of cancer pain Discuss pharmacologic treatment options, including anti-inflammatories, anticonvulsants, antidepressants Discuss intrathecal delivery system Discuss neurolysis for cancer pain, including alcohol and phenol Discuss neurosurgical options for cancer pain
is 65 60-90% of pts will have pain Pain from disease or treatment? In pediatrics, it is more commonly from treatment Pain as first sx of cancer tends to indicate advanced disease and is an independent predictor of poor prognosis
treatment In geriatric population, comorbidities and drug-drug interactions need to be taken into effect In patients with substance abuse history, there is greater reliance on diagnostic imaging Inmates have higher rates of cancer, increased mortality, and undertreated symptoms
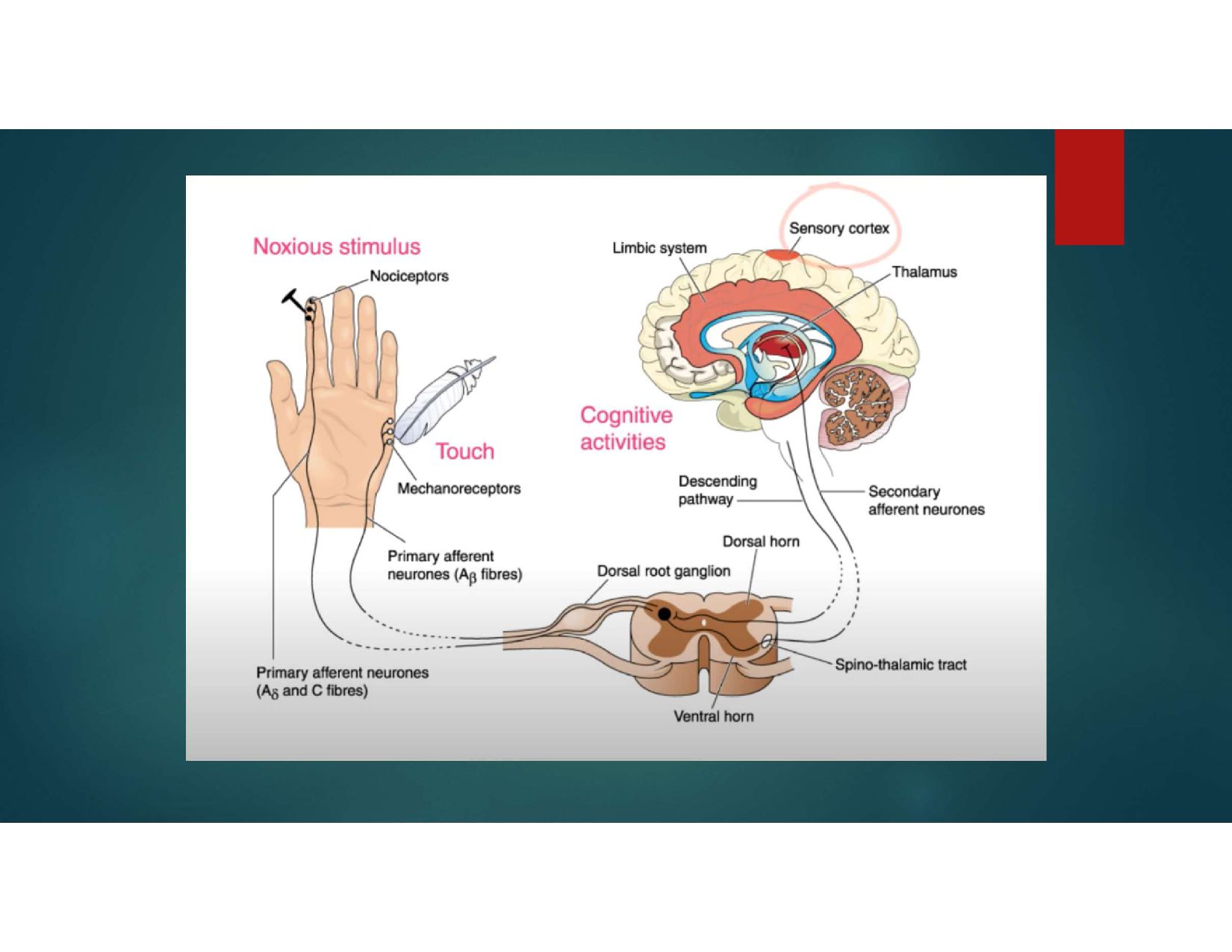
growth factor, Cytokines, ATP, Protons from dying cells These substances activate primary afferent and awaken silent nociceptors (feed forward loop) Primary afferent discharge leads to dorsal horn hyperexcitation and the activation of microglia Peripheral inhibition via activation of peripheral and central opioid receptors, Cox pathways and descending modulation
(via compression or ischemia/ hemorrhage, chemical or transection). Peripheral damage accumulation of abnormal sodium and calcium channels at the site of injury Alterations to gene expression of receptors Damaged neurons discharge