25% hepatic artery • Hepatic artery has higher O2 conc, so each supply 50% of hepatic O2 supply • Sympathetic innervations from T3 to T11 control resistance in hepatic venules • In presence of reduced portal venous flow, hepatic artery can increase flow by 100% to maintain hepatic O2 delivery known as hepatic arterial buffer response
site of anaerobic metabolism • Aids in blood glucose regulation through glucose buffering function • Protein synthesis, all plasma proteins except y-globulins • Deamination of amino acids produces ammonia • All coagulation factors except 3,5, and 8 synthesized in the liver • Vit K required for factors 2,7,9,10
fat absorption • breaks down many substances in the blood, including toxins • excretes bilirubin — a waste product of hemoglobin catabolism — in bile (excreted in feces)
each drug (by oxidation) • CYP2B6 = methadone (inactive), propofol • CYP2D6 = codeine(inactive), BB, some antiarrhythmics diltiazem, tramadol, captopril, zofran, hydrocodone/oxycodone(still active, metabolites more active) • Inhibited by fluoxetine and sertraline (SSRIs), haloperidol, cimetidine, quinidine • Morphine -> M3G (60%) and M6G (10%) • M6G – potent, accumulates in liver and renal failure and can result in severe resp depression
dexamethasone, Tylenol, midazolam, alfentanil, OCPs, • Inhibited by SSRI, macrolides, diltiazem, verapamil, azoles, grapefruit, anti HIV which can prolong effect of fentanyl • CYP2C19 = PPIs (omeprazole) and antidepressants, phenytoin, metoprolol, esmolol, atenolol, plavix, diazepam, propranolol, warfarin • CYP2D9 = phenytoin, warfarin, and ibuprofen • MC1R(in red heads) = may lead to increased analgesia in morphine - OPRM gene may render morphine less effective
kg/m2) or obese (BMI >30 kg/m2) • Associated comorbidities include HTN, diabetes, and sleep apnea • Obesity increases risk of hospital admission and length of hospital stay • 1998 NIH recommended bariatric surgery as primary treatment for morbid obesity (BMI >40 kg/m2 or BMI >35 kg/m2 associated with comorbidities) • Roux-en-Y gastric bypass best surgical treatment and laparoscopic approach preferred because of decreased pain, early ambulation, earlier discharge, quicker return to regular activity, and decreased wound complication rate when compared to open procedures.
PVR can lead to HTN -> inc LV wall stress by inc SV -> LV dilation -> LV hypertrophy • Can have increased PAP (exacerbated by hypercarbia and hypoxia) -> RV failure • Respiratory effects • increased O2 consumption and CO2 production with increased metabolic demand • decreased FRC secondary to dec ERV -> dec TLC; FRC further decreased in supine position and under GA/abdominal insufflation • Airway closure during normal ventilation -> inc pulm shunt -> hypoxemia
episodes of apnea (>10 sec cessation of airflow, despite continuous respiratory effect against a closed airway) and hypopnea (50% reduction in airflow or reduction associated with dec of SpO2 >4%) • Can lead to secondary polycythemia, hypoxemia, hypercapnia, which increases the risk of cardiac and cerebral vascular disease • Dx using STOP-BANG, definitive with polysomnography Obesity hypoventilation syndrome • Somnolence, cardiac enlargement, polycythemia, hypoxemia, and hypercapnia • Older, super obese (>50kg/m2), more restricted pulmonary function compared to OSA patients • Most severe form is Pickwickian syndrome • These patients rely on hypoxic ventilatory drive and may hypoventilate or even become apneic following emergence from GA after being given 100% O2 to breathe
