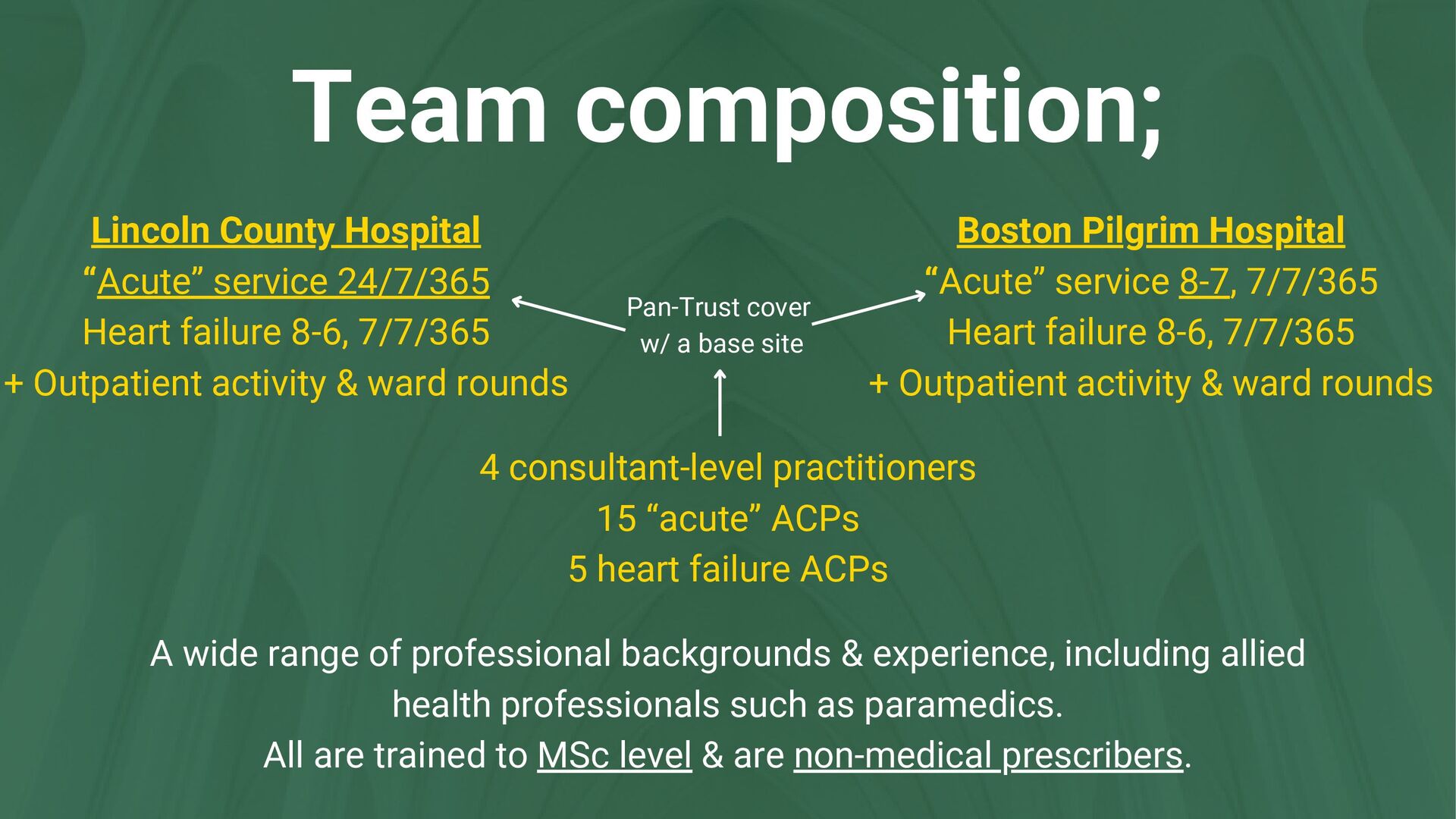
8-6, 7/7/365 + Outpatient activity & ward rounds Boston Pilgrim Hospital “Acute” service 8-7, 7/7/365 Heart failure 8-6, 7/7/365 + Outpatient activity & ward rounds 4 consultant-level practitioners 15 “acute” ACPs 5 heart failure ACPs A wide range of professional backgrounds & experience, including allied health professionals such as paramedics. All are trained to MSc level & are non-medical prescribers. Pan-Trust cover w/ a base site
& the angina “spectrum” Chest pain suspected to be cardiac in origin (often not - see next slide) Arrhythmia & cardiac arrest Acute heart failure / chronic decompensations Valvular dysfunction Endocarditis Pericarditis & Myocarditis Cardiac syncope (as opposed to undifferentiated)
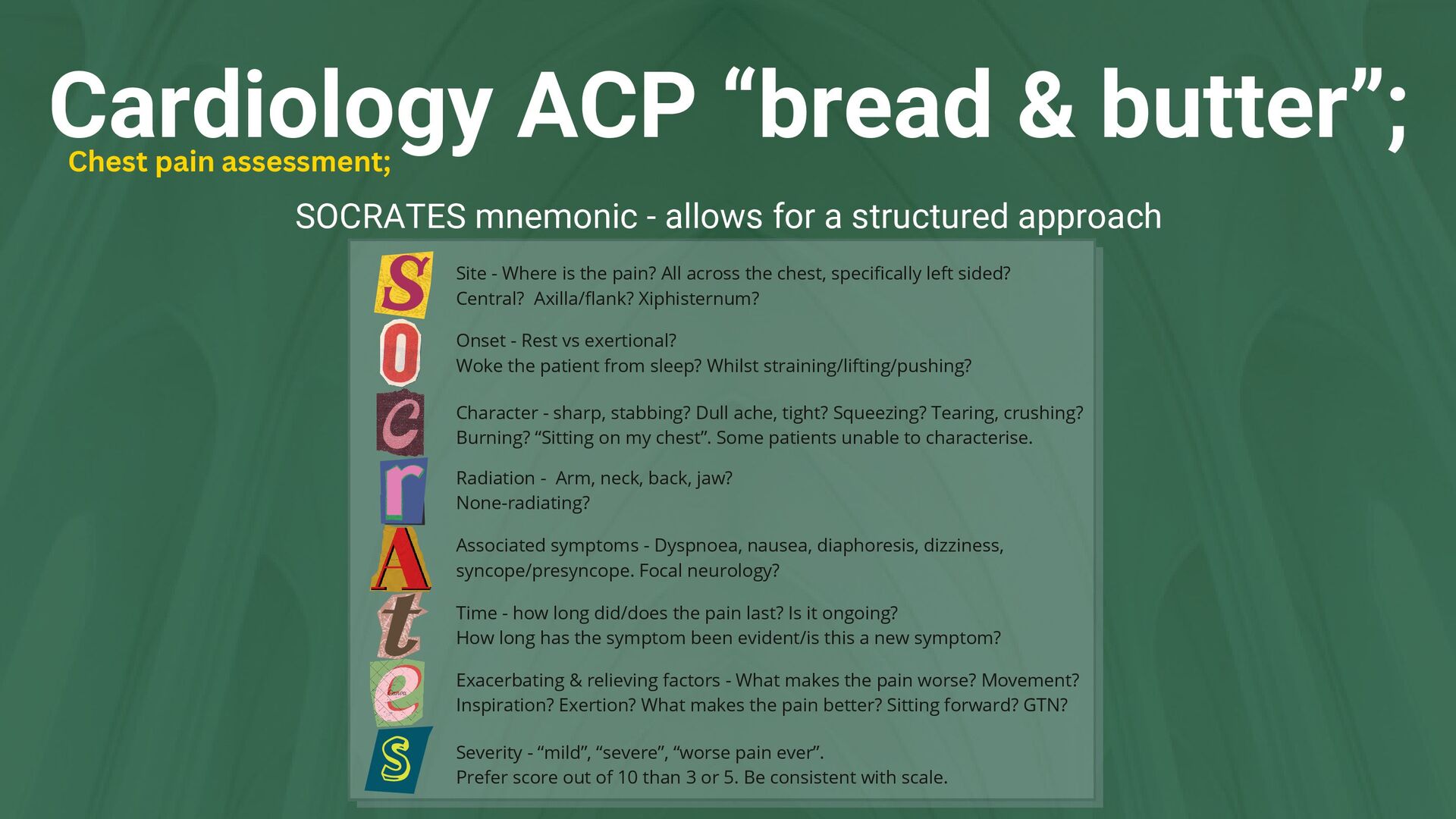
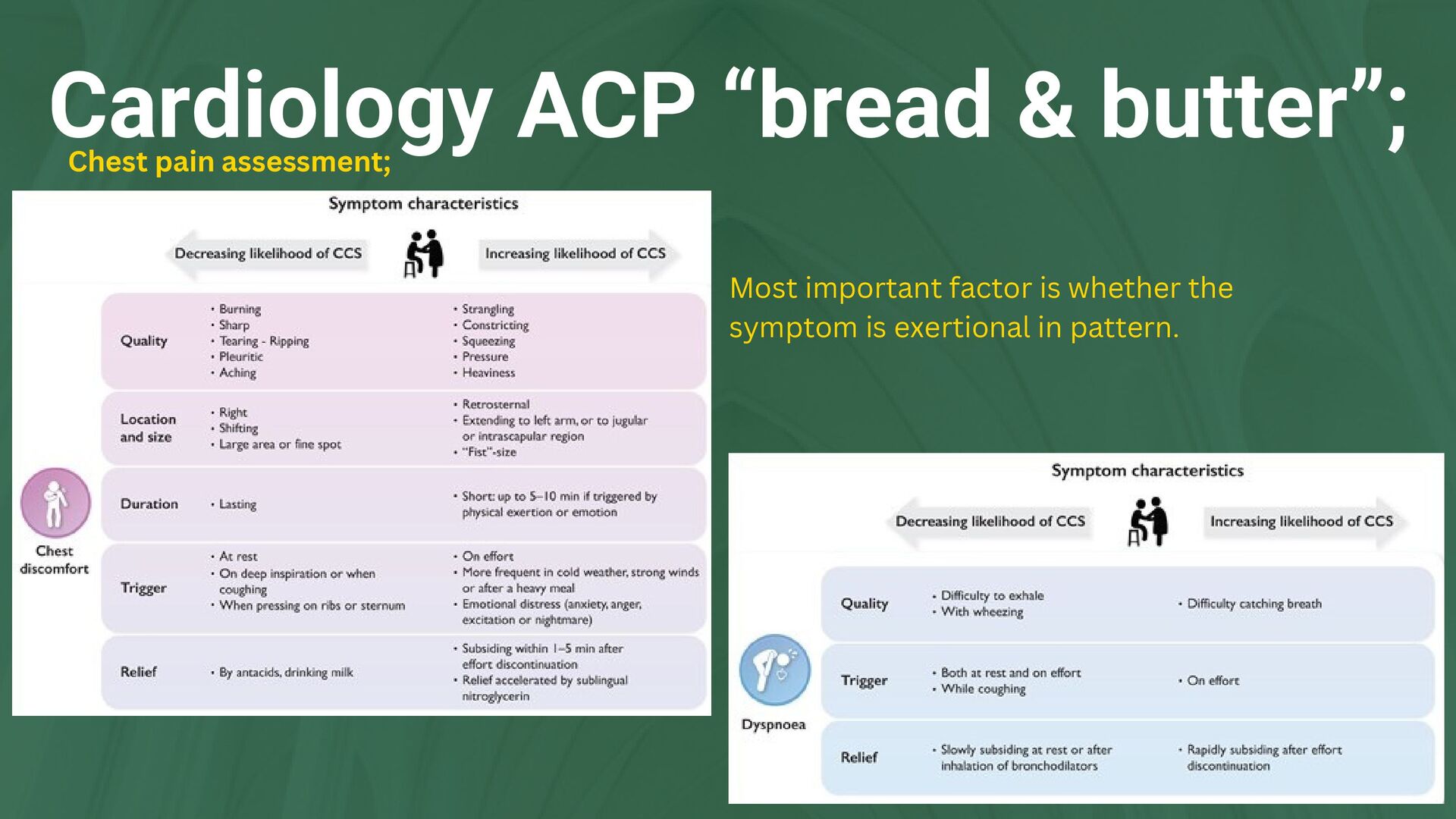
a structured approach Chest pain assessment; Severity - “mild”, “severe”, “worse pain ever”. Prefer score out of 10 than 3 or 5. Be consistent with scale. Onset - Rest vs exertional? Woke the patient from sleep? Whilst straining/lifting/pushing? Character - sharp, stabbing? Dull ache, tight? Squeezing? Tearing, crushing? Burning? “Sitting on my chest”. Some patients unable to characterise. Radiation - Arm, neck, back, jaw? None-radiating? Associated symptoms - Dyspnoea, nausea, diaphoresis, dizziness, syncope/presyncope. Focal neurology? Time - how long did/does the pain last? Is it ongoing? How long has the symptom been evident/is this a new symptom? Exacerbating & relieving factors - What makes the pain worse? Movement? Inspiration? Exertion? What makes the pain better? Sitting forward? GTN? Site - Where is the pain? All across the chest, specifically left sided? Central? Axilla/flank? Xiphisternum?
