The Essentials of 12-lead ECG & Rhythm Recognition.
A presentation I put together for a teaching session for non-speciality band 5s.
Due to the session being only 45 mins, this is a streamlined presentation of the basics, but may be of interest to those wanting a whistle-stop tour.
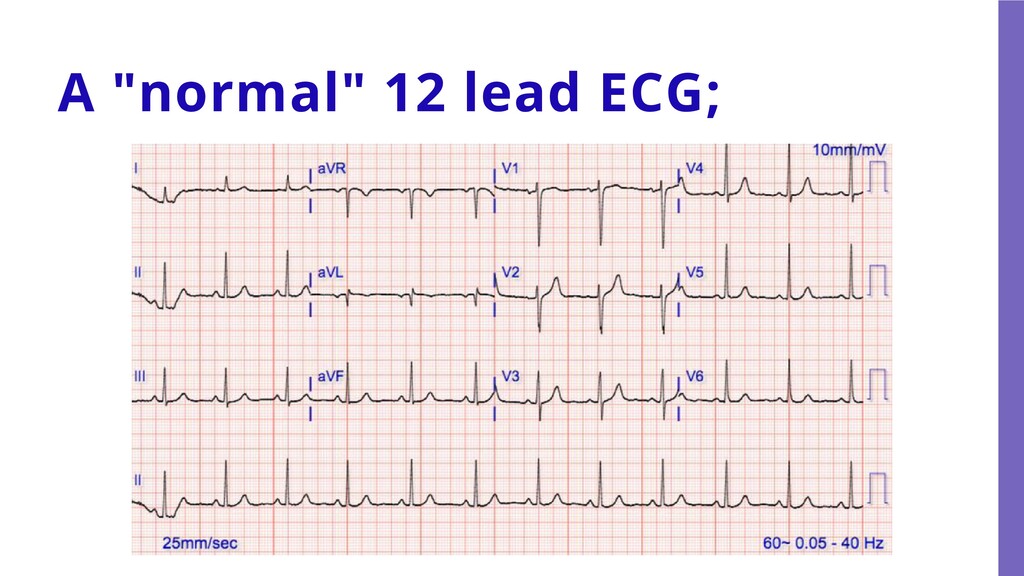
perform 3, 4, 5 lead rhythm monitoring. Identify the features of a "normal" ECG and heart rhythm, as well as what might not be normal. Understand how to approach the interpretation of a heart rhythm. Recognise red-flag abnormalities and when to get help.
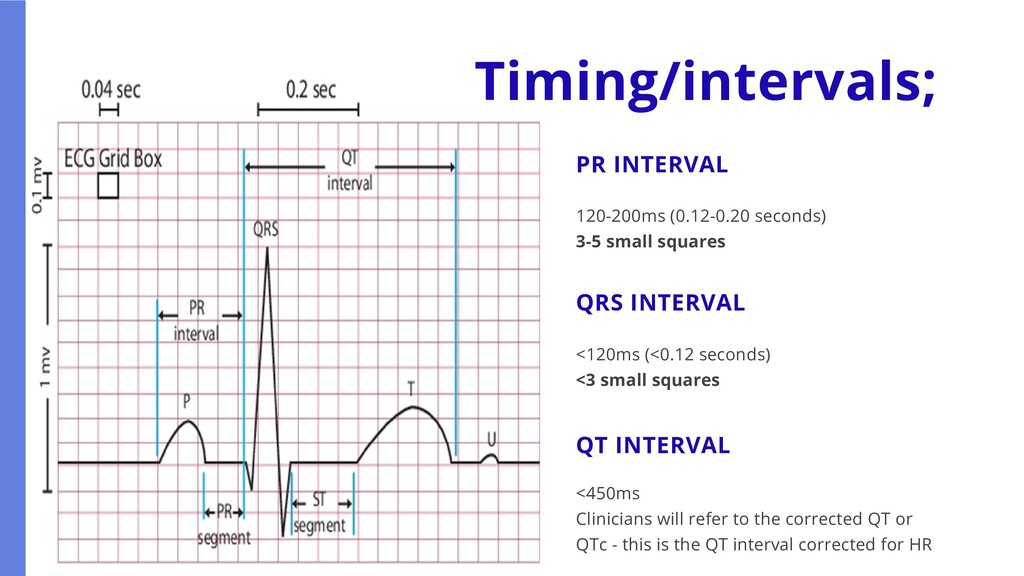
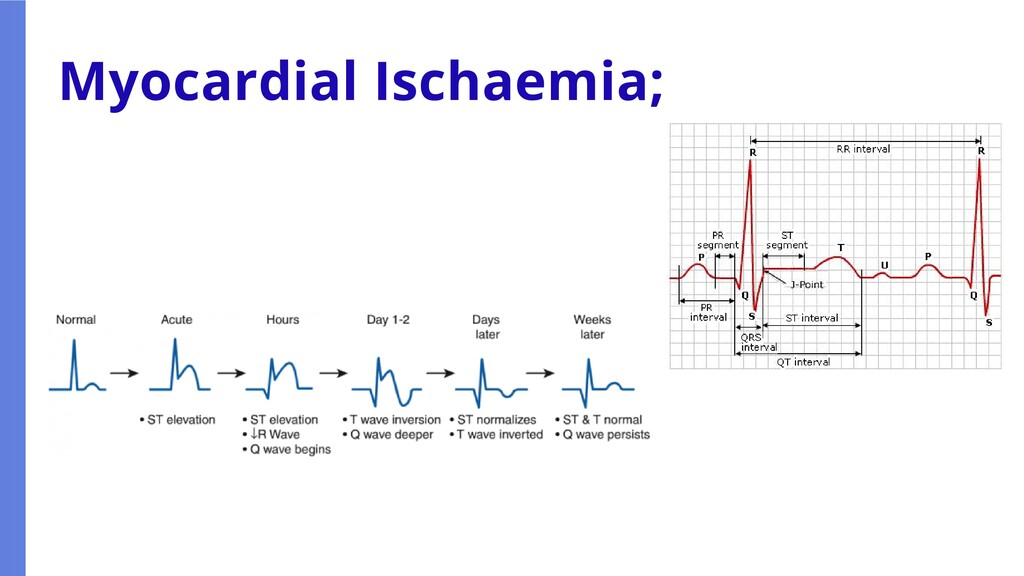
INTERVAL <120ms (<0.12 seconds) <3 small squares QT INTERVAL <450ms Clinicians will refer to the corrected QT or QTc - this is the QT interval corrected for HR
time (check date) First things first; Why was the ECG performed? What were the corresponding symptoms? How does this ECG relate to other vital signs such as BP? WHAT HAS CHANGED? How does this compare to previous ECGs and/or rhythm monitoring?
