Presented at 2015 OSEHRA Summit.
Background:
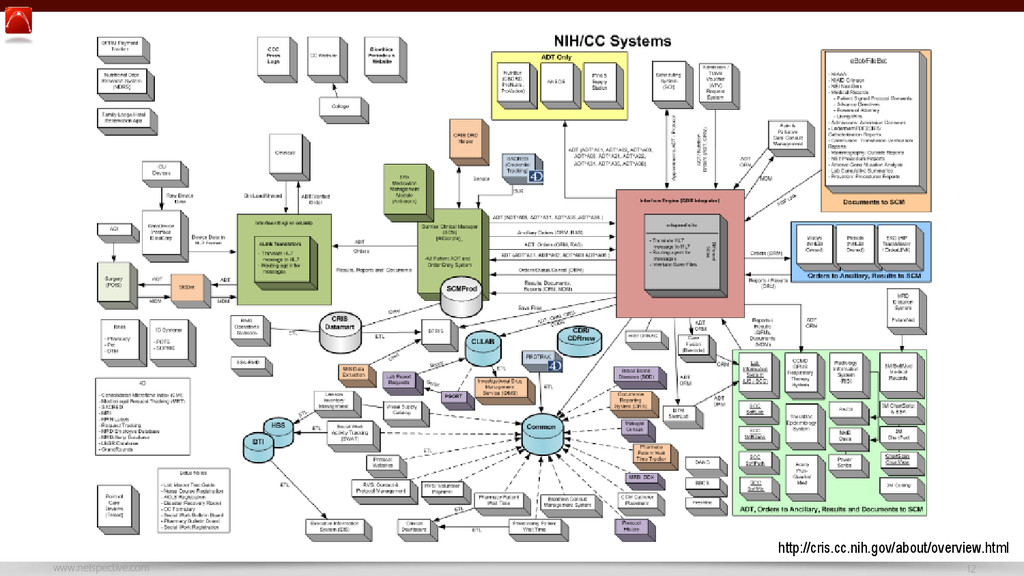
* Many enterprise apps are being built these days, most are designed to work as a stand alone system similar to consumer apps
* Healthcare-specific software engineering and integration tools are going to do more harm than good (industry-neutral is better).
Takeaways:
* Any enterprise app which acts like a consumer app that doesn’t integrate well into hospital or ambulatory systems and workflows is doomed
* There’s nothing unique about health IT data that justifies complex, expensive, or special technology.
* There’s a lot unique about healthcare workflows that require common technologies to be adapted properly.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
![Thank You Visit http://www.netspective.com http://www.healthcareguy.com E-mail [email protected] Follow @ShahidNShah Call](https://files.speakerdeck.com/presentations/57931b939f664b9c92bd4320a3cbe2f5/slide_31.jpg){kind=link}