Specifically address difficult airway management • Developed by international task force of anesthesiologists • Provides consideration for the development of a difficult airway management strategy including awake airway management • Updates equipment for standard and advanced difficult airway management • Recommends supplemental oxygenation before and throughout difficult airway management, including intubation and extubation • Offers noninvasive and invasive alternatives for difficult airway management • Emphasizes awareness of passage of time and limiting number of attempts • Recommendations for extubation of difficult airway
person(s) responsible for airway management to identify patient, medical, surgical, environmental and anesthetic factors that may indicate potential for a difficult airway • Conduct airway physical exam • Facial features - mouth opening, ability to prognath, head and neck mobility, prominent upper incisors, presence of a beard, upper lip bite test • Anatomic measurements and landmarks - mallampti scores, thyromental distance, sternomental distance, inter incisor distance, neck circumference
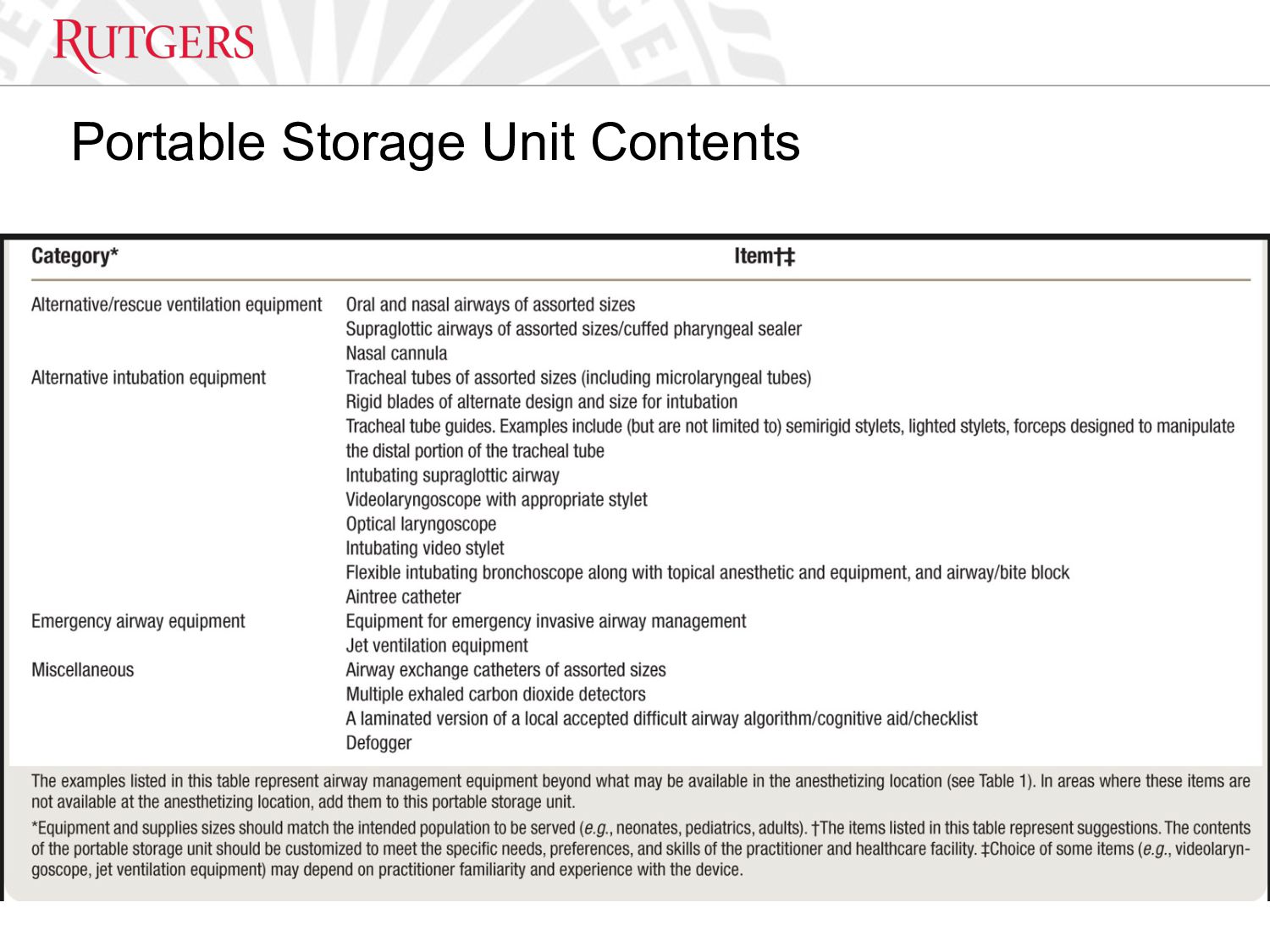
