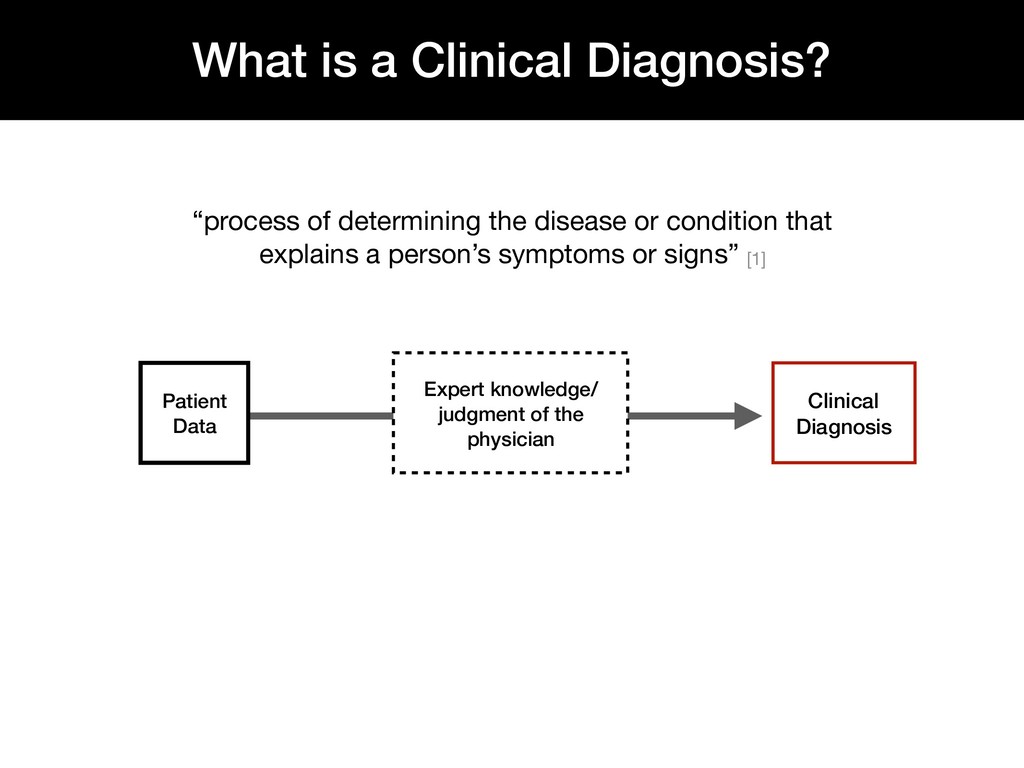
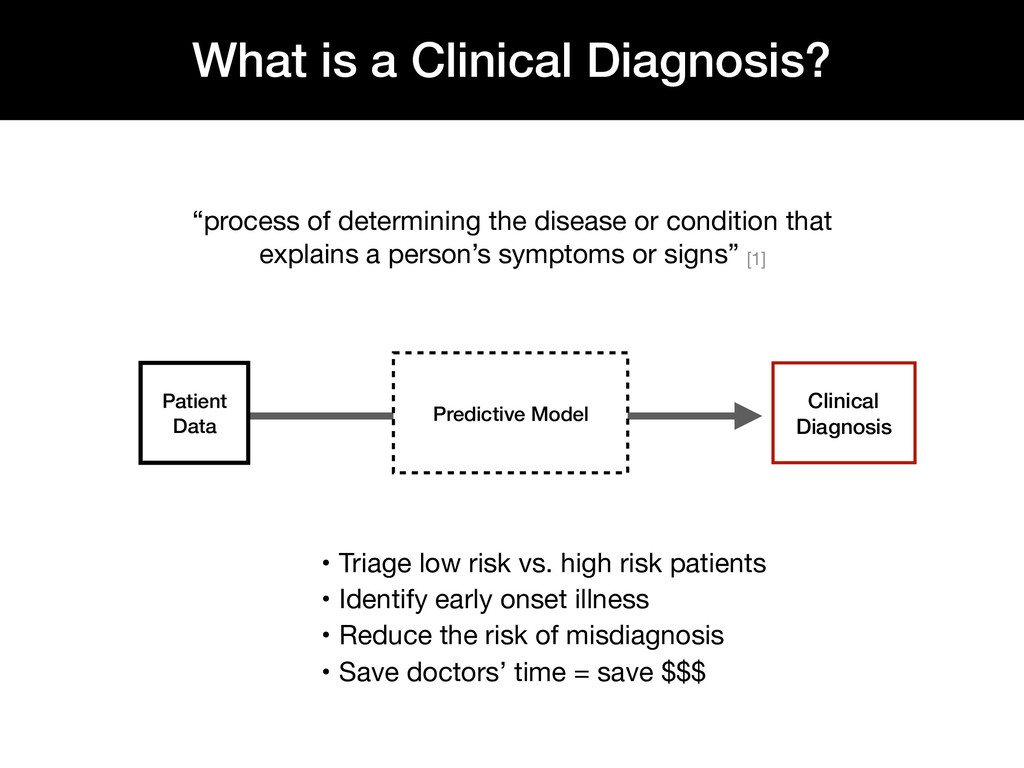
Diagnosis • Triage low risk vs. high risk patients • Identify early onset illness • Reduce the risk of misdiagnosis • Save doctors’ time = save $$$ “process of determining the disease or condition that explains a person’s symptoms or signs” [1]
