FLARES Over 30% of Active Flares in Inflammatory Bowel Disease Patients Are Associated with Gastrointestinal Infectious Agents Julajak Limsrivilai1,2, Zachary Saleh1, Laura Johnson1, Ryan W. Stidham1, Akbar K. Waljee1, Brian Gutermuth1, Shail Mahendra Govani3, Alexandra Brown1, Emily Briggs1, Krishna Rao1, Peter D.R. Higgins1 1. Department of Internal Medicine, University of Michigan 2. Mahidol University, Bangkok, Thailand 3. Department of Internal Medicine, South Texas VA, San Antonio, TX Slides: @ibddoctor Slide deck: https://speakerdeck.com/higgi13425
FLARES Clinical Question • A patient with Crohn’s disease is admitted to to the inpatient service with 8 bowel movements per day, pain, and dehydration. • The smart young intern has ordered a new PCR panel for GI infections. • Result: positive for E. coli (EPEC) • What to do with this result? PCR Results Positive
FLARES Intestinal Infections Matter in IBD • Gastrointestinal infections, including Salmonella and Campylobacter, are associated with the onset of IBD. • Clostridium difficile infection has been associated with IBD flares, longer hospital LOS, and increased colectomy in IBD. • Hypothesis: associations due to activation of the gut immune system, and lead to worsening of IBD. • Question: Can other gastrointestinal infections worsen IBD? Gastro 2006: 130:1588, Gut 2011;60:318-324, APT 2011;33:1322, IBD 2011;17:976
FLARES The Problem with GI PCR Panels • Detects organisms that are present in stool • Very sensitive testing • Presence of infectious agent does NOT equal infection! • Colonization occurs • Up to 8% of IBD patients colonized with C. difficile • Asymptomatic carriers exist • Mary Mallon • Gallstones reportedly colonized with Salmonella typhi (Ann Gastroenterol. 2013; 26(2): 132–134.)
