pre-operatively to enhance their body’s ability to cope with a stressful event and therefore improve their postoperative outcome. A group of interventions, integrated into the clinical pathway before a surgical procedure and aimed at both reducing imminent patient risk and promoting lasting beneficial effects on perioperative recovery and outcome.
a US national audit of patients undergoing elective orthopedic surgery, 35% of patients were found to have Hb levels <13 g/dL at preadmission testing 1 n In a large single-institution study in Spain, preoperative Hb was <13 g/dL in 19.4% of patients, and the prevalence of hematinic deficiencies was 33% for iron, 12.3% for vitamin B12 , and 3% for folate 2 n These results were also corroborated by a large series from Egypt and Scotland 3 1. Bierbaum BE et al. J Bone Joint Surg Am. 1999 2. Bisbe E et al. TATM. 2008 3. Saleh E et al. Br J Anaesth. 2007
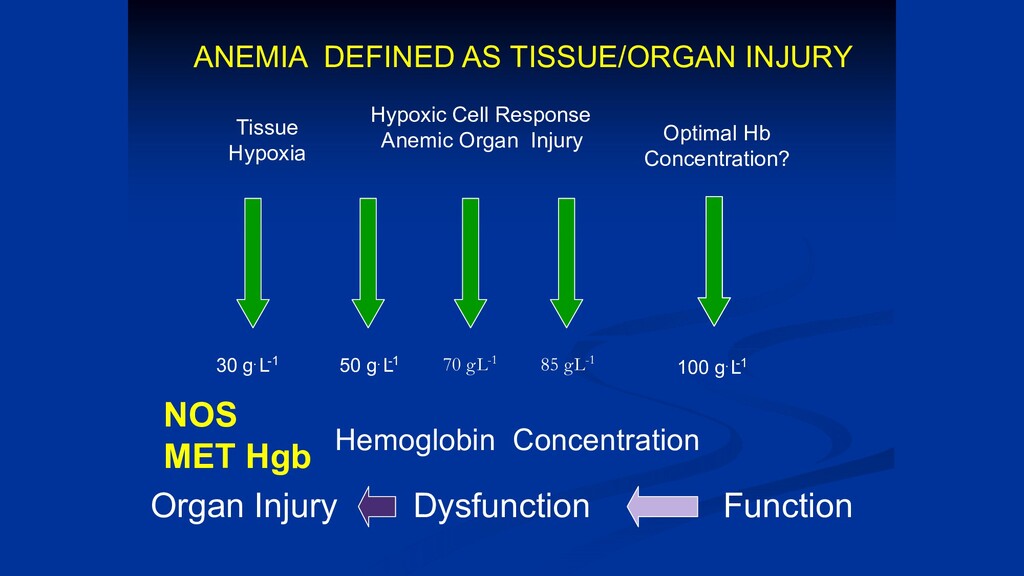
Hemoglobin Concentration 30 g L . -1 70 g.L-1 85 g.L-1 Tissue Hypoxia Hypoxic Cell Response Anemic Organ Injury Optimal Hb Concentration? Organ Injury Dysfunction Function ANEMIA DEFINED AS TISSUE/ORGAN INJURY NOS MET Hgb