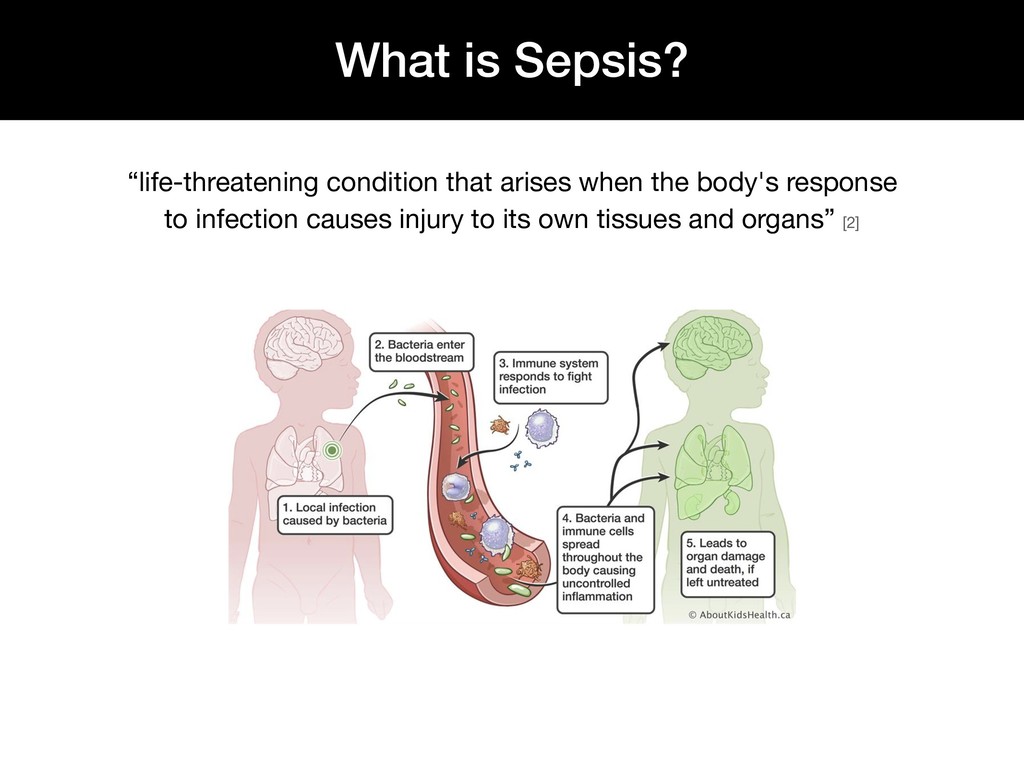
worldwide each year • Leading cause of death in the Intensive Care Unit (ICU) [3] • Responsible for 1 out of 3 hospital deaths [3] • Costs $20.3 billion each year in U.S. hospitals [4] • Every hour that passes before treatment begins, a