FLARES Questions We Want to Answer Question 1. Is the Presence of GI Infectious agents associated with Active IBD? 2. Which infectious agents are differentially associated with Active IBD? 3. Are there factors in the clinical presentation that predict positive tests? 4. Are particular medications associated with more frequent detection of GI infectious agents? 5. What is the clinical impact of the presence of GI infectious agents?
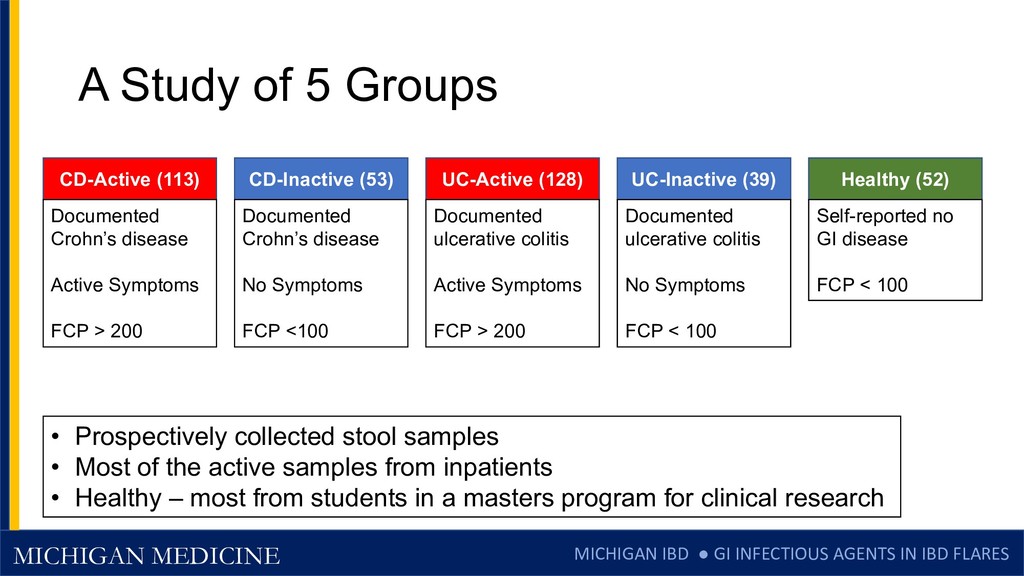
FLARES A Study of 5 Groups CD-Active (113) Documented Crohn’s disease Active Symptoms FCP > 200 CD-Inactive (53) Documented Crohn’s disease No Symptoms FCP <100 UC-Active (128) Documented ulcerative colitis Active Symptoms FCP > 200 UC-Inactive (39) Documented ulcerative colitis No Symptoms FCP < 100 Healthy (52) Self-reported no GI disease FCP < 100 • Prospectively collected stool samples • Most of the active samples from inpatients • Healthy – most from students in a masters program for clinical research
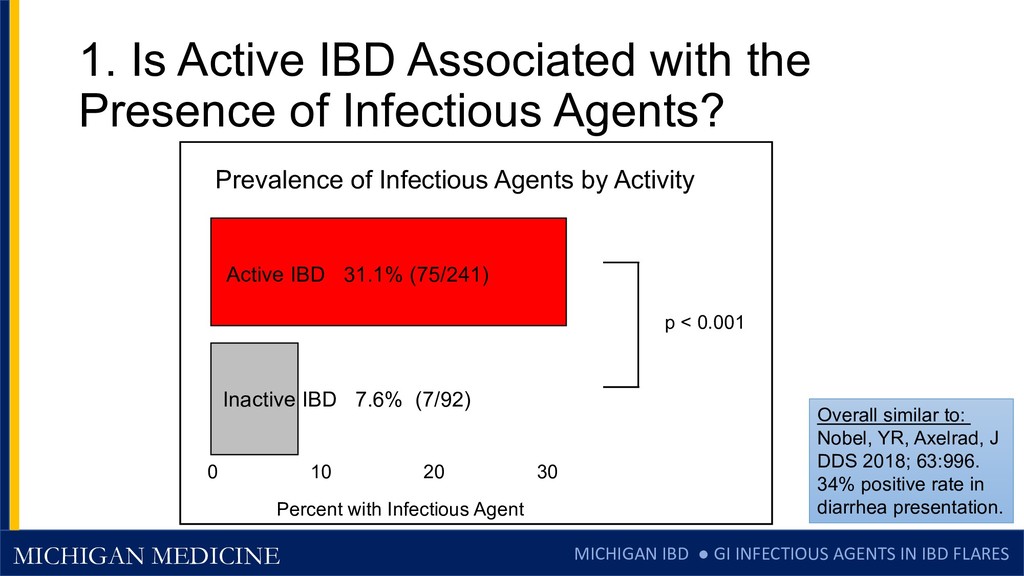
FLARES 1. Is Active IBD Associated with the Presence of Infectious Agents? p < 0.001 Overall similar to: Nobel, YR, Axelrad, J DDS 2018; 63:996. 34% positive rate in diarrhea presentation. 0 10 20 30 Percent with Infectious Agent Prevalence of Infectious Agents by Activity Active IBD 31.1% (75/241) Inactive IBD 7.6% (7/92)
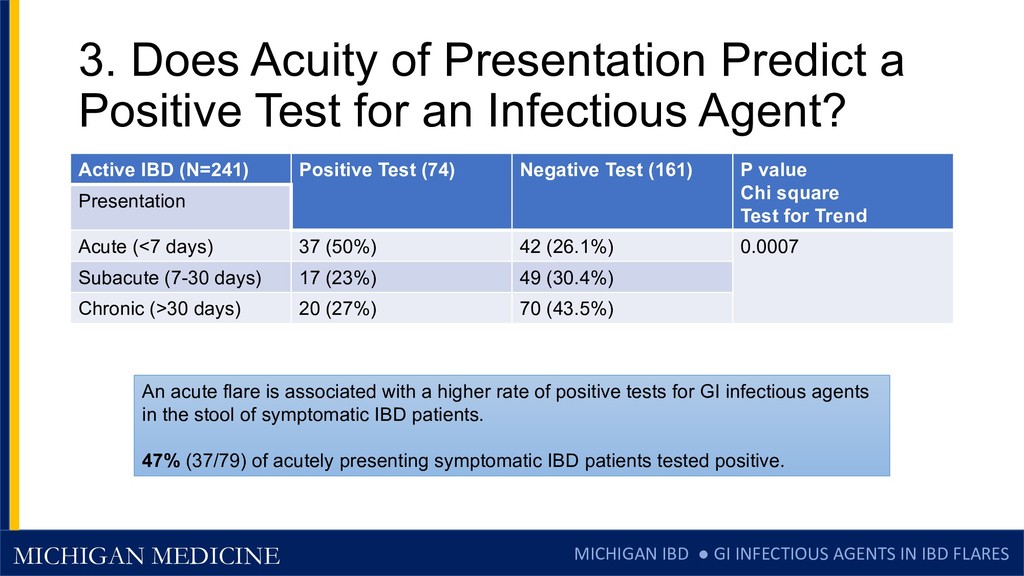
FLARES 3. Does Acuity of Presentation Predict a Positive Test for an Infectious Agent? Active IBD (N=241) Positive Test (74) Negative Test (161) P value Chi square Test for Trend Presentation Acute (<7 days) 37 (50%) 42 (26.1%) 0.0007 Subacute (7-30 days) 17 (23%) 49 (30.4%) Chronic (>30 days) 20 (27%) 70 (43.5%) An acute flare is associated with a higher rate of positive tests for GI infectious agents in the stool of symptomatic IBD patients. 47% (37/79) of acutely presenting symptomatic IBD patients tested positive.
