coccygeal vertebrae • About 70 cm long with cervical and lumbar convex, thoracic and sacral concave • In adults cord ends at L1-L2, in infants L3 while the dural sac ends at S2 in adults and S3 in infants
• Utilizes over 20% of total oxygen metabolism • Neurons consume 75-80% of energy produced in the brain • Cerebral vessels respond by mechanisms involving nitric oxide, prostaglandins, vasoactive peptides, potassium channels, and endothelin
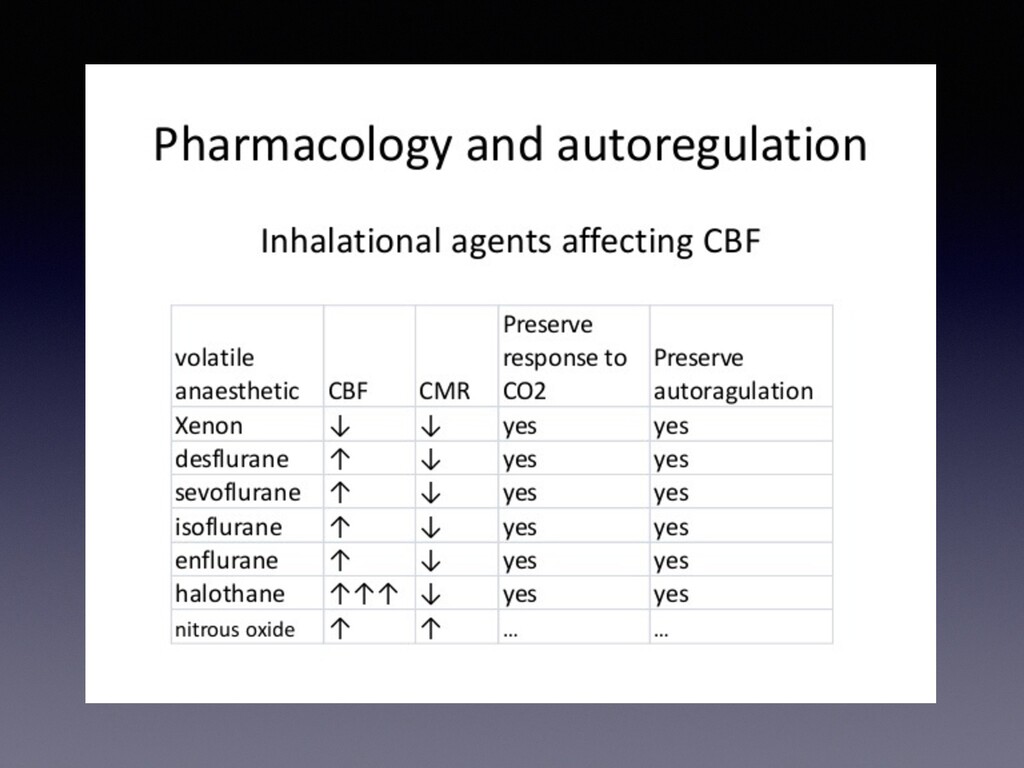
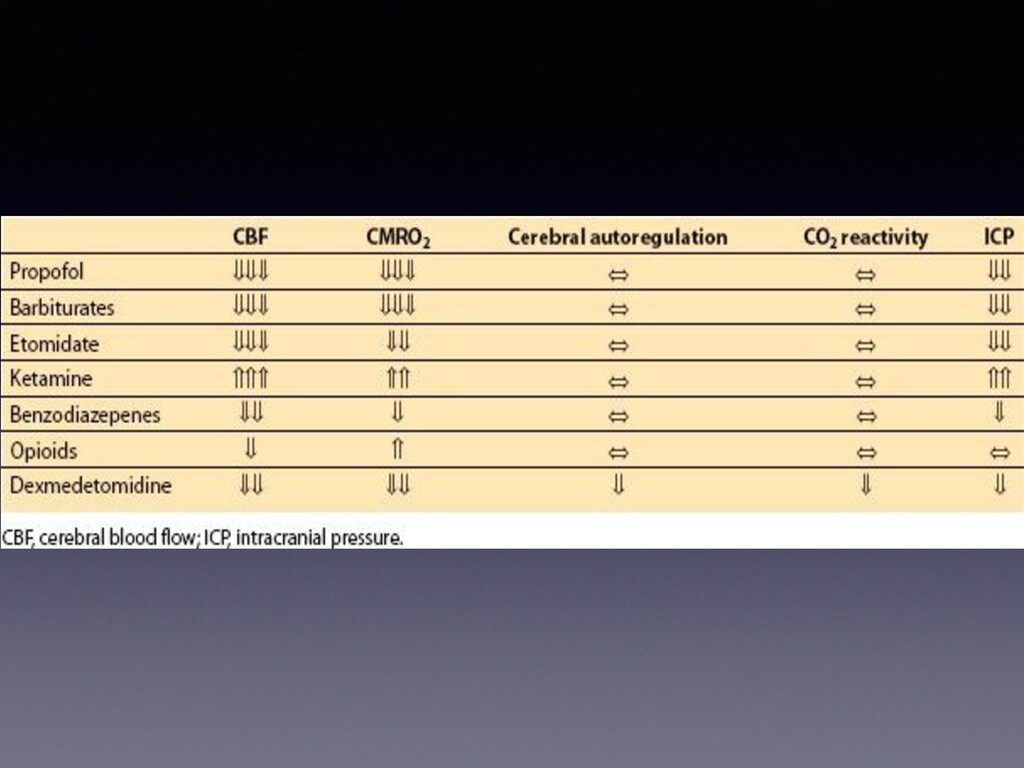
is the effect of the different anesthetic agents on CBF and CMRO2? Inhalation agents, narcotics, propofol, etomidate, ketamine, dexmedetomidine, and benzodiazepines?
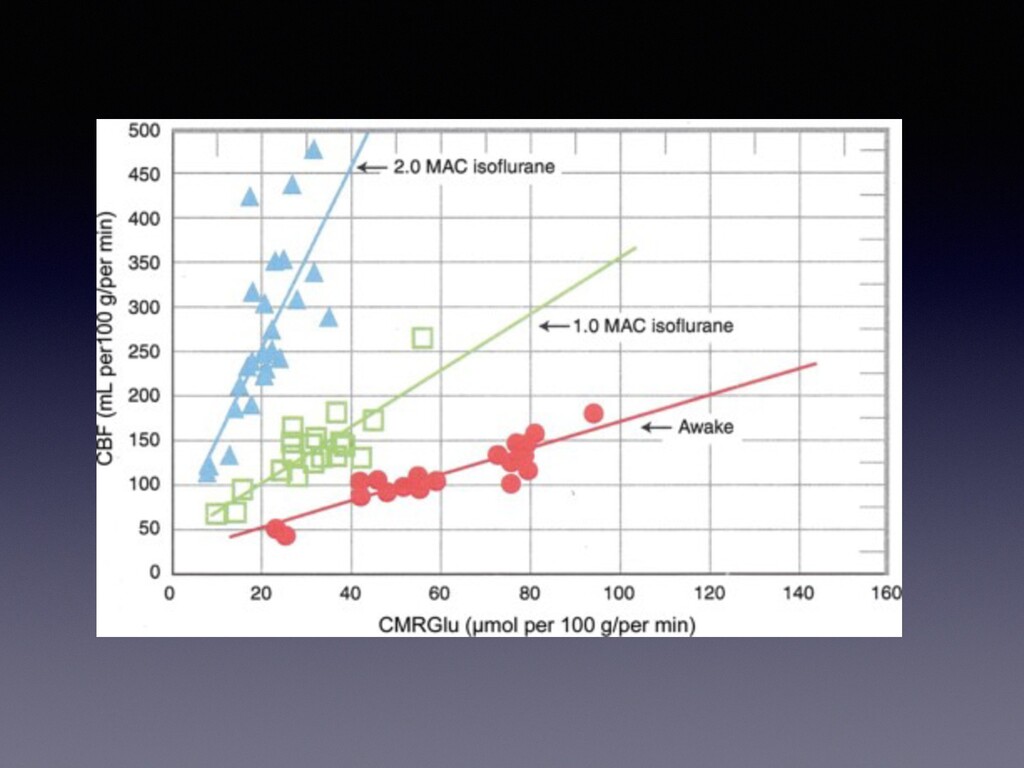
• CBF changes are directly proportional to PaCO2 • Volatile Anesthetics lead to