patient’s risk of death from sepsis increased by 4-8% [5]
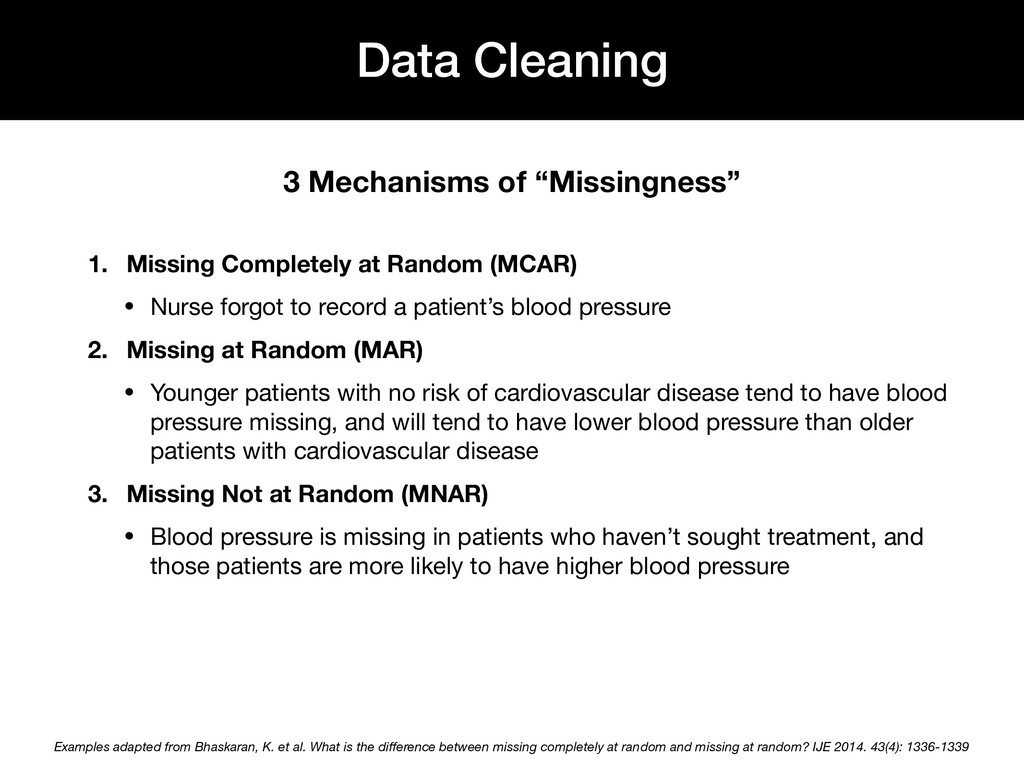
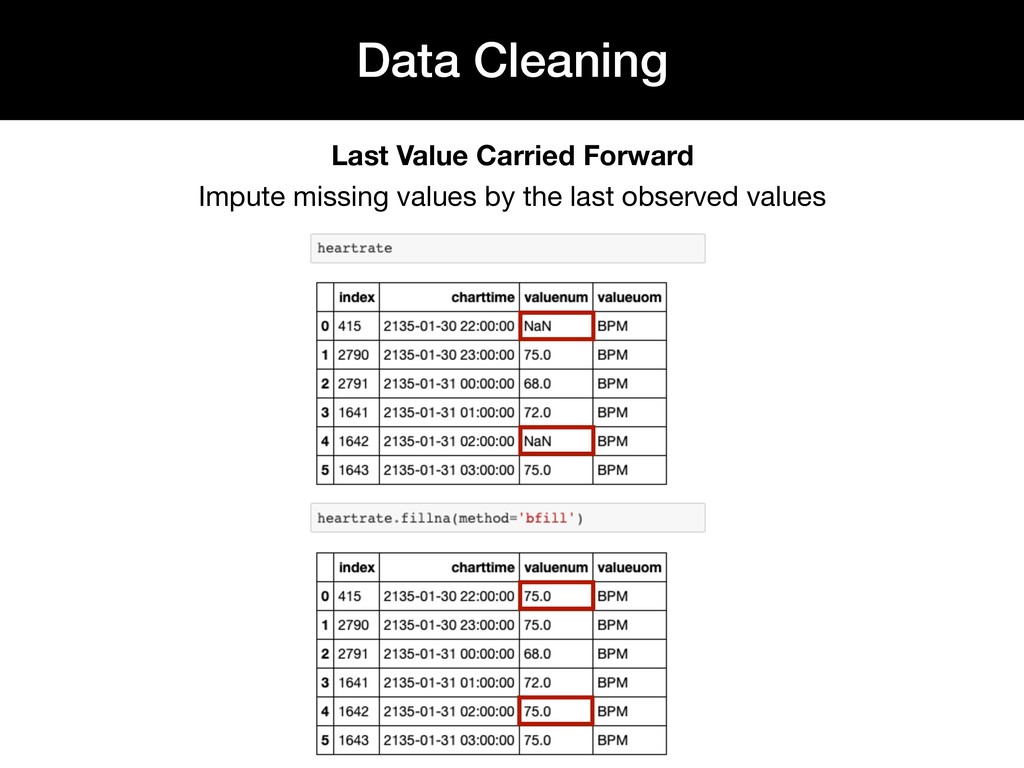
record a patient’s blood pressure 2. Missing at Random (MAR) • Younger patients with no risk of cardiovascular disease tend to have blood pressure missing, and