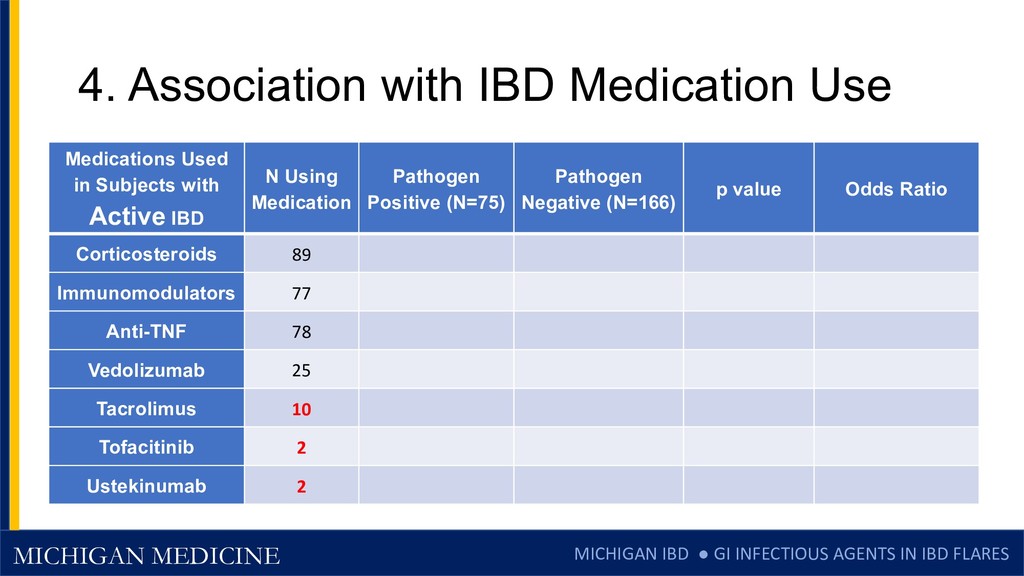
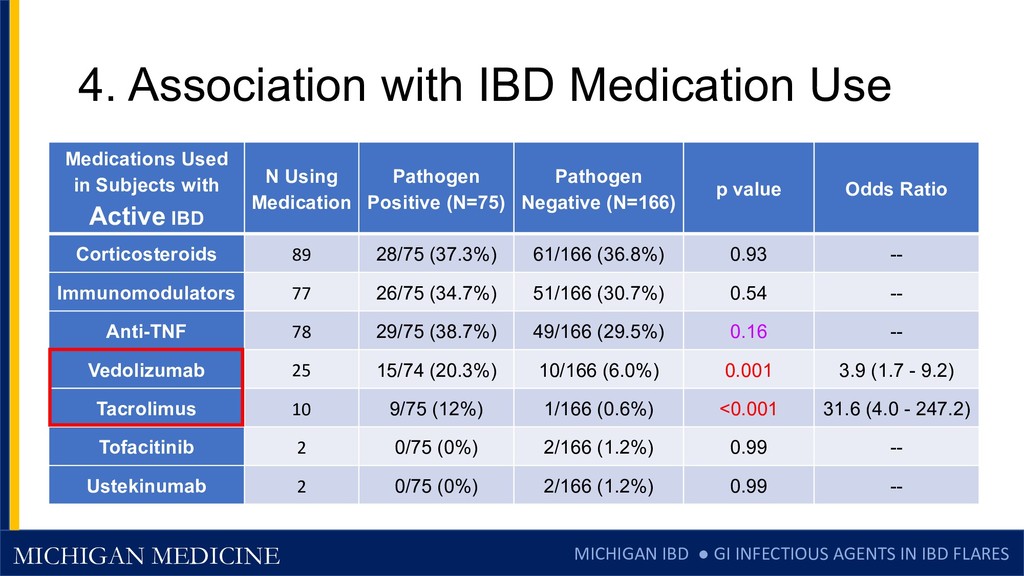
FLARES 4. Association with IBD Medication Use Medications Used in Subjects with Active IBD N Using Medication Pathogen Positive (N=75) Pathogen Negative (N=166) p value Odds Ratio Corticosteroids 89 Immunomodulators 77 Anti-TNF 78 Vedolizumab 25 Tacrolimus 10 Tofacitinib 2 Ustekinumab 2
FLARES 5. Clinical Outcomes with Positive Tests Clinical Outcome Positive Test (75) Negative Test (166) P value Steroids initiated 54.7% (41) 77.7% (129) 0.0001 Escalation of IBD Therapy 61.3% (46) 84.9% (141) <0.0001 Surgery within 90 days 13.3% (10) 18.7% (31) 0.31 Re-hospitalization in 90 days 16% (12) 20.5% (34) 0.41 Composite (steroids, re-hospitalization, surgery) 62.7% (47) 80.7% (134) 0.0027 Unexpected: a detectable GI infectious agent can be bad, but a true IBD flare without a detectable infectious agent produces worse outcomes.