uncoupling of CBF/CMRO2 • IV Anesthetics decrease CBF and decrease CMRO2 • Benzos decrease CMRO2, little effect on CBF • Succinylcholine – controversial but believed to increase CBF which can increase ICP • Opioids have minimal effects on CMRO2 and no effect on CBF unless rapid infusion
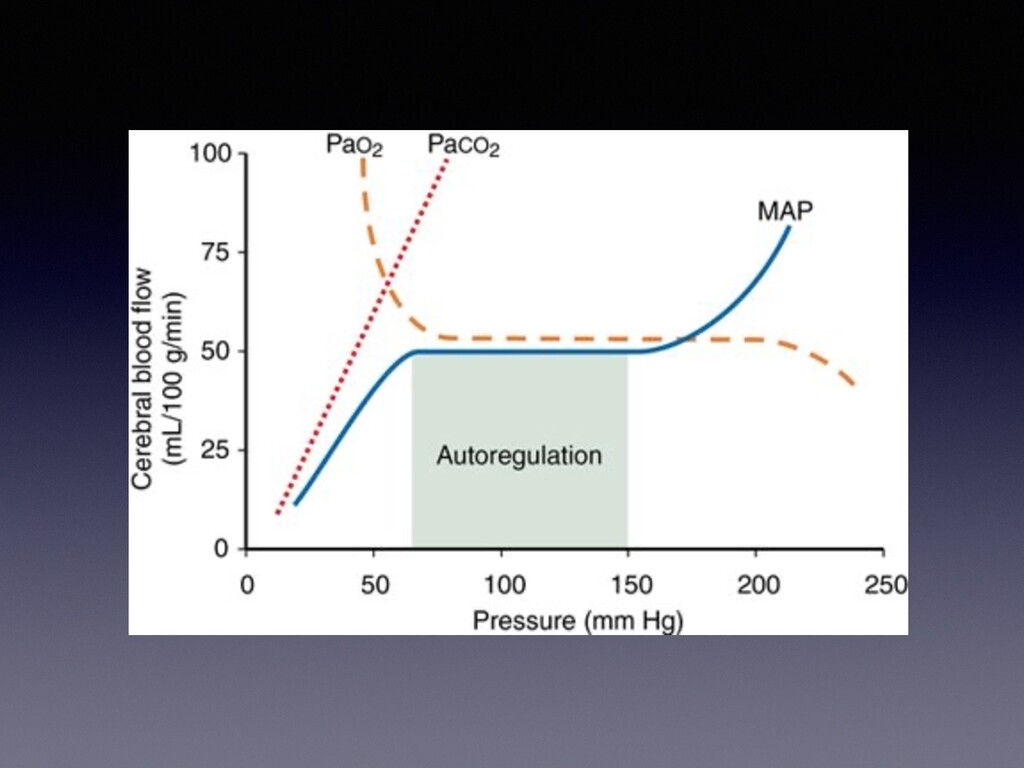
• Sedative hypnotic agents and mild hypothermia decrease flow and metabolism • What are some factors that directly effect CBF, not related to metabolism?
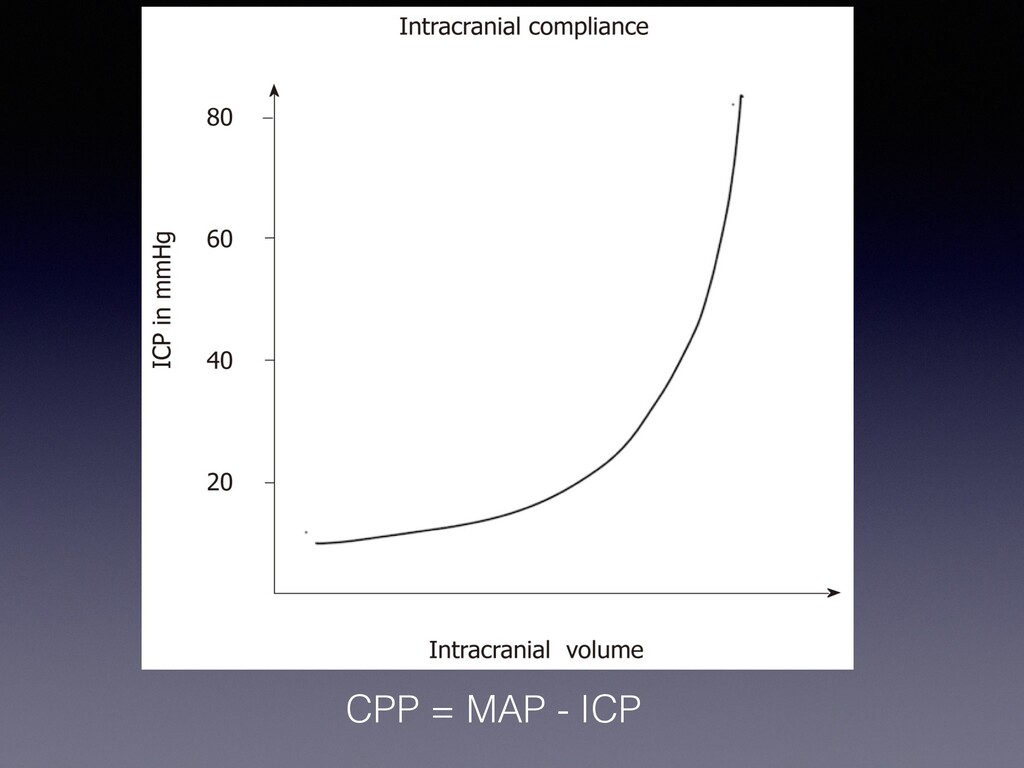
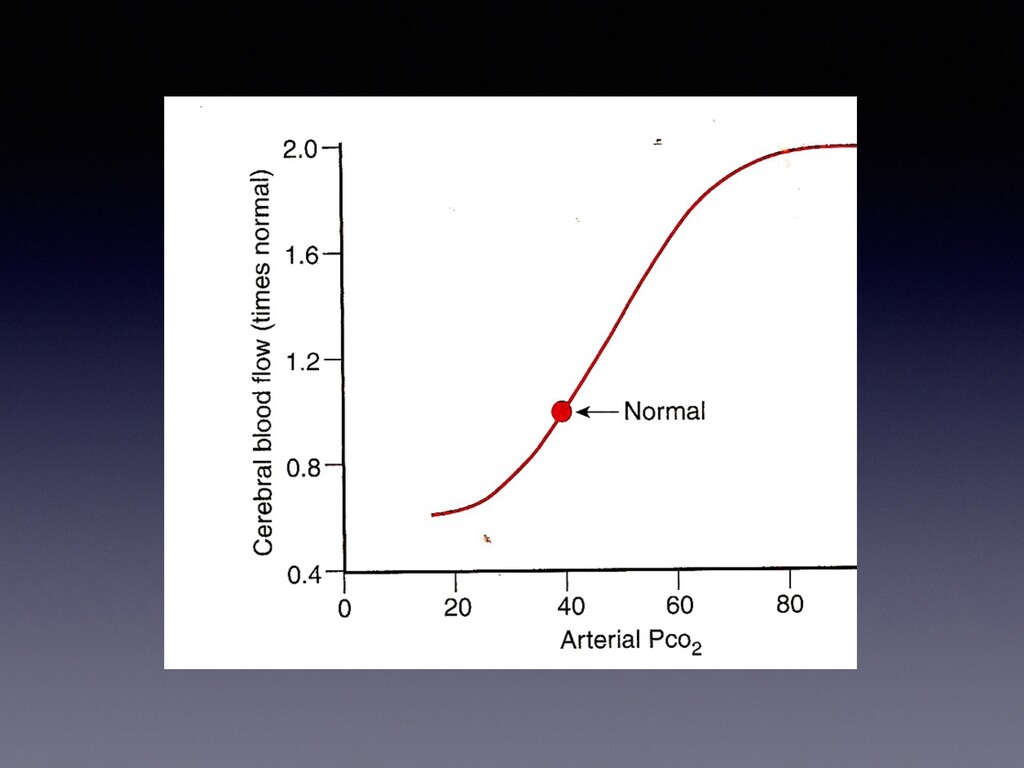
Hg change in PCO2 causes a 3% change in blood flow in a linear relationship • As CBF decreases so does CBV and is why hyperventilation is used to help control ICP. • Can you overdo this effect and does it dissipate over time as the CSF pH normalizes?