will tend to have lower blood pressure than older patients with cardiovascular disease 3. Missing Not at Random (MNAR) • Blood pressure is missing in patients who haven’t sought treatment, and those patients are more likely to have higher blood pressure Data Cleaning 3 Mechanisms of “Missingness” Examples adapted from Bhaskaran, K. et al. What is the difference between missing completely at random and missing at random? IJE 2014. 43(4): 1336-1339
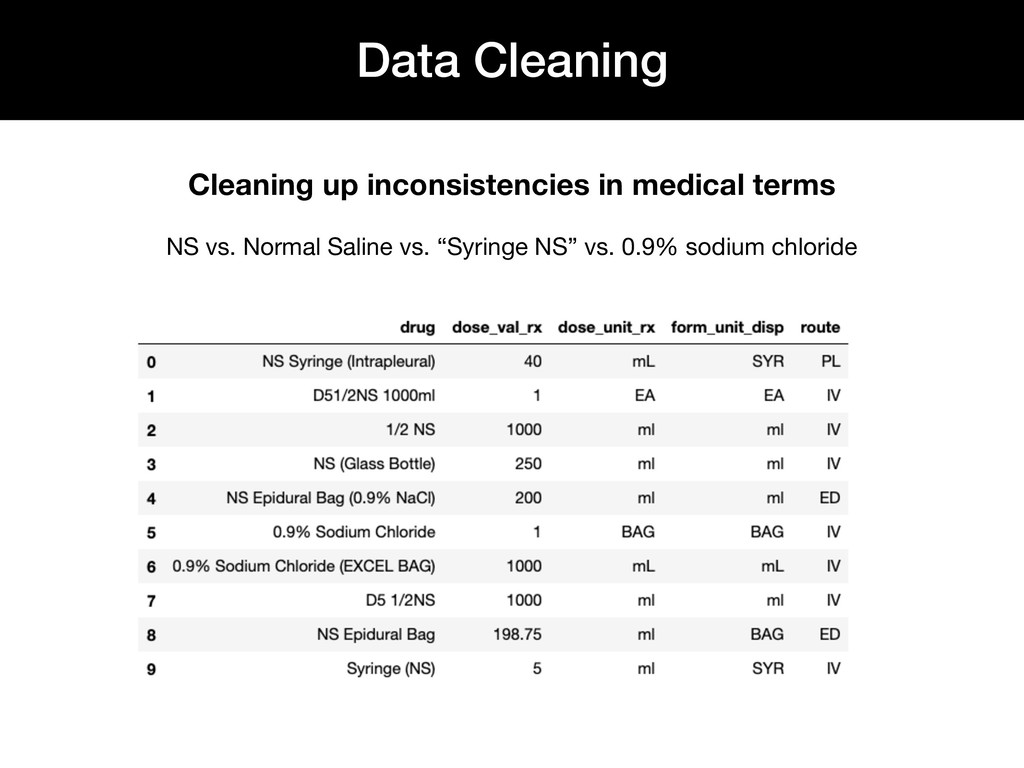
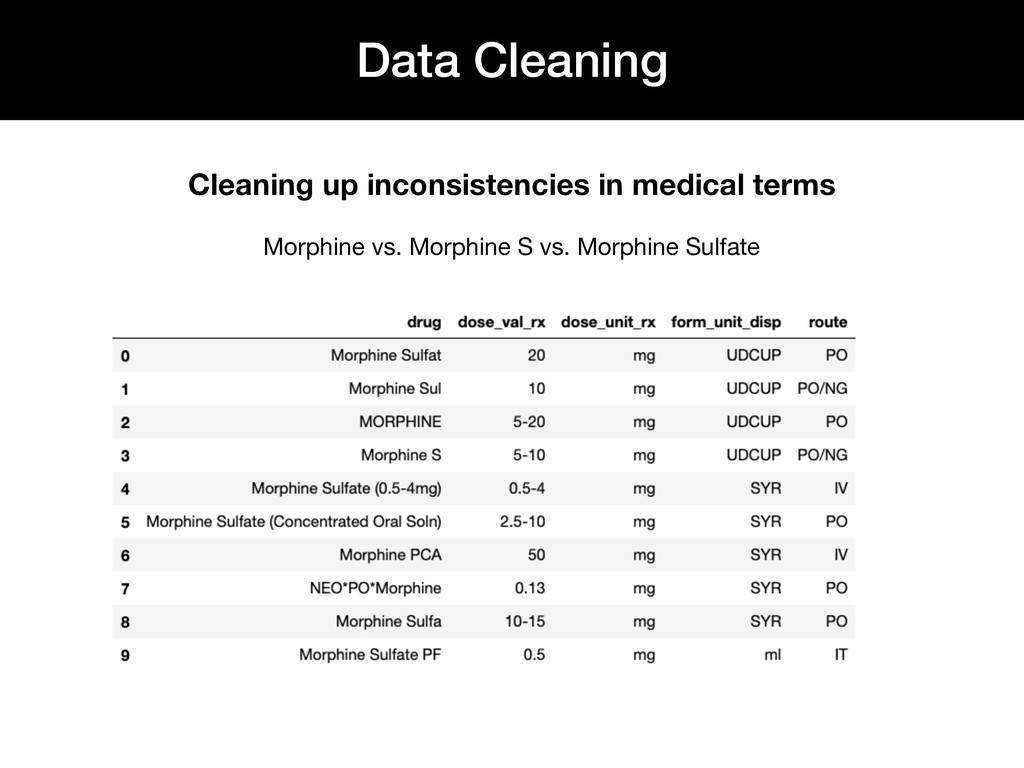
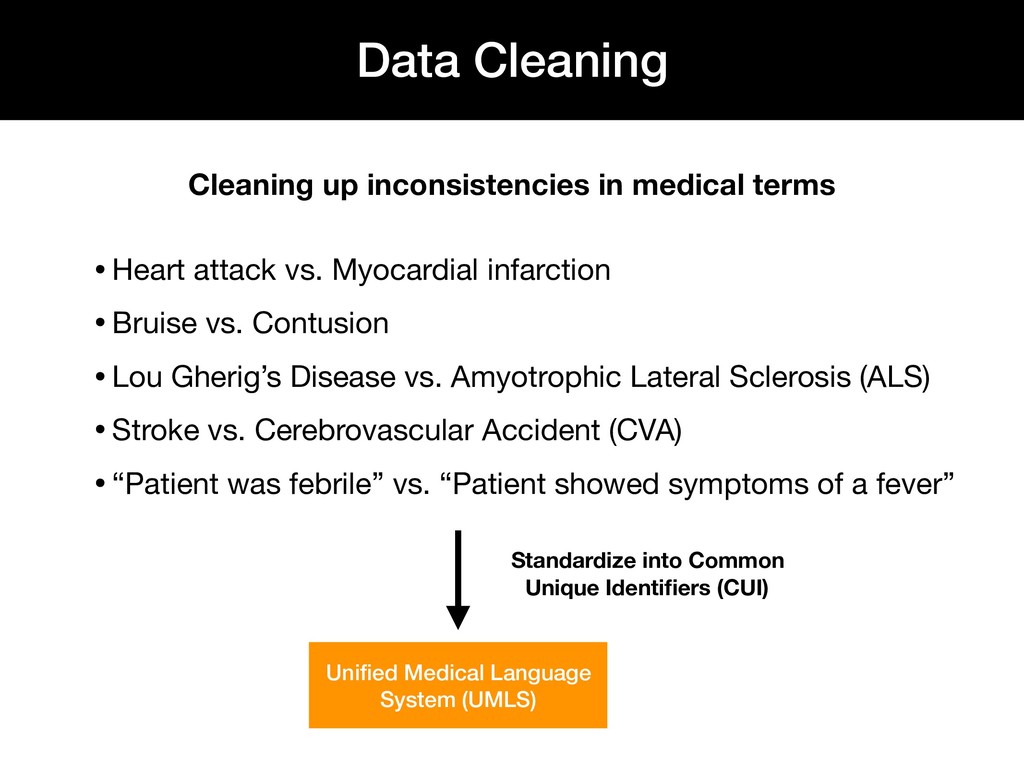