anemia before reaching a “Transfusion Threshold (TRIGGER)” n Use of other treatments before allogeneic blood n Avoid daily blood draws unless absolutely needed n Nutritional supplements • Iron • Folic Acid • B 12
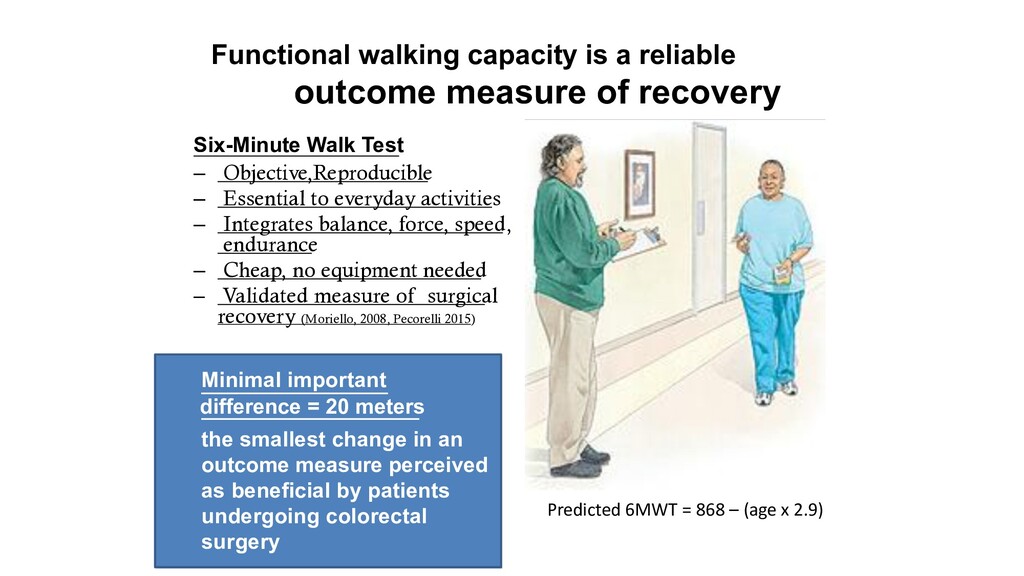
Six-Minute Walk Test – Objective,Reproducible – Essential to everyday activities – Integrates balance, force, speed, endurance – Cheap, no equipment needed – Validated measure of surgical recovery (Moriello, 2008, Pecorelli 2015) . Predicted 6MWT = 868 – (age x 2.9) Minimal important difference = 20 meters the smallest change in an outcome measure perceived as beneficial by patients undergoing colorectal surgery
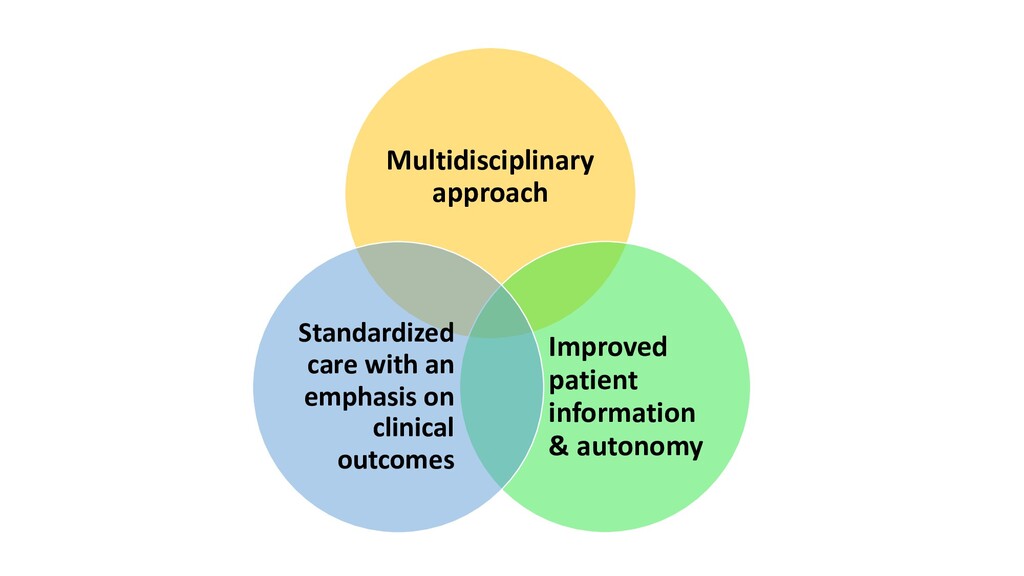
part of the ERAS program • • Requires a multidisciplinary approach Customize the program to each patient/surgery • • Proof of concept: increases functional capacity Can improve postoperative outcome
to minimize symptom burden, enhance functional recovery, improve outcomes and enable delivery of safe, effective, and value-based care to an increasing number of patients.