of the bed, oxygenation and ventilation to maintain PaO2 >100, PaCO2 30-35 • CSF drainage • Mannitol boluses at 0.25-1g/kg • 3% saline as similar effects as mannitol • Hyperventilation – but CBF drops 3-4% for every 1 mmHg decrease in PCO2
injury • Identify return or improvement of function • Although these modalities are sensitive and specific in spine surgery, there is a report that states, even with intraop response to decreased signals, it may not reduce rate of new or worsening perioperative neurological deficit(2010 Spine Journal)
Willis. It measures flow velocity which directly related to flow only if the diameter of the vessels is constant. Can detect emboli and debris, useful in CEA, bypass procedures, non-neurologic surgeries in TBI patients, detection of vasospasm in the Neuro ICU
glucose and O2 to support aerobic metabolism, generation of ATP and maintenance of cellular function • The goal is to lower the metabolic rate, less depletion of ATP reserves during ischemia • What is the newer research focused on?
transection at the T2 level 3 years ago is scheduled for suprapubic catheter placement. During surgery, he is noted to have an acute rise in blood pressure, to 204/115 mm Hg. Which of the following signs or symptoms is LEAST likely to coincide with this rise in blood pressure? • Headache • Nasal congestion • Skin flushing in lower extremities • Skin flushing in upper extremities
whether a patient is in a persistent vegetative state or a coma? • Ability to follow commands • Ability to communicate • Ability to make purposeful movements • Ability to open eyes
procedure and co-morbid conditions, invasive monitors pre or post induction • Muscle relaxant choice-is there a place for use of succinylcholine? • Consider patient's airway/ awake cases/ prone/ 180 degree head position/ pre or post op radiologic studies/monitoring
loss of airway (hypoxia, hypocarbia, and aspiration risk) is a greater risk than the increase in ICP associated with succinylcholine. • Use of a defasciculating dose of non-depolarizing muscle relaxant should be administered prior to using succinylcholine • Use of non-depolarizing muscle relaxant is generally recommended in non-emergent cases, making sure that the patient is fully relaxed and adequate hemodynamic conditions have been achieved prior to intubation
Colloid has no proven benefit • Mannitol effective for treatment of intracranial HTN • 3% hypertonic saline beneficial for treatment of severe intracranial hypertension (additionally, anti- inflammatory action) • Hyperglycemia worsens brain ischemia, control of hyperglycemia is important.
21% seems to be a number that most agree upon. • With ongoing intraop blood loss, it may be prudent to keep the HCT higher than 21% to maintain proper oxygen delivery to the brain.
is key with an awake patient who can easily be evaluated neurologically • Judicious use of narcotics with the most important goal the ability to evaluate the patient neurologically. Common practice is to use IV tylenol as the principle analgesic • Smooth emergence hemodynamically is also important with maintenance of normal BP. In some cases there are specific BP ranges which may be beneficial related to the surgical procedure.
patients with difficult airways, as in cervical spine cases with decreased ROM of the neck, and prone patients with airway edema, or the transphenoidal patient with acromegaly with the nose packed and blood in the airway • Deep extubation is the same as smooth awake extubation with a cooperative patient and can be accomplished with +/- lidocaine, small doses of precedex and minimizing long acting narcotics
secreting tumors • DI- intraop or more commonly post op may be treated with DDAVP if unresponsive to fluid restriction • Spinal drain used for injection of air or saline incases of supracellar extension or for treatment of patients with CSF leak
presenting symptoms • preoperative embolization- decreases intraoperative bleeding • Regional hyperemia in surrounding vessels post resection can cause vasogenic edema (lack of auto regulation capabilities) • Bleeding-always a risk • Close BP control and smooth extubation are important
across the aneurysmal sac, sudden increase in MAP or decrease in ICP can cause rupture • Vasospasm: immediate and 5-14 days after rupture • Blood pressure control: avoid spikes (at risk times: laryngoscopy, headapins, incision, and dissection around aneurysm) • Bleeding: arterial bleeding can be devastating with intraop rupture. • Clipping: conditions for clipping may necessitate use of adenosine • Smooth emergence and extubation important • +/- Post operative angiogram to evaluate flow and check for vasospasm
deployed across the aneurysm neck. Blood in the bypassed aneurysm then clots • Coiling- detachable coils fed in to the aneurysm eventually creating coil/ thrombus complex. Difficult accessibility or wide based aneurysms may not be coilable • Sedation vs general in code stroke patients: current belief is local is better than general as long as patient is cooperative enough to withstand the procedure.