is in the room • Ensure portable storage unit that contains specialized equipment for difficult airway management is available • If difficult airway is known or suspected - • Ensure skilled individual is present or immediately available to assist when feasible • Inform the patient of the special risks and procedures pertaining to management of the difficult airway • Properly position the patient, administer supplemental oxygen before initiating management and continue to deliver supplemental oxygen whenever feasible throughout the process including extubation • ASA standard monitoring performed immediately before, during and after airway management of all patients
bags at start of each shift • Always check McGrath • No medications in airway bag • Dispose of all medications appropriately at time of use • No McGrath available in pediatric bag! • Replace items in pediatric bag after use. • Be mindful of stock when handing off bag
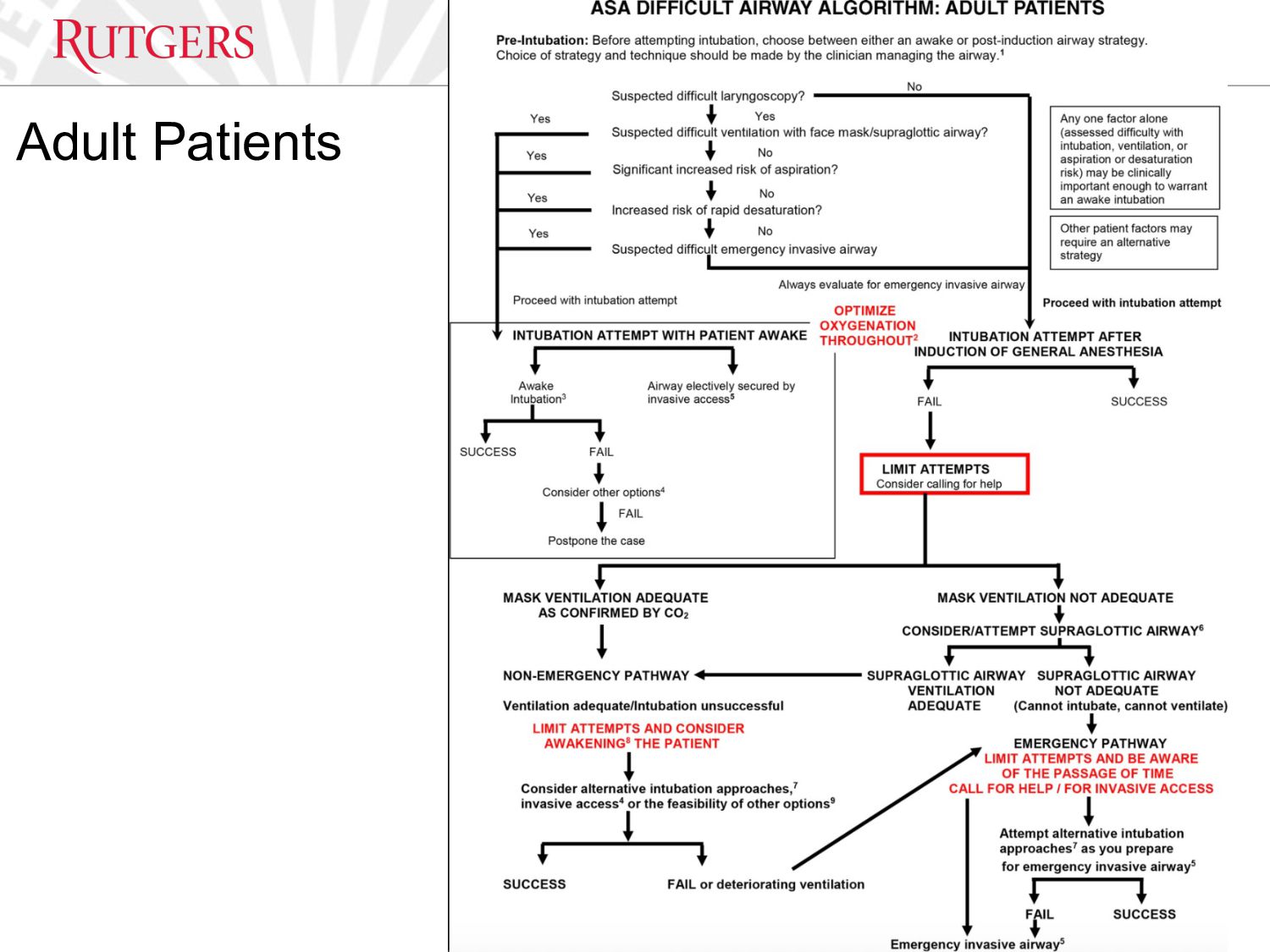
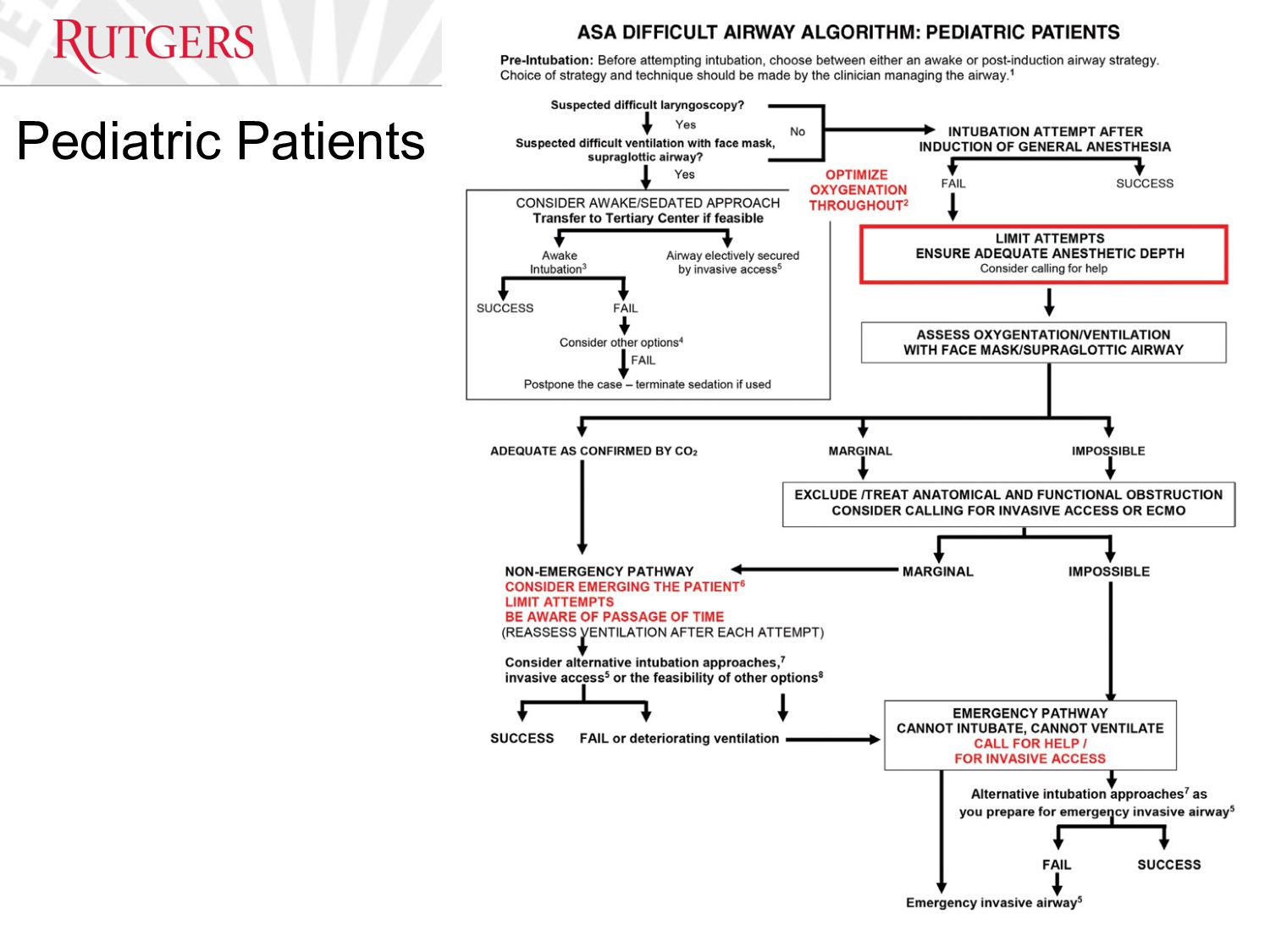
strategy for management of anticipated difficult airway and when appropriate, perform awake intubation • Before attempting intubation of the anticipated difficult airway, determine the benefit a noninvasive versus invasive approach to airway management • Be aware of the passage of time, number of attempts and oxygen saturation • Limit the number of attempts at tracheal intubation or supraglottic airway placement to avoid potential injury and complications • Ensure that an invasive airway is performed by an individual trained in invasive airway techniques, whenever possible • If the selected approach fails or is not feasible, identify an alternative invasive intervention
for help • Optimize oxygenation • Refer to an algorithm or cognitive aid • Determine benefit of waking/restoring spontaneous breathing • Determine benefit of a noninvasive versus invasive approach to airway management
or end-tidal carbon dioxide monitoring • If uncertain about location of tracheal tube, determine whether to remove it and attempt ventilation or use additional techniques to confirm positioning of the tracheal tube
for extubation and subsequent airway management • Assess patient readiness for extubation • Ensure that a skilled individual is present to assist with extubation when feasible • Select appropriate time and location for extubation when possible • Before attempting extubation, evaluate the risks and benefits of elective surgical tracheostomy • Evaluate risks and benefit of awake extubation versus extubation before return to consciousness • Use supplemental oxygen throughout extubation process
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}