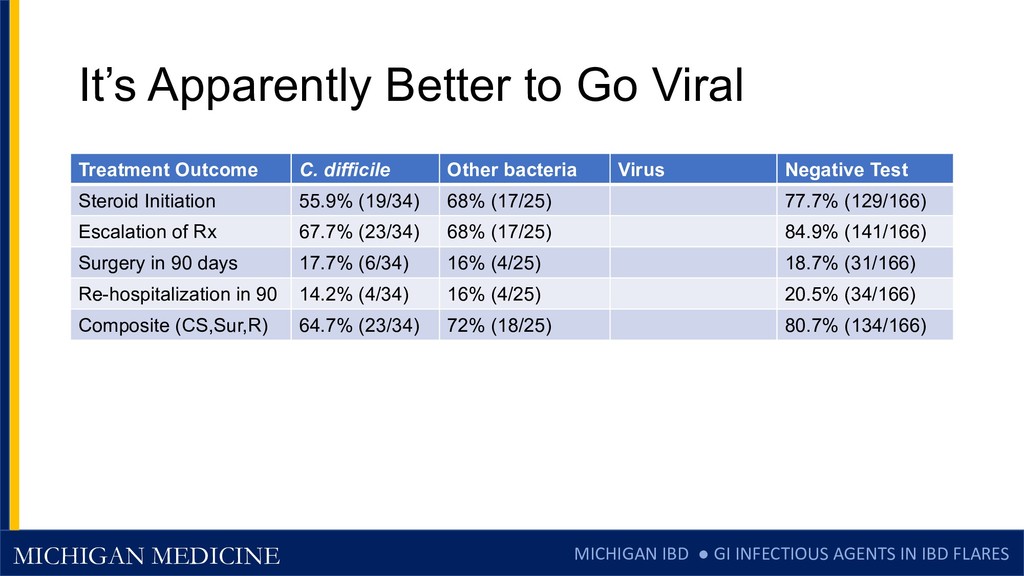
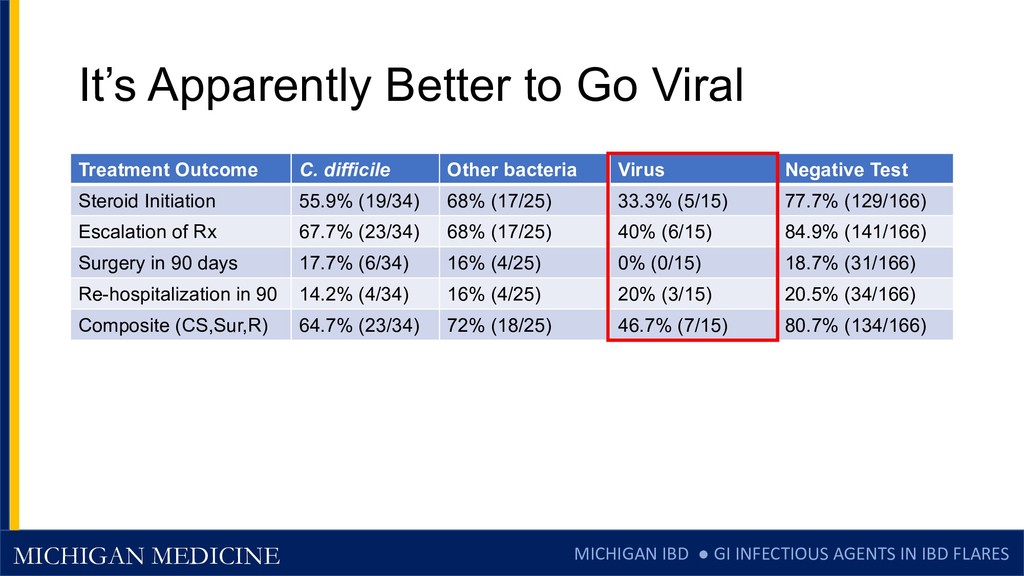
FLARES It’s Apparently Better to Go Viral Treatment Outcome C. difficile Other bacteria Virus Negative Test Steroid Initiation Escalation of Rx Surgery in 90 days Re-hospitalization in 90 Composite (CS,Sur,R)
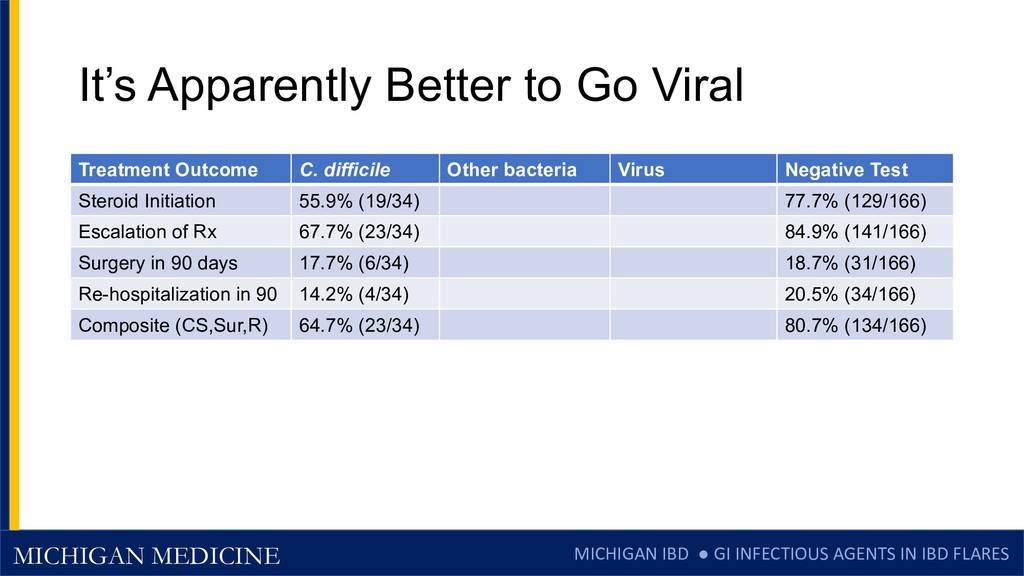
FLARES It’s Apparently Better to Go Viral Treatment Outcome C. difficile Other bacteria Virus Negative Test Steroid Initiation 55.9% (19/34) 77.7% (129/166) Escalation of Rx 67.7% (23/34) 84.9% (141/166) Surgery in 90 days 17.7% (6/34) 18.7% (31/166) Re-hospitalization in 90 14.2% (4/34) 20.5% (34/166) Composite (CS,Sur,R) 64.7% (23/34) 80.7% (134/166)
FLARES Limitations • Cross-sectional design = Associations, not causation. • Exploratory analyses of Q3-Q5 are hypothesis-generating. • Alternative explanations: • IBD flares could shift microbiome, allow increased colonization by pathogens • But most infectious agents occurred in acute onset • Immunosuppressive IBD meds for flares could be permissive for GI pathogen growth and expansion • Not much for steroids alone – but this may be true for triple IS (Vedo/Tacro/CS) • Results are from a single tertiary care center in Michigan • May not be generalizable to all settings • Pattern of GI infectious agents may be quite different in other locations, i.e. Bangkok, Thailand.