spontaneously and there is cross-talk to normal fibers and recruitment of silent nociceptors Excessive or absent discharge from primary afferents within the dorsal horn results in overall excitation an alteration in expression of NMDA receptors and functional loss of opioid and gabaminergic systems There is resultant hyperexcitation with increased receptive fields primary and secondary hyperalgesia, and allodynia Dorsal columns relay predominately to thalamus, giving rise to strong autonomic responses and efferent responses
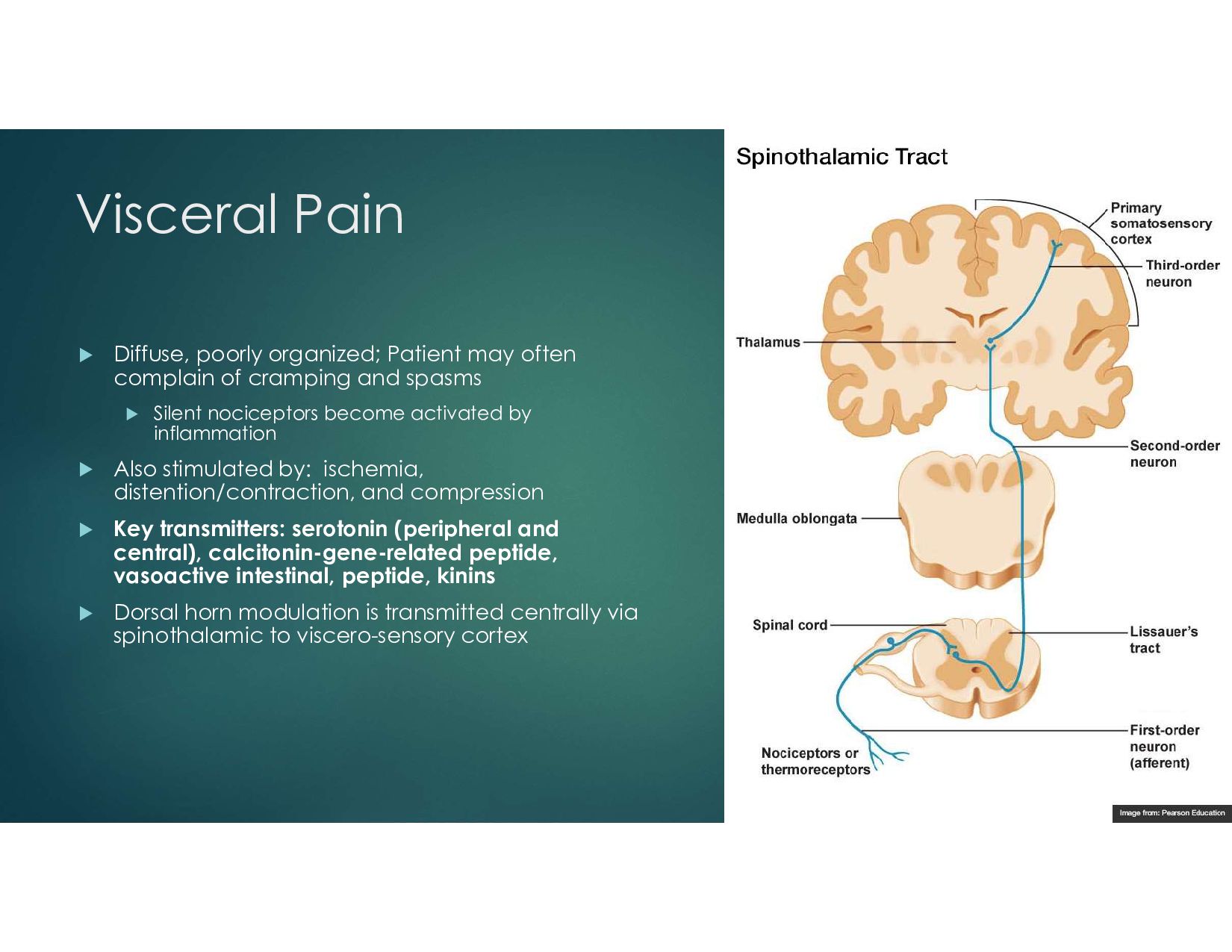
of cramping and spasms Silent nociceptors become activated by inflammation Also stimulated by: ischemia, distention/contraction, and compression Key transmitters: serotonin (peripheral and central), calcitonin-gene-related peptide, vasoactive intestinal, peptide, kinins Dorsal horn modulation is transmitted centrally via spinothalamic to viscero-sensory cortex
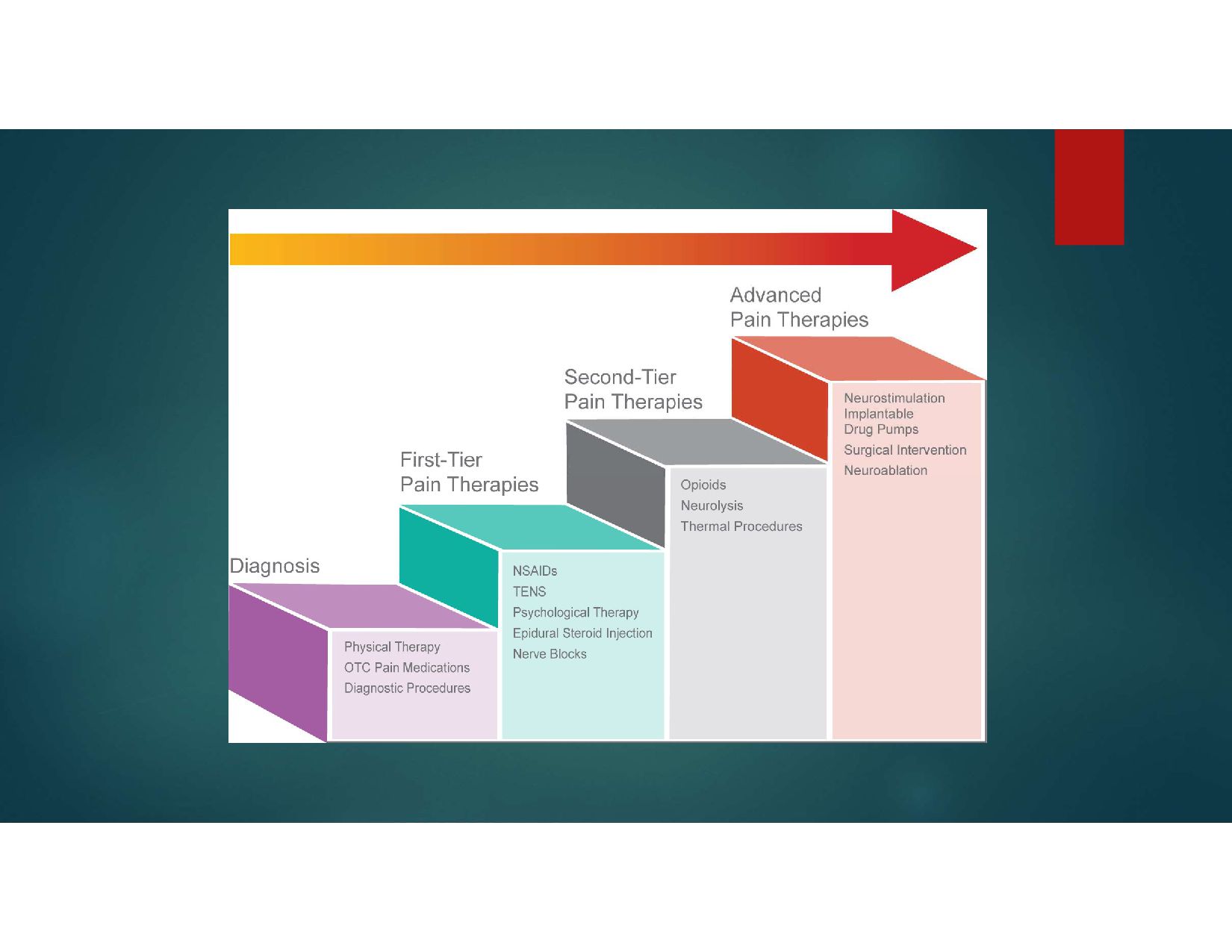
ibuprofen - Non specific - sulindac - Cyclooxygenase II specific Celecoxib and Meloxicam Anticonvulsant Agents Antidepressants Mixed mu agonists Mu agonists Alpha 2 agonists
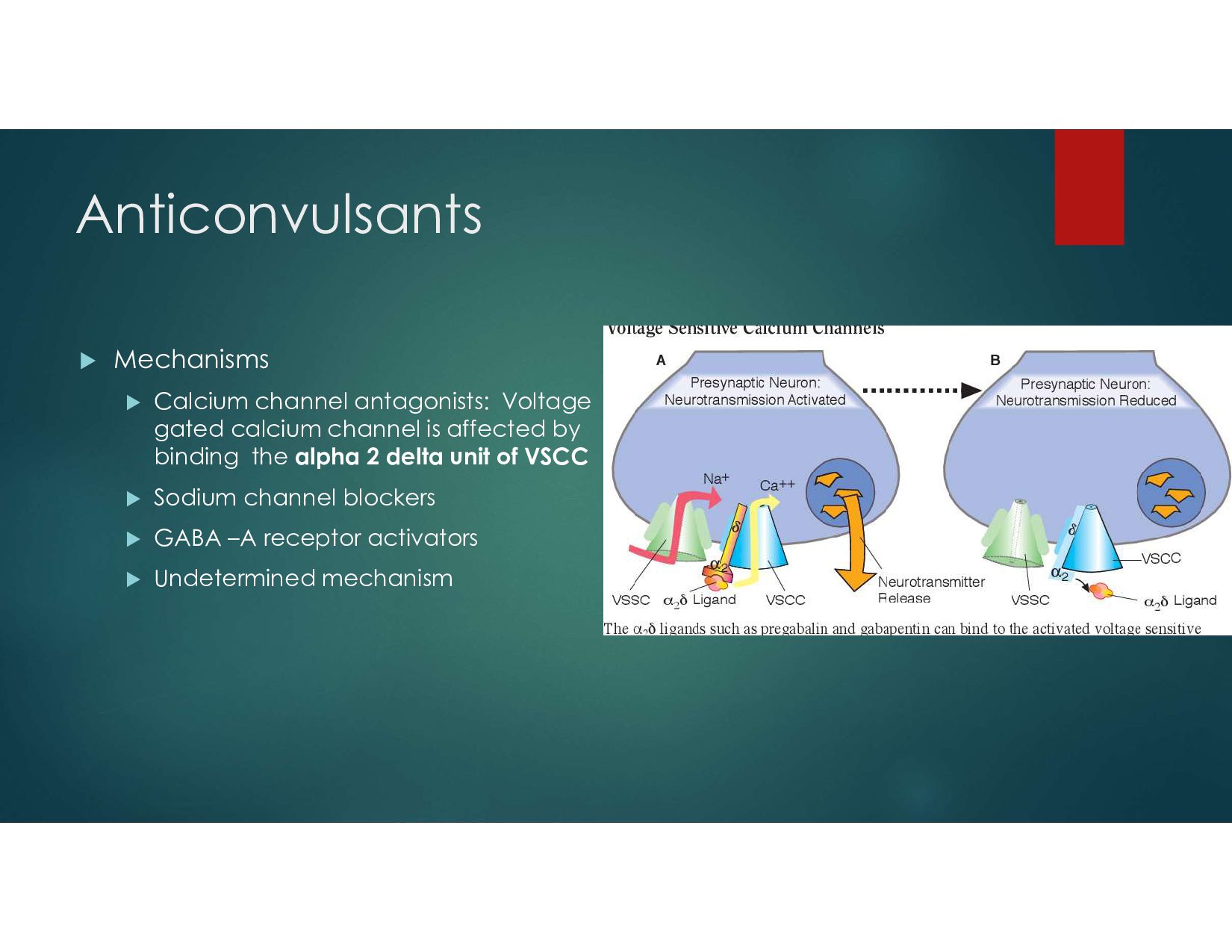
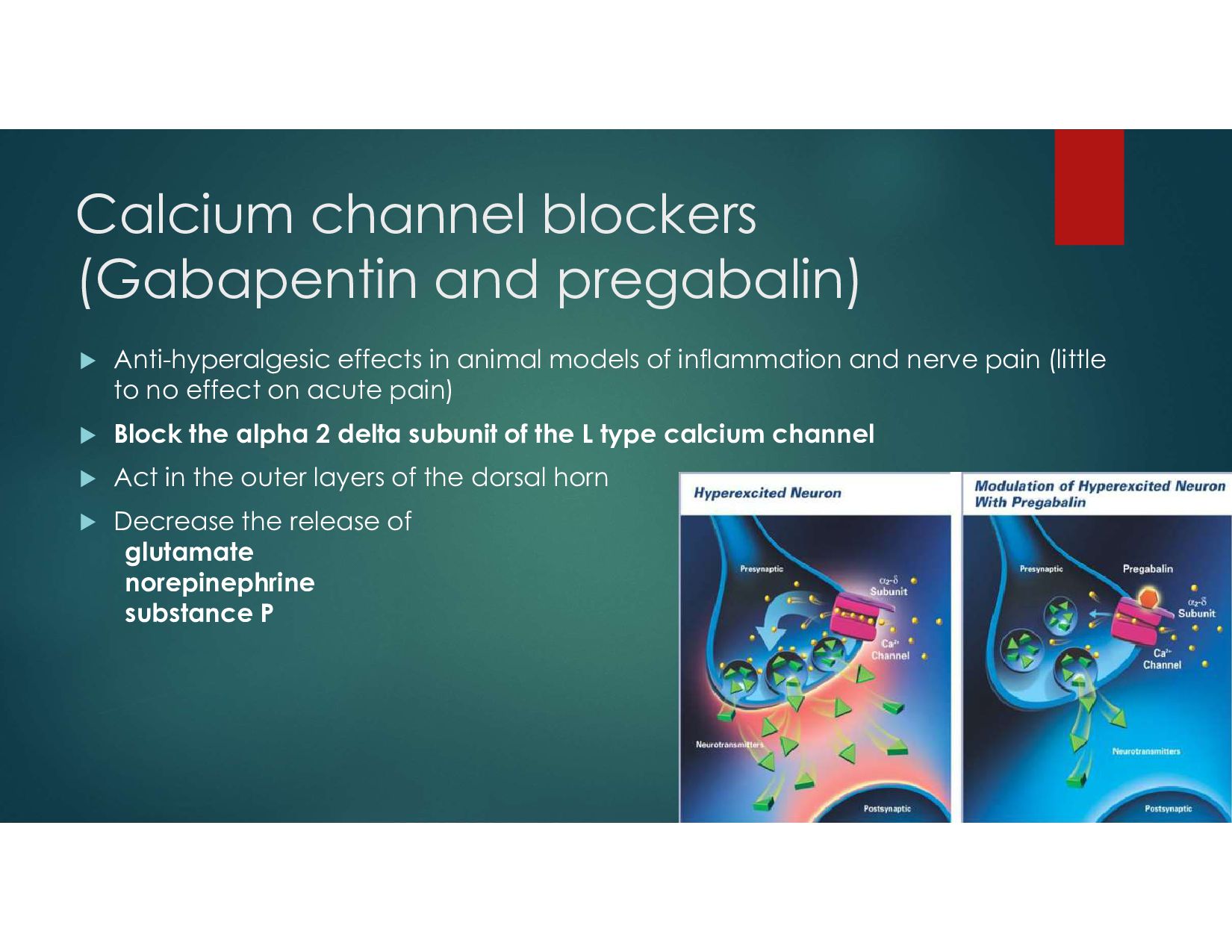
animal models of inflammation and nerve pain (little to no effect on acute pain) Block the alpha 2 delta subunit of the L type calcium channel Act in the outer layers of the dorsal horn Decrease the release of glutamate norepinephrine substance P
