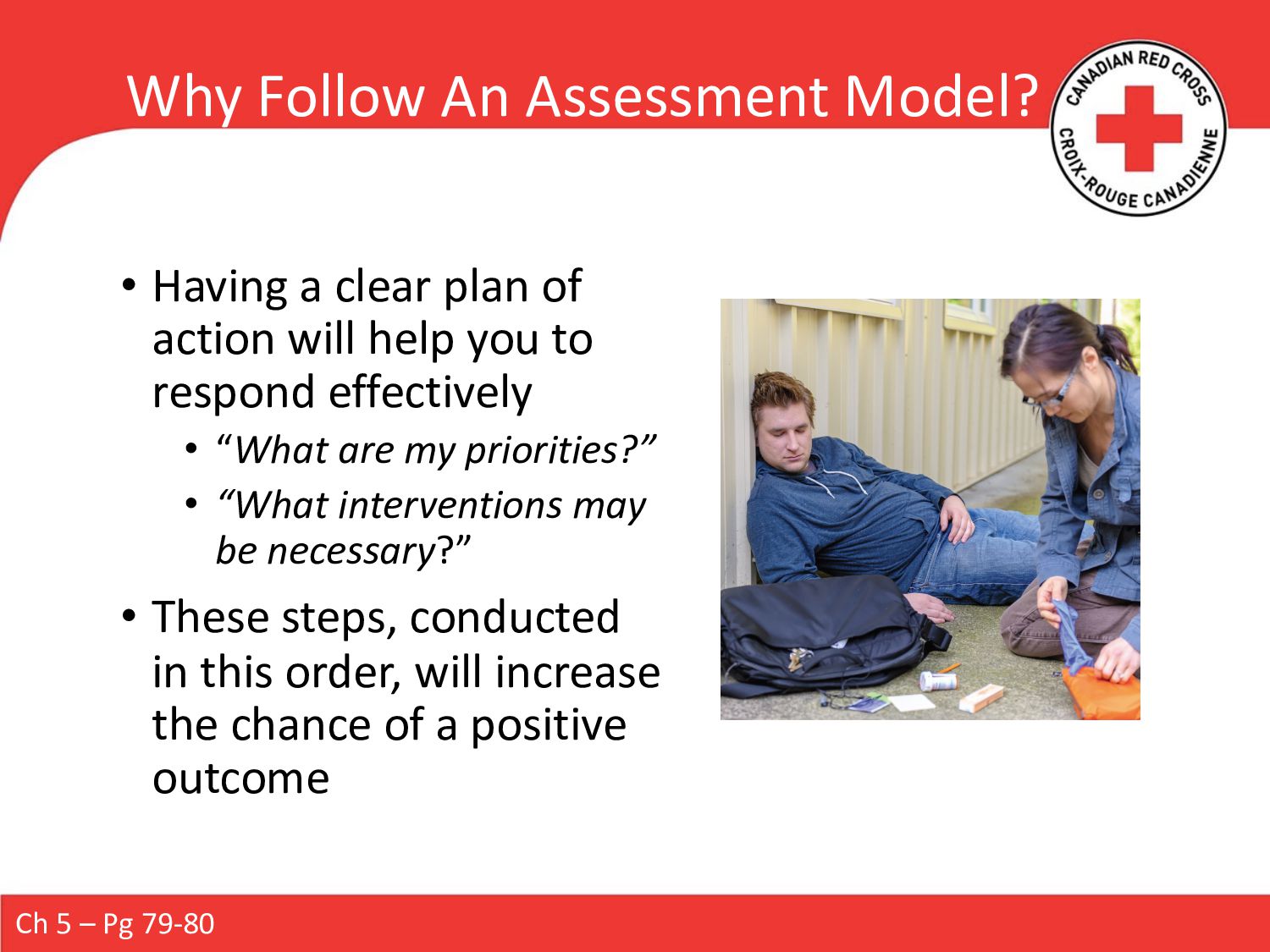
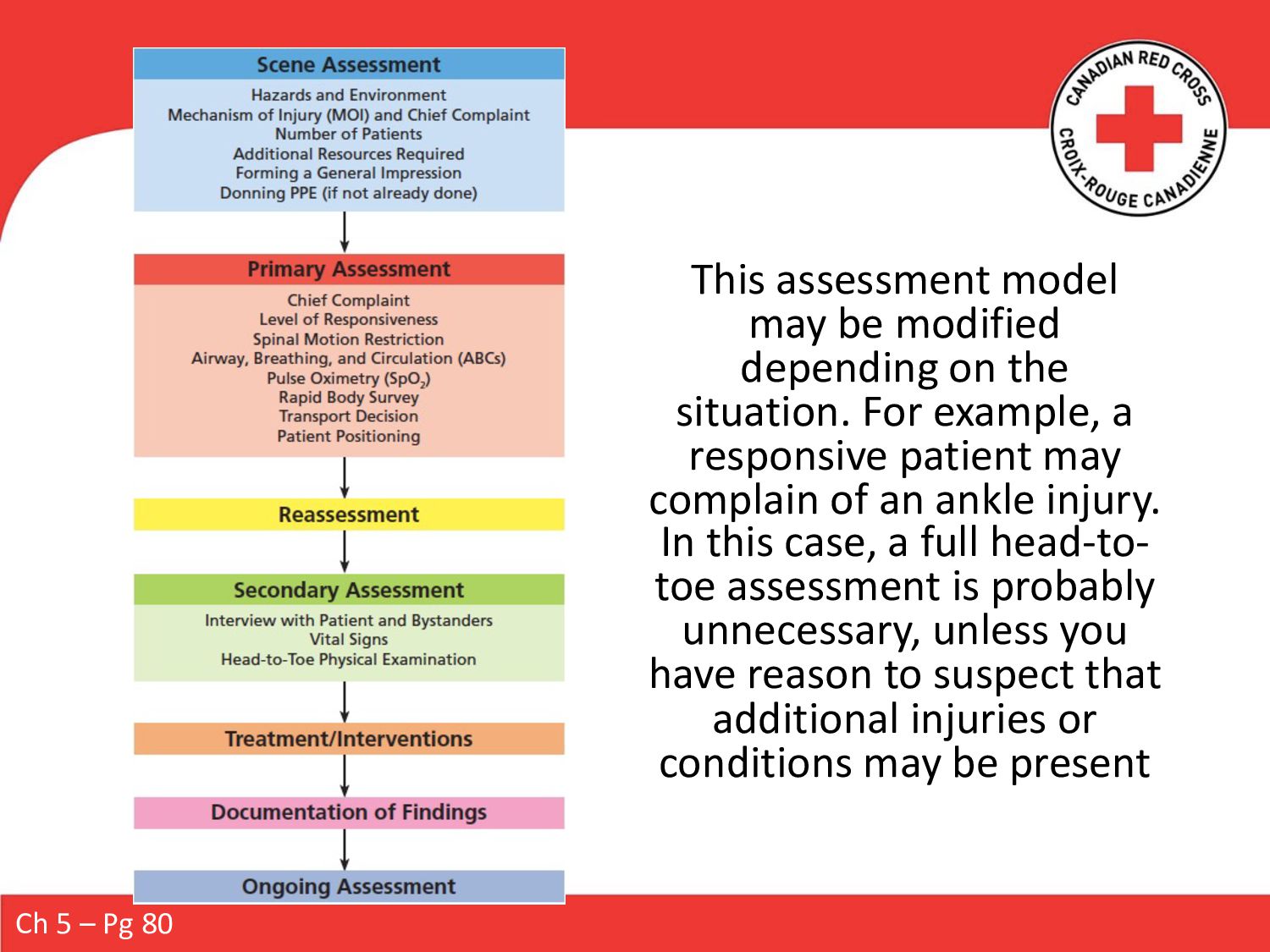
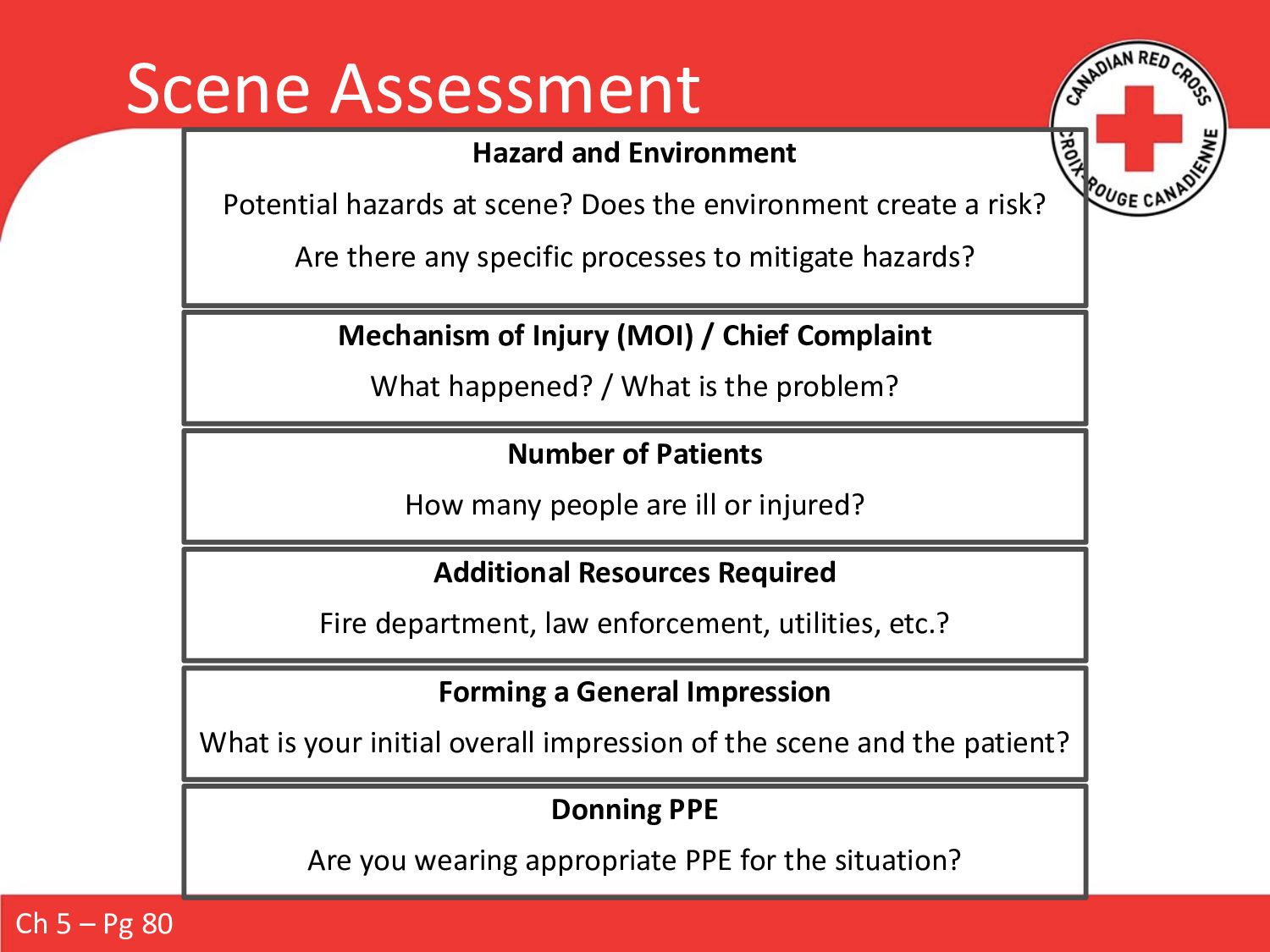
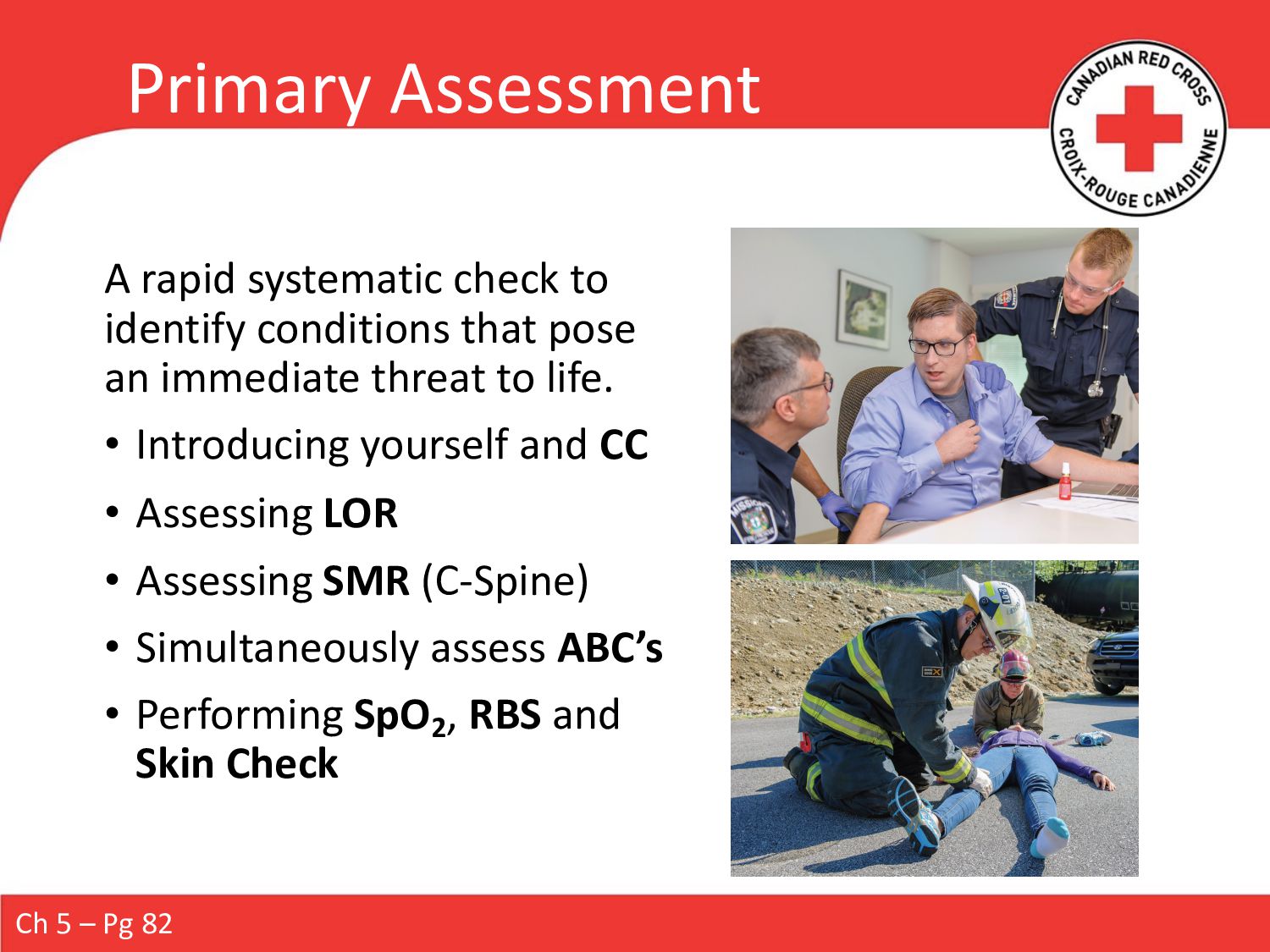
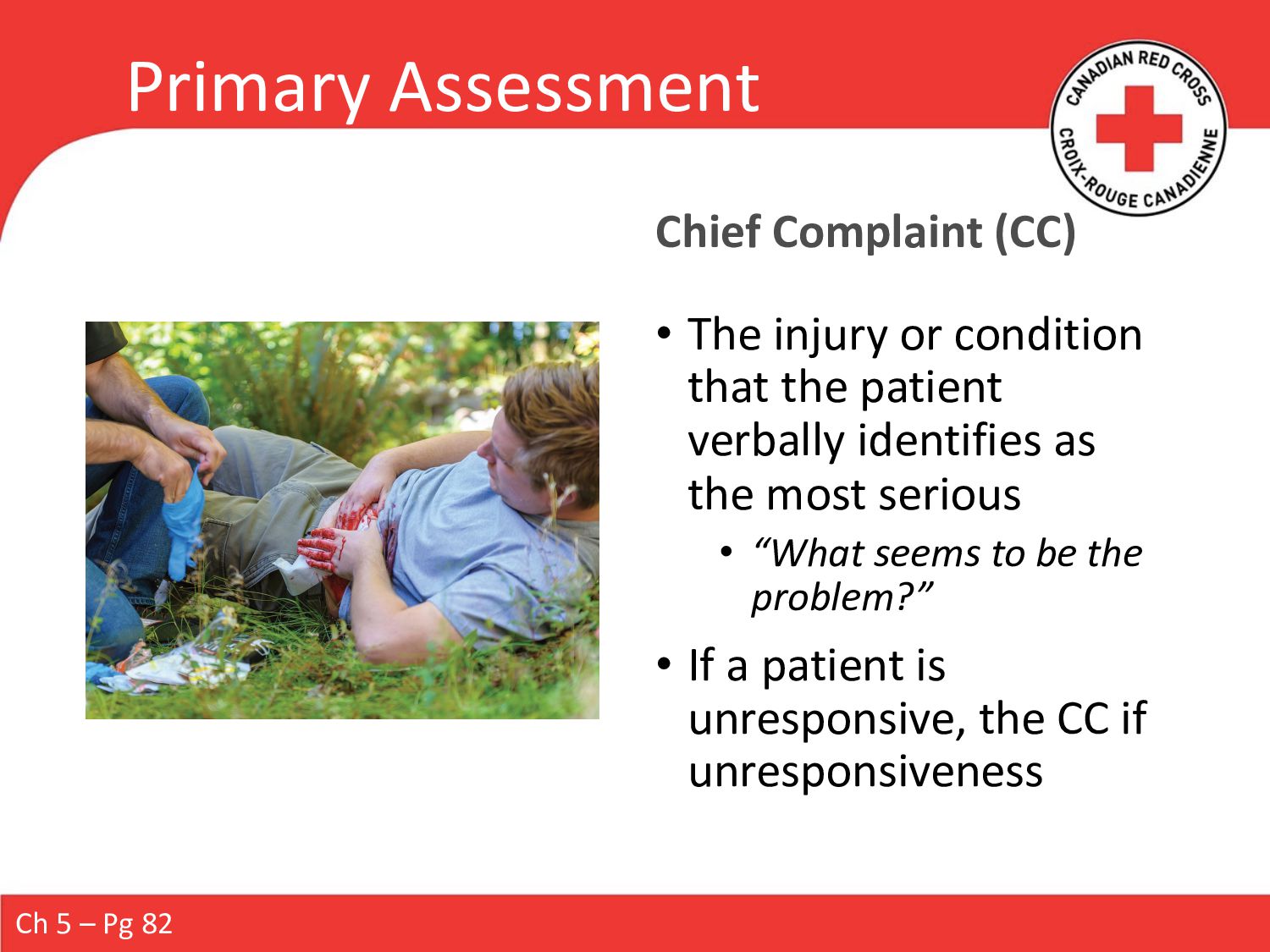