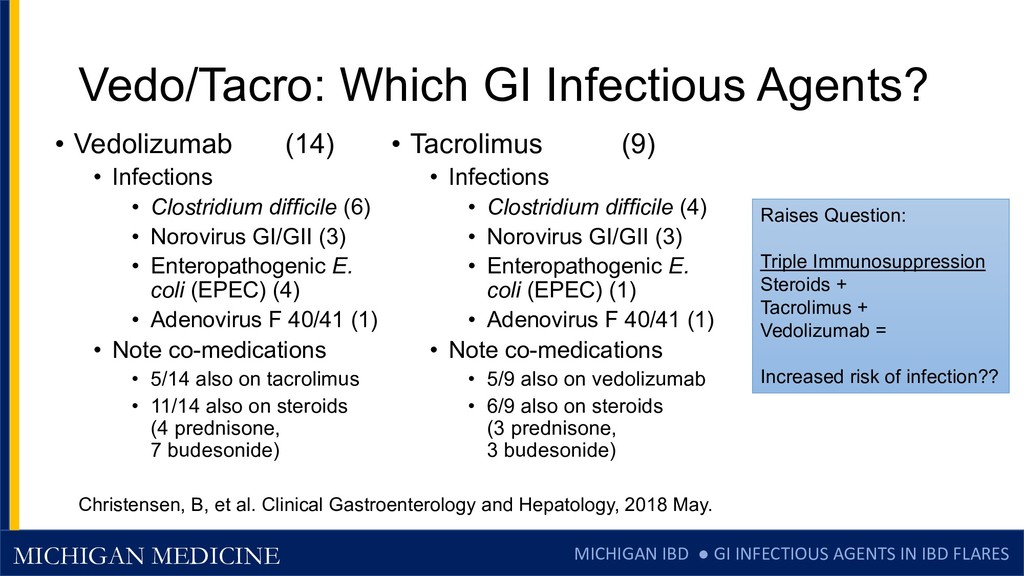
FLARES Conclusions • Active CD and UC patients have a higher rate (31.3%) of detectable GI infectious agents than asymptomatic patients (7.6%). • In IBD patients with acute flares (<7 days, abrupt onset), 47% had a detectable infectious agent in their stool. • Triple immunosuppression with steroids + Tacro + Vedo was associated with an increased presence of infectious agents. • Patients with detected infectious agents (especially viral) have less severe flares, and are often responsive to supportive care without corticosteroids.
FLARES Who To Test? •Test • Acute onset of symptoms • Active inflammation • Triple immunosuppression • Considering steroids •Treat • Clostridium difficile • Norovirus, other infections - Supportive care (IV fluids) • ? EPEC in CD Who to Treat?