efficacy at 2 weeks vs 2 months Fewer side effects, but still caution in renal disease Dosed : 25 – 75 mg QHS in elderly to max of 150 mg po/day In Diabetic Neuropathy: NNT =6.3
fibers with no effect on normal functioning A-delta and C-fibers Dose Initial 100mg po bid to tid Side effects: PANCYTOPENIA - agranulocytosis and aplastic anemia; CBC necessary every three weeks (blood tests 2-4 months) Steven Johnson Syndrome Toxic Epidermal Necrolysis Dizziness and gait disturbance Treatment models TG neuralgia- NNT<2, NNH 24 post CVA pain
Dose: 100mg Bid Side effects: Change in facial features (coarsening) Gingival hyperplasia sedation changes in motion stability Treatment models: Still used in recalcitrant oncology related pain Increases activity of cP450, decreasing efficacy of methadone, fentanyl, tramadol, mexiletine, lamotrigine, carbamazepine When co-administered with antidepressants, and valproic acid, the decreased activity of p450 will produce increased concentration of phenytoin
levels approximating 50-100 mcg/ml but these doses are never used when treating chronic pain Mech: GABA–A receptor agonist Side effects: CNS depression Target treatment groups: Change in migraine therapy, suppress cns compression by tumor
patch Useful near drain sites, chest tubes, recent large incisions Side effects include dizziness and blurred vision and at concentrations of 10mcg/ml, seizure and 25 mcg/ml cardiac depression, but these plasma levels do not result from the patches Lidocaine Patch
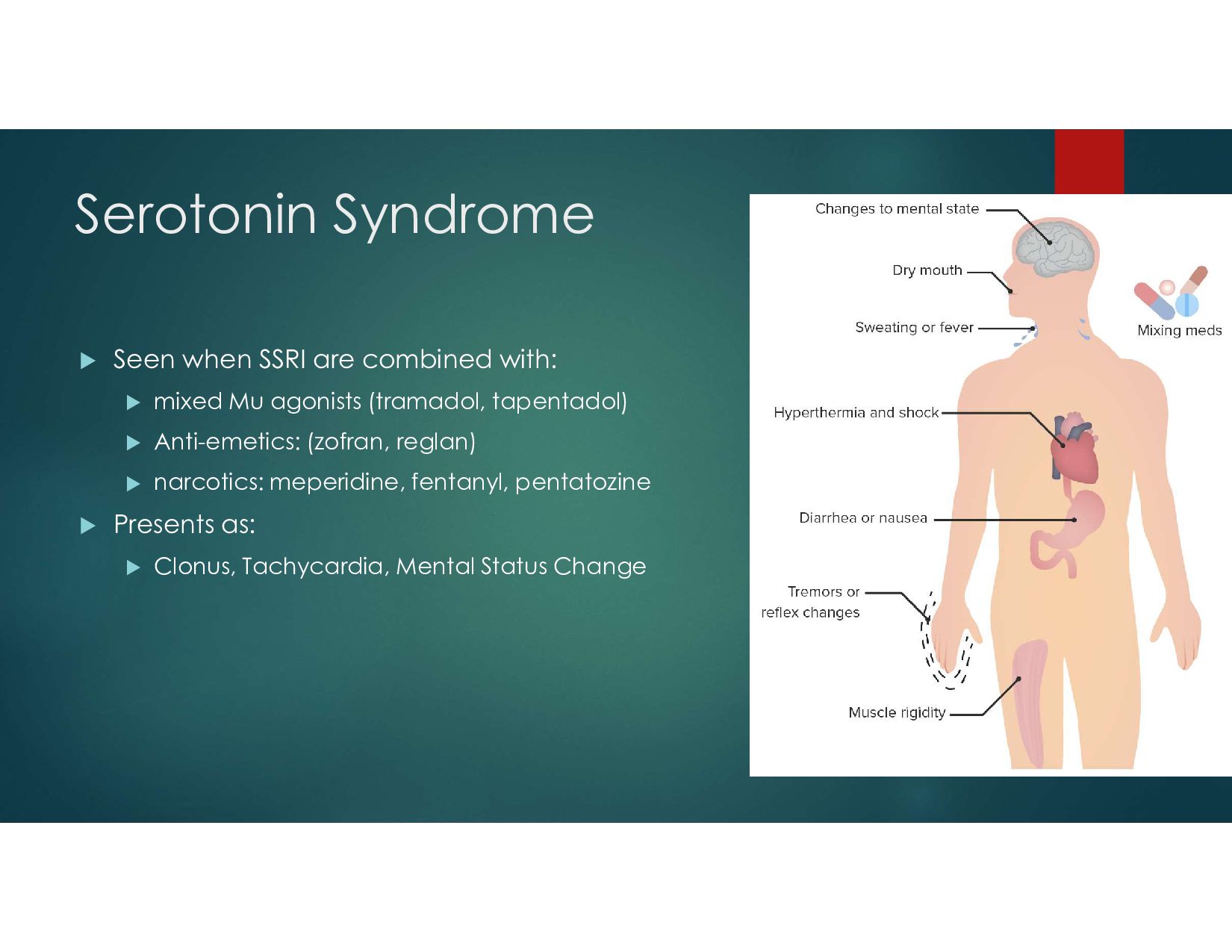
associated with chronic pain or resulting from the chronic painful condition There are three basic categories: TCA - example Elavil (amitriptyline) SSRI - example Prozac (fluoxetine; rarely used in oncology patients due to serotonin syndrome) SNRI – example Cymbalta (duloxetine)
and norepi, increasing synaptic levels of these meds They have independent analgesic properties at lower doses Differ in terms of side effects: anticholinergic, (dry mouth, constipation, blurred vision, urinary retention) antihistamine effects (sedation)
TCAs prolong the QT interval TCA decrease seizure threshold Some TCAs have documented analgesic properties All TCAs cause urinary retention, dry mouth, postural hypotension, weight gain Hepatic clearance involves the p450 system Meds which compete for the enzyme will increase levels when co-administered (SSRI, cimetidine, methylphenidate) P450 enzyme inducers will decrease serum TCA levels (phenobarbital, carbamazepine, cigarette smoking)
than TCA, but decrease seizure threshold Associated with easy bruising and osteoporosis Side effects include decreased libido, impotence, dystonia, akathisia, rare SIADH Few independent pain properties Never proven to be opioid sparing when compared to TCA Taper off slowly