and they were assumed as a dogma. Preoperative prolonged fasting, Mechanical bowel preparation and nasogastric tubes were thought to be necessary to empty the bowel to prevent intraoperative contamination and to prevent early passage of bowel content through an anastomotic suture line while it is healing. Drain tube was believed essential in any GIT surgery. Prolonged bed rest were recommended to facilitate abdominal wall healing.
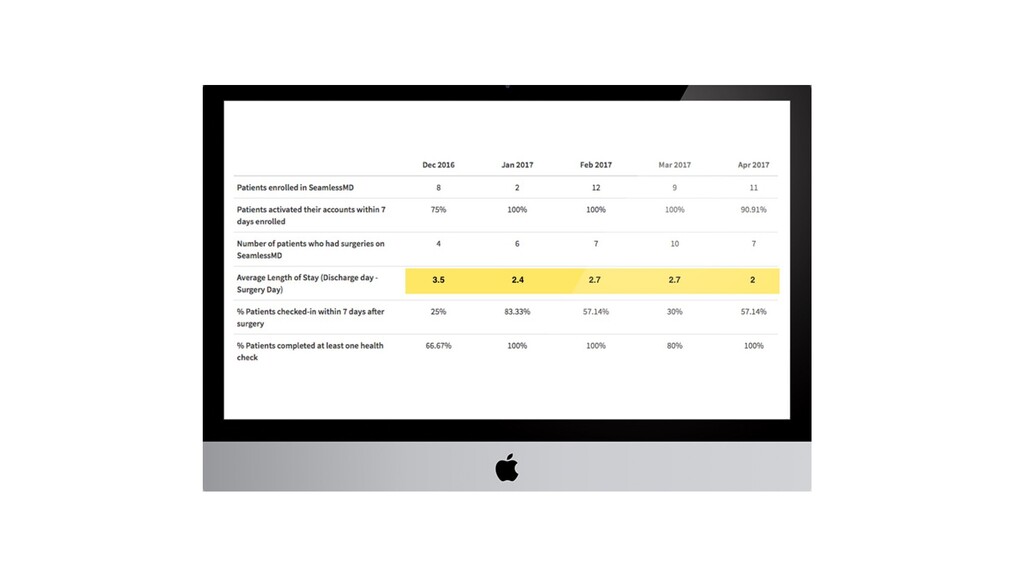
2 weeks •Schedule meetings for the next 6 month •Plan audit process 0-2 month •Review best practices •Write draft protocol 3 