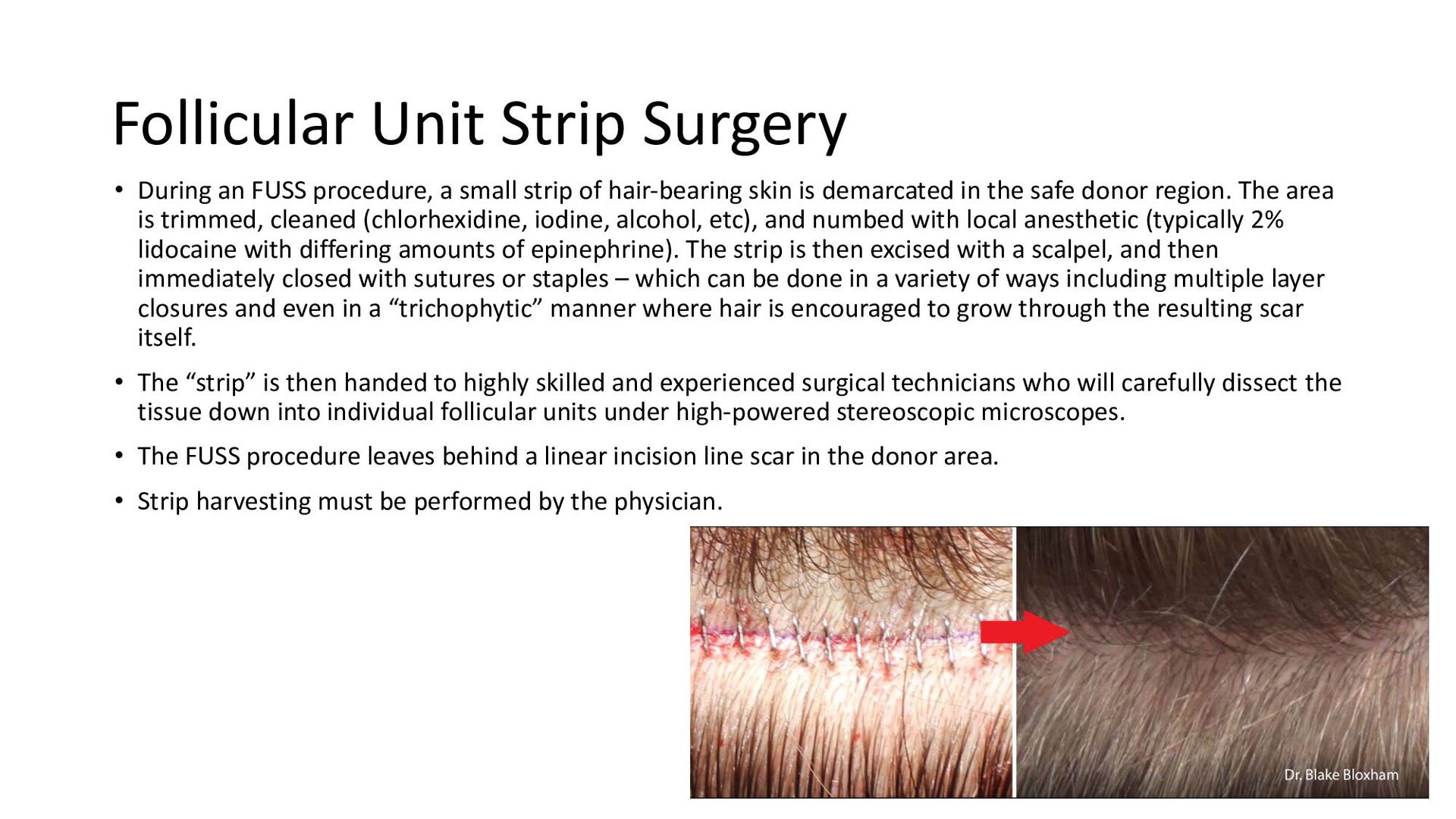
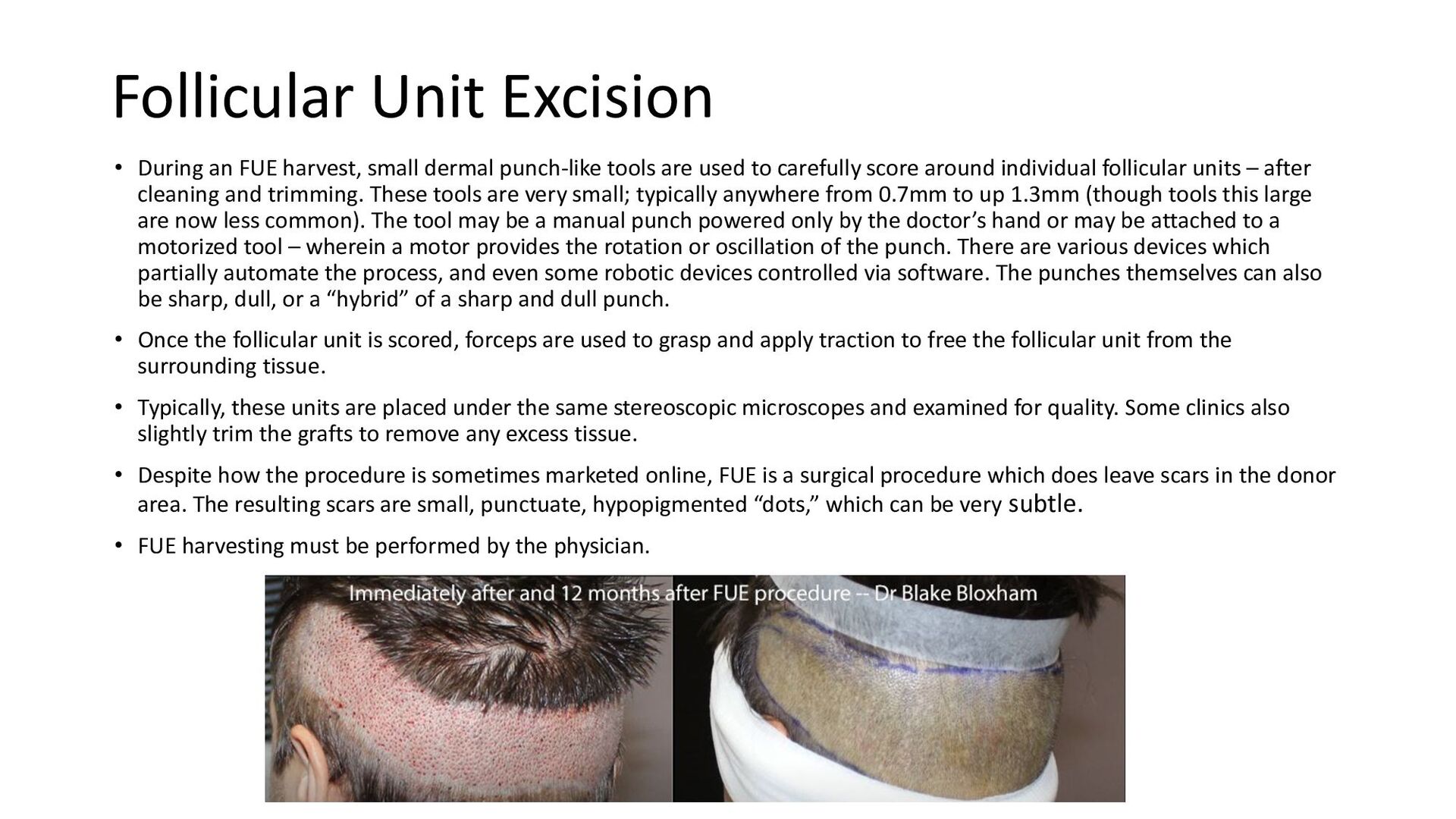
Feller & Bloxham Philadelphia uses the latest techniques and technologies to perform hair transplants. Our modern hair transplant techniques include both FUE (follicular unit extraction) and FUT (follicular unit transplant). With FUE, individual hair follicles are extracted from the donor area and transplanted into the recipient area, resulting in natural-looking, permanent results. With FUT, a strip of skin is removed from the donor area and divided into individual follicles for transplantation. Learn more about the differences between FUE and FUT on our website. Schedule your consultation today and get the look you've always wanted!
URL : https://philadelphiahairtransplant.com/hair-transplant
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}