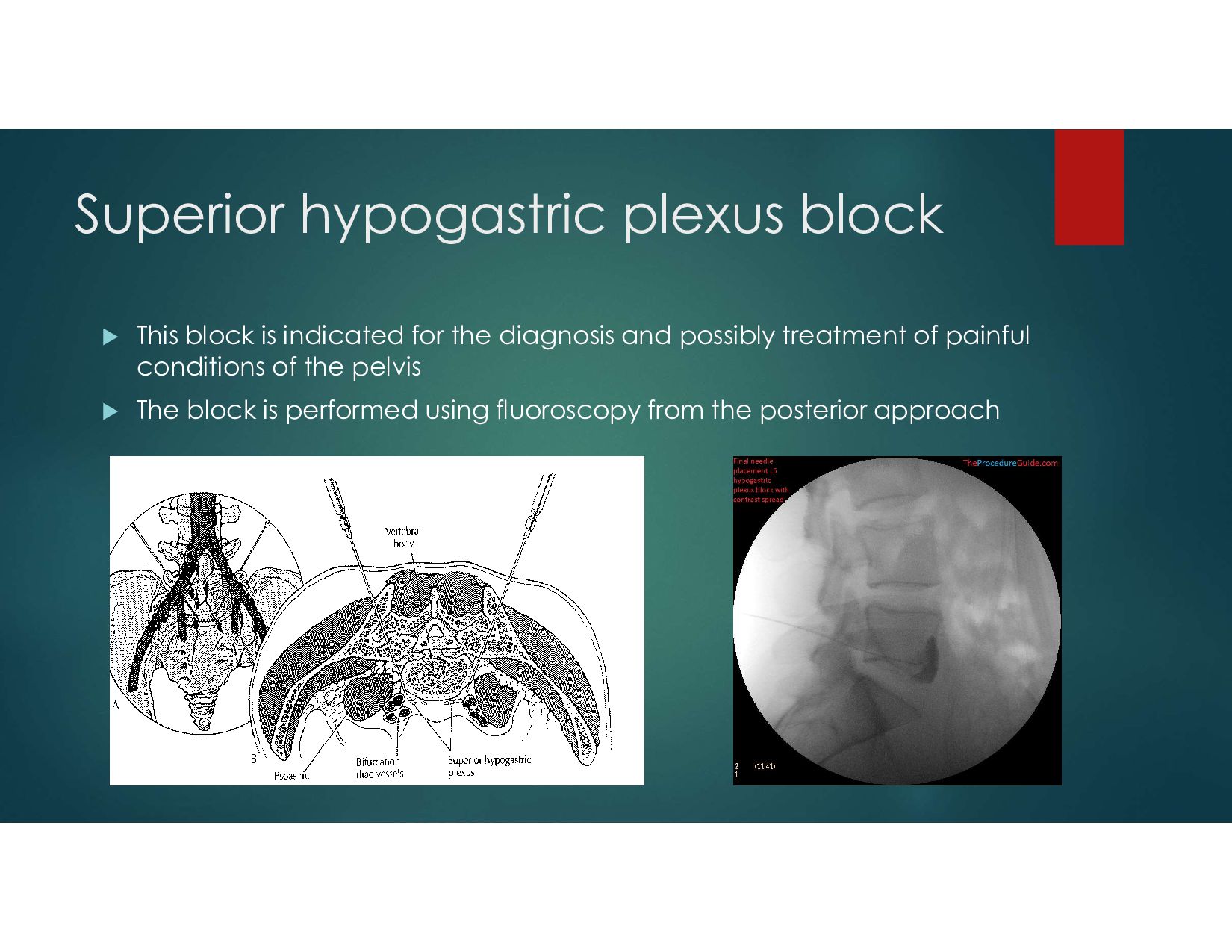
Superior Hypogastric Plexus Block Uses: Pancreatitis, acute and chronic Diagnostic Treatment of abdominal ischemia Treatment of acute pain after arterial embolization for cancer pain Treatment of pain secondary to upper abdominal malignancy
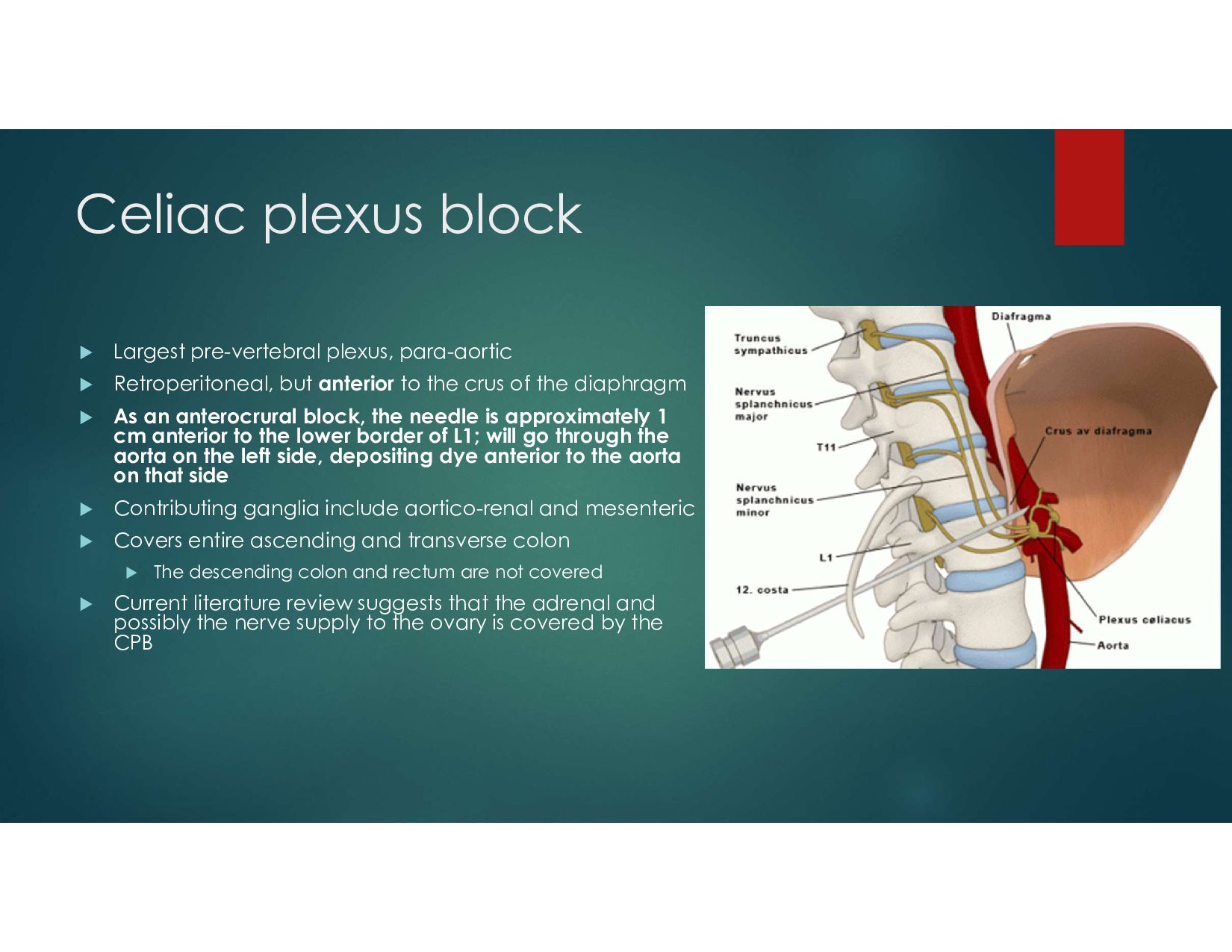
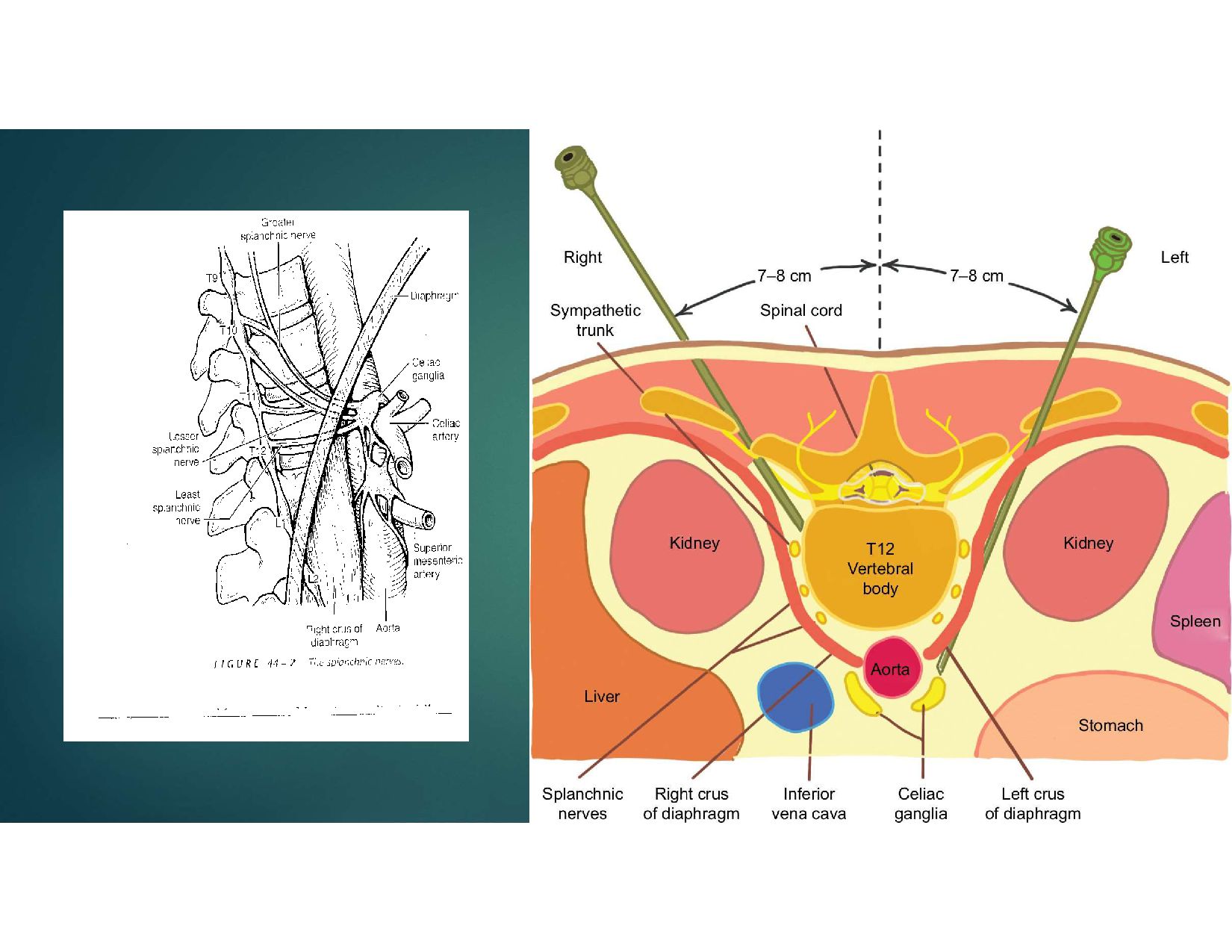
but anterior to the crus of the diaphragm As an anterocrural block, the needle is approximately 1 cm anterior to the lower border of L1; will go through the aorta on the left side, depositing dye anterior to the aorta on that side Contributing ganglia include aortico-renal and mesenteric Covers entire ascending and transverse colon The descending colon and rectum are not covered Current literature review suggests that the adrenal and possibly the nerve supply to the ovary is covered by the CPB
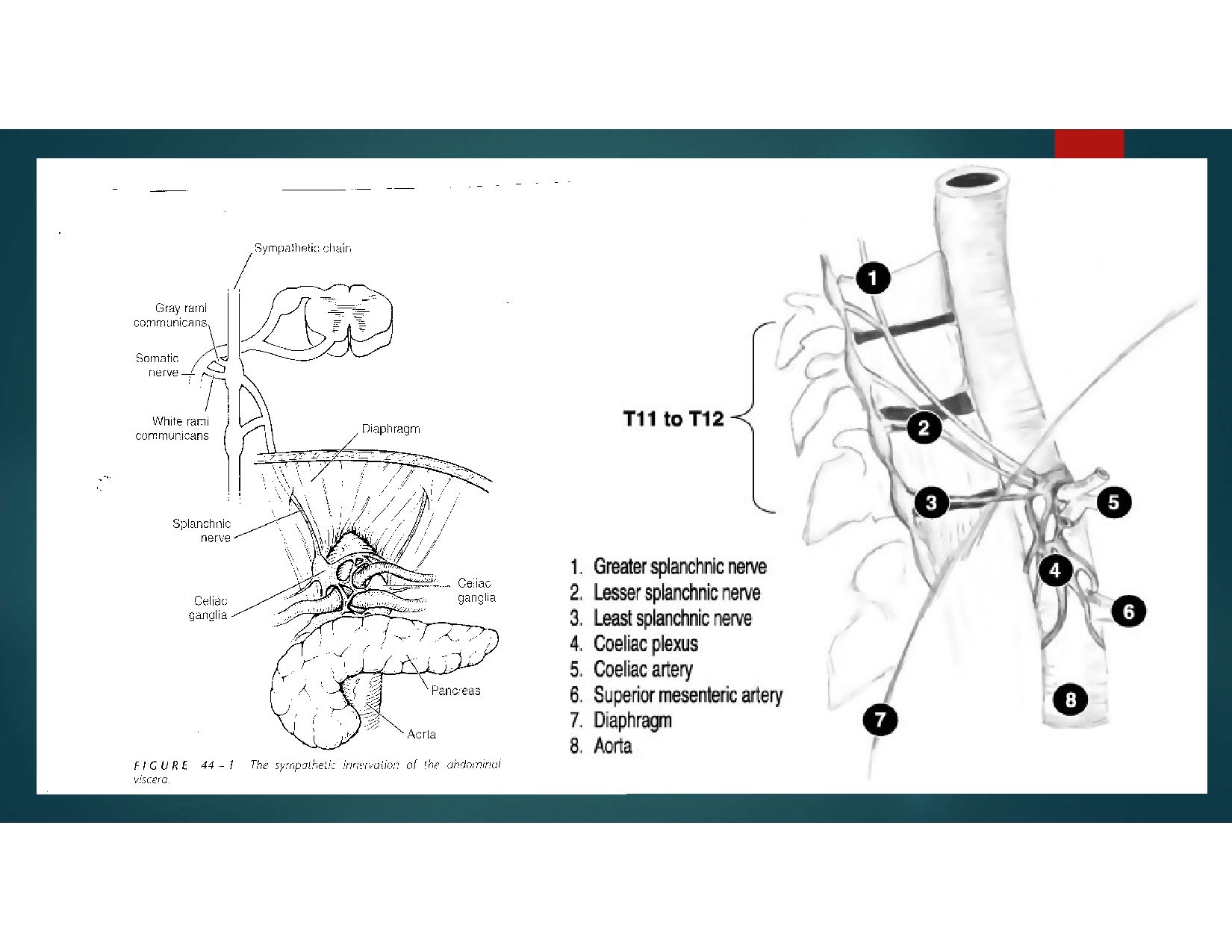
the SPLANCHNIC NERVES Afferent sensory fibers C type silent nociceptors which run with the above fibers Parasympathetic fibers from the vagus nerve Sympathetic afferents
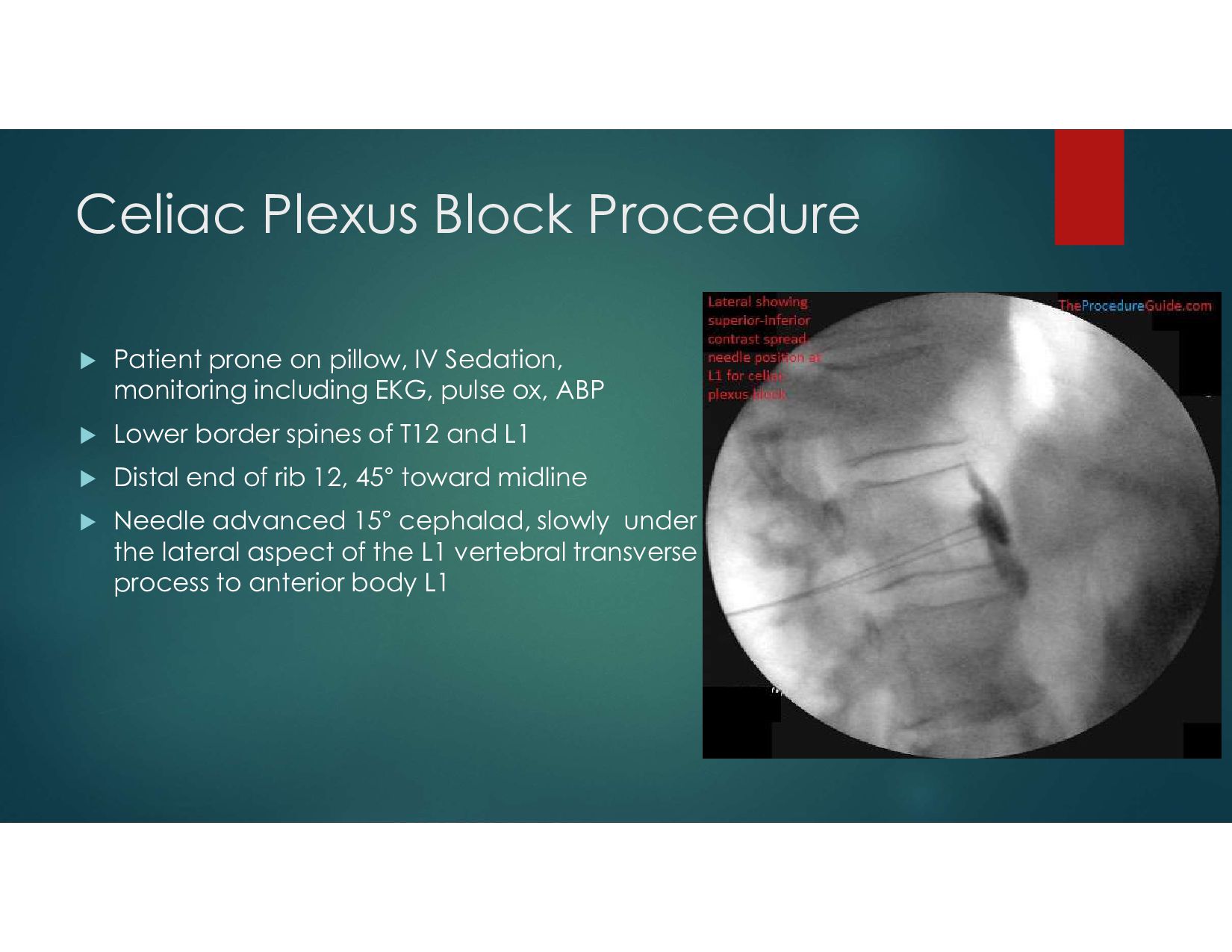
Sedation, monitoring including EKG, pulse ox, ABP Lower border spines of T12 and L1 Distal end of rib 12, 45° toward midline Needle advanced 15° cephalad, slowly under the lateral aspect of the L1 vertebral transverse process to anterior body L1