vs. Myocardial infarction •Bruise vs. Contusion •Lou Gherig’s Disease vs. Amyotrophic Lateral Sclerosis (ALS) •Stroke vs. Cerebrovascular Accident (CVA) •“Patient was febrile” vs. “Patient showed symptoms of a fever” Standardize into Common Unique Identifiers (CUI) Unified Medical Language System (UMLS)
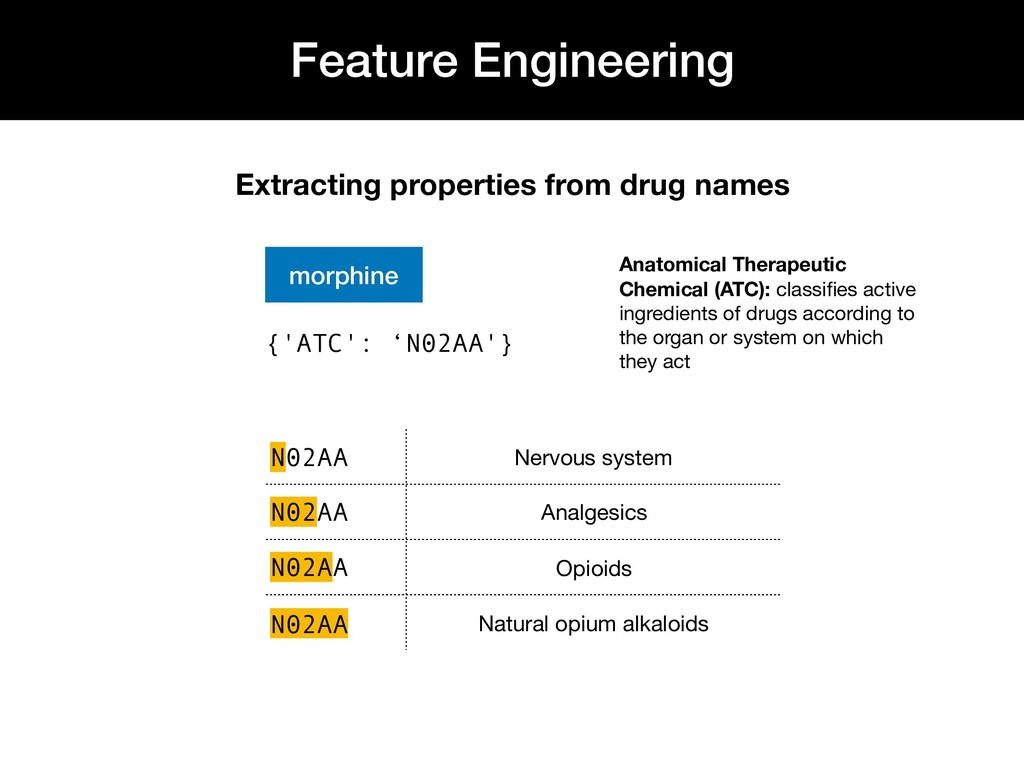