FLARES Thank You to the Team Julajak Limsrivilai Ryan Stidham Krishna Rao Emily Briggs Laura Johnson Lexi Brown Zach Saleh Shail Govani Akbar Waljee Brian Gutermuth
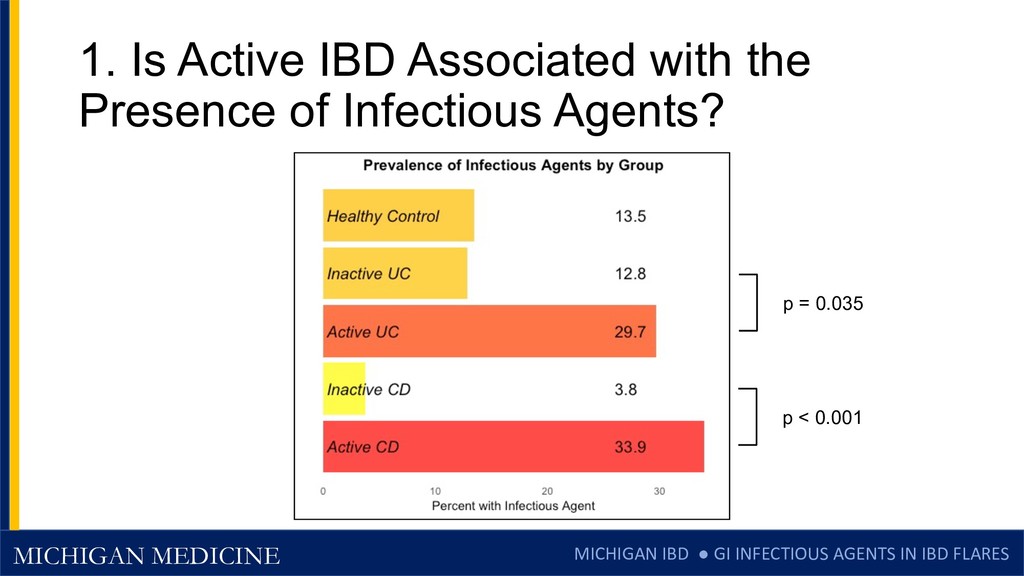
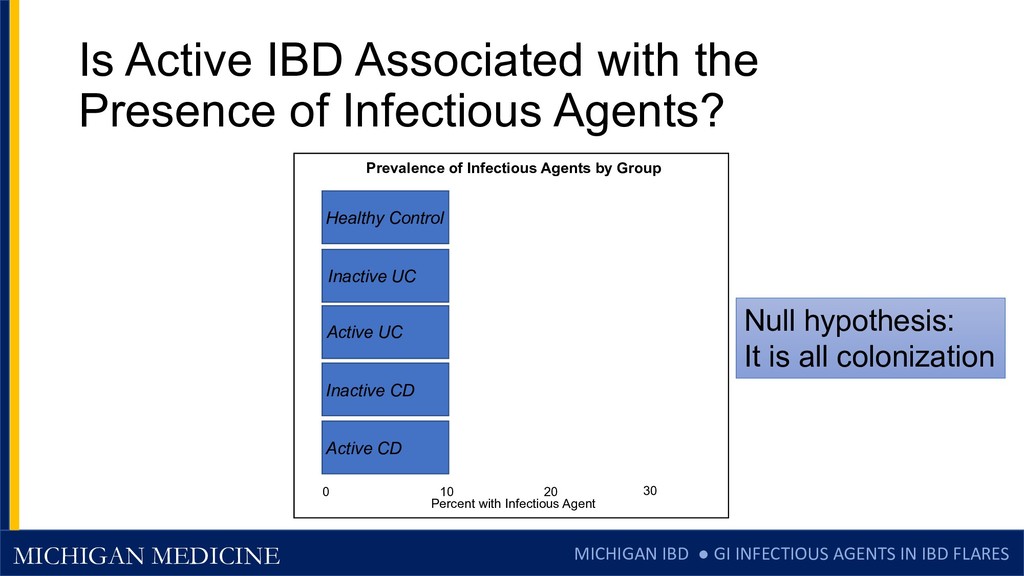
FLARES Is Active IBD Associated with the Presence of Infectious Agents? Prevalence of Infectious Agents by Group Percent with Infectious Agent 0 10 20 30 Healthy Control Inactive UC Active UC Inactive CD Active CD Null hypothesis: It is all colonization
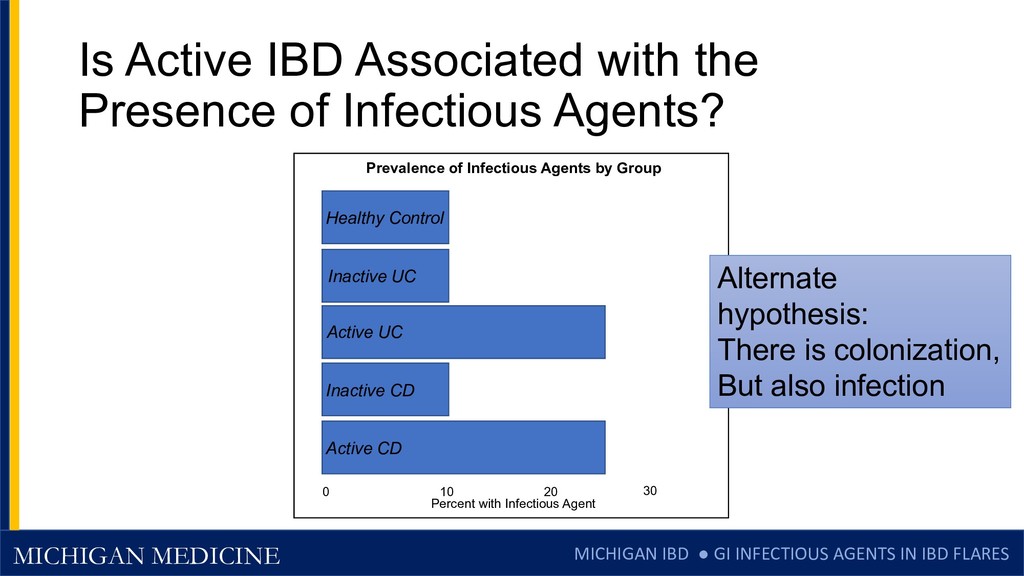
FLARES Is Active IBD Associated with the Presence of Infectious Agents? Prevalence of Infectious Agents by Group Percent with Infectious Agent 0 10 20 30 Healthy Control Inactive UC Active UC Inactive CD Active CD Alternate hypothesis: There is colonization, But also infection
FLARES Role of the Sponsor in the Research • Sponsor (Biomerieux) reviewed the scientific proposal • Sponsor provided testing device, test kits • Sponsor paid $4000 US for technician time • Sponsor was not involved in drafting slides or manuscript • None of the investigators has any financial relationship with the sponsor.