local anesthetic + steroid Neurolytic same volume of phenol or alcohol after successful block following contrast dye study Phenol 6%-12% anesthetic hyperbaric delayed effects Alcohol painful on injection hypobaric immediate effects alcohol has been associated with spasm of the major spinal arteries causing transient paralysis
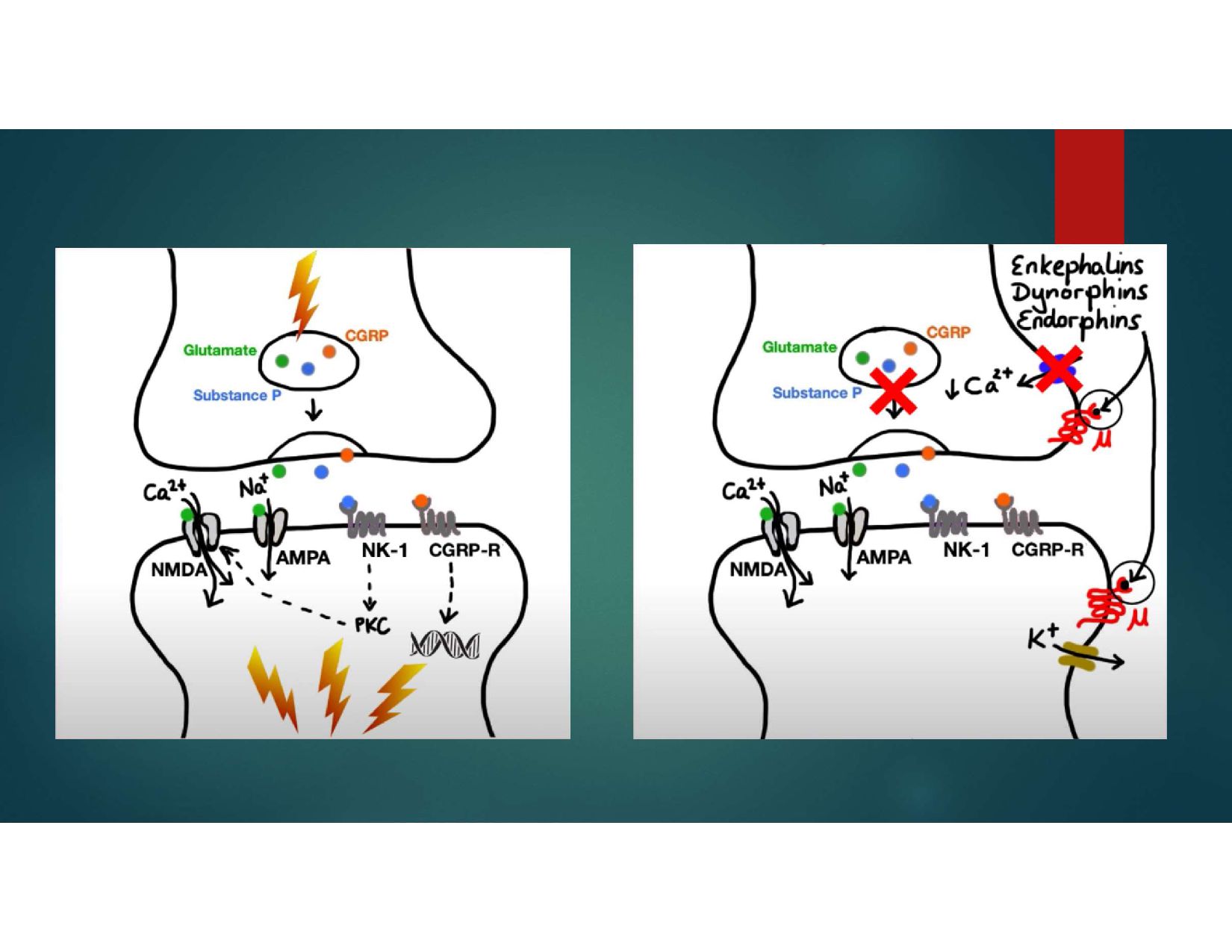
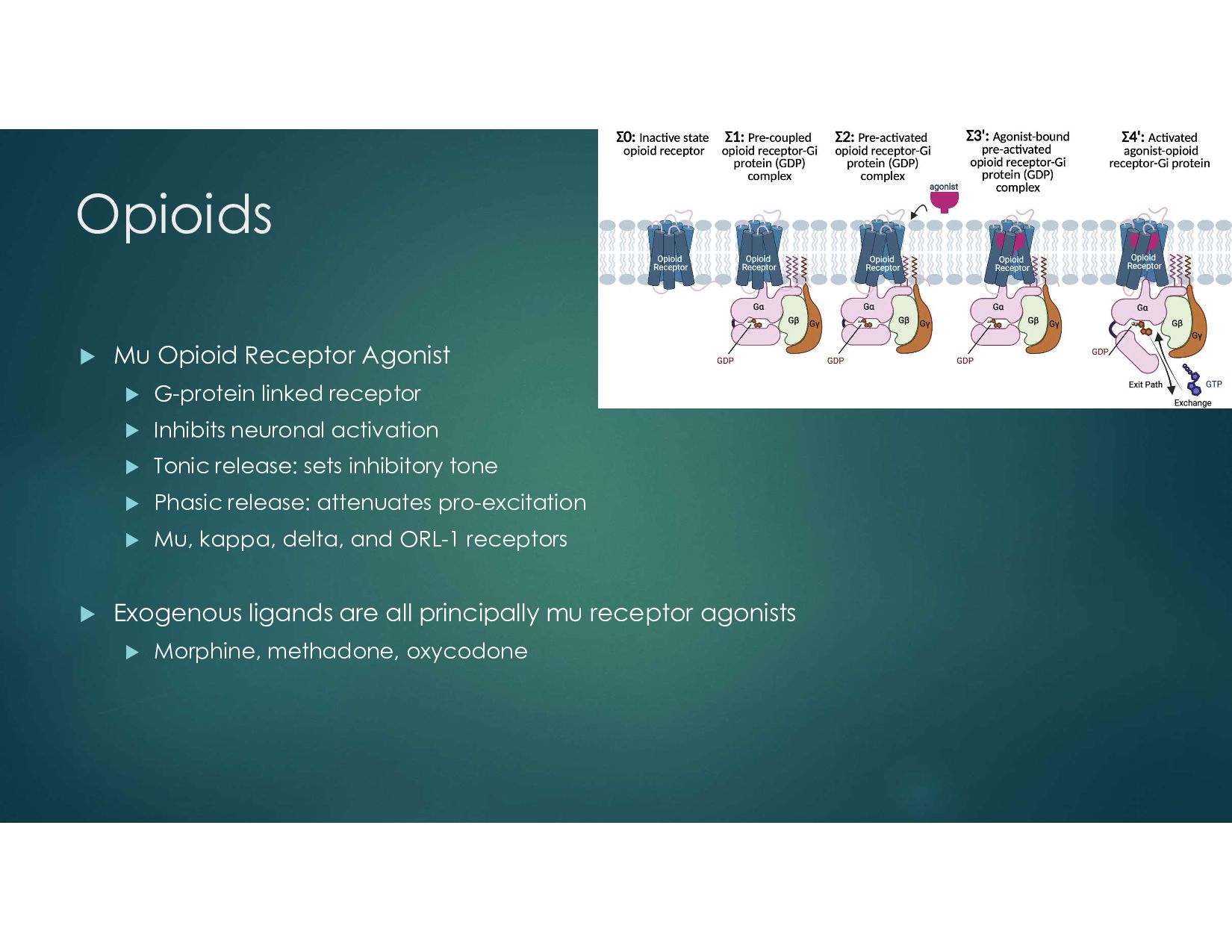
by interacting with mu, delta or kappa opioid receptors The opioid receptors are coupled to G1 proteins and the actions of the opioids are mainly inhibitory They close N-type voltage-operated calcium channels and open calcium- dependent inwardly-rectifying potassium channels This results in hyperpolarization and a reduction in neuronal excitability They also decrease intracellular cAMP which modulates the release of nociceptive neurotransmitters (e.g. substance P)
therapy Surgical decompression for spinal tumors Non surgical decompression- Cryotherapy, RFA Chemical Denervation of tumor involved areas Augmentation of tumor involved areas Spinal Cord Stimulation Intrathecal Pumps
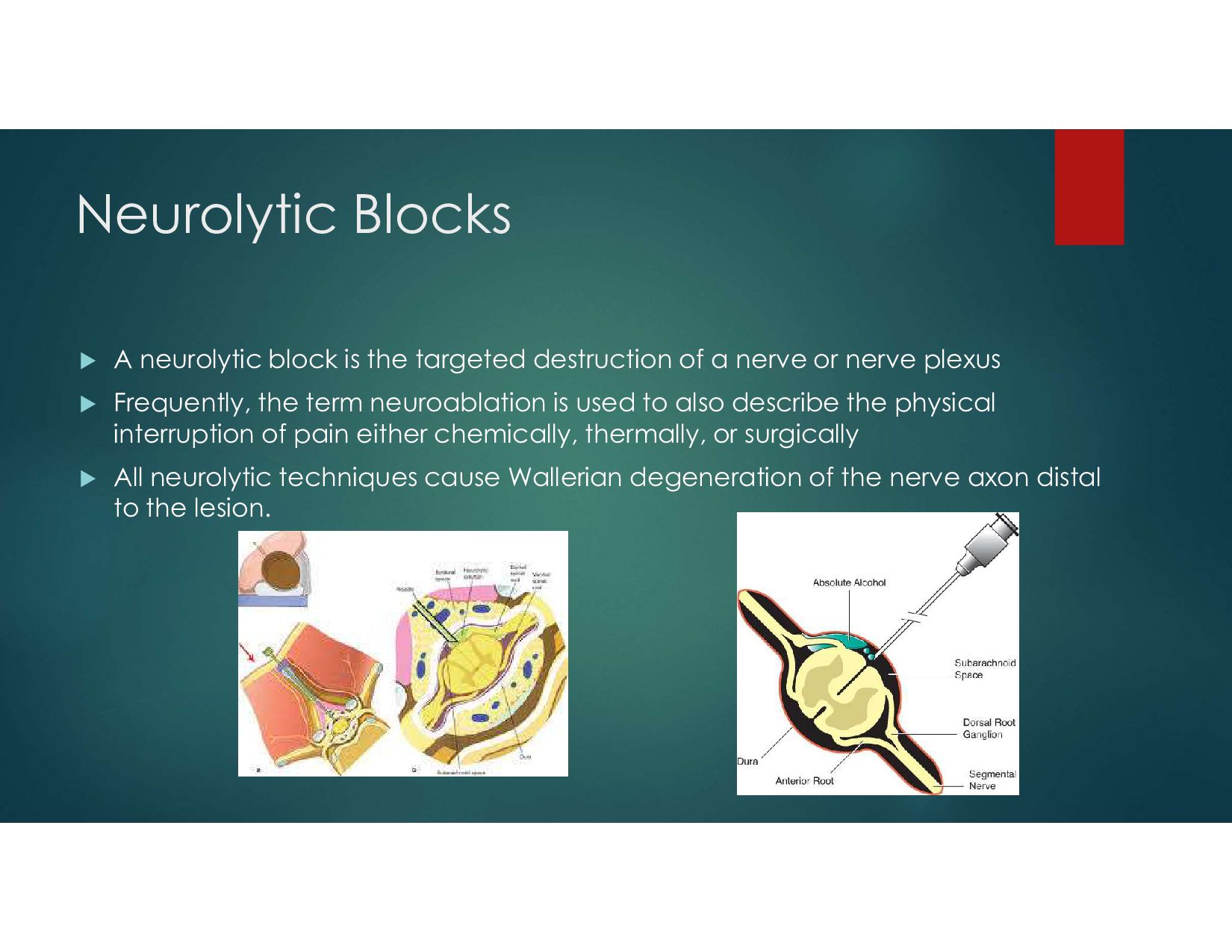
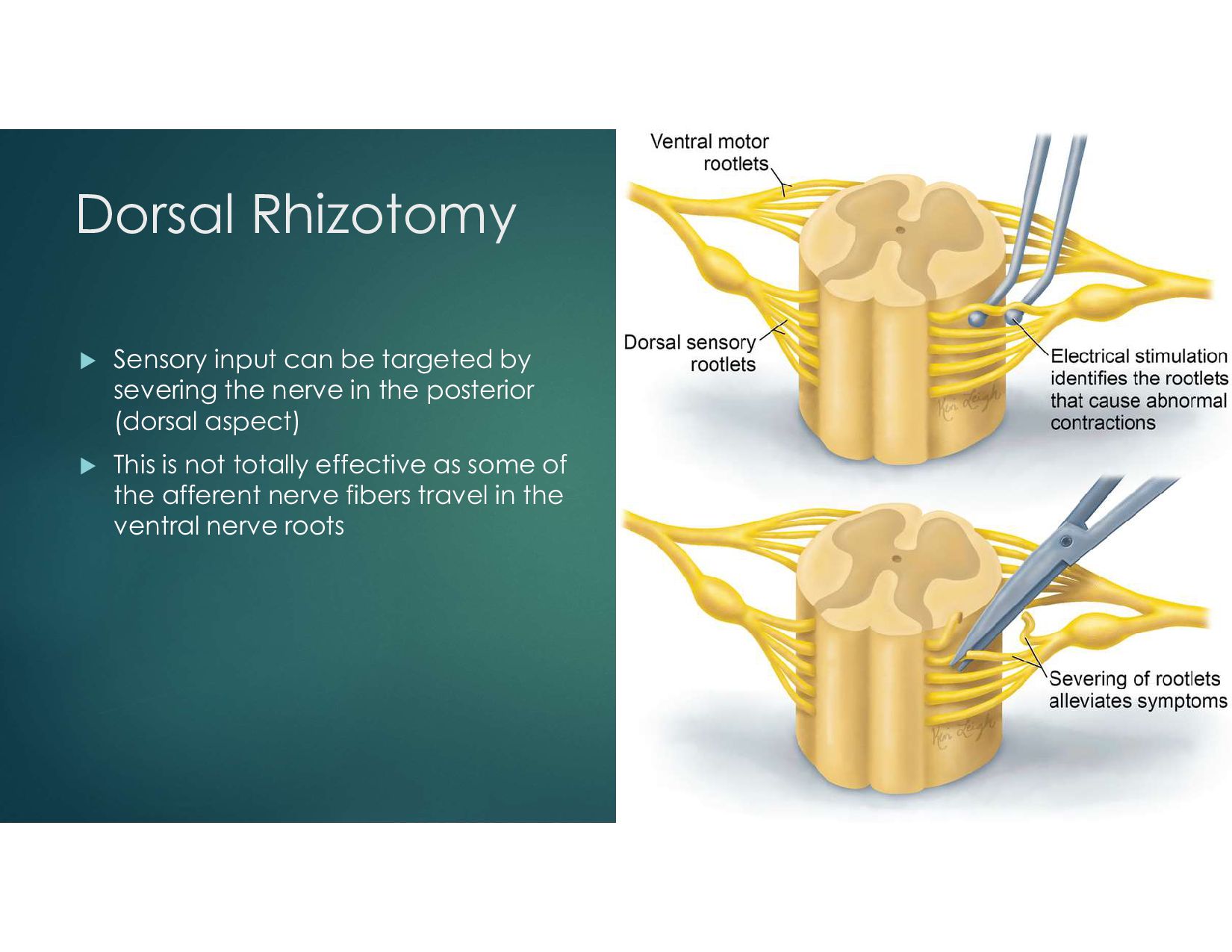
of a nerve or nerve plexus Frequently, the term neuroablation is used to also describe the physical interruption of pain either chemically, thermally, or surgically All neurolytic techniques cause Wallerian degeneration of the nerve axon distal to the lesion.