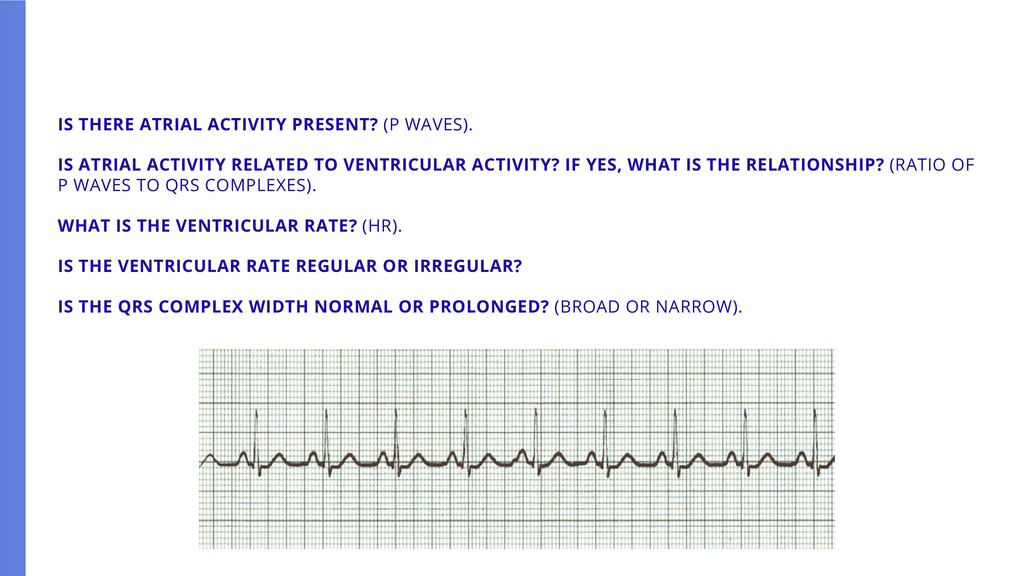
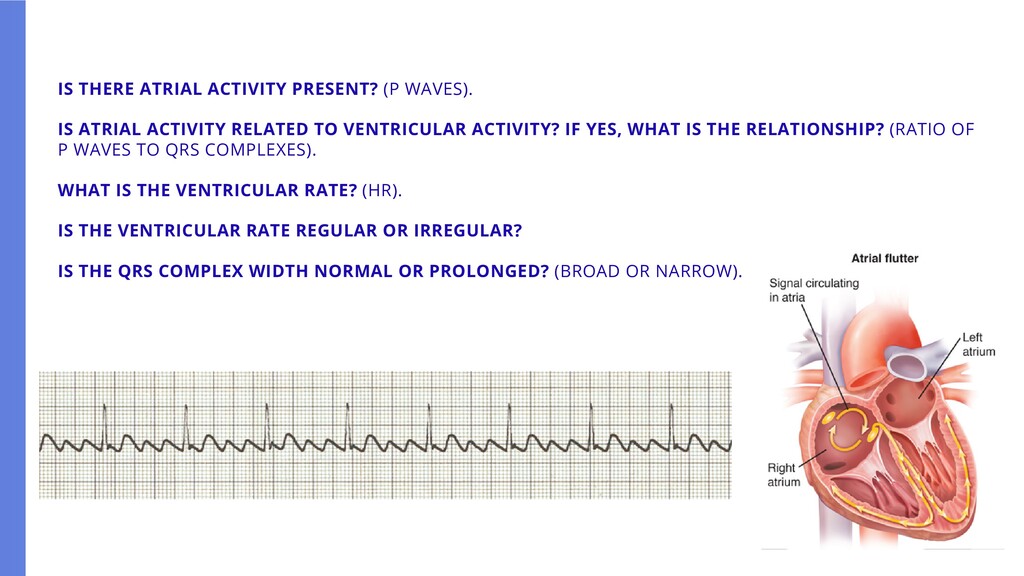
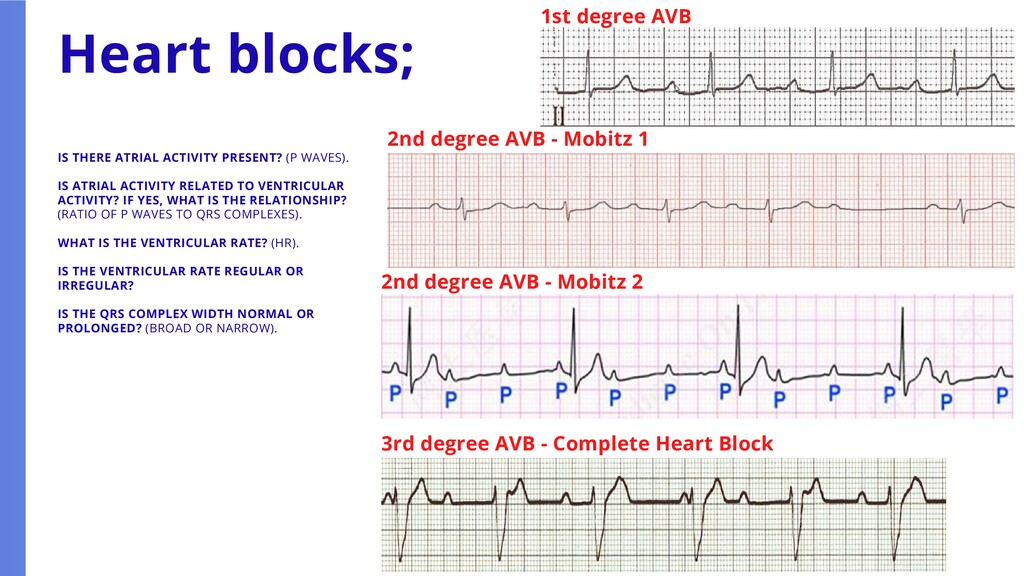
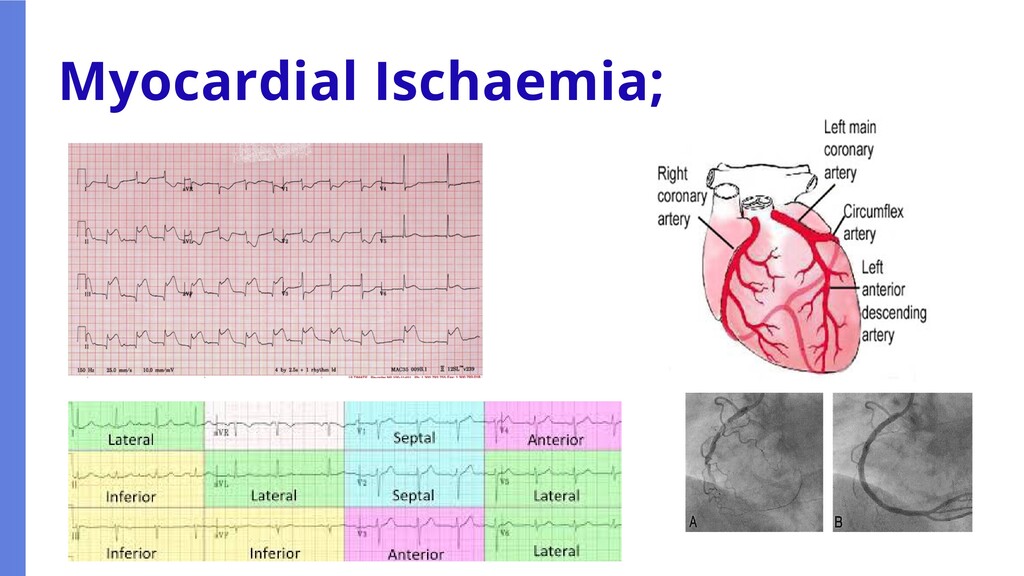
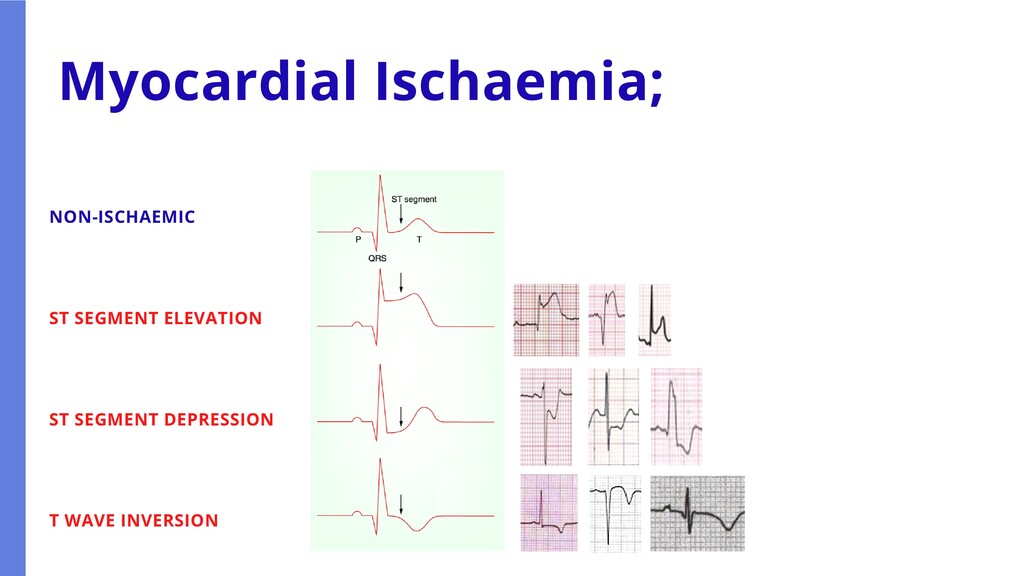
