and will be available after the webinar. • The slides will also be available after the webinar. • All attendees are on mute. • Please submit your questions in the questions box on the right-hand side of your screen to be answered at the end of the session. 2
• Medicare and Medicaid Expenditures on Duals • Characteristics of Dual-Eligibles • Innovative Care Models Gaining Traction • Clinical Complexity of Duals • Psychosocial Factors Impacting Duals • Restructuring Required to Serve Duals • Care Coordination for Duals
duals: • Eligibility levels for Medicaid vary by state • Medicaid pays for all Medicare premiums and cost sharing • Eligible for full Medicaid benefits under State Plan – Partial benefit duals: • Qualified Medicare Beneficiary (QMB) – income ≤100% FPL – Medicaid pays all Medicare premiums, deductibles, and cost sharing • Specified Low-Income Medicare Beneficiary (SLMB) – income > 100% FPL and < 120% FPL – Medicaid pays Medicare Part B premium • Qualified Individual (QI) – income ≥ 120% FPL and < 135% FPL – Medicaid pays Medicare Part B premium 7
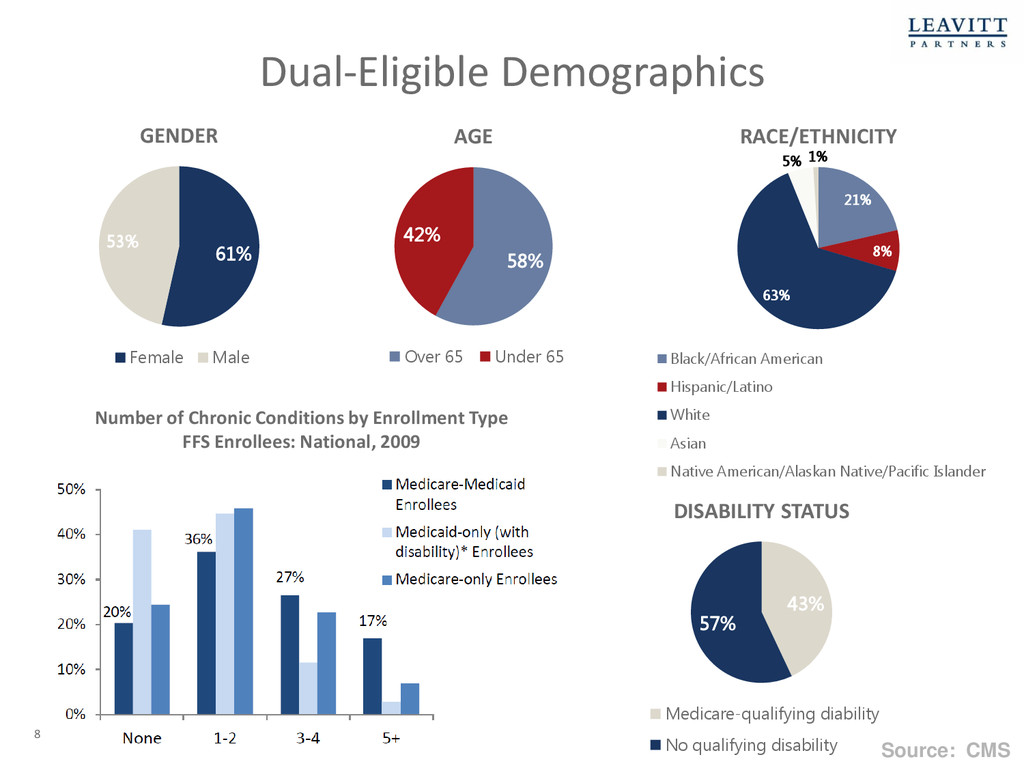
8% 63% 5% 1% RACE/ETHNICITY Black/African American Hispanic/Latino White Asian Native American/Alaskan Native/Pacific Islander 61% 53% GENDER Female Male 43% 57% DISABILITY STATUS Medicare-qualifying diability No qualifying disability Number of Chronic Conditions by Enrollment Type FFS Enrollees: National, 2009 Dual-Eligible Demographics Source: CMS 8
between State, CMS, and health plan • Health Plan receives prospective blended rate to provide comprehensive, coordinated care • PMPM rate reflects “aggregate savings percentage” applied to both Medicaid and Medicare • Models: Capitated Model 13