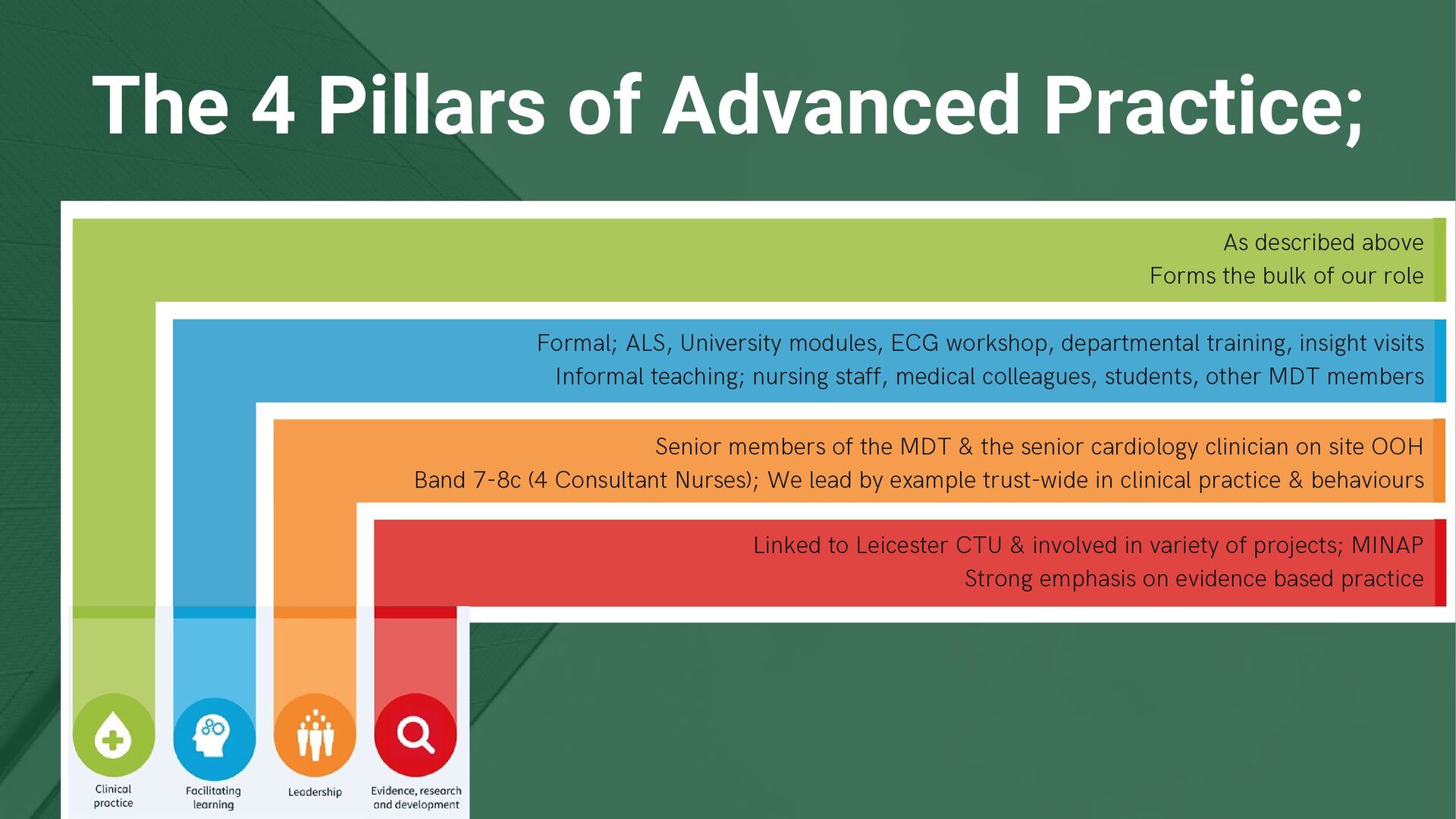
the bulk of our role Formal; ALS, University modules, ECG workshop, departmental training, insight visits Informal teaching; nursing staff, medical colleagues, students, other MDT members Senior members of the MDT & the senior cardiology clinician on site OOH Band 7-8c (4 Consultant Nurses); We lead by example trust-wide in clinical practice & behaviours Linked to Leicester CTU & involved in variety of projects; MINAP Strong emphasis on evidence based practice
independent decision making High level of responsibility Highly respected (& relied upon) by other members of the MDT Significant investment in training compared to other roles (beyond MSc pathway) Opens up a wide range of career opportunities Maintain patient contact - historically lost in more senior nursing roles Supportive peers Not-so positives; High expectation for self-directed study & almost continuous ongoing study “Lone” working Admin! High level of responsibility Significant risk for stress/burnout - shifts can be intense
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}