neurologic assessment by stroke team and CT within 25min, interpretation within 45 min, fibrinolytic tx/thrombectomy within 1 hour of arrival/3hours after onset of symptoms, tpa for up to 4.5hours.
secondary rebleeding, cerebral ischemia, and hydrocephalus • Rebleeding often occurs within 24-48 hrs • Vasospasm often concern and large cause of post SAH morbidity and mortality
for tumor resection 5 days ago. Was taken back to OR for drainage of scalp abscess. Pt has been in recovery room for 2 hours and is still somnilent and not following commands. He received 250mcg of Fentanyl intra-op and anesthesia was maintained with nitrous oxide-isoflurane. Currently he withdraws from pain and his pupils are 3mm equal and reactive. TOF is 4/4. Patient was neuro intact prior to the procedure. What's the next best step?
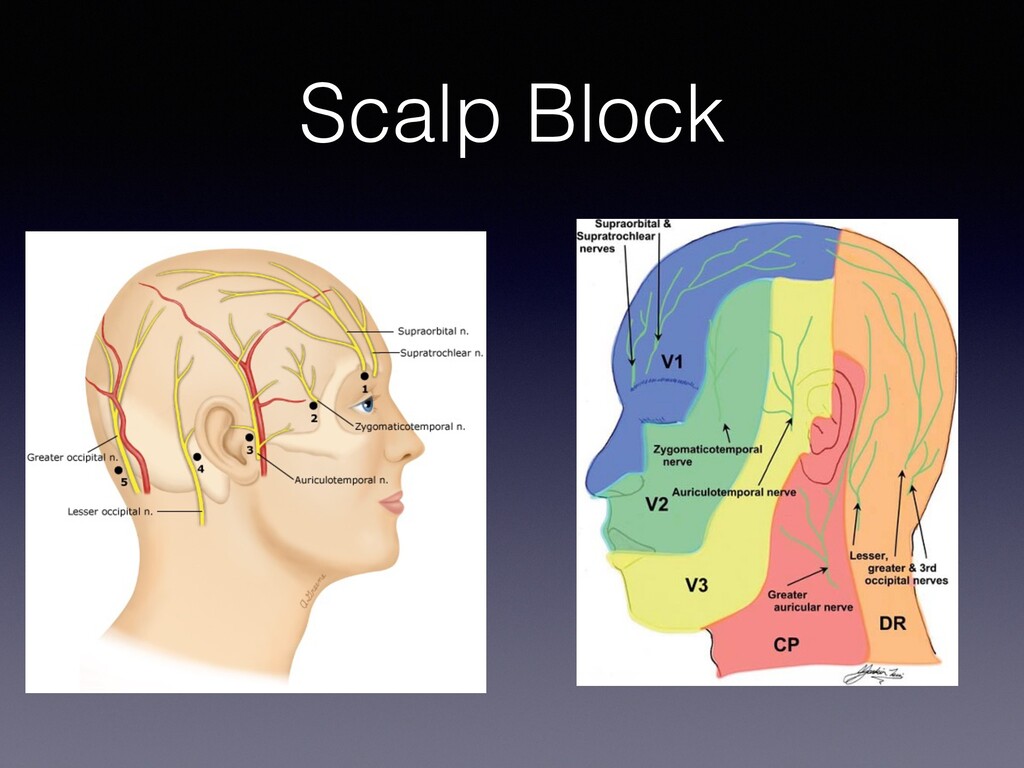
: tumors in the eloquent areas of the brain (primary motor and somatosensory cortex) • monitoring/ECOG-intraoperative EEG • Toleration of procedure: patient selection important • asleep/awake/asleep technique replaced by awake/sedated with precedex and low dose remifentanil • Intraoperative seizure: treated with iced saline and judicious doses of versed or propofol if needed(maintain airway and spontaneous) • Scalp block:nusing .25% bupivicaine • Neurophysiological monitoring to assess motor or speech
or other conditions such as essential tremor. • Performed under deep sedation with periods of wakefulness for testing the placement • Electrodes are placed in the sub-thalamic nucleus(STN), during part I and 1-2 weeks later the generator is placed during part 2 • STN is used for Parkinsons, other areas are used for other diseases
with open resection • A laser lead is placed in the center of the tumor utilizing MRI and CT guidance and the ablation is performed with direct MRI guidance under general anesthesia • This methodology may not be utilized for larger tumors outside the functional radius of the laser heated area • This procedure may extend the life of patients with inoperable tumors
• Other injuries should be considered when plan anesthetic(hypotension and anemia) • ICP-high ICP frequently found in TBI patients • Hypothermia- only true effective method for brain protection • Barbiturate coma utilized for severe ICP if inoperable or in combination with hemicraniectomy
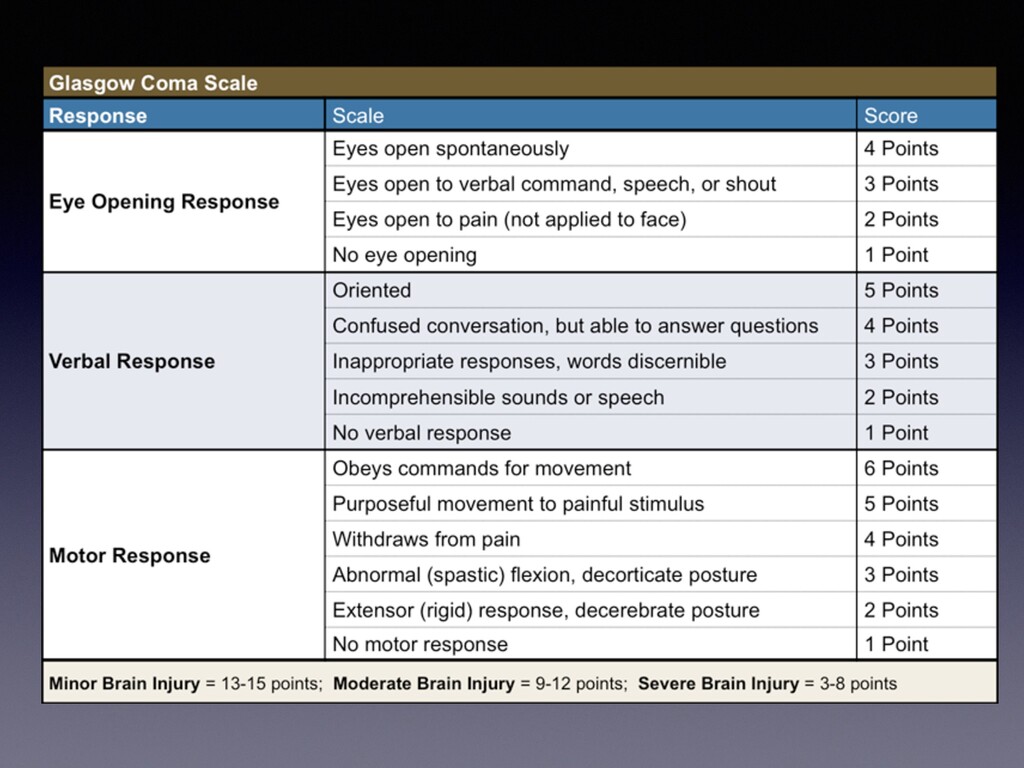