• State shares in savings resulting from state designed and implemented initiatives to improve quality and reduce costs for both Medicare and Medicaid • Providers continue to receive separate FFS payments from Medicaid and Medicare • Care coordination entity receives PMPM payment • Models: Managed Fee-for-Service Model 14
State Plan and Medicare Advantage • Must have contracts with State Medicaid agency to coordinate services • States are increasingly using D-SNP model to manage their long term services and supports by requiring Medicaid managed care plans to also be approved D-SNPs* Duals Special Needs Plans (D-SNPs) * AZ, HI, MA, MN, NM, TN, TX, WI 15
Mental Health Parity and Addiction Equity Act (MHPAEA) • Long term services and supports integration including Medicaid home and community based services • Opportunities and challenges of integrating more and new services, including non-medical services Integrating Services Beyond Primary And Acute Care 16
Here • CMS Funded Resource Center, Resources for Integrated Care. Available Here • Data Analysis Brief: Medicare-Medicaid Dual Enrollment from 2006 through 2013. Available Here • CMS Medicare-Medicaid Enrollee Information. Available Here • Medicare-Medicaid Coordination Office Fiscal Year 2014 Report to Congress. Available Here • MEDPAC Dual-Eligible Beneficiaries. Available Here 17
Are a Very Unmanaged Population • Not accustomed to managed care processes • Utilization Management • Case Management • Fragmented, uncoordinated expensive care • Long Term Care • Home Health • DME • Imaging • Services fraught with fraud, waste and abuse 19 *2013 Dual-Eligible Beneficiaries of Medicare and Medicaid: Characteristics, Health Care Spending, and Evolving Policies, Congressional Budget Office. More than 40 percent of duals use community-based and institutional long-term services and other social support services - a far greater percentage than for other Medicare or Medicaid beneficiaries.*
by poverty • 86% are below 150% Federal Poverty Level* • Multiple comorbid conditions • Leading conditions including Diabetes, COPD, Congestive Heart Failure, Dementia and Osteoporosis. • Higher rates of disability • Serious polypharmacy issues • Expensive DME requirements • Lack of medical home or PCP • Frequent ED use • Frequent and protracted inpatient admissions 20 *Kaiser Family Foundation.
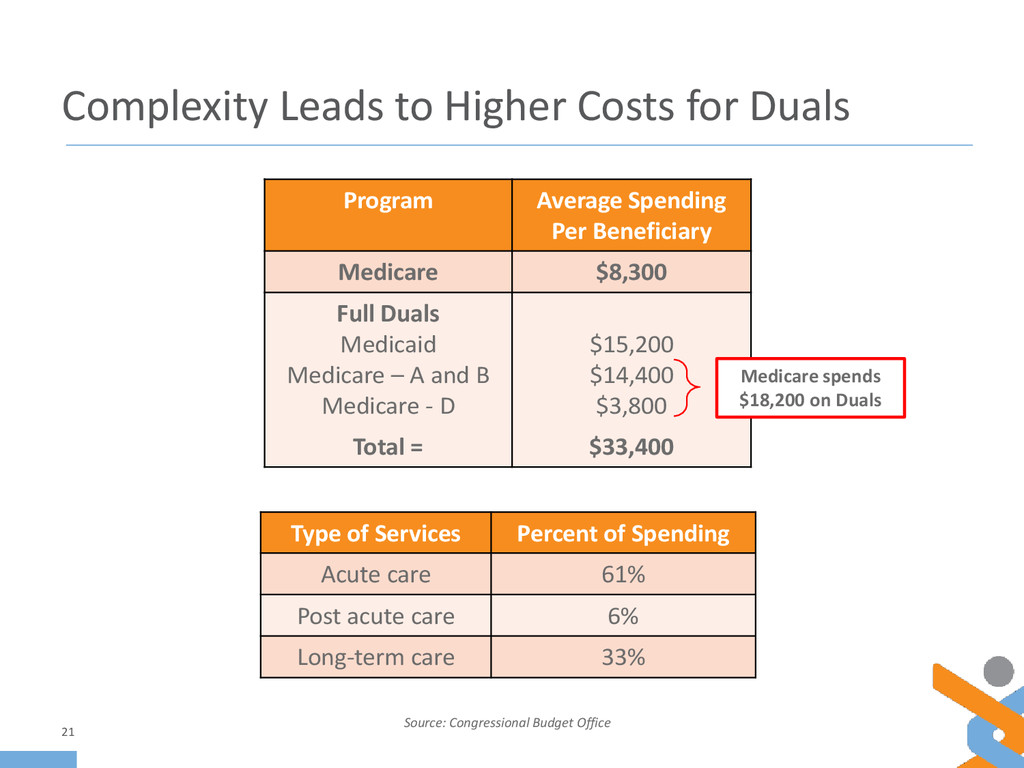
21 Source: Congressional Budget Office Program Average Spending Per Beneficiary Medicare $8,300 Full Duals Medicaid Medicare – A and B Medicare - D $15,200 $14,400 $3,800 Total = $33,400 Medicare spends $18,200 on Duals Type of Services Percent of Spending Acute care 61% Post acute care 6% Long-term care 33%
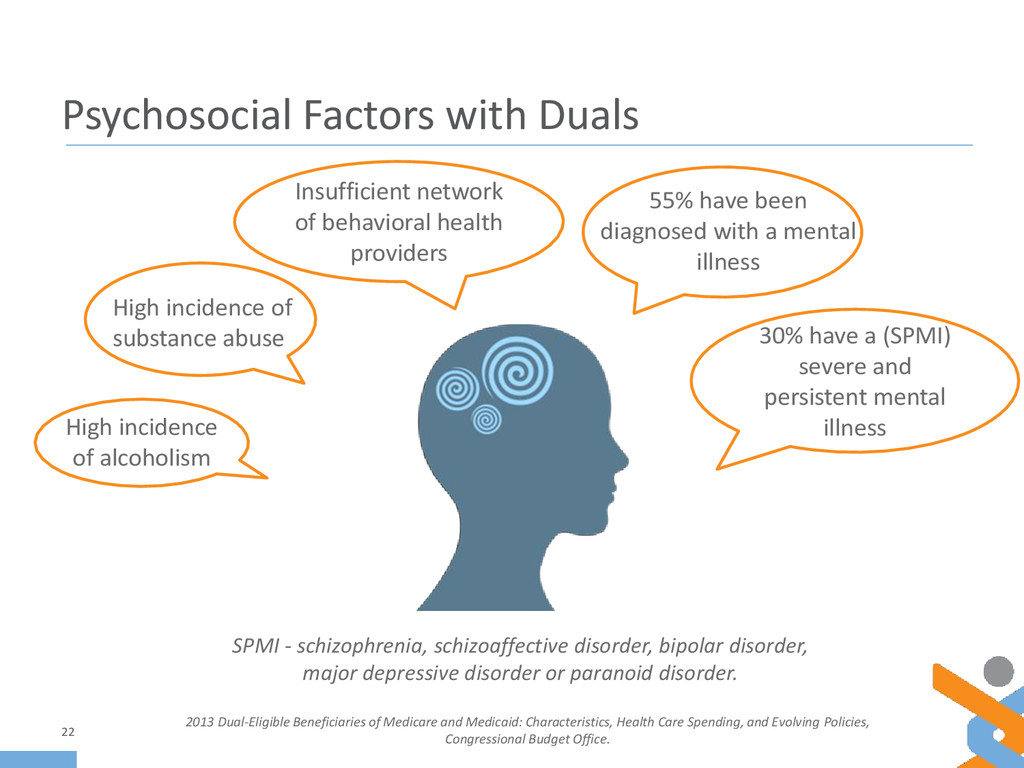
Beneficiaries of Medicare and Medicaid: Characteristics, Health Care Spending, and Evolving Policies, Congressional Budget Office. 55% have been diagnosed with a mental illness High incidence of substance abuse High incidence of alcoholism Insufficient network of behavioral health providers 30% have a (SPMI) severe and persistent mental illness SPMI - schizophrenia, schizoaffective disorder, bipolar disorder, major depressive disorder or paranoid disorder.