NPO duration, alcohol and smoking cessation, review of nutritional status, discussion of carb loading, DVT prophylaxis, and postop pain management • Evaluate any patient who had previous bariatric surgery for metabolic changes that can include protein, vitamin, iron, and calcium deficiencies
Review list of current meds, including nonprescription appetite suppressors and diet drugs since many of these drugs can have important side effects • Airway exam to assess difficulty of ventilation and intubation • Large neck circumference and high Mallampati score may predict difficult intubation • Review of previous anesthetic records will reveal airway difficulty or ease with past surgical procedures
desaturation with apnea due to dec FRC and O2 reserve • If anticipate difficult airway should perform awake intubation with FOB or video laryngoscope after adequate airway analgesia with airway blocks or topical anesthesia • Proper patient positioning to facilitate intubation with direct laryngoscopy , ear level with sternum “sniffing position” • Aids for difficult intubation such as short laryngoscope handle, variety blades, LMA, video laryngoscope, bougie, and equipment for cricothyroidotomy, and transtracheal jet ventilation
may be inaccurate if anatomy of upper arm does not allow a proper fit • Cuff pressures can be obtained from forearm • Reliable peripheral IV, central line only if unable to obtain peripheral IV • Proper padding during positioning • Multimodal intraoperative prophylaxis for PONV • DVT prophylaxis
positioning to change leading to mainstem intubation and hypoxemia, PTX • Improper positioning of Veress needle can lead to pneumomediastinum, subcutaneous emphysema, or massive gas embolism
Tylenol, NSAIDs, dexmedetomidine • PCA with opioid dose based on LBW, avoid morphine and dilaudid (prolonged onset and duration of action increases risk of respiratory depression) • Maximize oxygenation • Semi-recumbent and reverse Trendelenburg position to help increase FRC • supplemental O2 • CPAP/BiPAP for patients who typically use it • Encourage early enteral nutrition and mobilization
liver disease, acute hepatitis (elevation in transaminase with elevation in INR), encephalopathy, and illness less than 26 weeks • MCC acetaminophen toxicity (39%), indeterminant (18%), idiosyncratic (19%), and acute viral hepatitis (12%) • Other etiologies include drugs (phenytoin, halothane), autoimmune disease, Wilson’s disease, Budd-Chiari syndrome, HELLP syndrome, acute fatty liver of pregnancy, and toxins.
elevated CO, low arterial BP, and low SVR. • Enhanced endogenous production or diminished hepatic clearance of vasodilating substances, such as nitric oxide, carbon monoxide, and endogenous cannabinoids, and the inflammatory response to bacterial translocation causes splanchnic arterial vasodilation • Increased venous capacitance from formation of portosystemic shunts because portal HTN increases venous capacitance and contributes to hyperdynamic circulation • Reduced responsiveness to B agonists