after a roll over MVA. His BP is 90/60, HR 125 and O2 saturation 97% on 2L NC. He opens his eyes to painful stimulation, is speaking incomprehensible words and withdraws both upper and lower extremities to pain only. What is his GCS?
from her husband. In the ER trauma bay, the patient is giving inappropriate responses to questions being asked. Her eyes open upon verbal command and shows purposeful movement in all extremities to painful stimuli.
for induction most acceptable? • A patient with myotonic dystrophy • A patient with muscular dystrophy • A patient with myasthenia gravis • A patient with multiple sclerosis • A patient with T6 spinal cord transection 2 months ago
o Stroke o Spinal cord injury o Intracranial lesions leading to upper motor neuron injury - Burns (24 hours up to 1-2 years after burn injury) - Prolonged immobility (greater than 24 hours) - Prolonged exposure to neuromuscular blockers - Myopathies o Duchenne muscular dystrophy - Denervating Disorders o Multiple sclerosis o Guillain-Barré syndrome o Amyotrophic lateral sclerosis
post synaptic membrane of NMJ • Resistant to succinylcholine • Sensitive to nondepolarizing muscle relaxants • Treatment: cholinesterase inhibitors (pyridostigmine), corticosteroids, immunosuppressants, IVIG and plasmapheresis
presynaptic voltage gated calcium ion channels resulting in decreased release of ACh • Often associated with small cell lung cancer • Sensitive to effects of BOTH depolarizing and nondepolarizing muscle relaxants • Treatment: 3.4-diaminopyridine
an autoimmune response in association with an infectious process • Most common after respiratory or GI illness (campylobacter, Haemophilus, Mycoplasma, EBV) • Succinylcholine should be avoided because of danger of hyperkalemia • Autonomic dysfunction is common involving sympathetic and parasympathic NS • Cardiovascular manifestations can include hypertension, hypotension, brady/tachyarrhythmias
damage to the central nervous system • Clinical criteria for diagnosis (age of onset is between 10- 50 years) signs and symptoms of CNS white matter disease, two or more attacks separated by a month or more and involvement of two or more anatomic areas • Do not use succinylcholine. NDNMB's are safe to use but may have varying sensitivity due to baseline limb weakness • Treatments include corticosteroids, Interferon-beta, glatiramer acetate, azathioprine, and low-dose mexthotrexate.