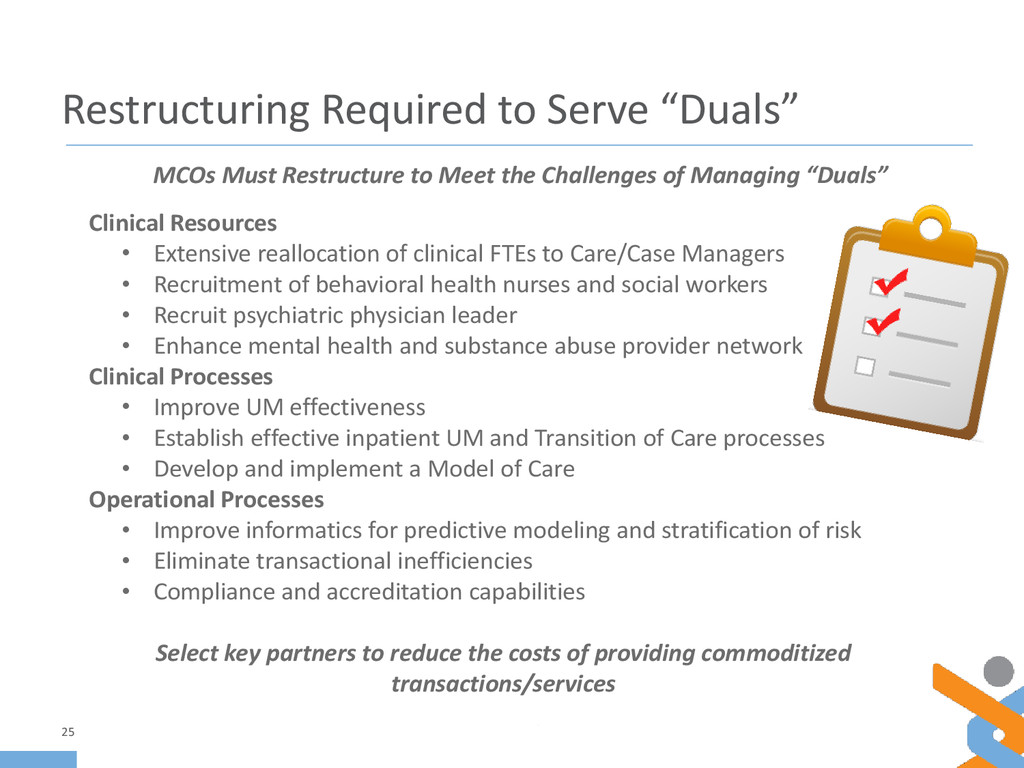
• Extensive reallocation of clinical FTEs to Care/Case Managers • Recruitment of behavioral health nurses and social workers • Recruit psychiatric physician leader • Enhance mental health and substance abuse provider network Clinical Processes • Improve UM effectiveness • Establish effective inpatient UM and Transition of Care processes • Develop and implement a Model of Care Operational Processes • Improve informatics for predictive modeling and stratification of risk • Eliminate transactional inefficiencies • Compliance and accreditation capabilities Select key partners to reduce the costs of providing commoditized transactions/services 25 MCOs Must Restructure to Meet the Challenges of Managing “Duals”
Model of Care – Care Coordination • Health Risk Assessments • Individualized Care Plans • Interdisciplinary Care Team (ICT) • Transitions in Care Integrated care and service delivery • Unified medical, behavioral and social support care across all interventions • High-contact, on-the-ground support and coordination for Members, Community Resources, Providers and Plan. 26 Align with key partners to fill in any gaps in the Model of Care
Eligible for Medicare and Medicaid • Clinically complex with multiple chronic conditions and behavioral co- morbidities – Drives up the cost of care – Requires a new level of care coordination and clinical expertise • Opportunities exist to integrate care and other services to better serve this population • Align with key partners to help you best serve your members 27
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}