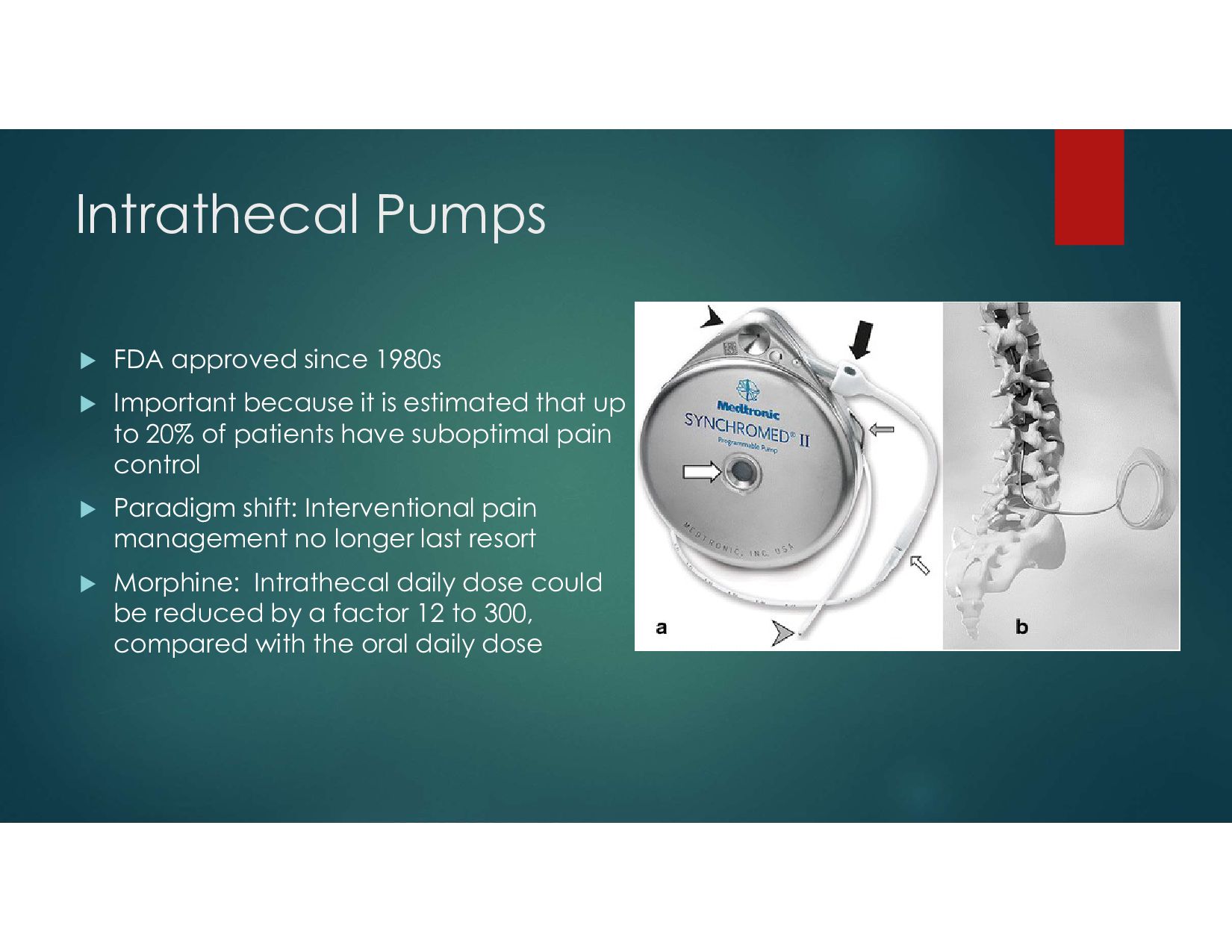
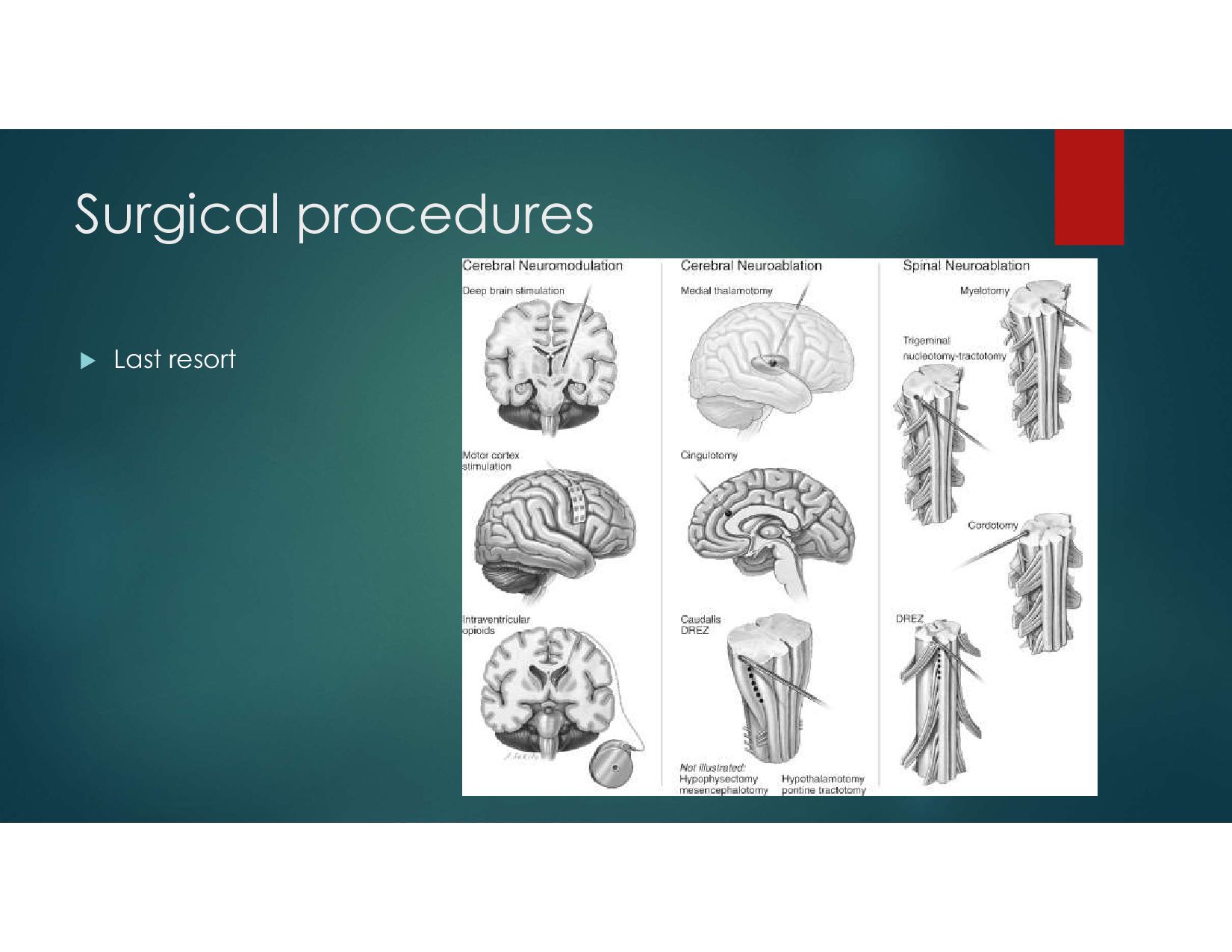
it is estimated that up to 20% of patients have suboptimal pain control Paradigm shift: Interventional pain management no longer last resort Morphine: Intrathecal daily dose could be reduced by a factor 12 to 300, compared with the oral daily dose
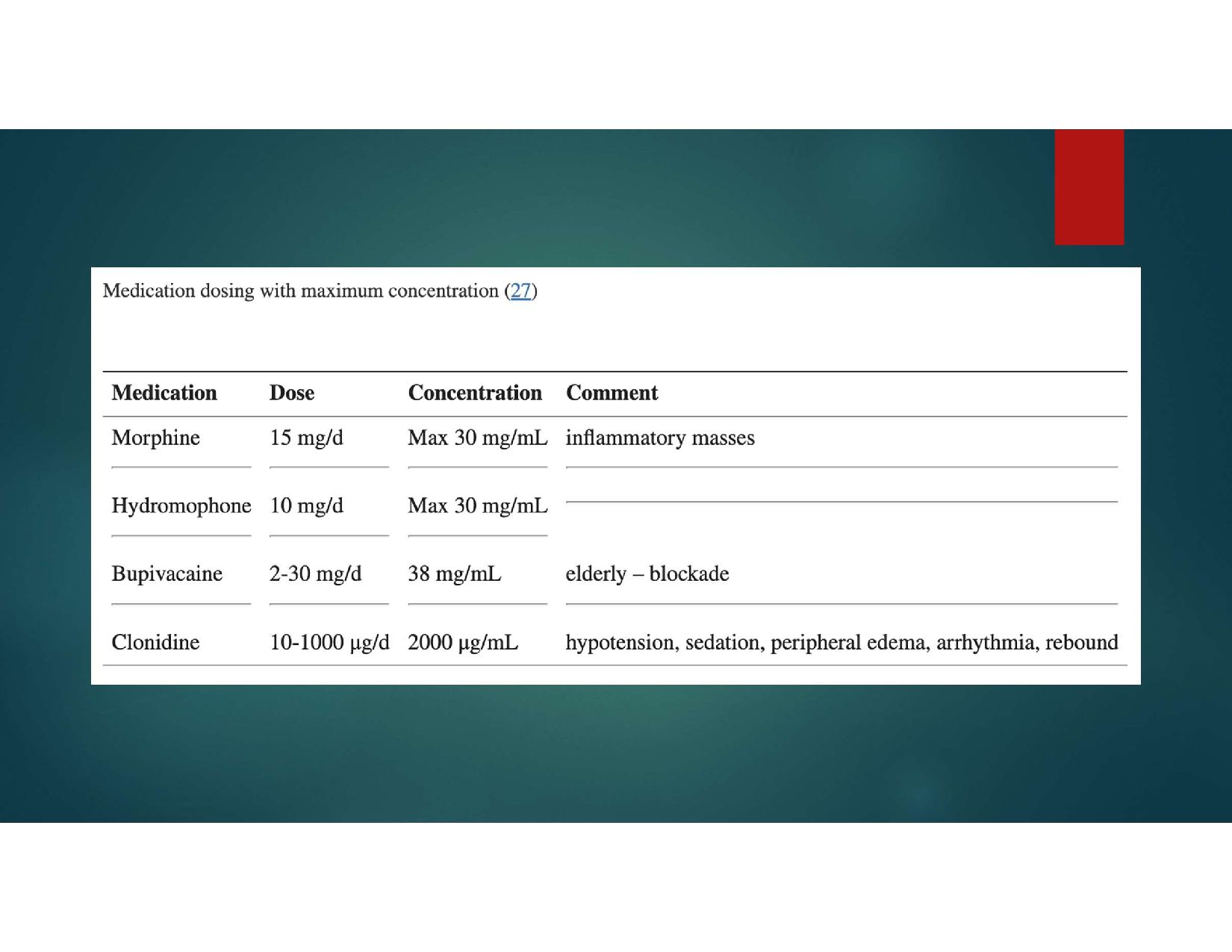
directly to the spinal fluid It consists of a small battery-powered, programmable pump that is implanted under the subcutaneous tissue of the abdomen and connected to a small catheter tunneled to the site of spinal entry Sophisticated drug dose regimens can be instituted Implanted pumps need to be refilled every 1 to 3 months There is no evidence showing whether it is more clinically effective to use bolus or continuous dosing.