liver disease, vascular smooth muscle proliferation, vasoconstriction, intimal proliferation, and fibrosis all present as obstruction causing increase resistance to pulmonary blood flow. • RV overload, RHF, increased liver transplantation mortality risk, especially if mean PAP > 35 mmHg • Diagnosis- mean PAP > 25 at rest and PVR > 240 dyne normal pulmonary cap wedge pressure
shunts and chronic hypoxia, or leads to pulmonary vasoconstriction and medial hyperplasia, increased vascular resistance and pulmonary HTN • Present with orthodeoxia, platypnea, cyanosis, digital clubbing • Diagnosis: presence of liver disease with portal HTN and cirrhosis, Aa gradient > 15 mmHg, Treatment: liver transplant
and cirrhosis have increases risk of mortality after liver transplant • GI bleeding, diarrhea from infection or lactulose administration, and diuretic medications change circulatory function via hypovolemia and can cause renal injury. • Cirrhosis progression leads to reduction in SVR causing compensatory activation of renin angiotensin and sympathetic nervous systems, which leads to ascites, edema, and vasoconstriction of the intrarenal circulation and renal hypoperfusion
to splanchnic arterial vasodilation • Criteria for HRS • Cirrhosis with ascites, serum Cr greater than 1.5 mg/dL • No improvement of Cr after 2 days of diuretic withdrawal and volume expansion with albumin • Absence of shock • No current or recent treatment with nephrotoxic drugs • Absence of parenchymal kidney disease
progressive impairment of renal function (usually result of acute insult such as SBP or a large volume paracentesis) with a doubling of the initial serum Cr to levels greater than 2.5 mg/dL or a 50% reduction in the 24 hr CrCl to lower than 20ml per min in less than 2 weeks • Short term mortality of > 50% • Type II HRS • Impaired renal function and serum Cr >1.5 mg/dL and do not meet criteria for type I HRS
promote both bleeding and thrombosis • Inadequate synthesis of all coagulation factors (except vWF), thrombocytopenia, platelet function defects, dysfibrinogenemia, and elevated tissue plasminogen activator (tPA) levels cause bleeding • Elevations of vWF and factor VIII and decreased levels of ADAMTS-13, protein C, protein S, antithrombin, plasminogen • With the balance of decreased production of coagulation factors and decreased production of procoagulant factors, PT is unreliable tool for evaluating tendency to bleed or clot
hep patients may exhibit increased CNS sensitivity to anesthetics • Alcoholic patients display cross tolerance to both iv and volatile anesthetics, concern for cardiac depression effect of alcohol additive with anesthetics and alcoholic CMP
hepatic vein is less than 5 mmHg • Intrahepatic vascular resistance and portal venous blood flow increase this gradient • Portal hypertension produced endogenous vasodilators that cause splanchnic vasodilation which increases portal blood flow and further exacerbates portal hypertension