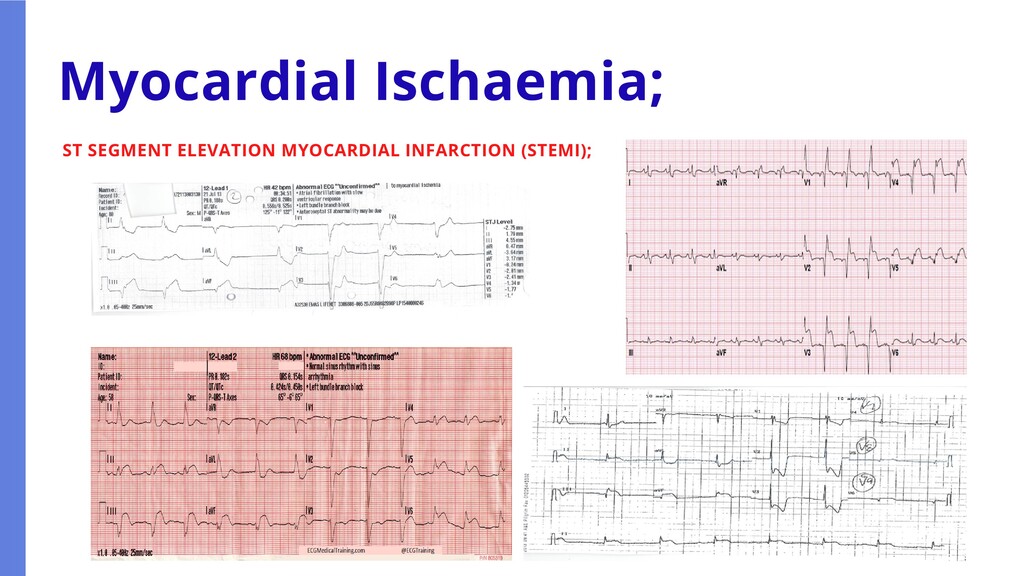
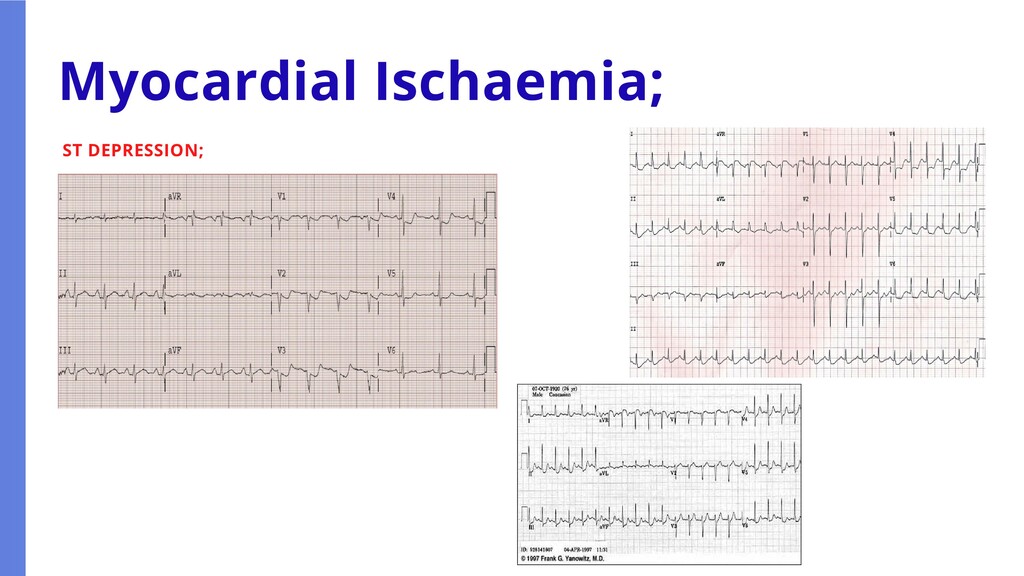
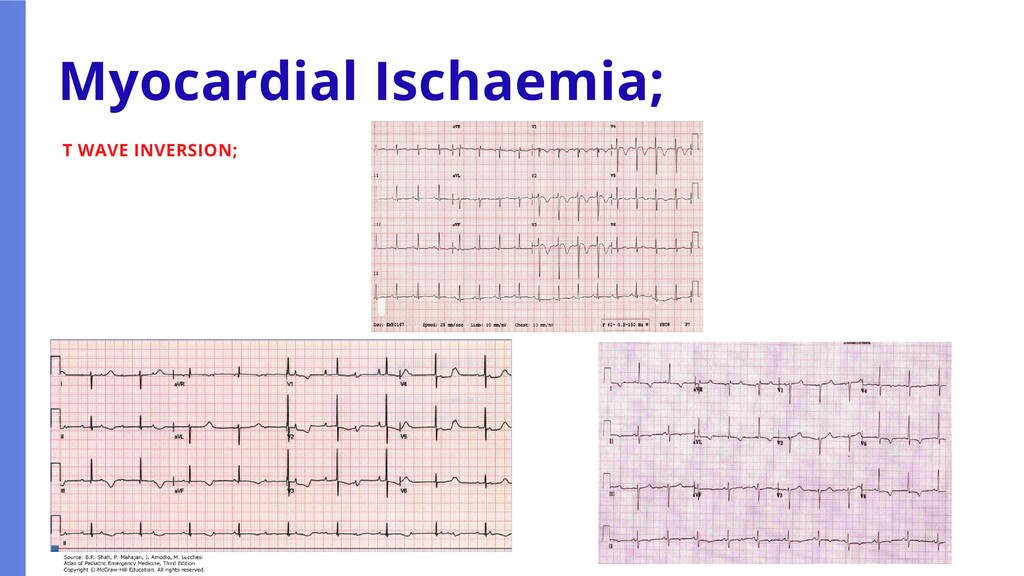
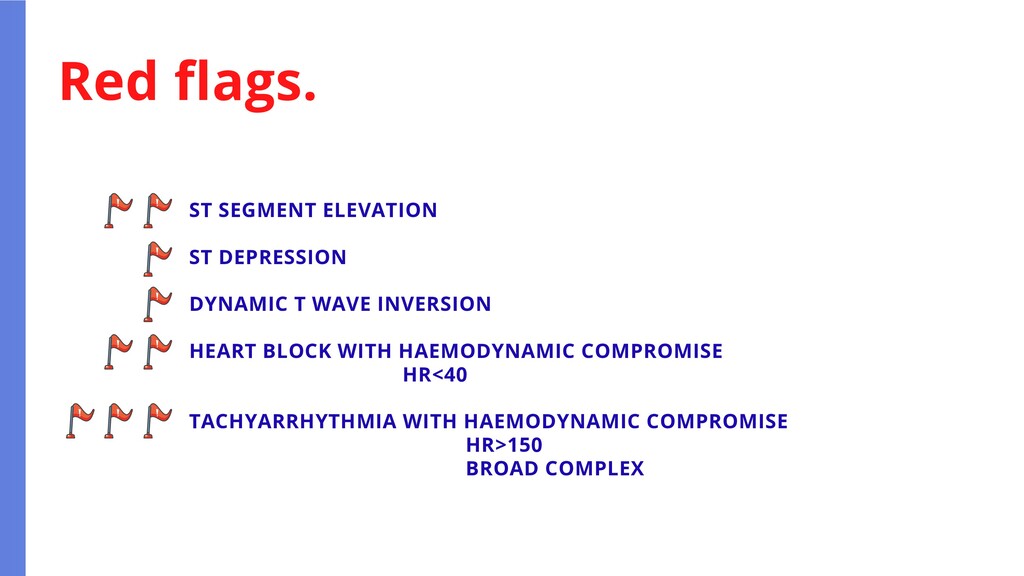
RELATED TO VENTRICULAR ACTIVITY? IF YES, WHAT IS THE RELATIONSHIP? (RATIO OF P WAVES TO QRS COMPLEXES). WHAT IS THE VENTRICULAR RATE? (HR). IS THE VENTRICULAR RATE REGULAR OR IRREGULAR? IS THE QRS COMPLEX WIDTH NORMAL OR PROLONGED? (BROAD OR NARROW). ADDITIONALLY FOR 12 LEAD ECGS; WHAT IS THE ST SEGMENT DOING? How to interpret the rhythm; If you can answer these questions and communicate this, you can describe a rhythm/ECG to another HCP without needing to fully interpret what you are seeing.