FLARES Clinical and Trial Implications • How often are flares and “failed” therapies due to infections with Norovirus or EPEC, rather than true CD flares? • At the onset of flares, consider testing for infection and avoiding steroids if positive – supportive care often sufficient (with the exception of CDI) • For clinical trials • Do some subjects enter trials with norovirus or EPEC, then improve? (placebo response rate increased) – endoscopic entry criteria important. • Do some subjects drop out of IBD trials due to Noro/EPEC infections? (did not truly fail therapy)
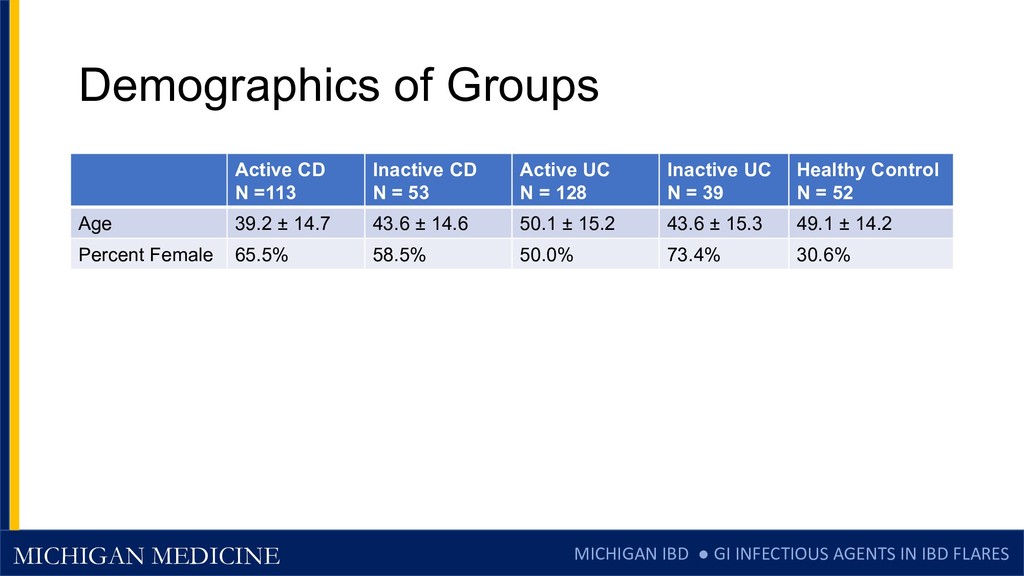
FLARES Demographics of Groups Active CD N =113 Inactive CD N = 53 Active UC N = 128 Inactive UC N = 39 Healthy Control N = 52 Age 39.2 ± 14.7 43.6 ± 14.6 50.1 ± 15.2 43.6 ± 15.3 49.1 ± 14.2 Percent Female 65.5% 58.5% 50.0% 73.4% 30.6%
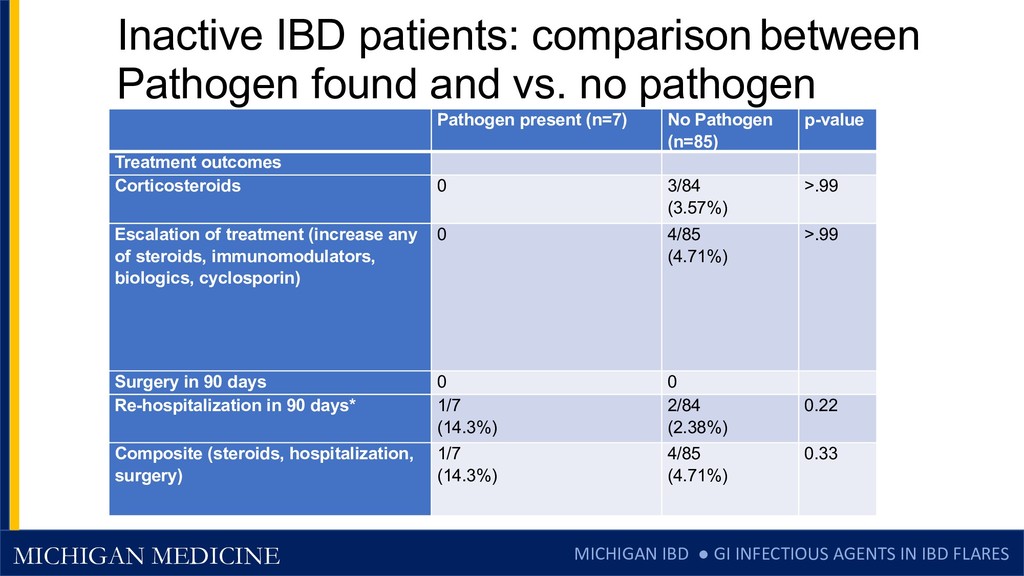
FLARES Inactive IBD patients: comparison between Pathogen found and vs. no pathogen Pathogen present (n=7) No Pathogen (n=85) p-value Treatment outcomes Corticosteroids 0 3/84 (3.57%) >.99 Escalation of treatment (increase any