• May need to consult cardiologist, pulmonologist, nephrologist, or infectious disease • Evaluate hepatic function with a thorough history and physical • focus on cause and degree of hepatic impairment • History of alcohol or drug abuse, certain medications • Signs and Symptoms of Liver Injury • Jaundice, easy bruising, biliary colic, abdominal distention, ascites, palmar erythema, spider angiomas, gynecomastia, asterixis, ecchymoses, encephalopathy, AKI, electrolyte disturbances, cardiac or pulmonary dysfunction, or coagulopathy
function • ALT primarily localized in liver • Helps differentiate alcoholic (ratio >2) vs viral liver dz (ratio <1) • Indices of bile flow obstruction • Alkaline phosphatase (AP), y-glutamyl transferase, 5-nucleotidase, bilirubin • Tests of hepatic synthetic function: serum albumin and coagulation testing • Hypovolemia common, assess patient volume status
including Angiotensin II, AVP, and NE • May be modulated by release of NO, prostacyclin, and other endothelial derived factors in response to humoral and mechanical stimuli • Serum albumin level qualitatively and quantitively decreased • Albumin has three major indications in Rx of cirrhotic patient 1. Large volume paracentesis (4-5L) 2. Presence of SBP to prevent renal impairment, pt with bili >4mg/dl and Cr >1 mg/dl 3. Presence of Type I HRS (use beneficial in conjunction with splanchnic vasoconstriction)
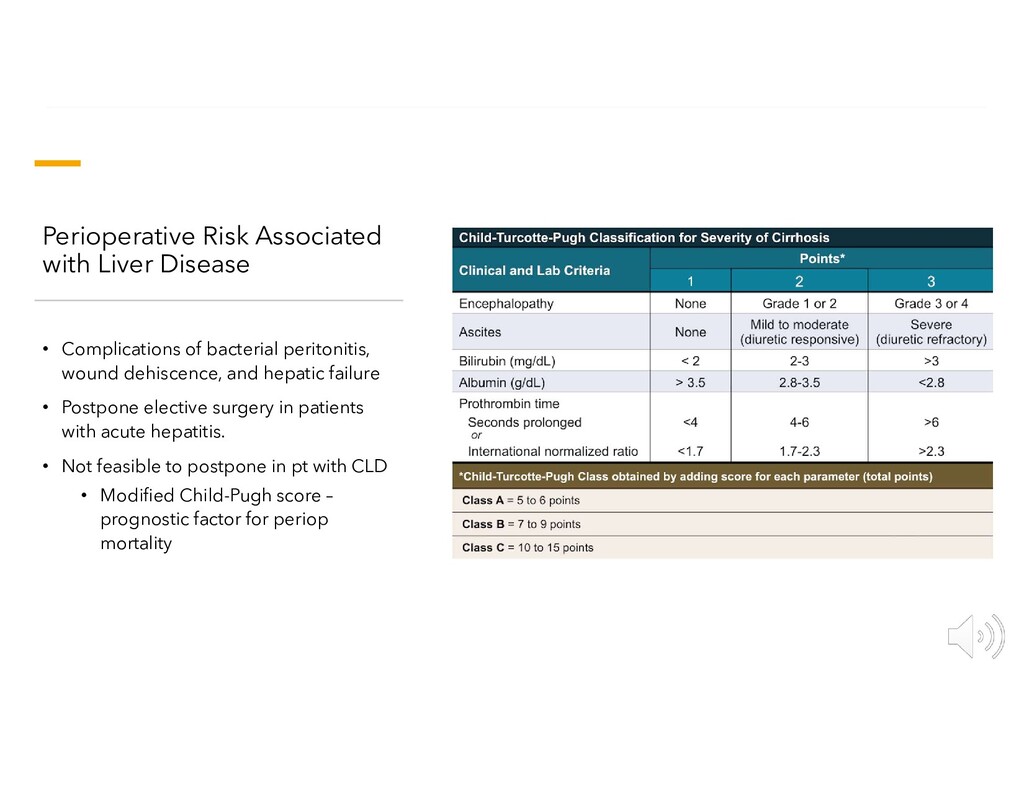
peritonitis, wound dehiscence, and hepatic failure • Postpone elective surgery in patients with acute hepatitis. • Not feasible to postpone in pt with CLD • Modified Child-Pugh score – prognostic factor for periop mortality
vasoactive infusions • Optimizing central blood volume and renal status while minimizing ascites (low sodium diet/ diuretic therapy) • Improving encephalopathy(rifaximin/lactulose) • Treat coagulopathy if active bleeding with FFP, cryoprecipitate, PRBCs, or platelets dictated by clinical and lab assessment • Minimize surgical risk through consideration of less invasive approach
have restricted hepatic clearance (ex. Benzos, Opioids) • Affected by protein binding, induction or inhibition of hepatic enzymes, age, and hepatic pathology • High extraction ratios (>0.7) undergo extensive first pass metabolism (ex. Ketamine, Etomidate, Propofol) • Significantly affected by alterations in hepatic blood flow (hemodynamic changes or hepatic inflow clamping during liver resection) • Short elimination half lives, may not see a significant prolongation
hepatic blood flow • Increased hepatic venous pressure • Controlled PPV with high mean airway pressures reduces VR and CO • reduce BP and increase sympathetic tone • Standard induction dose IV anesthetics ok to use because termination by redistribution rather than metabolism and excretion • Prolonged DOA with larger or repeated doses, especially opioids
of distribution, protein binding, drug metabolism, and drug elimination are common • Increased Vd for highly ionized drugs such as NMBs resistance observed requiring larger loading dose, smaller than normal maintenance • Succinylcholine prolonged due to decreased pseudocholinesterase