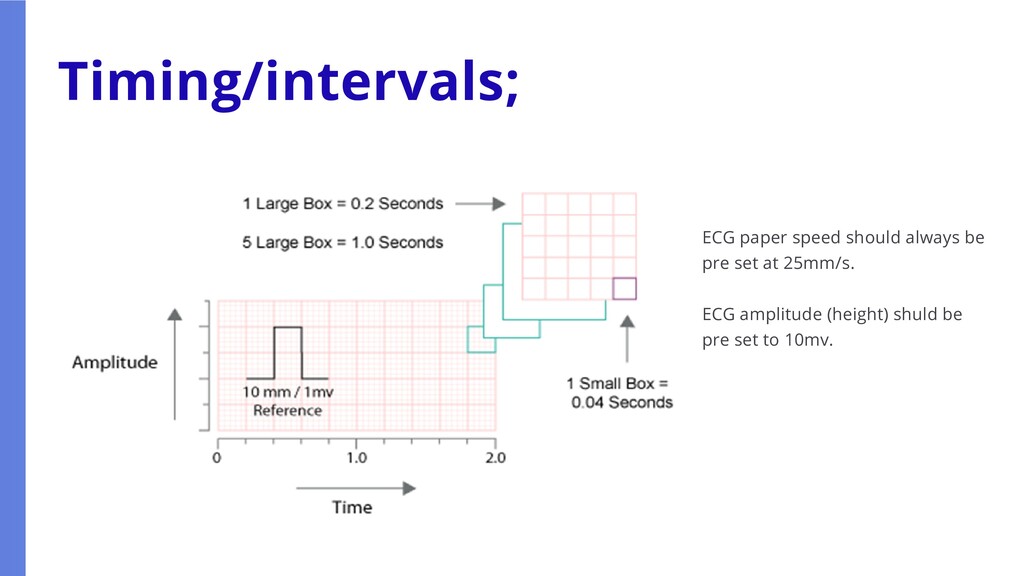
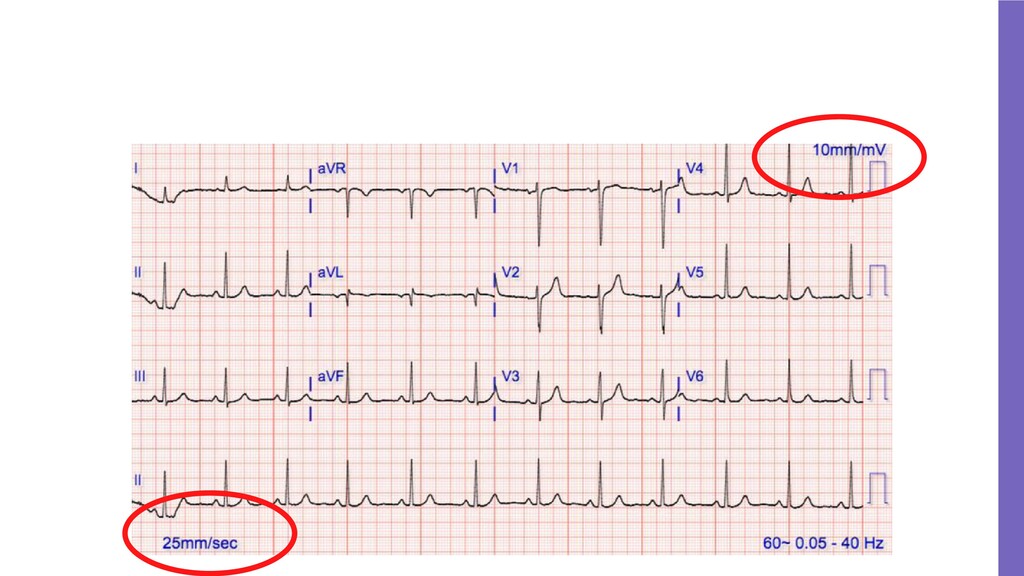
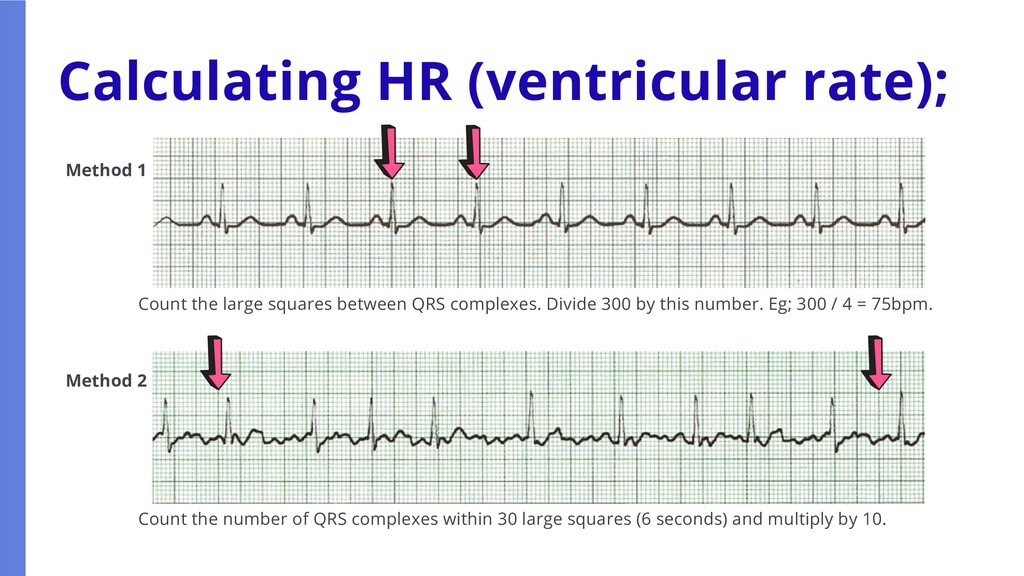
large squares between QRS complexes. Divide 300 by this number. Eg; 300 / 4 = 75bpm. Count the number of QRS complexes within 30 large squares (6 seconds) and multiply by 10.
