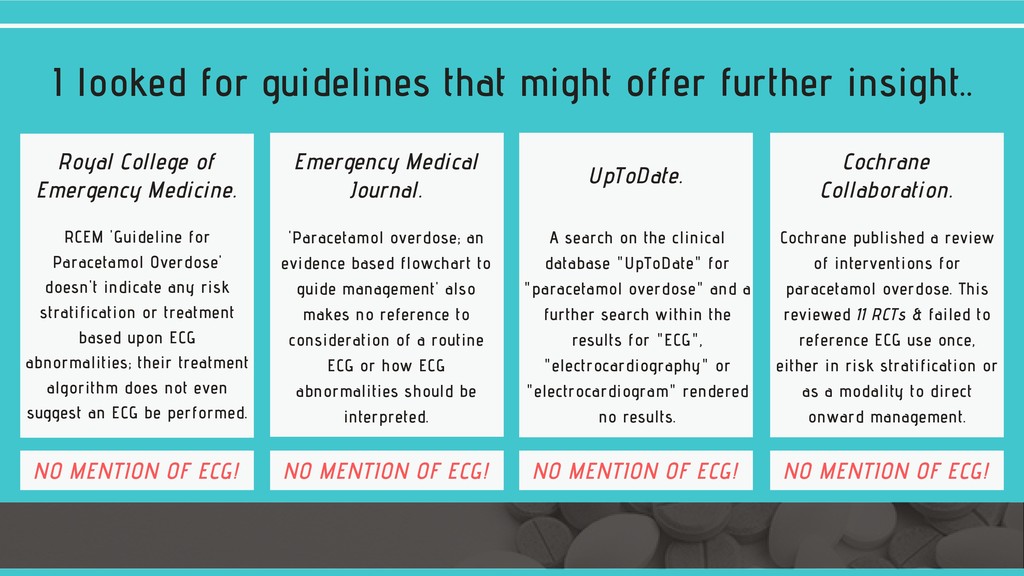
Interventions for paracetamol (acetaminophen) overdose (Review). Cochrane Library, Cochrane Database of Systematic Reviews. 2018, issue 2, art no. CD003328. John Wiley & Sons, Ltd. Armour, A. and Slater SD. (1993) Paracetamol cardiotoxicity. Postgraduate Medical Journal. 69, 52-54. Contractor, H., Gauge, V., Nabi, S., Titu, H., Arya, S. and Naqvi, N. (2011) ST segment elevation secondary to paracetamol overdose. Therapeutic Advances in Cardiovascular Disease. 2011, 4(1) 83-85. Rahman, A., Chowdhury, A. and Jabeen, S. (2019) Changes in ECG among patients with drug induced poisoning in a tertiary care hospital. Bangladesh Medical Research Council Bulletin 44(3), 160-167. Ralapanawa, U., Jayawickreme, KP., Ekanayake, EMM., and Dhammika Menike Dissssanayake, AMS. (2016) A study on paracetamol cardiotoxicity. Pharmacology and Toxicology 2016, 17:30. Royal College of Emergency Medicine (2017) “Paracetamol overdose: new guidance on the use of intravenous acetylcysteine” and “paracetamol poisoning proforma to guide ED management of oral ingestion in adults”. Both available at https://www.rcem.ac.uk/RCEM/Quality-Policy/Clinical_Standards_Guidance/RCEM_Guidance.aspx? WebsiteKey=b3d6bb2a-abba-44ed-b758-467776a958cd&hkey=862bd964-0363-4f7f-bdab-89e4a68c9de4&RCEM_Guidance=6 UpToDate (2019) https://www.uptodate.com/home, Wolters Kluwer. Wallace, C., Dargan , P. and Jones AL (2002) Paracetamol overdose: an evidence based flowchart to guide management https://emj.bmj.com/content/19/3/202 References.
![ST/T wave abnormalities in paracetamol [acetaminophen] overdose. B Y S](https://files.speakerdeck.com/presentations/0e58f7cb38e343f1ad144159ea2730c1/slide_0.jpg){kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}