frequent sinus pauses • Acquired AV block • Complete AV dissociation • Advanced 2nd degree (two or more consecutive P waves) • Symptommatic 2nd degree AV block, Mobitz 1 and 2 • Mobitz 2 with widened QRS or bifascicular block • Exercise induced second or third degree AV block
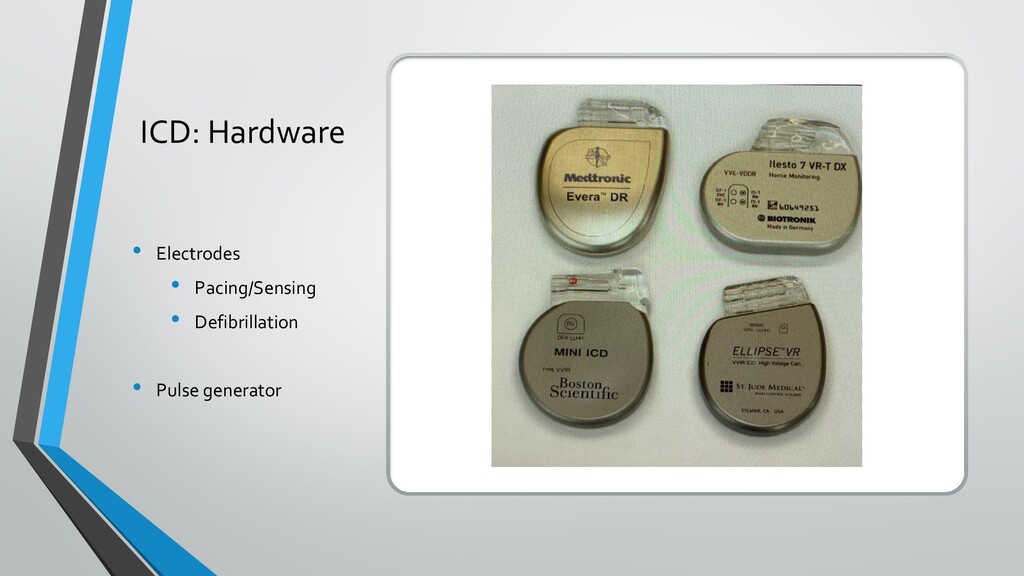
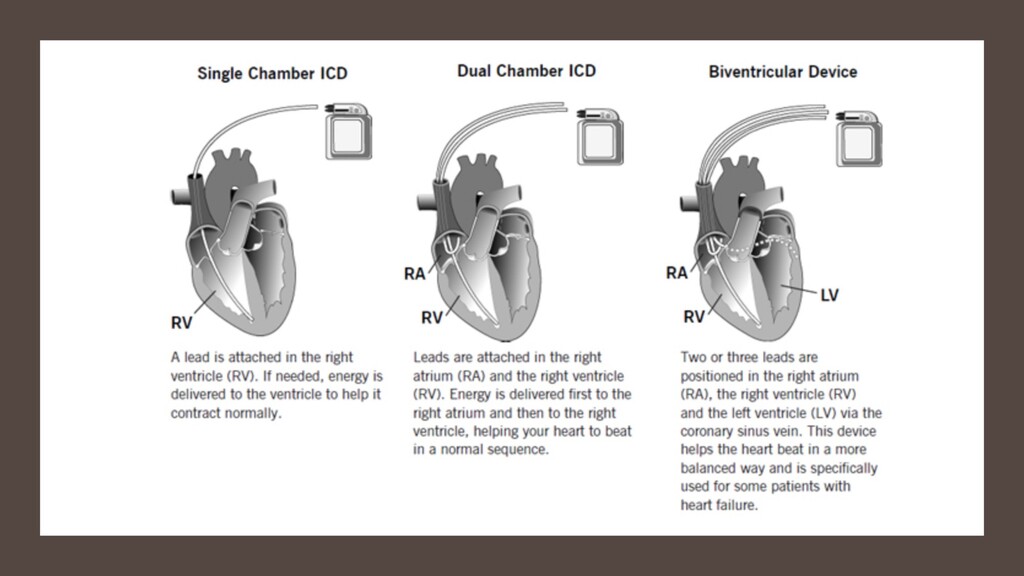
• Trans venous systems: Trans venous electrodes to transmit electrical impulses from the pulse generator to the heart • Epicardial: Direct stimulation through pulse generator attached to the hearts surface • Leadless system: Newer innovation – Medtronic devices
when in the presence of an electromagnetic field – externally. • Most common culprit => Electrosurgery unit • Unipolar or Bipolar • True Bipolar or Integrated Bipolar
device’s magnet response should be known • Most devices will default into asynchronous pacing at a fixed rate • ICD -> a magnet will suspend the tachyarrhythmia detection and therapy • Avoidance of inappropriate shocks • Should be reprogrammed to an asynchronous mode in pacer dependent patients to avoid oversensing or inhibition • Important to note, a magnet will never change a pacing mode of an ICD and inhibition may still occur
to indicate presence of magnet • If there is no beeping then it means device malfunction • Asynchronous pacing at 100BPM • Medtronic: Tone emitted upon device detection of magnet; asynchronous pacing at 85BPM • St Jude: No sound confirmation; Asynchronous at 100BPM • Biotronik: No sound confirmation; asynchronous VOO pacing at 70-90 BPM • Microport/Sorin: Pacing rate to 90, no sound; Asynchronous pacing at 96BPM and then gradually decreasing to 80
the patient should be seen by a rep post operatively • Patient should remain on continuous ICU level monitoring until reprogramming takes place • ICD: EKG, pulse ox and defibrillator pads should be kept in place until patient is reprogrammed or seen by rep • If suspicion is high that arrhythmia took place or device malfunction occurred then clinical acumen prevails and patient should be seen. • Air on side of caution -> if there is a question have patient seen.
need to be done unless it was done within the last three to six months and is working well. • When appropriate alter the pacemaker to an asynchronous pacing mode by placing a magnet. Also, for ICD’s remove antitachycardic function. • Prevent current running through generator • Post op interrogation is not needed if no EMI occurred • Interrogate CIED after emergency surgery for all patients with these devices
the procedures happening in a hospital are outpatient procedures… • Cell phones now have wireless chargers that can alter device generators and affect normal functioning, transcutaneous muscle nerve stimulators • Interrogation studies show about 10% of patients with these devices have outside unintended magnet mode induction events.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}