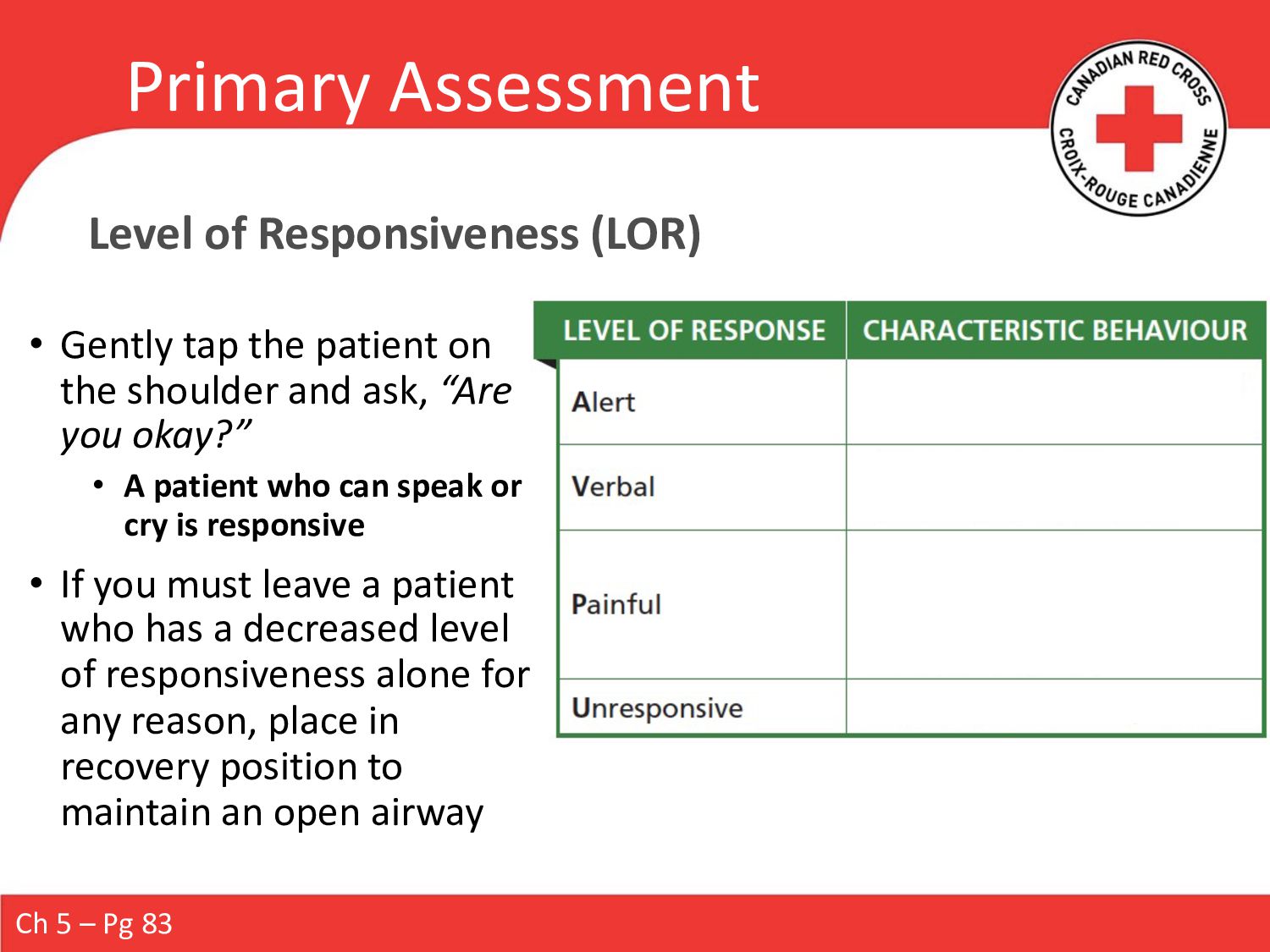
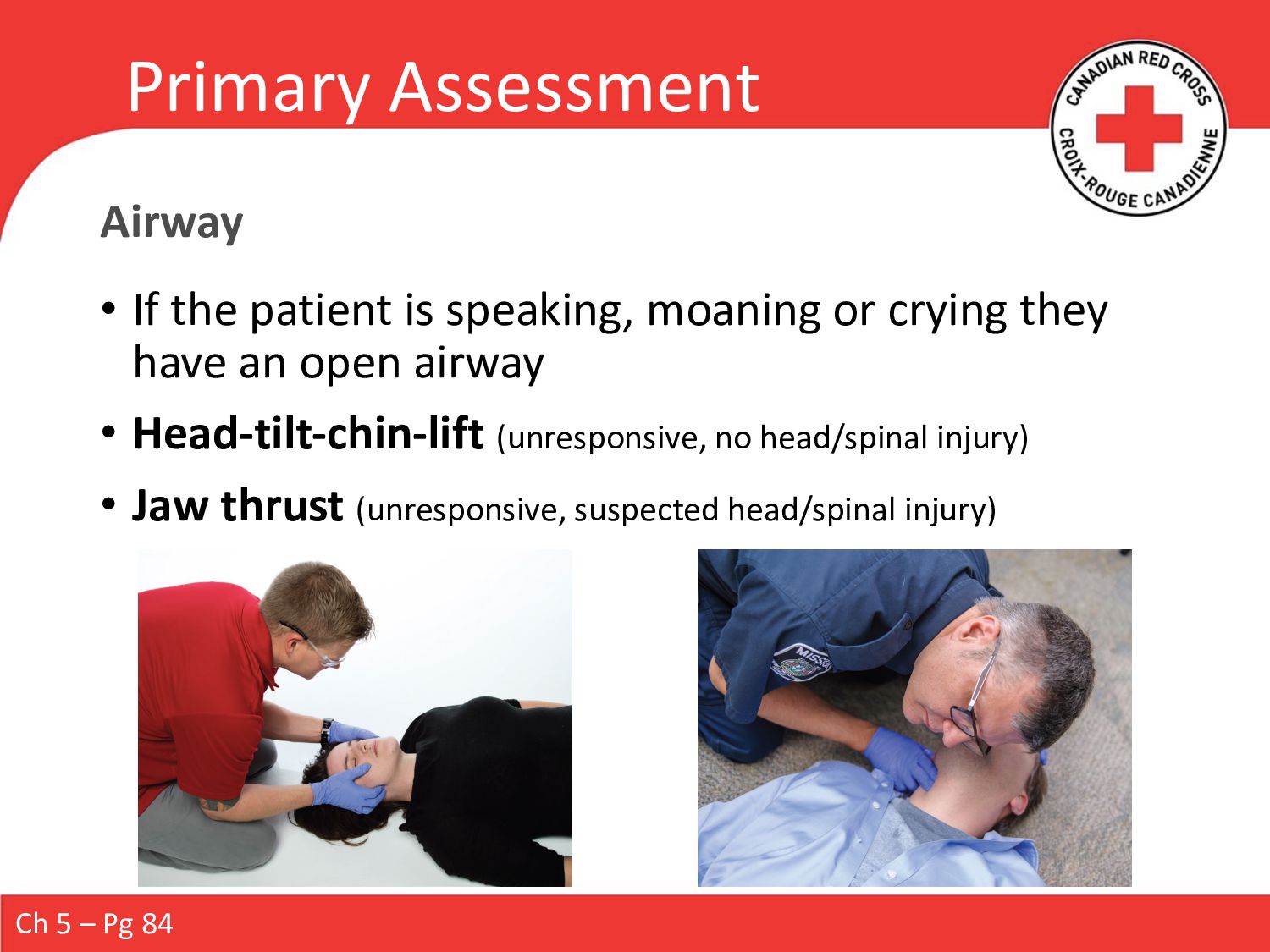
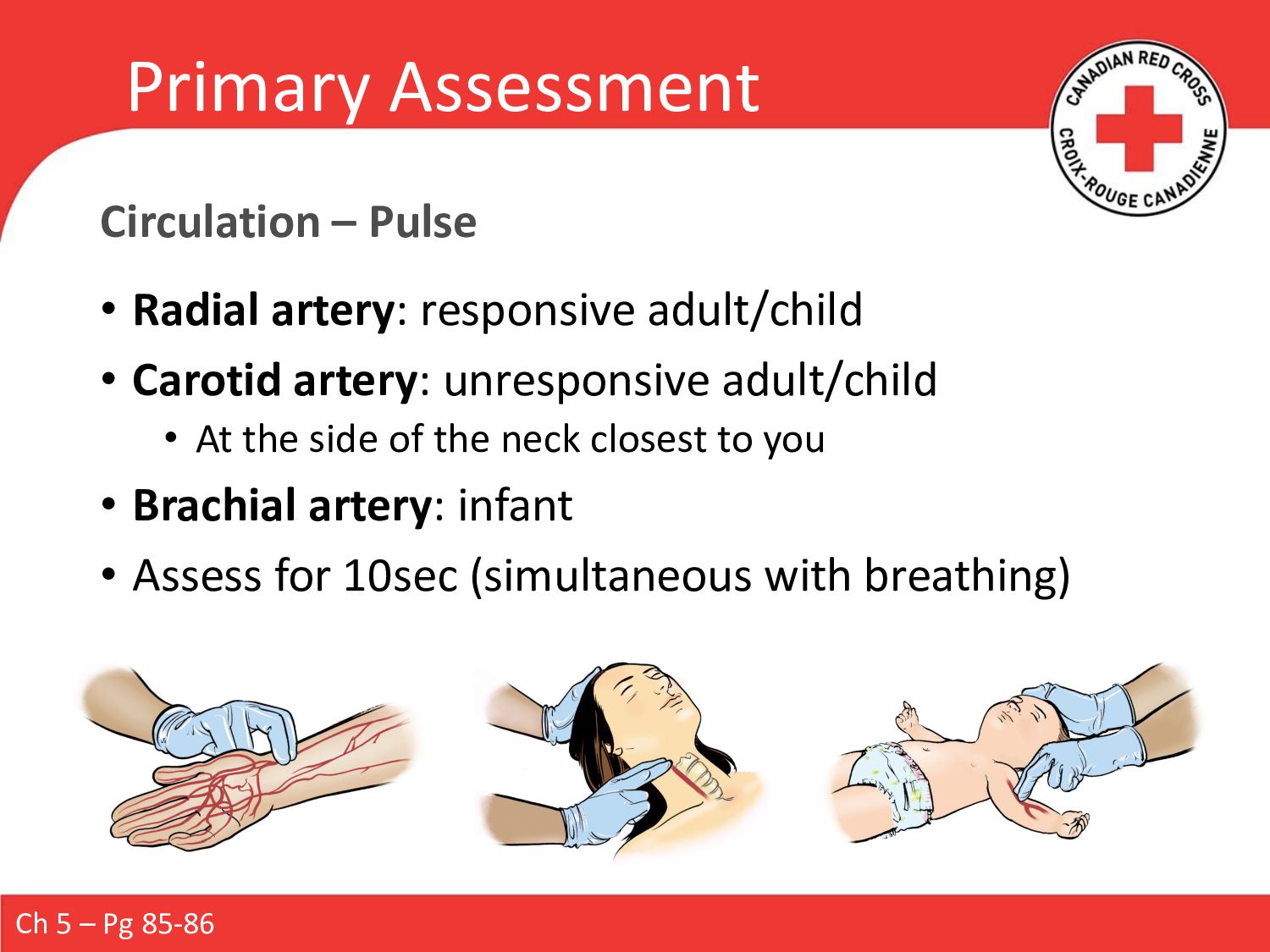
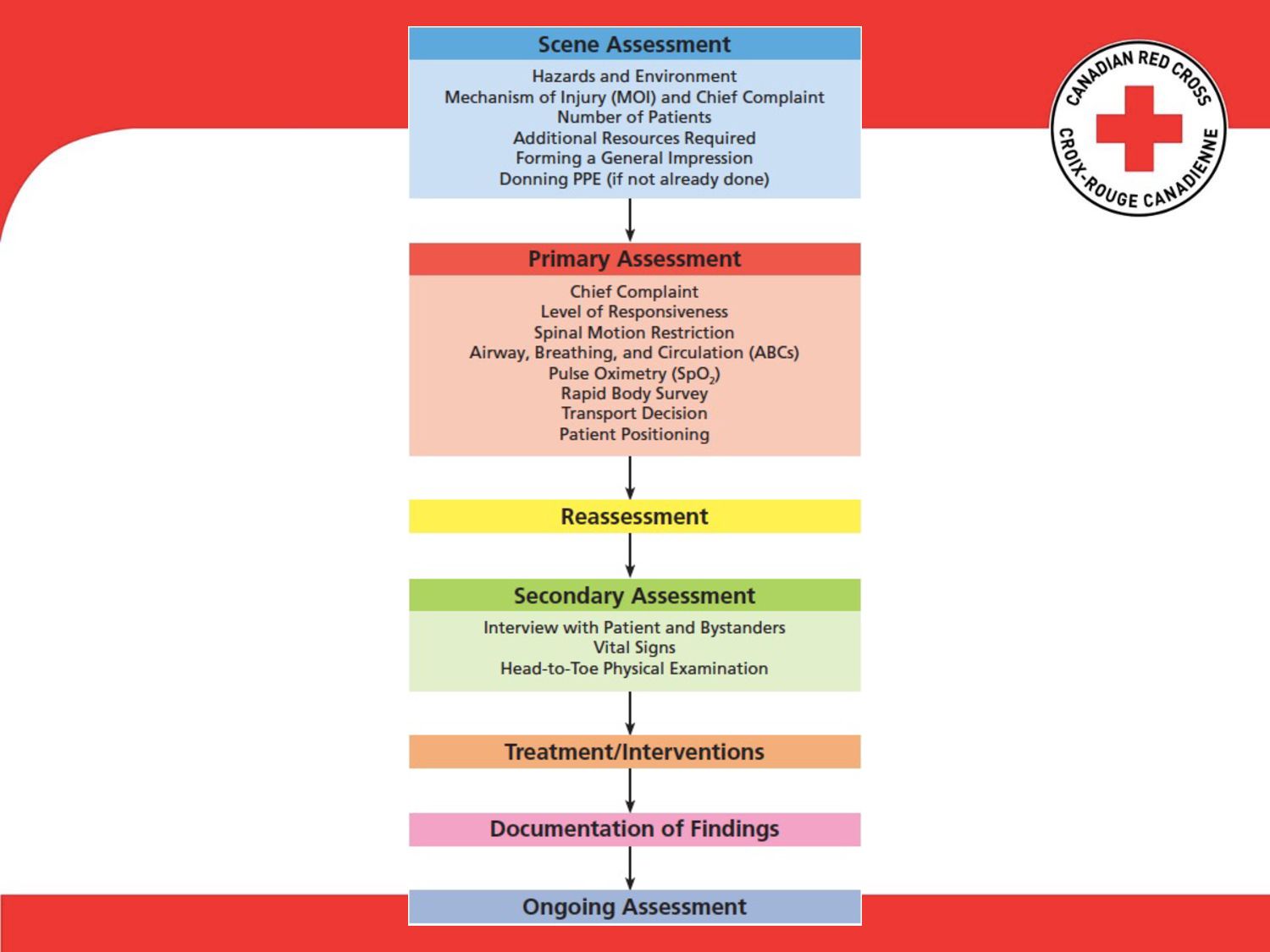