Sevoflurane and Isoflurane cause little reduction in hepatic blood flow at conc of 1 MAC • maintain hepatic arterial buffer response • Iso results in dose dependent reduction at MAC conc >1 • Desflurane reduces hepatic blood flow by 30% at conc of 1 MAC • Halothane results in greatest reduction hepatic blood flow and production of reactive intermediates during metabolism can result in halothane hepatitis • Nitrous oxide can lead to inhibition of methionine synthase resulting in Vit B12 deficiency with prolonged or repeated exposure • IV Anesthetics • May have increased risk for Propofol-related infusion syndrome with prolonged use
Patients with ascites have increased risk for aspiration requiring RSI and intubation (Succinylcholine may be CI) • Significant hemodynamic changes may occur, blood should be available with fluid warmer, pressors, consider utilizing rapid transfusion device
Hemorrhage • Electrolyte imbalance • Hypoglycemia • Hypothermia • DIC • Pulmonary insufficiency • (>90% patients will develop some form of resp complication such as atelectasis, effusion, PNA)
block can reduce hepatic blood flow and this effect may not be reversed when block related hypotension is corrected by catecholamines. • CI with coagulopathy and thrombocytopenia • Alternative nerve blockades may be appropriate such as TAP or ESP blocks • Tylenol, NSAIDs if labs within normal limits • PCA opioid analgesic
decompress portal HTN in setting of esophageal varices and/or intractable ascites. • CI: heart failure, pulmonary HTN, and severe tricuspid regurgitation • Sedation can be used but GA gives the benefit of limited patient movement, controls diaphragmatic excursion, and reduces risk of aspiration • Preop assessment of fluid and coagulation status • Complications • PTX or vascular injury while accessing jugular vein • Dysrhythmias during catheter insertion due to stimulation of endocardium • Hemorrhage secondary to extrahepatic artery or portal vein puncture
monitoring for low (<5cmH2O) to normal CV pressures help limit blood loss • Portal triad clamping well tolerated hemodynamically and has little effect on liver function. • Ischemic preconditioning followed by continuous inflow clamping for up to 75 mins was equally effective to intermittent inflow clamping for protection against postop liver injury • Air embolism can be a complication with larger hepatectomy and tumor near vena cava
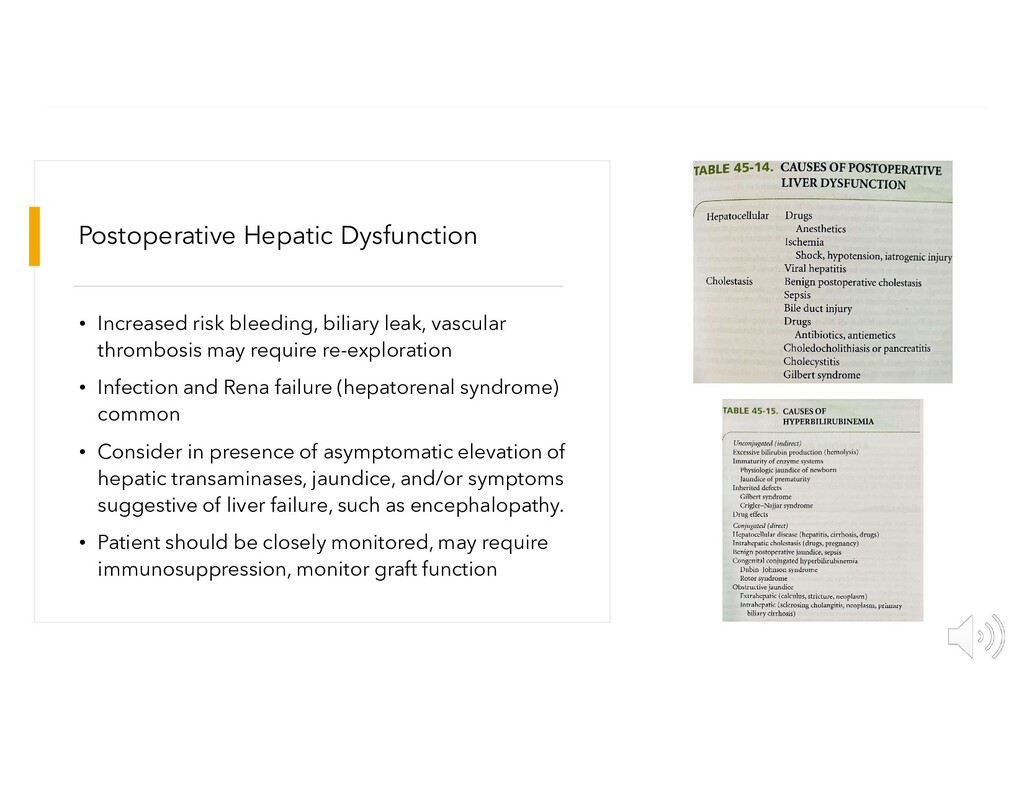
thrombosis may require re-exploration • Infection and Rena failure (hepatorenal syndrome) common • Consider in presence of asymptomatic elevation of hepatic transaminases, jaundice, and/or symptoms suggestive of liver failure, such as encephalopathy. • Patient should be closely monitored, may require immunosuppression, monitor graft function
estimates disease severity and 3 month survival in patients with chronic liver disease • Prioritizes organ allocation • Ranges from 6-40 points, calculated using • Serum bilirubin, serum creatinine, and INR • Patient with higher score are higher on transplant list and have a greater short term risk of dying from liver disease.