month •Present draft to multidisciplinary team •Stakeholders sign off on the final draft 5 month •Create patient education app with SeamlessMD •Educate front line staff 6 month •Set launch date •Launch pilot 9 month •Gather all stakeholders for presentation 12 month •Estimate completion of the pilot Timeline
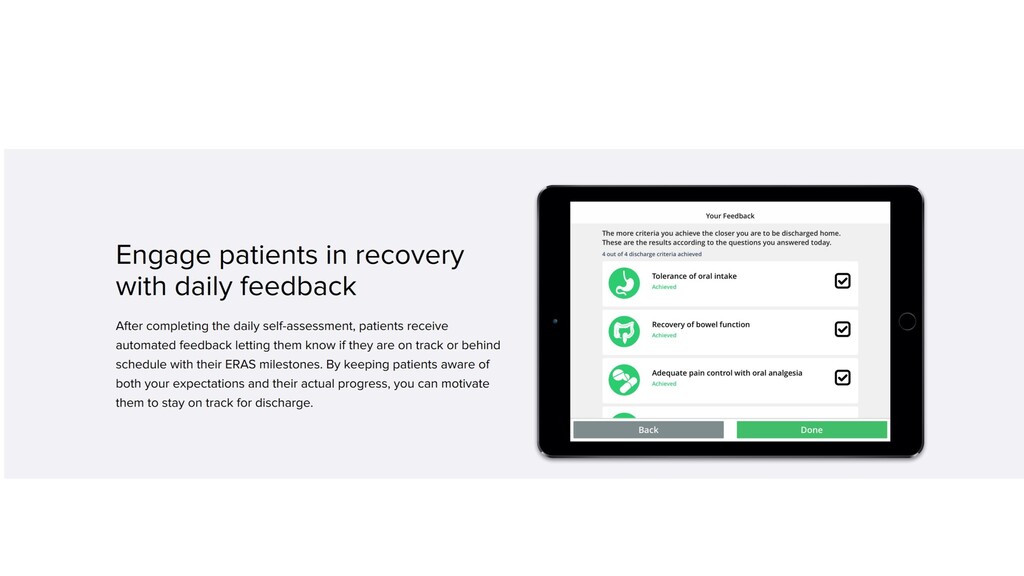
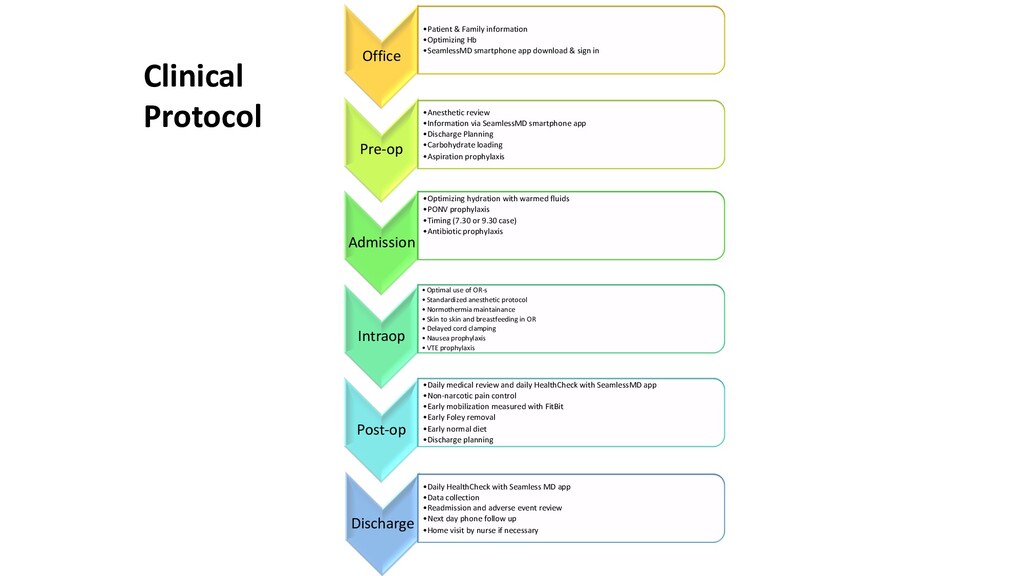
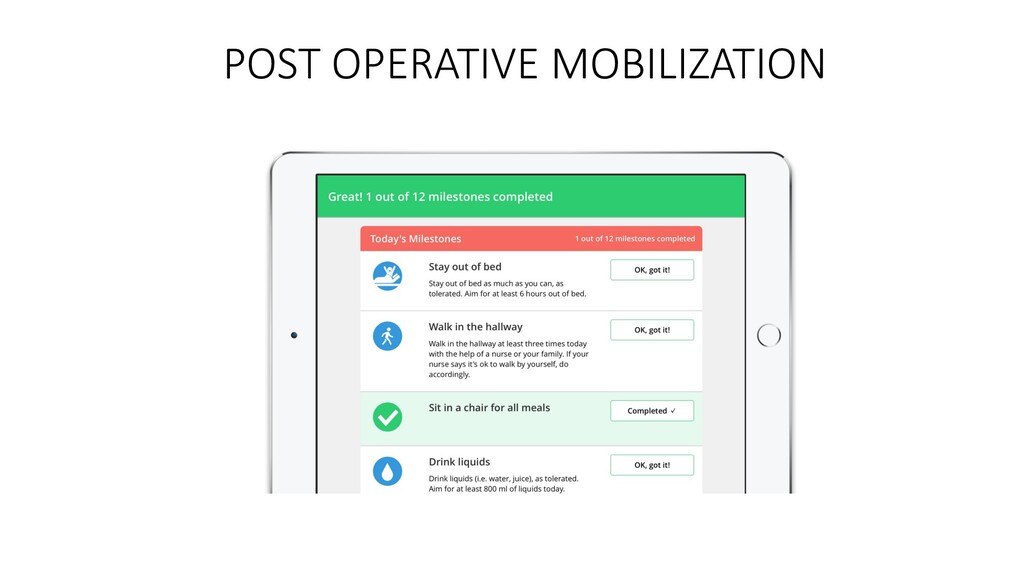
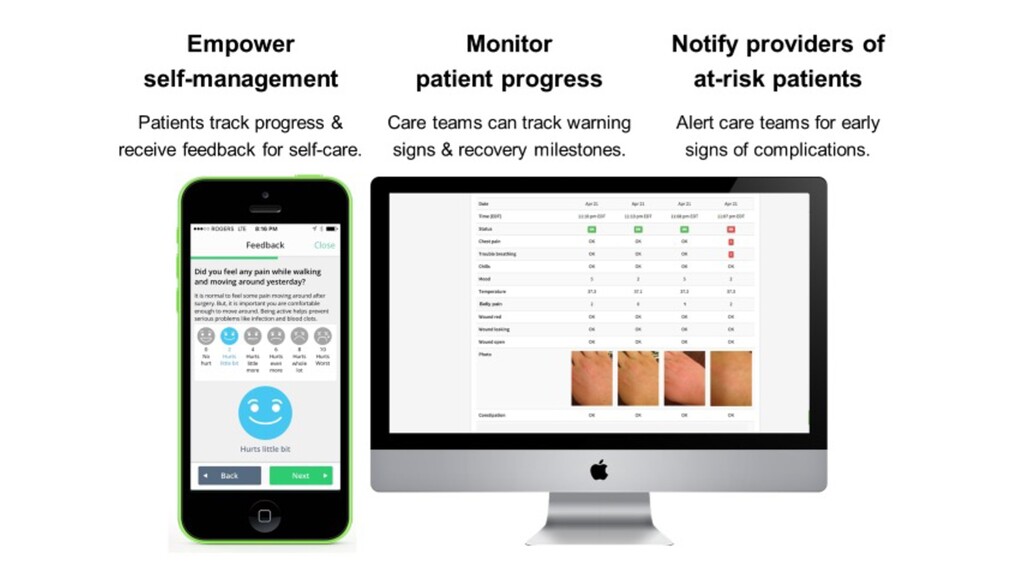
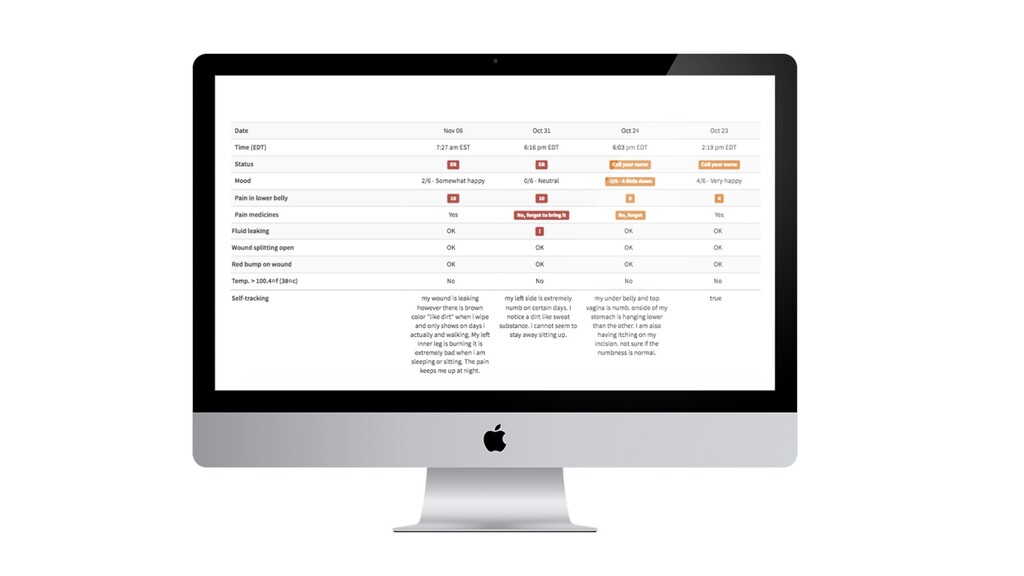
download & sign in Pre-op •Anesthetic review •Information via SeamlessMD smartphone app •Discharge Planning •Carbohydrate loading •Aspiration prophylaxis Admission •Optimizing hydration with warmed fluids •PONV prophylaxis •Timing (7.30 or 9.30 case) •Antibiotic prophylaxis Intraop •Optimal use of OR-s •Standardized anesthetic protocol •Normothermia maintainance •Skin to skin and breastfeeding in OR •Delayed cord clamping •Nausea prophylaxis •VTE prophylaxis Post-op •Daily medical review and daily HealthCheck with SeamlessMD app •Non-narcotic pain control •Early mobilization measured with FitBit •Early Foley removal •Early normal diet •Discharge planning Discharge •Daily HealthCheck with Seamless MD app •Data collection •Readmission and adverse event review •Next day phone follow up •Home visit by nurse if necessary Clinical Protocol
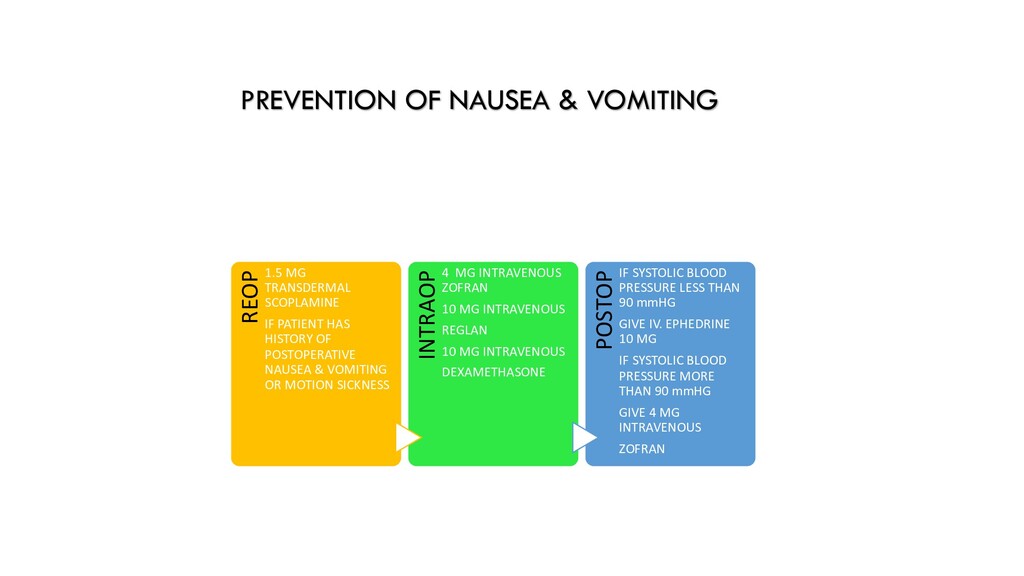
IF PATIENT HAS HISTORY OF POSTOPERATIVE NAUSEA & VOMITING OR MOTION SICKNESS INTRAOP 4 MG INTRAVENOUS ZOFRAN 10 MG INTRAVENOUS REGLAN 10 MG INTRAVENOUS DEXAMETHASONE POSTOP IF SYSTOLIC BLOOD PRESSURE LESS THAN 90 mmHG GIVE IV. EPHEDRINE 10 MG IF SYSTOLIC BLOOD PRESSURE MORE THAN 90 mmHG GIVE 4 MG INTRAVENOUS ZOFRAN
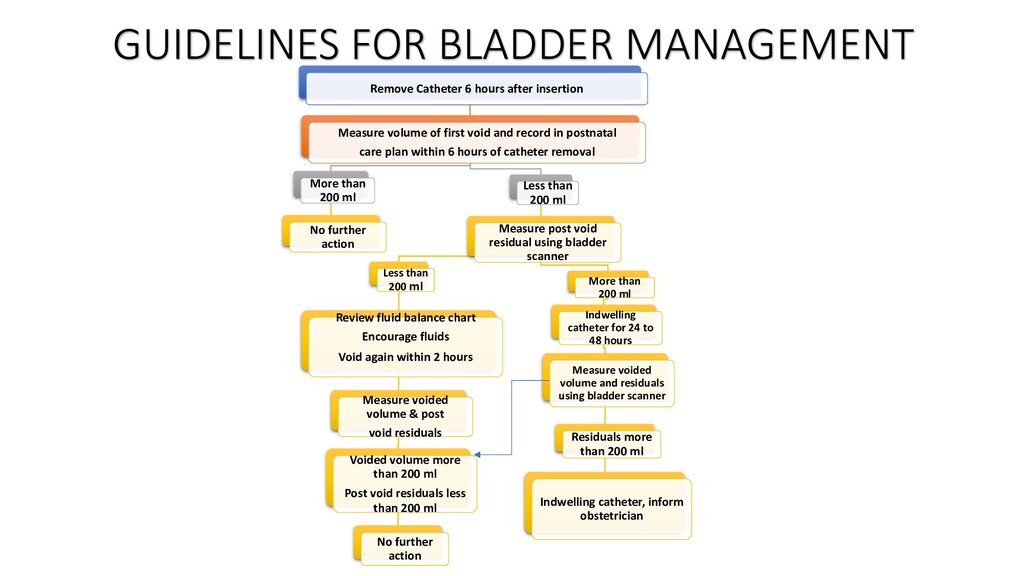