with bolus option for breakthrough pain Lower doses of drug generally produce fewer adverse effects sedation, cognitive deficits, fatigue, and constipation Intrathecal drug administration can provide more effective analgesia than systemically administered Early implementation may lead to improved survival (Smith, T.J. et al. 2002. Journal of Clinical Oncology) Minimize divergence of medications
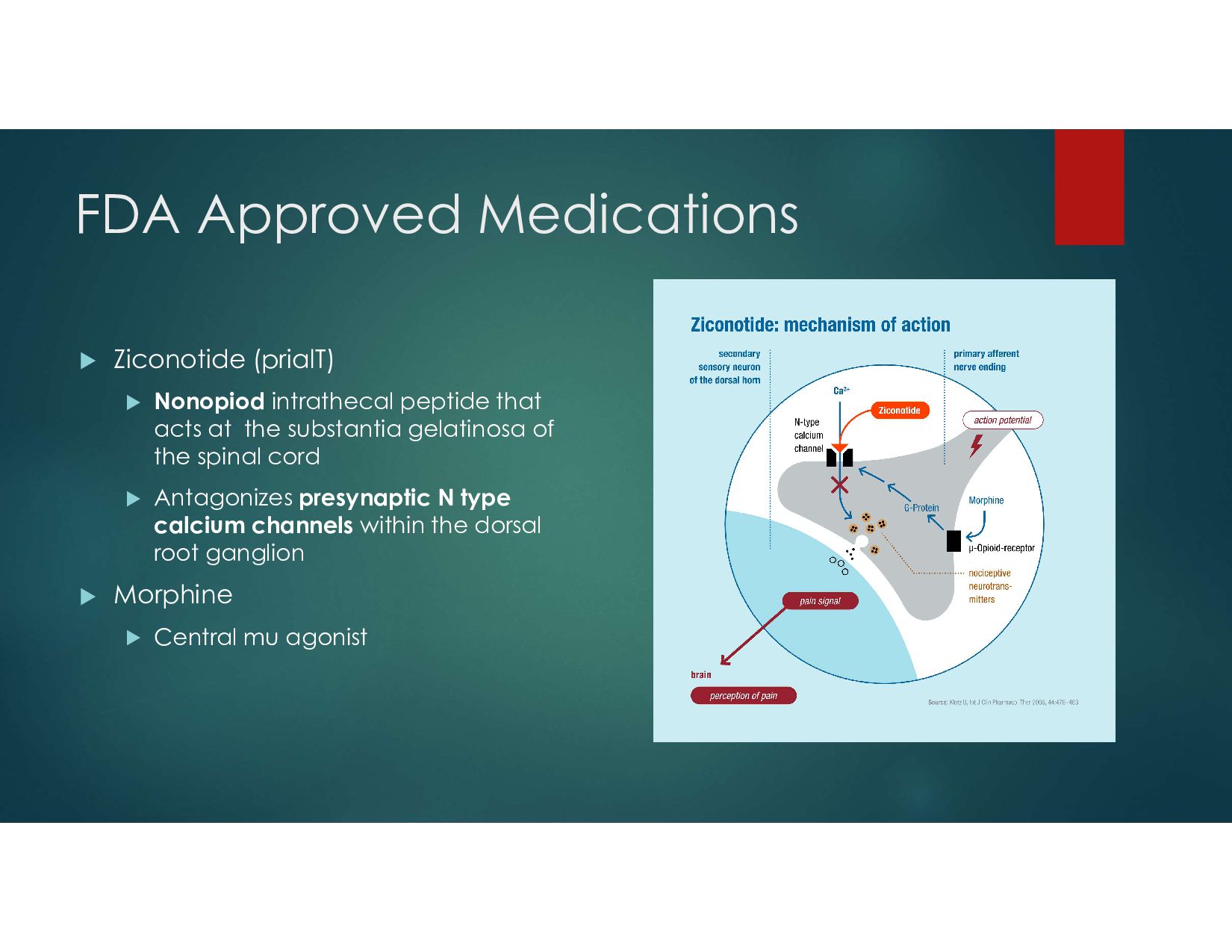
that acts at the substantia gelatinosa of the spinal cord Antagonizes presynaptic N type calcium channels within the dorsal root ganglion Morphine Central mu agonist
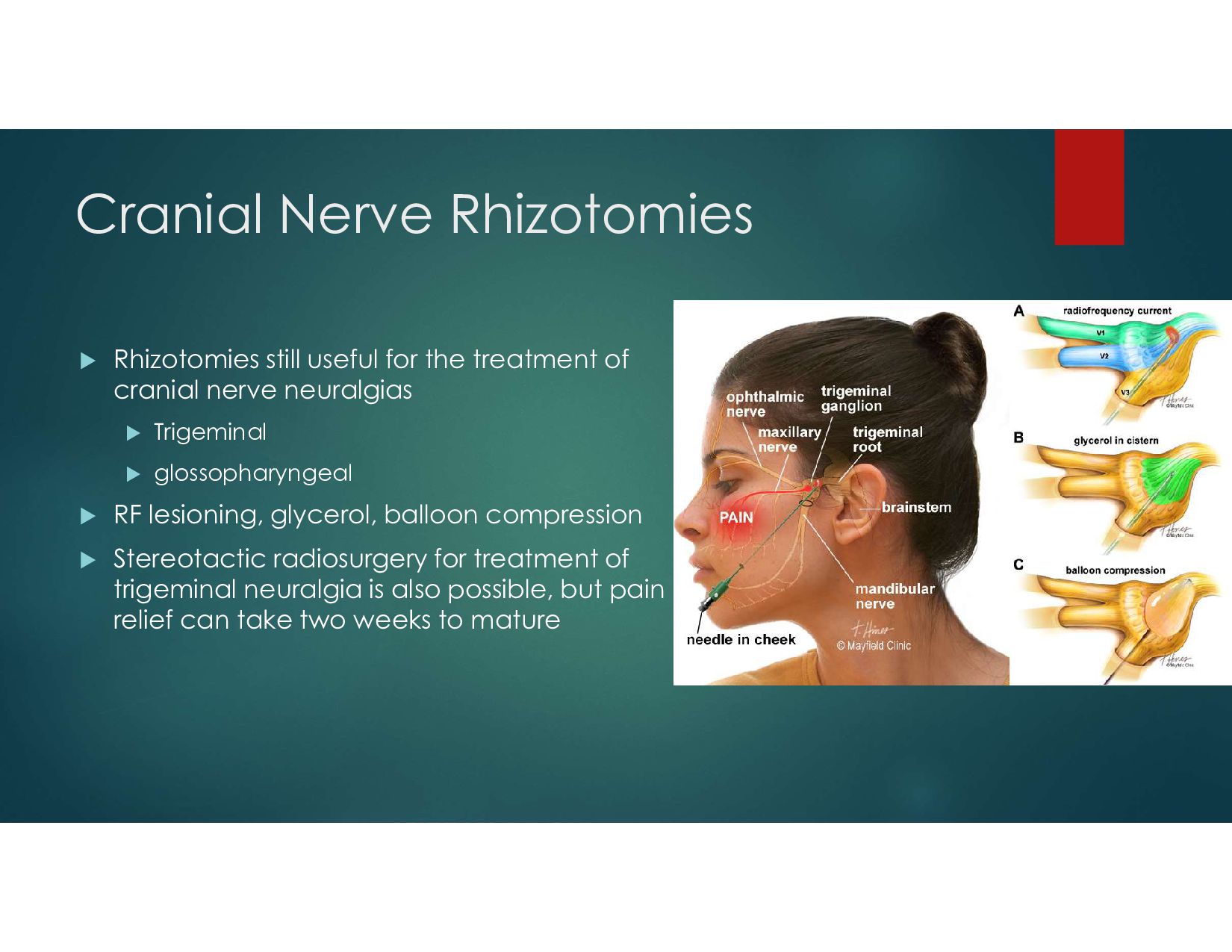
of cranial nerve neuralgias Trigeminal glossopharyngeal RF lesioning, glycerol, balloon compression Stereotactic radiosurgery for treatment of trigeminal neuralgia is also possible, but pain relief can take two weeks to mature
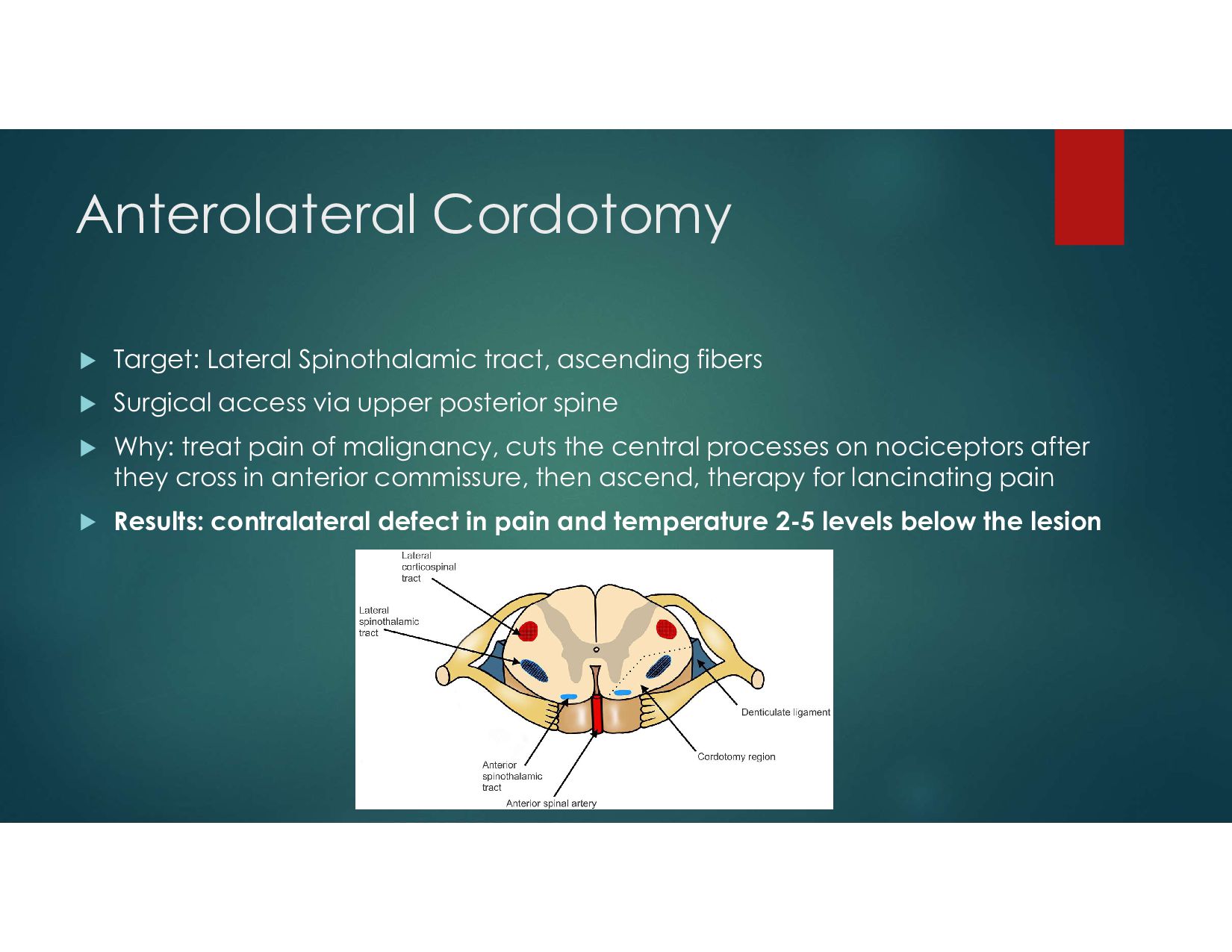
Surgical access via upper posterior spine Why: treat pain of malignancy, cuts the central processes on nociceptors after they cross in anterior commissure, then ascend, therapy for lancinating pain Results: contralateral defect in pain and temperature 2-5 levels below the lesion
lobotomy procedure that was perfected by Freeman and Watts RF lesions of bilateral anterior cingulate gyrus Indicated for intractable pain of malignant origin “Psychosurgery” May be used for OCD
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}