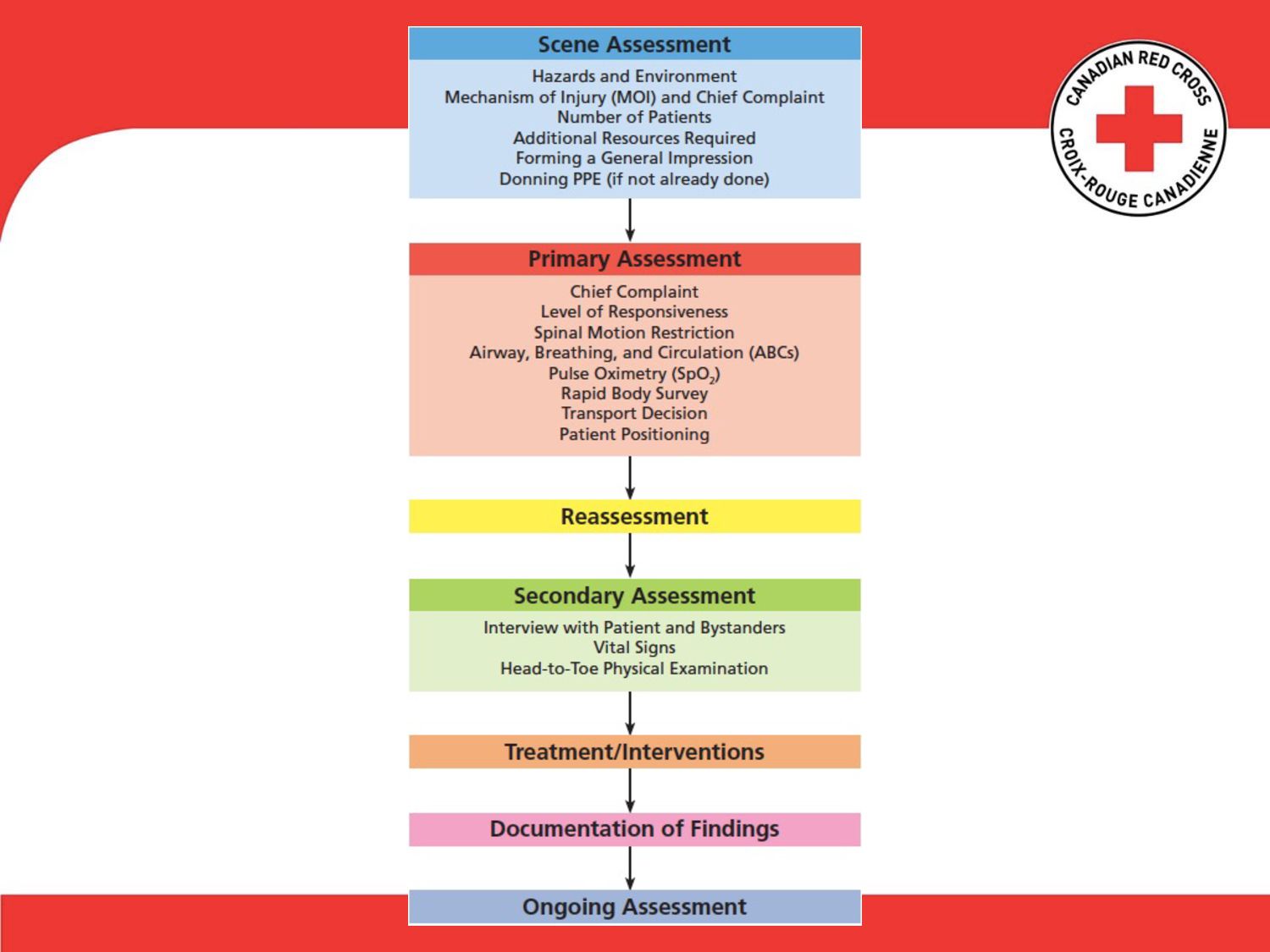
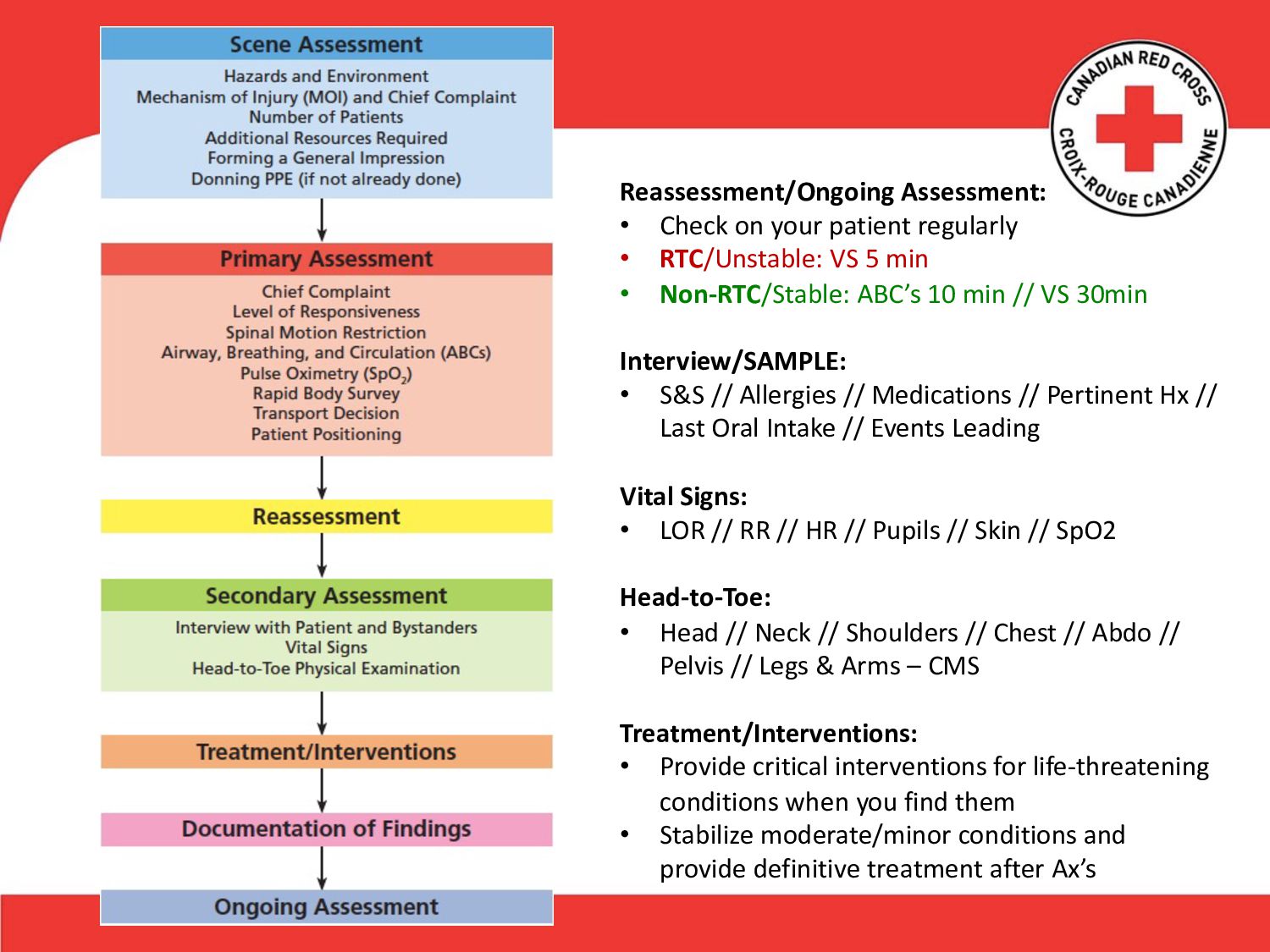
When you arrive at the scene of an emergency, after ensuring the safety of yourself and others, you must quickly determine whether the patient has any life-threatening injuries or conditions by conducting a primary assessment. This includes assessing the patient’s level of responsiveness and his or her airway, breathing, and circulation. Once the primary assessment is complete, you can begin your secondary assessment, which includes interviewing the patient (or bystanders), assessing and documenting vital signs, and conducting a thorough physical exam. Having a clear plan of action will help you to respond effectively in any emergency situation. The important questions are “What are my priorities?” and “What interventions may be necessary?” The general steps in this section will provide answers to these questions (Figure 5–1).
These steps, conducted in this order, help to ensure your safety and that of the patient and bystanders. They will also increase the patient’s chance of a positive outcome.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}