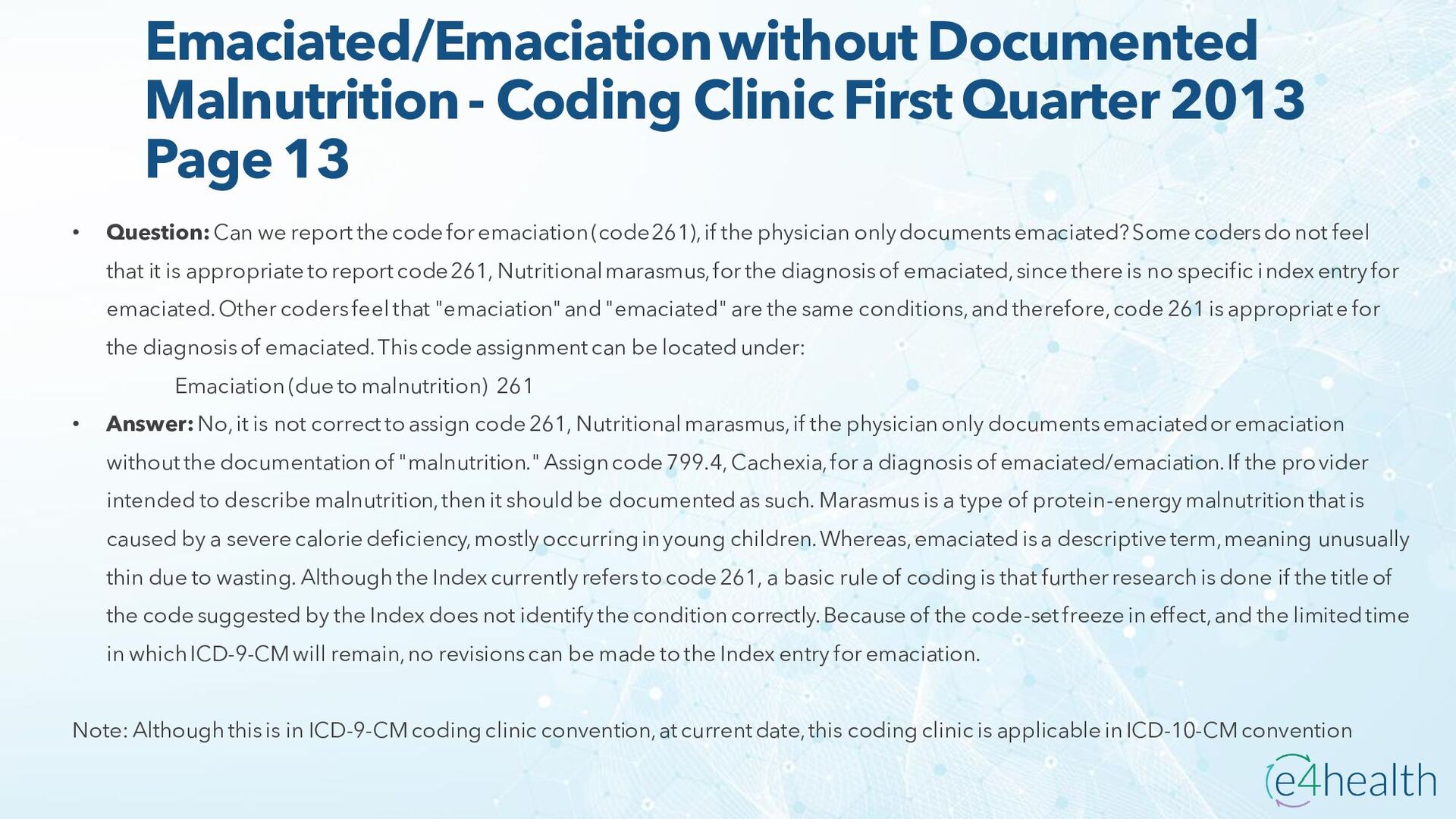
Page 13 • Question:Can we report the code for emaciation (code 261), if the physician only documents emaciated? Some coders do not feel that it is appropriate to report code 261, Nutritional marasmus, for the diagnosis of emaciated, since there is no specific index entry for emaciated. Other coders feel that "emaciation" and "emaciated" are the same conditions, and therefore, code 261 is appropriate for the diagnosis of emaciated. This code assignment can be located under: Emaciation (due to malnutrition) 261 • Answer:No, it is not correct to assign code 261, Nutritional marasmus, if the physician only documents emaciated or emaciation without the documentation of "malnutrition." Assign code 799.4, Cachexia, for a diagnosis of emaciated/emaciation. If the provider intended to describe malnutrition, then it should be documented as such. Marasmus is a type of protein-energy malnutrition that is caused by a severe calorie deficiency, mostly occurring in young children. Whereas, emaciated is a descriptive term, meaning unusually thin due to wasting. Although the Index currently refers to code 261, a basic rule of coding is that further research is done if the title of the code suggested by the Index does not identify the condition correctly. Because of the code-set freeze in effect, and the limited time in which ICD-9-CM will remain, no revisions can be made to the Index entry for emaciation. Note: Although this is in ICD-9-CM coding clinic convention, at current date, this coding clinic is applicable in ICD-10-CM convention
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}