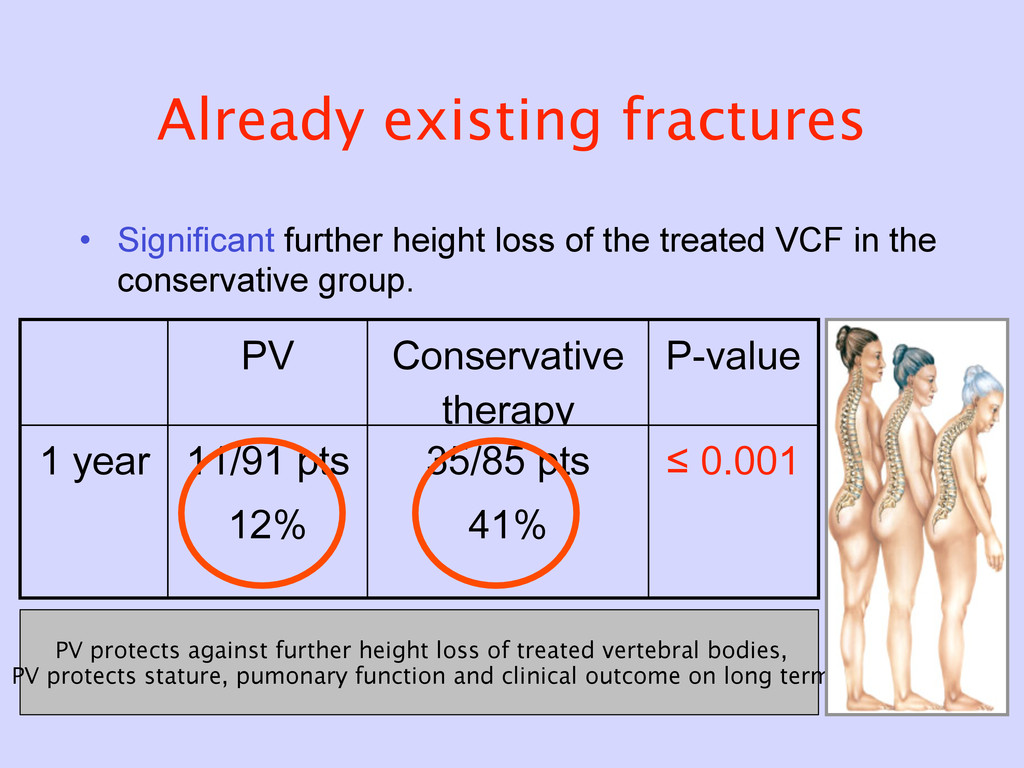
treated VCF in the conservative group. PV Conservative therapy P-value 1 year 11/91 pts 12% 35/85 pts 41% ≤ 0.001 PV protects against further height loss of treated vertebral bodies, PV protects stature, pumonary function and clinical outcome on long term
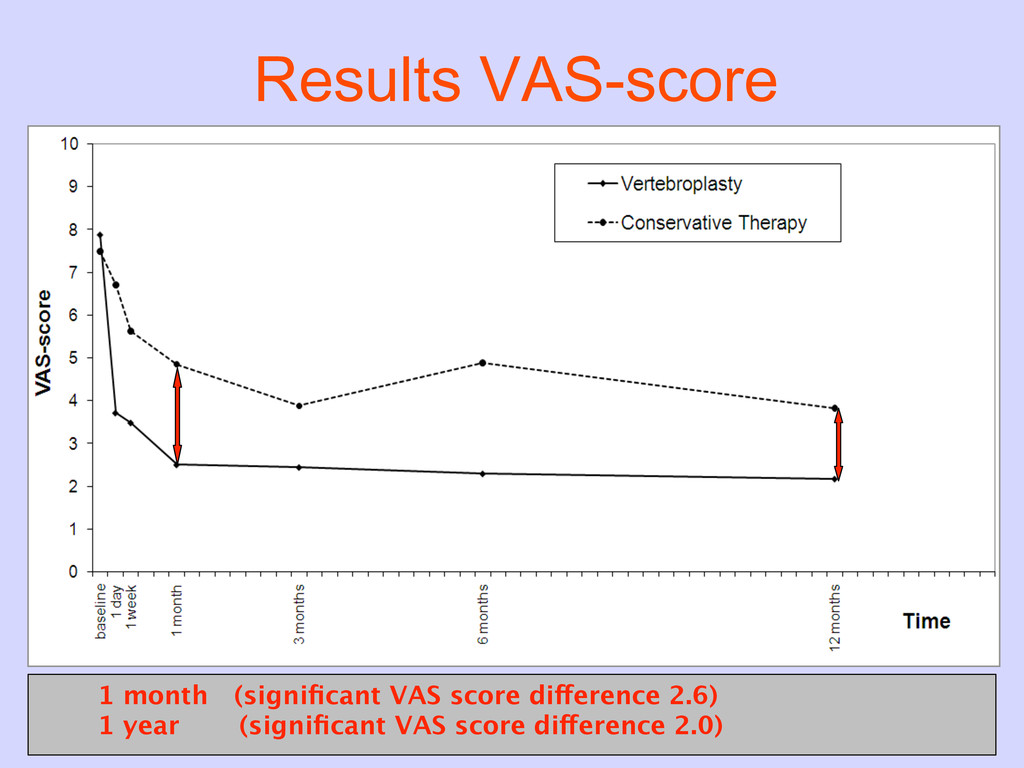
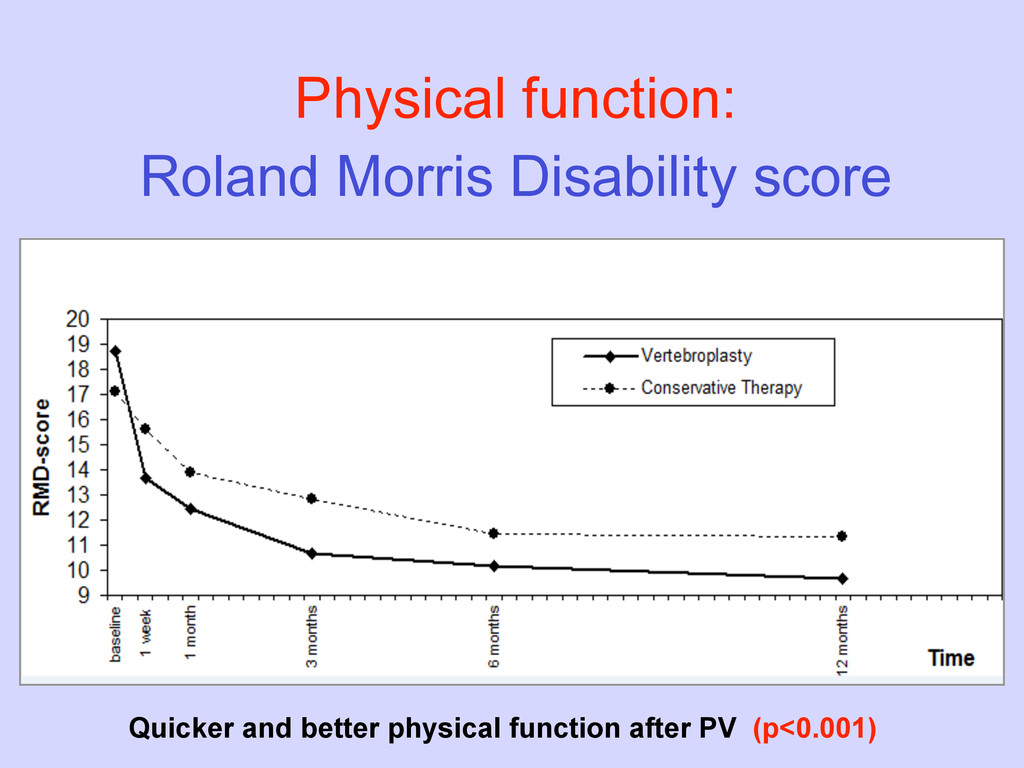
with an acute osteoporotic VCF and ungoing pain, PV is effective and safe. • Pain relief after PV is immediate, sustained during one year and significant better compared to conservative therapy, at acceptable costs.
more pragmatic study provides the clinician with directly applicable information on how to best treat the patient. • 2 Sham studies, lacked a control group without intervention and the best treatment option remains unclear for the clinician.
→ harm and damage • Vertos II, The Lancet → showed the power of PV • but it is not enough, since – Evidence Based Medicine demands high level of evidence – Health Insurance Companies know how to abuse it… • There is a difference in Level of Evidence between – two Sham studies = 1a level of evidence – Vertos II = 1b level of evidence we have to act again…
insurances to convince them to continue to reimburse PV • authors submitted letters to the editor and commentaries about the Sham studies and Vertos II – Gangi + Clark – Anselmetti – Murphy – Waldlaw + Van Meirhaeghe – Toms ,……………..critical views and comments. • but I believe, the only real solution to the problem is… to obtain Level of Evidence : 1a
versus the Sham intervention in selected patients with an acute osteoporotic VCF using the strict inclusion criteria as in Vertos II. • osteoporotic VCF, VAS score > 5 • local back pain < 6 weeks • bone edema on MRI Vertos IV ! randomized for PV or Sham intervention
study + strict inclusion criteria – Australia (1) – The Netherlands (4) • Financial support come from Dutch government + Company • The sample size calculated (using G-Power) – 142 patients are required for this study – we assume a withdrawal rate of 20% – 180 patients will be enrolled, 90 in each group. – conform Kallmes we expect a 1.5 point difference in pain relief, measured by VAS score. Vertos IV
March 2011 • expect enrollment 180 patients in 1 year (5 centers) • believe first publication in 2-3 years I hope to share with you our preliminary results much sooner, next year, here at this symposium in Paris! more information on Vertos IV in Trial registration http://www.clinicaltrials.gov September 2010 Vertos IV
March 2011 • expect enrollment 180 patients in 1 year (5 centers) • believe first publication in 2-3 years I hope to share with you our preliminary results much sooner, next year, here at this symposium in Paris! more information on Vertos IV in Trial registration http://www.clinicaltrials.gov September 2010 Thank you for your attention Vertos IV
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}