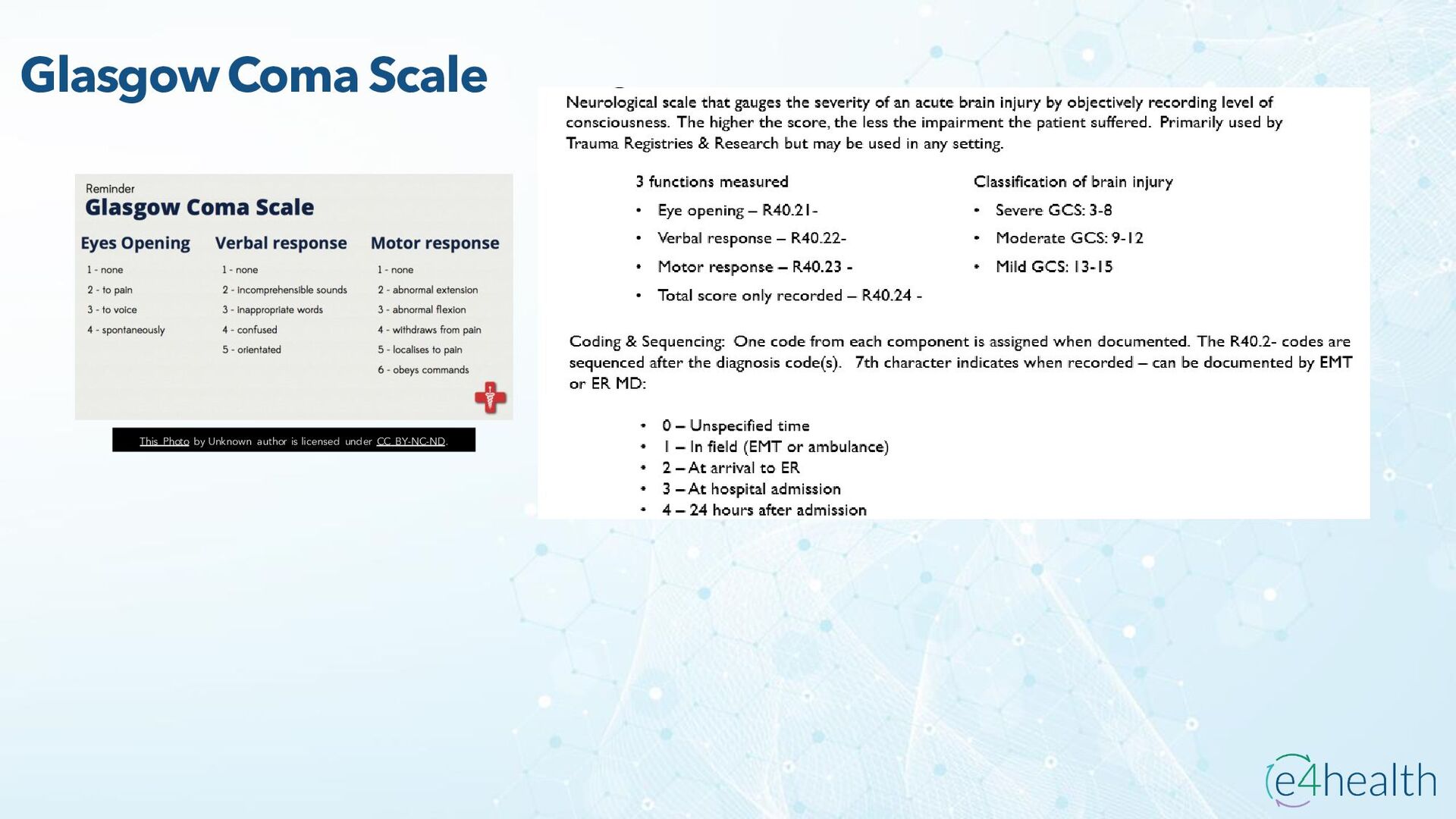
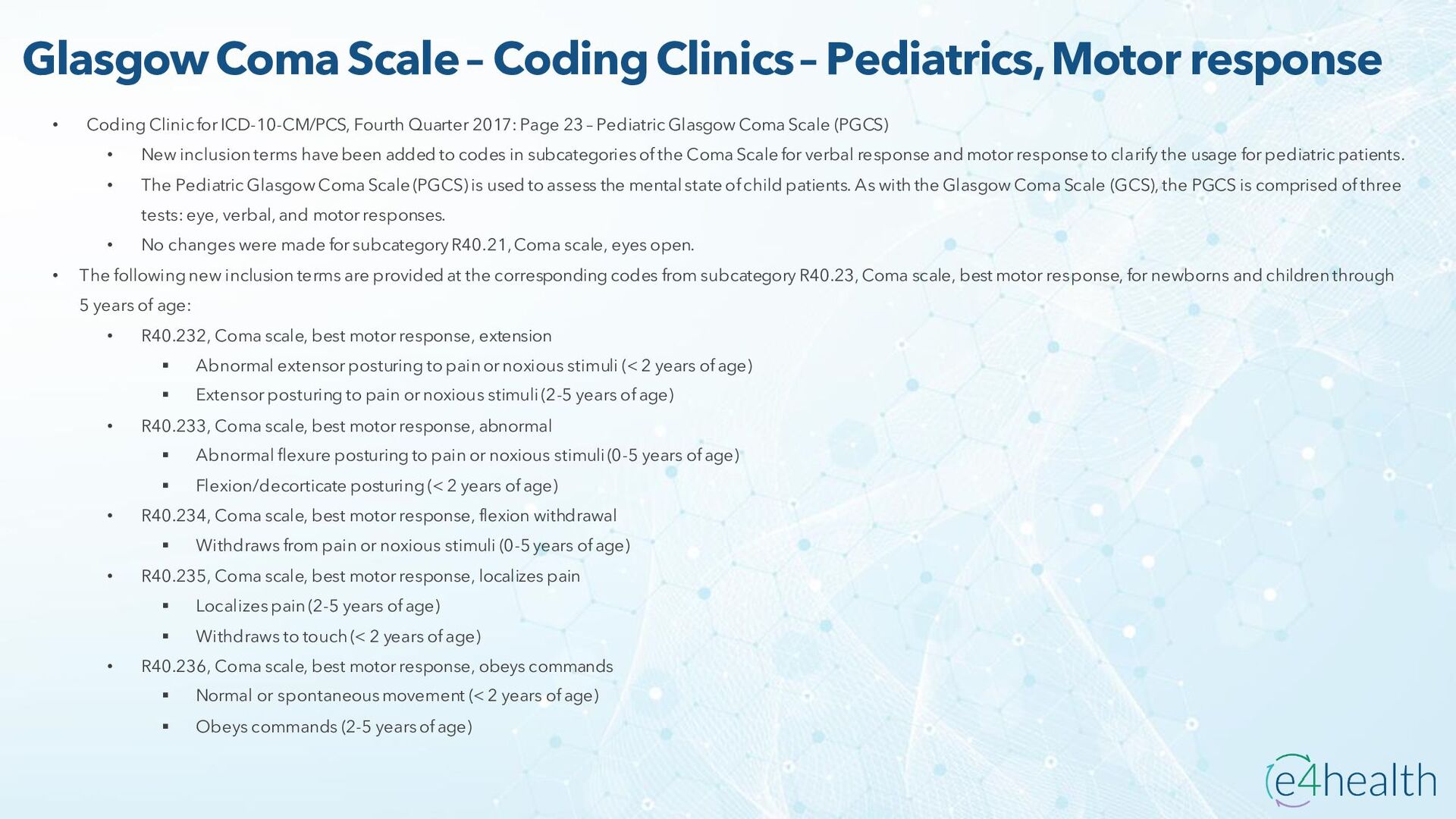
• Coding Clinic for ICD-10-CM/PCS, Fourth Quarter 2017: Page 23 – Pediatric Glasgow Coma Scale (PGCS) • New inclusion terms have been added to codes in subcategories of the Coma Scale for verbal response and motor response to clarify the usage for pediatric patients. • The Pediatric Glasgow Coma Scale (PGCS) is used to assess the mental state of child patients. As with the Glasgow Coma Scale (GCS), the PGCS is comprised of three tests: eye, verbal, and motor responses. • No changes were made for subcategory R40.21, Coma scale, eyes open. • The following new inclusion terms are provided at the corresponding codes from subcategory R40.23, Coma scale, best motor response, for newborns and children through 5 years of age: • R40.232, Coma scale, best motor response, extension ▪ Abnormal extensor posturing to pain or noxious stimuli (< 2 years of age) ▪ Extensor posturing to pain or noxious stimuli (2-5 years of age) • R40.233, Coma scale, best motor response, abnormal ▪ Abnormal flexure posturing to pain or noxious stimuli (0-5 years of age) ▪ Flexion/decorticate posturing (< 2 years of age) • R40.234, Coma scale, best motor response, flexion withdrawal ▪ Withdraws from pain or noxious stimuli (0-5 years of age) • R40.235, Coma scale, best motor response, localizes pain ▪ Localizes pain (2-5 years of age) ▪ Withdraws to touch (< 2 years of age) • R40.236, Coma scale, best motor response, obeys commands ▪ Normal or spontaneous movement (< 2 years of age) ▪ Obeys commands (2-5 years of age)
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}