of steroids, immunomodulators, biologics, cyclosporin) 0 4/85 (4.71%) >.99 Surgery in 90 days 0 0 Re-hospitalization in 90 days* 1/7 (14.3%) 2/84 (2.38%) 0.22 Composite (steroids, hospitalization, surgery) 1/7 (14.3%) 4/85 (4.71%) 0.33
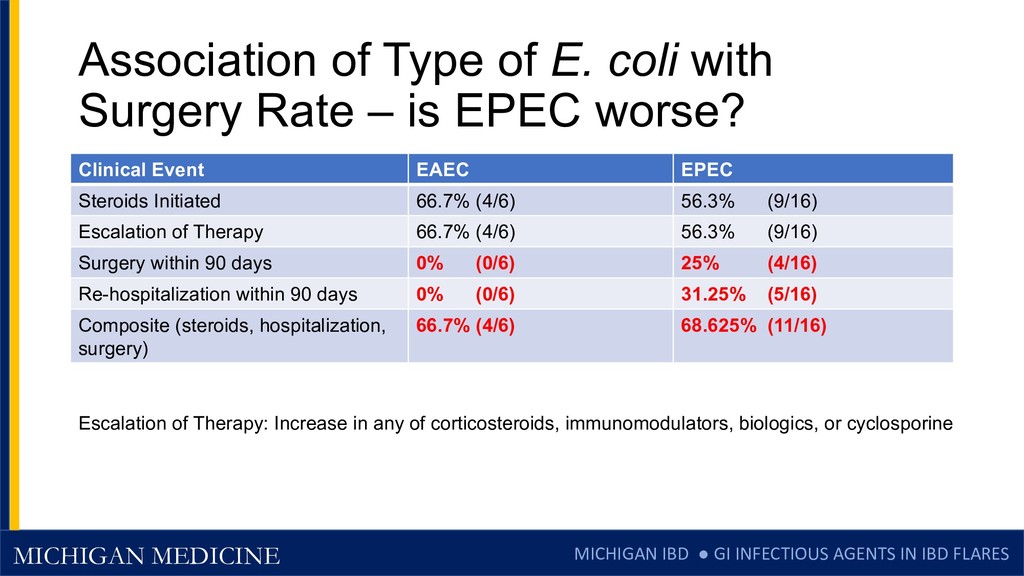
FLARES Association of Type of E. coli with Surgery Rate – is EPEC worse? Clinical Event EAEC EPEC Steroids Initiated 66.7% (4/6) 56.3% (9/16) Escalation of Therapy 66.7% (4/6) 56.3% (9/16) Surgery within 90 days 0% (0/6) 25% (4/16) Re-hospitalization within 90 days 0% (0/6) 31.25% (5/16) Composite (steroids, hospitalization, surgery) 66.7% (4/6) 68.625% (11/16) Escalation of Therapy: Increase in any of corticosteroids, immunomodulators, biologics, or cyclosporine
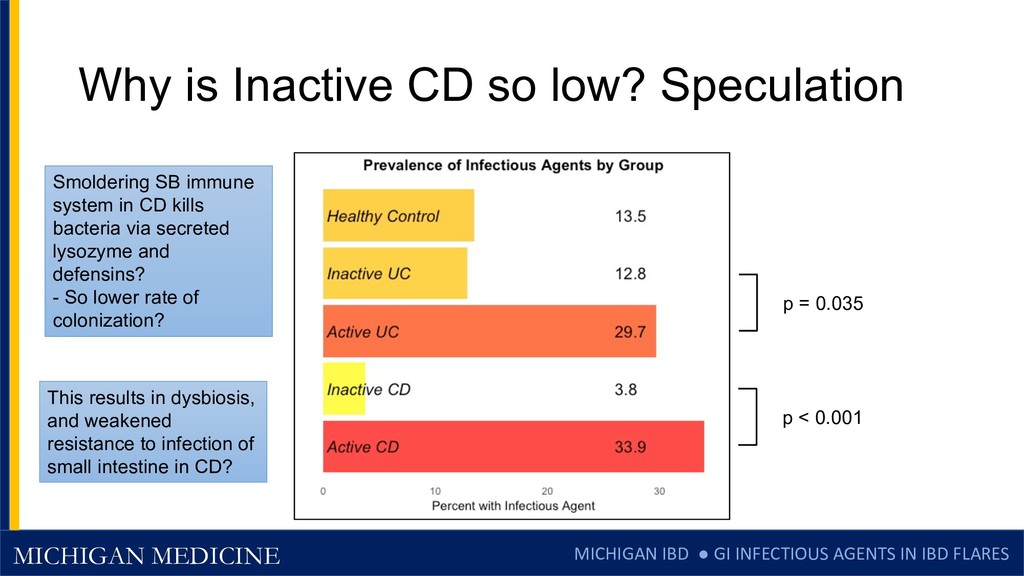
FLARES Why is Inactive CD so low? Speculation p = 0.035 p < 0.001 Smoldering SB immune system in CD kills bacteria via secreted lysozyme and defensins? - So lower rate of colonization? This results in dysbiosis, and weakened resistance to infection of small intestine in CD?
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}