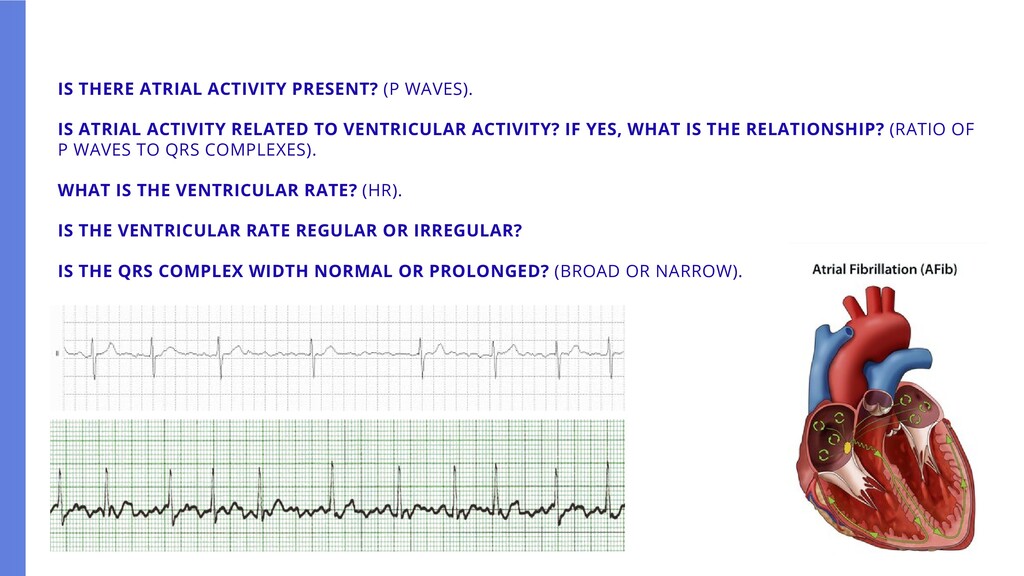
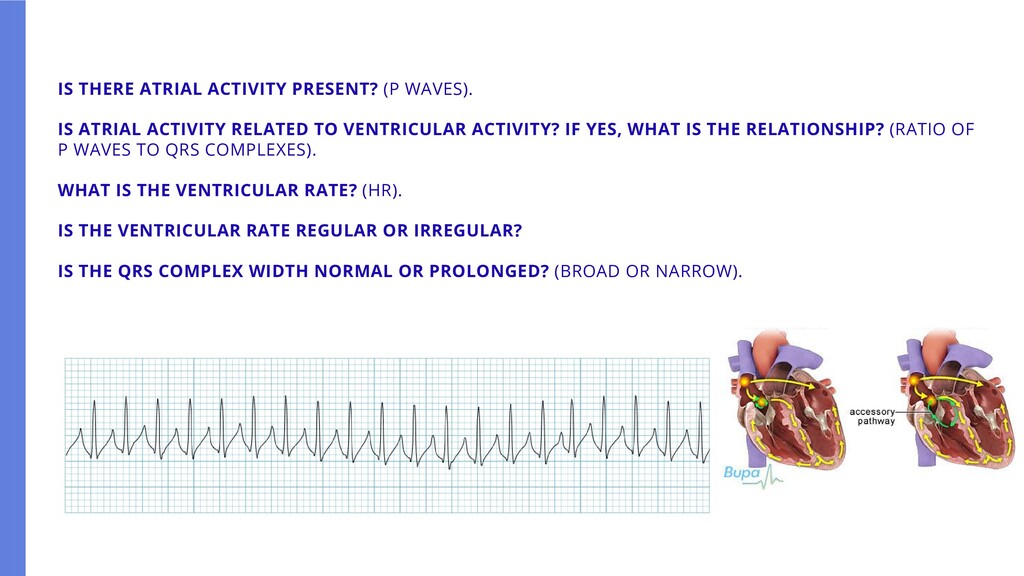
RELATED TO VENTRICULAR ACTIVITY? IF YES, WHAT IS THE RELATIONSHIP? (RATIO OF P WAVES TO QRS COMPLEXES). WHAT IS THE VENTRICULAR RATE? (HR). IS THE VENTRICULAR RATE REGULAR OR IRREGULAR? IS THE QRS COMPLEX WIDTH NORMAL OR PROLONGED? (BROAD OR NARROW).
RELATED TO VENTRICULAR ACTIVITY? IF YES, WHAT IS THE RELATIONSHIP? (RATIO OF P WAVES TO QRS COMPLEXES). WHAT IS THE VENTRICULAR RATE? (HR). IS THE VENTRICULAR RATE REGULAR OR IRREGULAR? IS THE QRS COMPLEX WIDTH NORMAL OR PROLONGED? (BROAD OR NARROW).
RELATED TO VENTRICULAR ACTIVITY? IF YES, WHAT IS THE RELATIONSHIP? (RATIO OF P WAVES TO QRS COMPLEXES). WHAT IS THE VENTRICULAR RATE? (HR). IS THE VENTRICULAR RATE REGULAR OR IRREGULAR? IS THE QRS COMPLEX WIDTH NORMAL OR PROLONGED? (BROAD OR NARROW).
RELATED TO VENTRICULAR ACTIVITY? IF YES, WHAT IS THE RELATIONSHIP? (RATIO OF P WAVES TO QRS COMPLEXES). WHAT IS THE VENTRICULAR RATE? (HR). IS THE VENTRICULAR RATE REGULAR OR IRREGULAR? IS THE QRS COMPLEX WIDTH NORMAL OR PROLONGED? (BROAD OR NARROW).