to atrophy and brain cells to die leading to worsened cognitive dysfunction and dementia • Involves amyloid-B protein; deposition of amyloid plaques, neurofibrillary tangles, and neuronal apoptosis • Treatment includes acetylcholineasterase inhibitors (donepezil, rivastigmine, galantamine) and NMDA inhibitor (Memantine)
dopaminergic cells in basal ganglia • Levodopa used in combination with drugs such as carbidopa (peripheral decarboxylase inhibitor) and entacapone (catechol-o- methyltransferase inhibitor) that prevent adverse peripheral effects of dopamine
• Can experience delayed emergence and increased likelihood of resp complications • Decreased plasma cholinesterase activity may prolong response to succinylcholine
disease of motor neurons, upper and lower • Riluzole a glutamate release inhibitor is only drug approved for ALS • May be sensitive to nondepolarizing muscle relaxants • Can have hyperkalemic response with use of succinylcholine. Spinal anesthesia is usually avoided
Pathology involves insufficient or abnormal proteins that form the cytoskeleton of the muscle membrane • Duchenne muscular dystrophy • Becker muscular dystrophy • Emery-Dreifuss muscular dystrophy
infancy, developmental delay, feeding difficulties and respiratory dysfunction • May be susceptible to malignant hyperthermia • Succinylcholine should be avoided and may be sensitive to NDNMB's • Myotonic dystrophy – dysfunction of ion channels in muscle membrane
intermittent weakness • Sodium ion channel mutation that causes prolonged muscle membrane depolarization and flaccid paralysis • Attacks can be provoked by potassium loading, rest after exercise, stressful situations and cold temperatures • Treatment: glucose, insulin, epinephrine, calcium
or potassium ion-channels. cause weakness by partial depolarization of the muscle cells, without generating action potentials. • Triggers: hypothermia, rest after exercise, metabolic alkalosis, carbohydrate loading, meals with high Na content • intraoperatively, monitor potassium levels and avoid glucose solutions or solutions with a high sodium content.
begin electroconvulsive therapy (ECT). Which of the following is the LEAST likely response to ECT? • Bradycardia • Short term memory loss • Decreased cerebral blood flow • Tachycardia
medication, bipolar disorder, schizophrenia • Generalized epileptic seizure induced by electrical stimulation of the brain • Duration of the seizure is important for the overall therapeutic effect • Contraindications
patient who will undergo electroconvulsive therapy (ECT). Which of the following intravenous drugs would be the LEAST appropriate for this patient, given the type of procedure being performed? • Etomidate • Glycopyrrolate • Lidocaine • Remifentanil
Stoelting, Michael K. Cahalan, M. Christine Stock, Rafael Ortega, Sam R. Sharar, and Natalie F. Holt. Clinical Anesthesia. Wolters Kluwer. 8th ed. 2017. • Butterworth, John F., David C. Mackey, and John D. Wasnick. Morgan & Mikhail's Clinical Anesthesiology. McGraw-Hill. 6th ed. 2018. • Miller, Ronald D. and Manuel C. Pardo, Jr. Basics of Anesthesia. Elsevier. 6th ed. 2011. • OpenAnesthesia.org. IARS. 2021. • Trentman, Terrence L., Brantley D. Gaitan, Bhargavi Gali, Rebecca L. Johnson, Jeffrey T. Mueller, Steven H. Rose, and Toby N. Weingarten. Faust's Anesthesiology Review. Elsevier. 5th Ed. 2020.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}