hepatic failure and life expectancy of less than 7 days without a liver transplant • Include patients who develop ALF without a history of liver disease, suffer from primary graft nonfunction or hepatic artery thrombosis within 7 days of a liver transplant, or have acutely decompensated Wilson disease
of hemodynamic changes related to blood loss and surgical compression of major vessels • Anhepatic - vascular occlusion of inflow to liver and ends with reperfusion • Neohepatic - opening portal vein and reperfusion of graft • reperfusion syndrome: cold, acidotic hyperkalemic solution that may contain emboli and vasoactive agents flushed from graft into Vena cava, may lead to hypotension, RV dysfunction, arrhythmia, even cardiac arrest, and may be preempted by prophylactic administration of ca chloride and sodium bicarbonate • Ischemic/reperfusion injury: impaired reperfusion due to severe endothelial dysfunction and rarely may lead to primary nonfunction of graft
intercostal muscles • Hypovolemia leads to hypotension and tachycardia and if not managed can result in shock • Patient my have decreased VR due to abdominal distension • Lab tests: CBC, BMP, ABG, EKG, type and cross • Avoid oral premedication, versed, opioids, anticholinergics
daily into the upper GI tract • SBO with vomiting may indicate about 3L fluid accumulated in bowel • If patient presents with hemodynamic instability then 6L can be present • Hinder diaphragmatic movement leading to decreased FRC, Vt which results in decreased PaO2 and increased PaCO2, • Decrease venous return secondary to decreased negative intrathoracic pressure and direct vena cava compression • Nasogastric decompression can reduce bowel distention improve pulmonary ventilation and reduce aspiration risk
• 2 large bore IVs • Arterial line (must determine if needed preinduction or postinduction depending on patients clinical status and PMHx) • CVC, CVP monitoring • Fluid warmers
to suction • Place patient in reverse Trendelenburg position • Preoxygenation with 100% O2 until End tidal O2 near 100% • Awake intubation with adequate airway analgesia vs. Rapid Sequence Induction with Etomidate (concern for hypotension) and Succinylcholine and ?cricoid pressure
intestinal obstruction will expand colon making it difficult for surgeon to operate • Increased bowel ischemia and necrosis • Extubate awake, LLD position, after return of upper airway reflexes
Postoperative Respiratory Problems • Abdominal distention and pain • Residual effects of inhaled and IV anesthetics • Reduction 15-20% FRC more than a week after any upper abdominal surgery
bronchospasm, and atelectasis • May exhibit tachycardia, tachypnea, coughing, cyanosis, and shock • Arterial hypoxemia earliest and most reliable sign of aspiration • Supportive management • Antibiotics only warranted in patients who show signs of a bacterial pulmonary infection with positive gram stain or culture, or those with known fecal material aspiration (as with lower intestinal obstruction)
persistent vomiting, abdominal pain with weight loss/anorexia, PUD, dyspepsia, heartburn despite medical therapy, diarrhea, hematemesis, or melena • Therapeutic indications for upper endoscopy: esophageal dilation, removal foreign body, sclerotherapy or banding esophageal varices, hemostasis with direct thermal or injection therapy, PEG tube placement, decompression of sigmoid volvulus or megacolon, polypectomy, ERCP, myotomy, stent placement • Colonoscopy indications: gross or occult bleeding, new onset constipation or unexplained diarrhea/abdominal pain, screening or surveillance inflammatory bowel disease, and screening for neoplasm
may require GETA • Preop • careful H&P • Assess risk of aspiration, bleeding, cardiovascular conditions, resp complications 2/2 chronic reflux, pancreatitis may present with ascites/ pleural effusions • Intraop • CO2 insufflation can increase risk of aspiration, may decrease VR, make ventilation difficult by reducing FRC • Pt positioning, supine vs LLD vs prone -> affect ventilation, aspiration risk, access to airway
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}