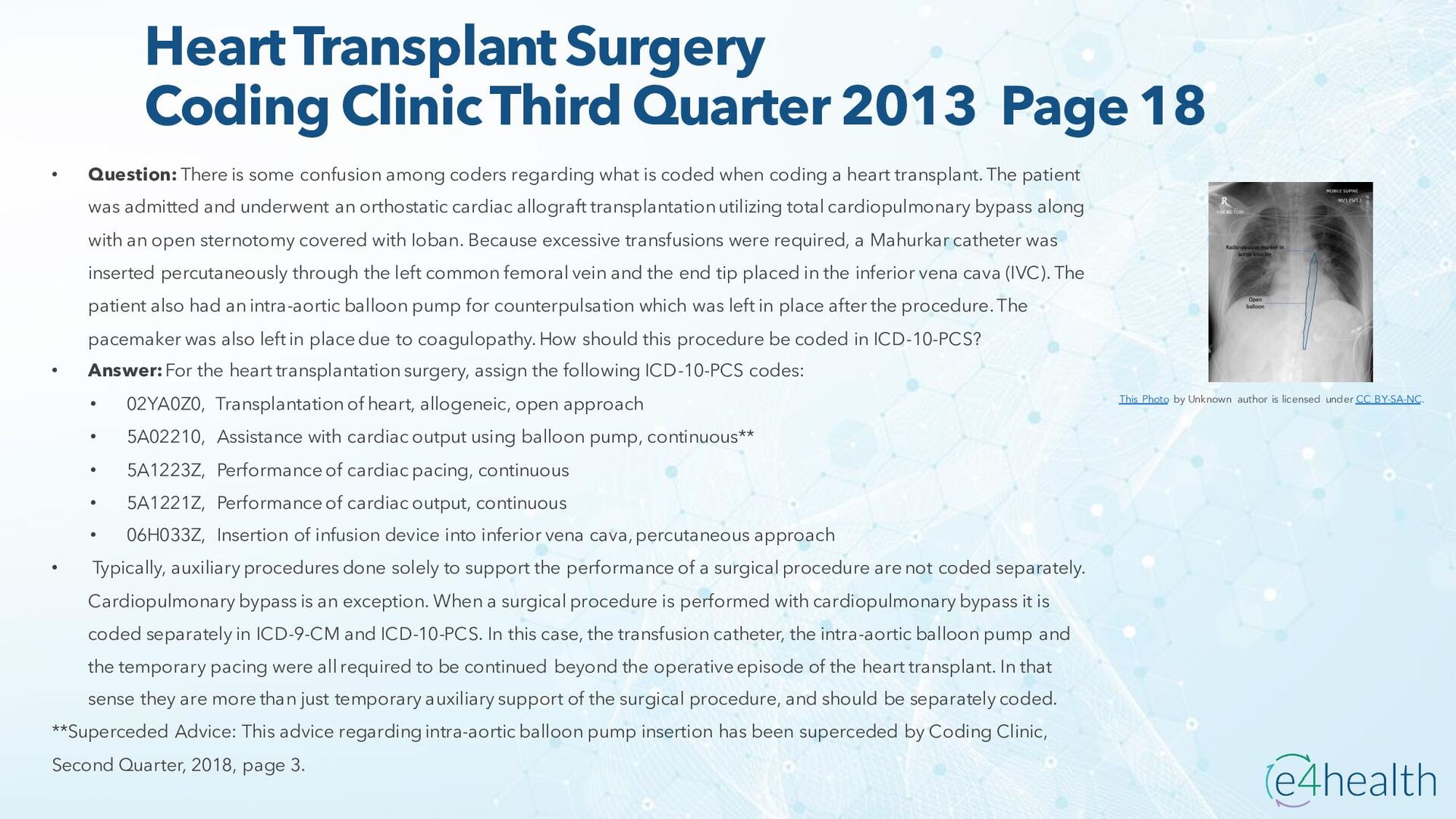
• Question: There is some confusion among coders regarding what is coded when coding a heart transplant. The patient was admitted and underwent an orthostatic cardiac allograft transplantation utilizing total cardiopulmonary bypass along with an open sternotomy covered with Ioban. Because excessive transfusions were required, a Mahurkar catheter was inserted percutaneously through the left common femoral vein and the end tip placed in the inferior vena cava (IVC). The patient also had an intra-aortic balloon pump for counterpulsation which was left in place after the procedure. The pacemaker was also left in place due to coagulopathy. How should this procedure be coded in ICD-10-PCS? • Answer: For the heart transplantation surgery, assign the following ICD-10-PCS codes: • 02YA0Z0, Transplantation of heart, allogeneic, open approach • 5A02210, Assistance with cardiac output using balloon pump, continuous** • 5A1223Z, Performance of cardiac pacing, continuous • 5A1221Z, Performance of cardiac output, continuous • 06H033Z, Insertion of infusion device into inferior vena cava, percutaneous approach • Typically, auxiliary procedures done solely to support the performance of a surgical procedure are not coded separately. Cardiopulmonary bypass is an exception. When a surgical procedure is performed with cardiopulmonary bypass it is coded separately in ICD-9-CM and ICD-10-PCS. In this case, the transfusion catheter, the intra-aortic balloon pump and the temporary pacing were all required to be continued beyond the operative episode of the heart transplant. In that sense they are more than just temporary auxiliary support of the surgical procedure, and should be separately coded. **Superceded Advice: This advice regarding intra-aortic balloon pump insertion has been superceded by Coding Clinic, Second Quarter, 2018, page 3. This Photo by Unknown author is licensed under CC BY-SA-NC.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}