off’ - this term is outdated. Up to 15% of chest pain presentations to the ED will have ER. More common <50yrs, less common >70yrs. Physiological basis remains poorly understood. Historically thought to be benign. In the past 20 years multiple studies have shown a link to threatening arrhythmia and sudden cardiac death (SCD). Risk stratification remains challenging & controversial, although increasingly less so.
that a new definition was urgently needed. It proposed the below criteria, which subsequently was reiterated by a further consensus meeting in 2016; ERP is present if the following criteria are met; There is end-QRS notch or slur on the downslope of a prominent R-wave. If there is a notch, it should lie entirely above the baseline. The onset of a slur must also be above the baseline. J-point is >0.1mV in 2 or more contiguous leads, excluding v1-v3. QRS duration is <120ms. ST elevation in the absence of a notched or slurred J-point should not be described as ER. a. b. c. Macfarlane et al (2015) Antzelevitch et al (2016)
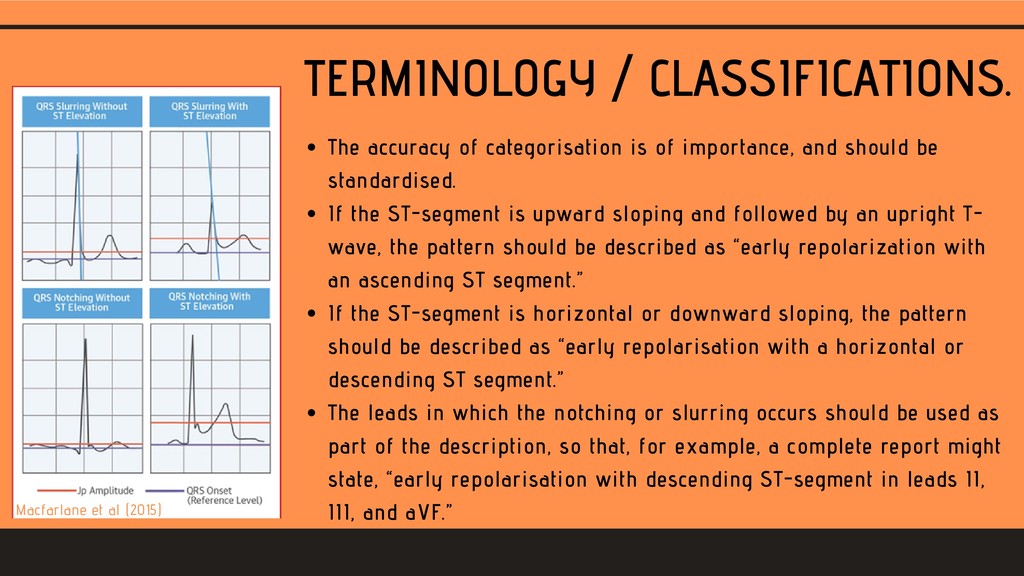
and should be standardised. If the ST-segment is upward sloping and followed by an upright T- wave, the pattern should be described as “early repolarization with an ascending ST segment.” If the ST-segment is horizontal or downward sloping, the pattern should be described as “early repolarisation with a horizontal or descending ST segment.” The leads in which the notching or slurring occurs should be used as part of the description, so that, for example, a complete report might state, “early repolarisation with descending ST-segment in leads II, III, and aVF.” Antzelevitch et al (2016) Macfarlane et al (2015)