void and record in postnatal care plan within 6 hours of catheter removal More than 200 ml No further action Less than 200 ml Measure post void residual using bladder scanner Less than 200 ml Review fluid balance chart Encourage fluids Void again within 2 hours Measure voided volume & post void residuals Voided volume more than 200 ml Post void residuals less than 200 ml No further action More than 200 ml Indwelling catheter for 24 to 48 hours Measure voided volume and residuals using bladder scanner Residuals more than 200 ml Indwelling catheter, inform obstetrician GUIDELINES FOR BLADDER MANAGEMENT
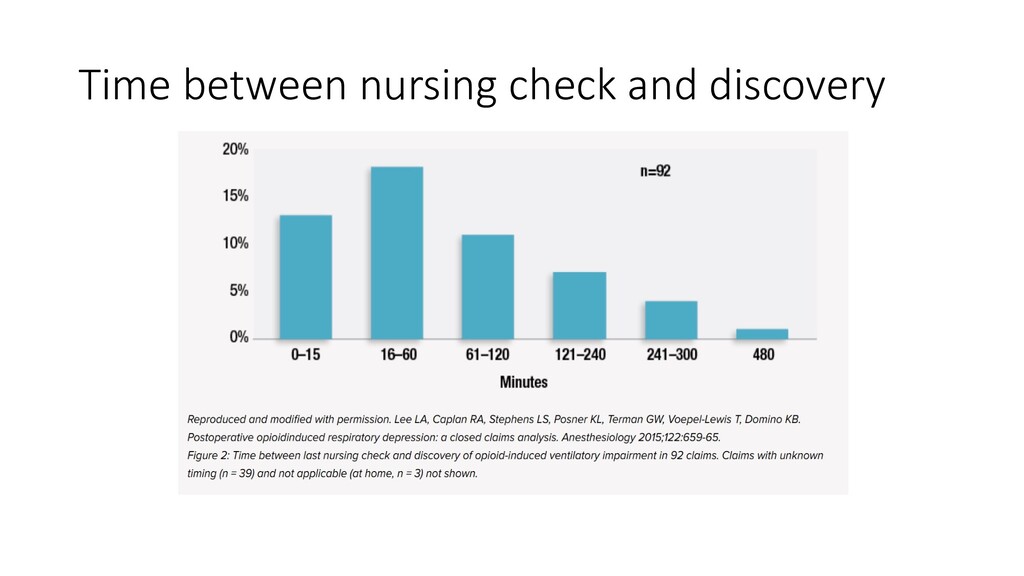