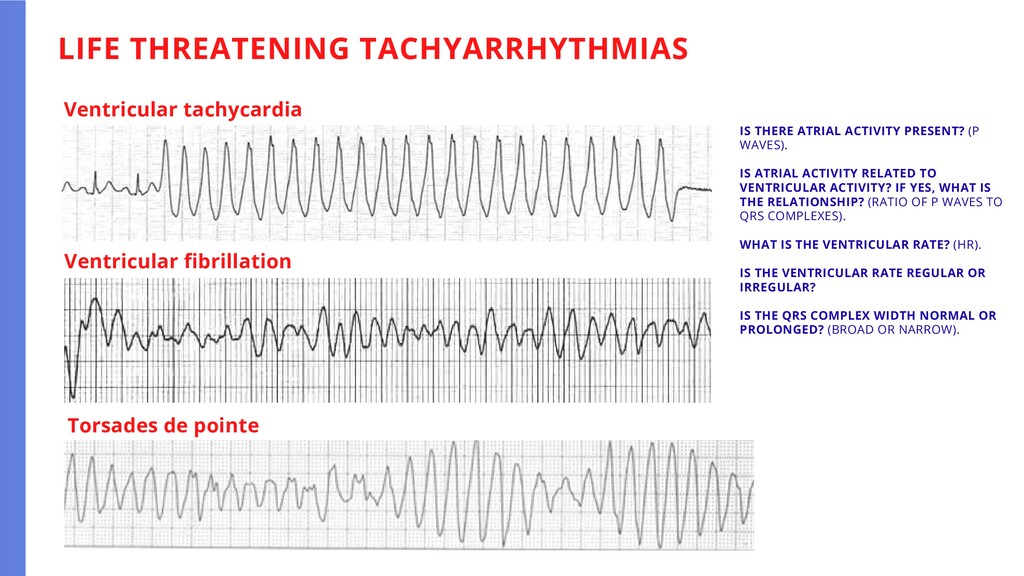
RELATED TO VENTRICULAR ACTIVITY? IF YES, WHAT IS THE RELATIONSHIP? (RATIO OF P WAVES TO QRS COMPLEXES). WHAT IS THE VENTRICULAR RATE? (HR). IS THE VENTRICULAR RATE REGULAR OR IRREGULAR? IS THE QRS COMPLEX WIDTH NORMAL OR PROLONGED? (BROAD OR NARROW). LIFE THREATENING TACHYARRHYTHMIAS Ventricular tachycardia Ventricular fibrillation Torsades de pointe
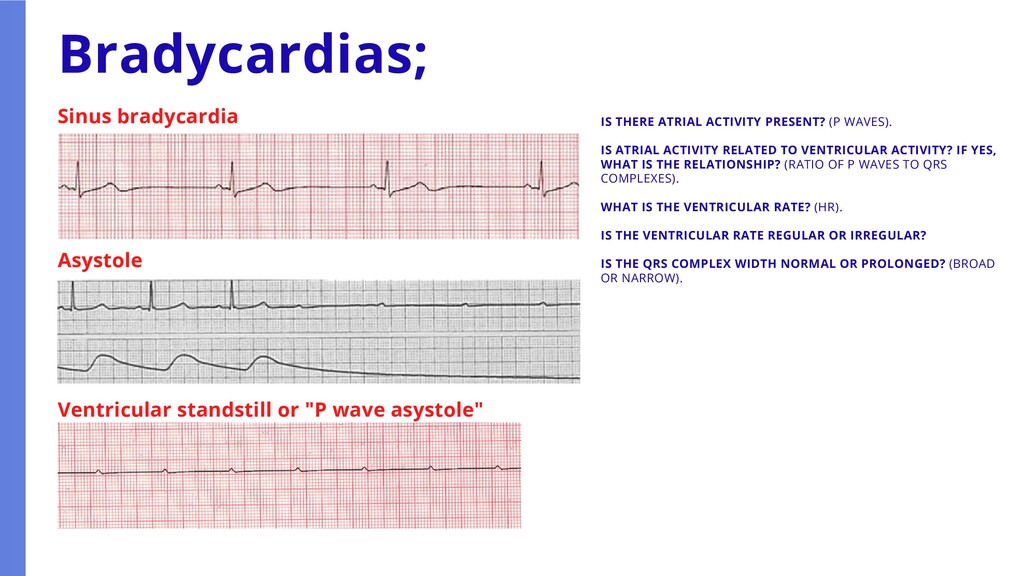
RELATED TO VENTRICULAR ACTIVITY? IF YES, WHAT IS THE RELATIONSHIP? (RATIO OF P WAVES TO QRS COMPLEXES). WHAT IS THE VENTRICULAR RATE? (HR). IS THE VENTRICULAR RATE REGULAR OR IRREGULAR? IS THE QRS COMPLEX WIDTH NORMAL OR PROLONGED? (BROAD OR NARROW). Bradycardias; Sinus bradycardia Asystole Ventricular standstill or "P wave asystole"
RELATED TO VENTRICULAR ACTIVITY? IF YES, WHAT IS THE RELATIONSHIP? (RATIO OF P WAVES TO QRS COMPLEXES). WHAT IS THE VENTRICULAR RATE? (HR). IS THE VENTRICULAR RATE REGULAR OR IRREGULAR? IS THE QRS COMPLEX WIDTH NORMAL OR PROLONGED? (BROAD OR NARROW). Heart blocks; 1st degree AVB 2nd degree AVB - Mobitz 1 2nd degree AVB - Mobitz 2 3rd degree AVB - Complete Heart Block
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}