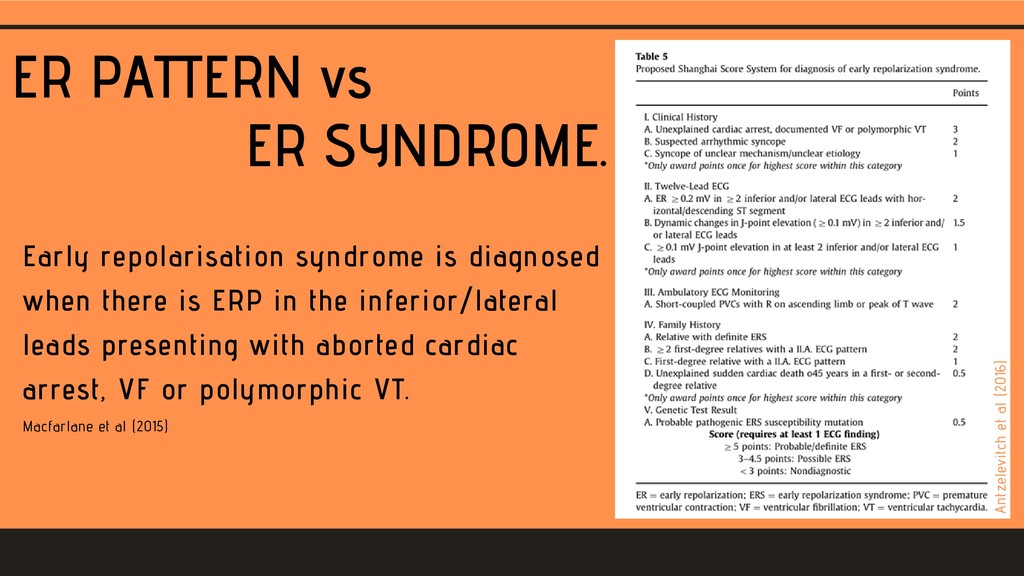
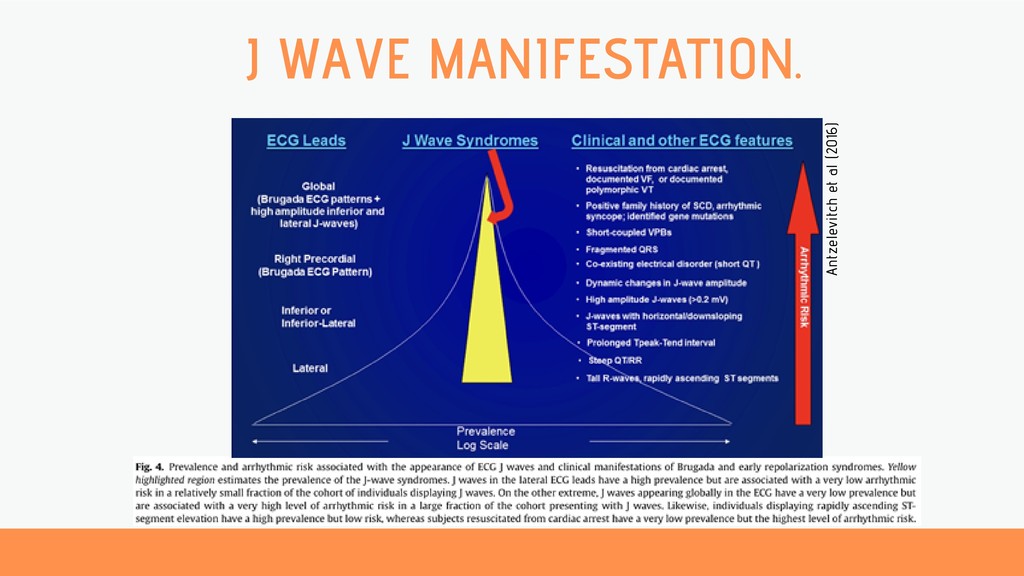
when there is ERP in the inferior/lateral leads presenting with aborted cardiac arrest, VF or polymorphic VT. Antzelevitch et al (2016) Macfarlane et al (2015) Antzelevitch et al (2016)
spectrum with BrS; Many clinical similarities – suggesting similar pathophysiology. Males predominate both syndromes (71% of BrS & 80% of ERS). Incidence of VF highest in third decade of life; ?linked to testosterone. ERP is prevalent in Africans/African-Americans, but apparently not associated with high risk.
the inferior leads – predicts cardiac and arrhythmic death. The incidental discovery of a J-wave should not be interpreted as a marker of ‘high risk’ for SCD since the odds are extremely low. Presence of a J-wave on the ECG may increase the probability of VF from 3.4:100,000 to 11:100,000. Viskin et al (2014). Rosso et al (2011).
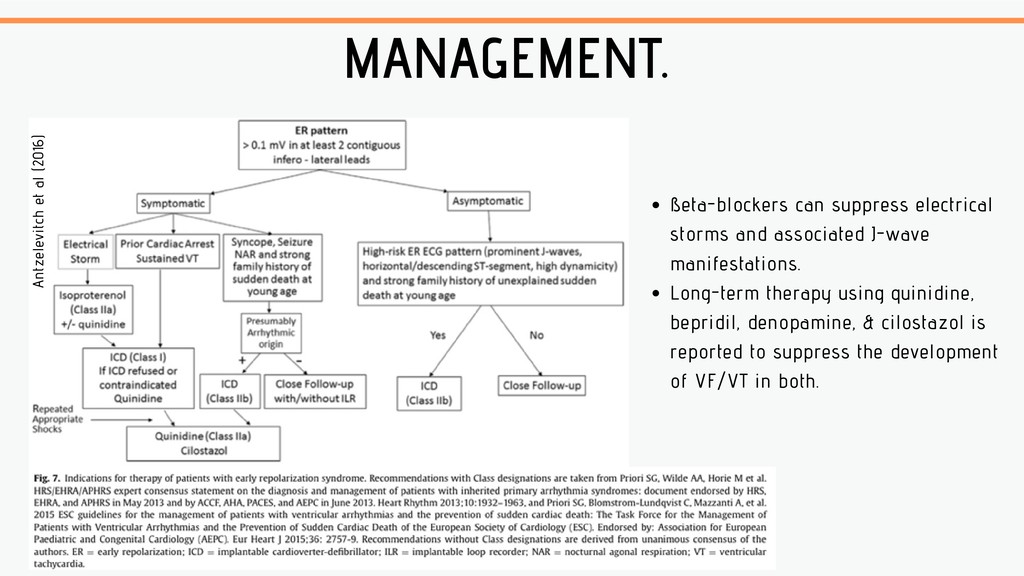
Long-term therapy using quinidine, bepridil, denopamine, & cilostazol is reported to suppress the development of VF/VT in both. Antzelevitch et al (2016)
benign. ERS lies on a spectrum with BrS. ERP in the anterior leads appears more likely to be ‘benign’, with inferior/lateral ERP more likely to be high risk. Care must still be taken when labelling anterior ER/non-specific STE as "BER". Symptomatic ERS is an indication for ICD implantation. In the absence of syncope, or a strong family history of sudden cardiac death (SCD), the finding of the ERP does not merit further investigation. Asymptomatic ERS should receive ‘close’ follow up.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}