continuous ward monitoring should be the standard-of-care for high risk patients since vital signs at 4- to 6-h intervals clearly miss many (and probably most) rescue opportunities and 90% of the adverse events are happening on POD 1.
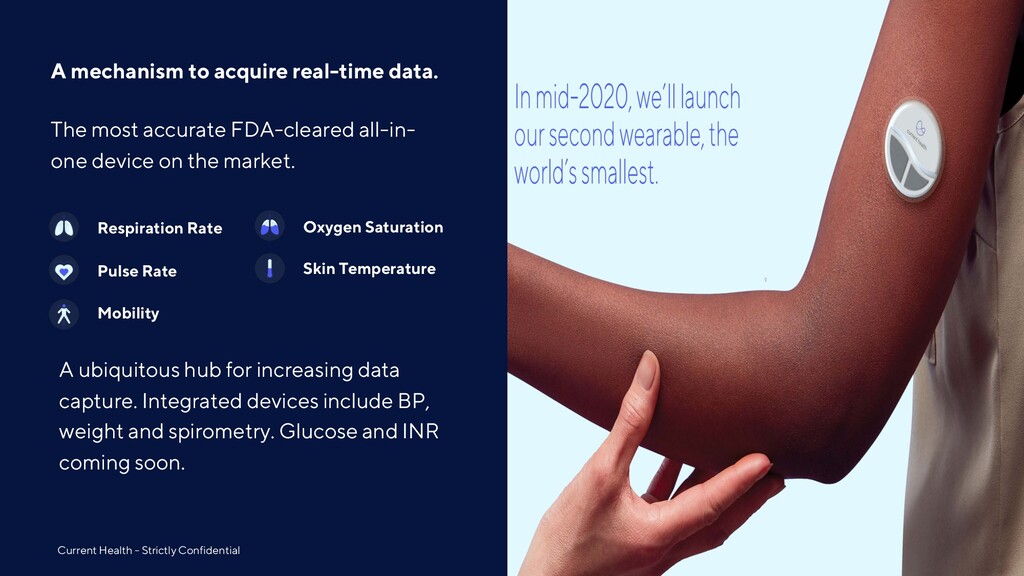
Confidential 10 The most accurate FDA-cleared all-in- one device on the market. Respiration Rate Pulse Rate Oxygen Saturation Skin Temperature Mobility A ubiquitous hub for increasing data capture. Integrated devices include BP, weight and spirometry. Glucose and INR coming soon.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}