US • Currently approximately 45,000 CRNA in US • Relatively advanced age of average Anesthesiologist higher than mean physicians. 56% over 55 years old (Merritt-Hawkins) • Tend to retire younger. • Tend to cluster in metropolitan areas 91.6% of Anesthesiologists • Medicare limitations on new Anesthesia Residency spots. (1997 Balanced Budget Act)
in last 2 decades • Increased use of anesthesia services in out-of-OR locations. Cath labs, radiology suites, etc. • Drags on Demand: • Impending shortage of surgeons and surgical subspecialists, esp. regionally
of 12,500 Anesthesiologists in nect 20 years. • Need 25% growth to cover attrition and new needs • Shortage especially worse in rural,southern, and south central regions of the US
a UNIT basis • Initial rate based on case complexity – BASE UNITS • Base units set by CMS, they are reviewed and updated annually • Base Units are added to Time Units • Every 15 minutes = 1 unit The addition of the Base units and time units determines the units billed for that case.
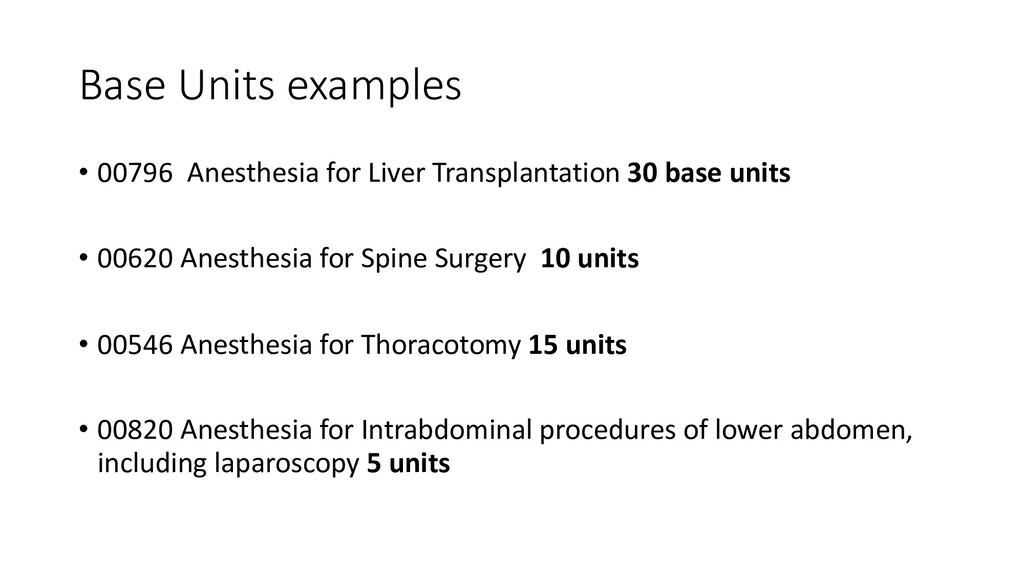
base units • 00620 Anesthesia for Spine Surgery 10 units • 00546 Anesthesia for Thoracotomy 15 units • 00820 Anesthesia for Intrabdominal procedures of lower abdomen, including laparoscopy 5 units
case 5 base units + 4 time units = 9 units Anesthesia for Thoractomy – 2.5 hours 15 based units + 10 time units = 25 9 units per hour vs. 10 units per hour Multiply units by unit rate to get payment per case
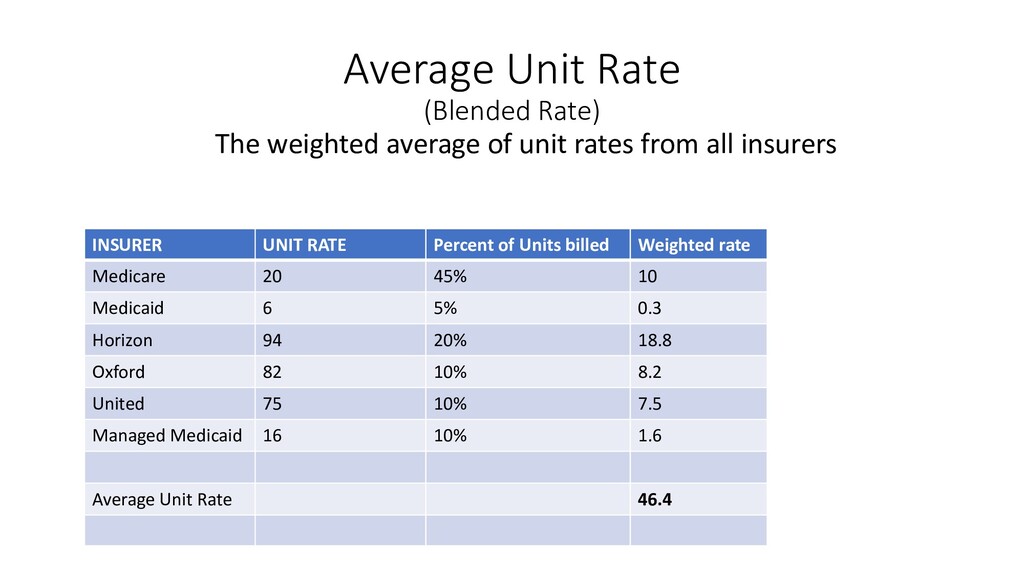
CMS administrators • Medicaid rates set by formula looking at total covered lives • Private insurance rates set by negotiation for in-network rates • Out-of-network rates set by provider, but not necessarily accepted by insurance companies
$15-$35/unit Private Insurance $50 - $110/unit Out-of-network billed to private insurance >$100/unit • Same 9 unit Diagnostic Lap. could range in value from $42 - $900
a specific institution • Usually set by local demographics and hospital referral/transfer patterns However • Work with institution to create new programs • Expand services to ASC or other Hospitals with better mix • Negotiate better rates!
a set rate for a proscribed service Common in Labor Epidural billing, perioperative nerve blocks, and other perioperative procedure eg. Aline, CVP • Bundled Rate – Insurer pays one global rate to hospital for a service, including the professional fees. The physicians negotiate with the hospital for their share of the bundle.
• Typically salaried position with/without overtime and call pay • Considered most stable practice model • Opportunities for research, teaching, and innovation • Easier foray into hospital administration • Built in HR advantages • No ownership, only economic value is in salary and benefits • Typically lower salary than non-academic salary
Contract with hospitals and ASCs for services • Only as stable as relationship to hospital/health system • Partnership vs. Salary • Local Governance Board of directors
all partnerships are created equally • Voting membership? • Full profit sharing? • Equity ownership? • Do you have ownership interest in all ventures? • Buyout? • Everything must be in writing!
Contract with hospitals and ASCs for services • Ownership may not be physician – Private equity • None or little input on governance • Distant ownership • NO real partnership - Salaried position, some local profit sharing • More stable than smaller groups • Large economies of scale
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}