Chemical (ATC): classifies active ingredients of drugs according to the organ or system on which they act N02AA Nervous system N02AA Analgesics N02AA Opioids N02AA Natural opium alkaloids {'ATC': ‘N02AA'}
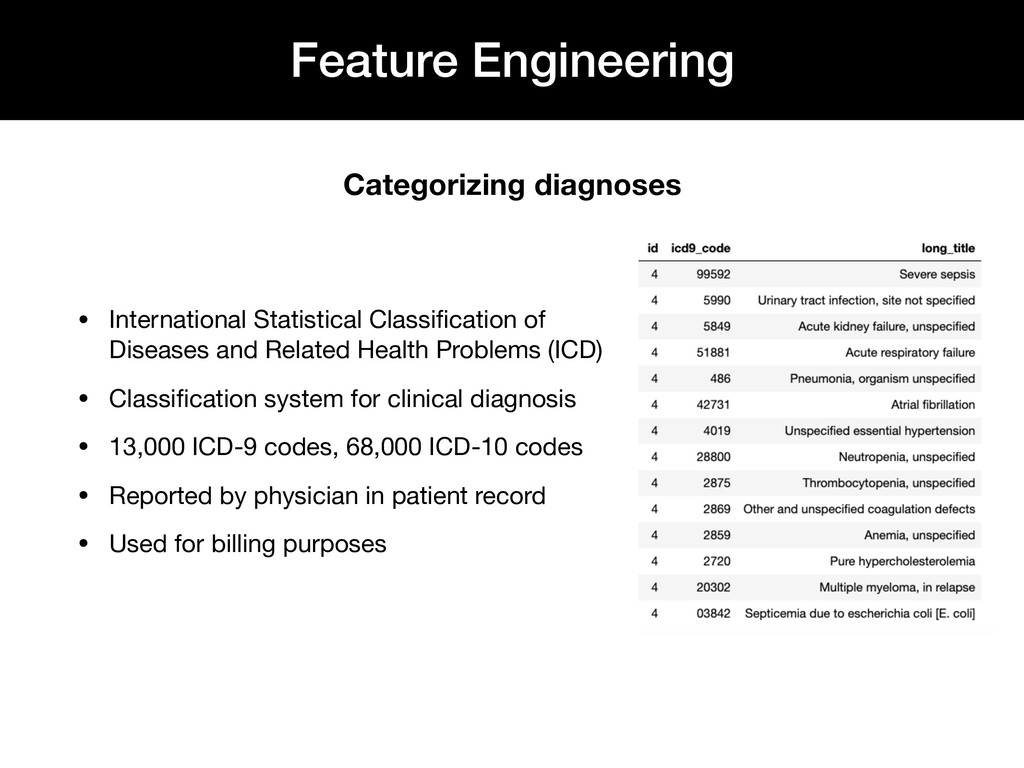
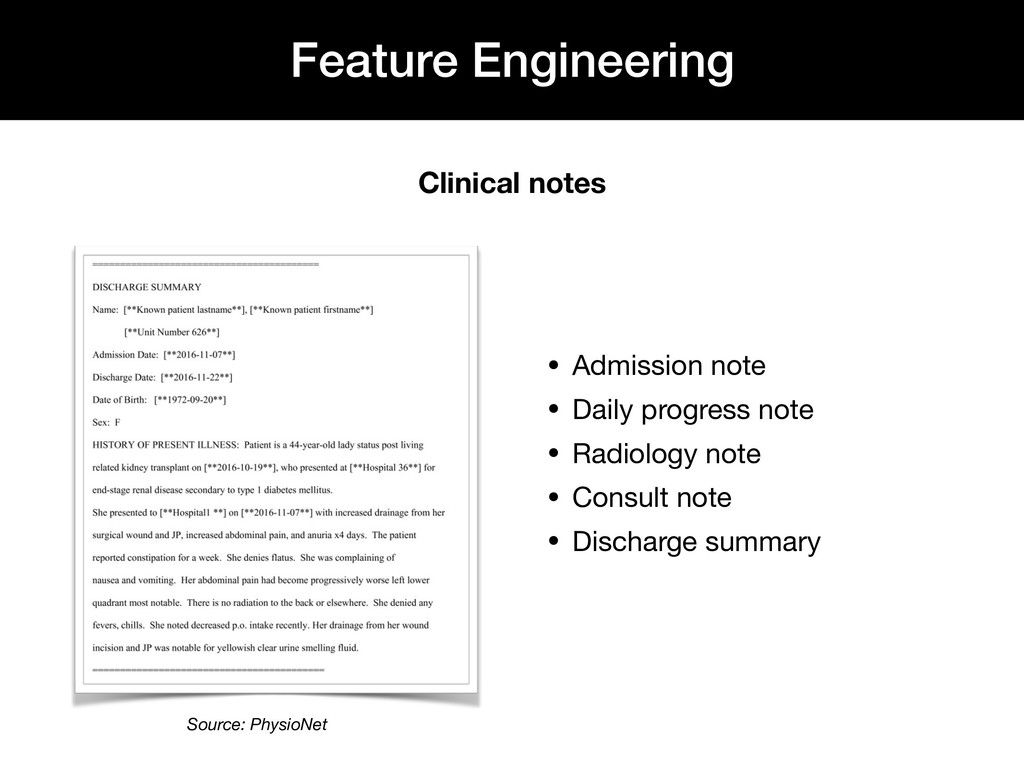
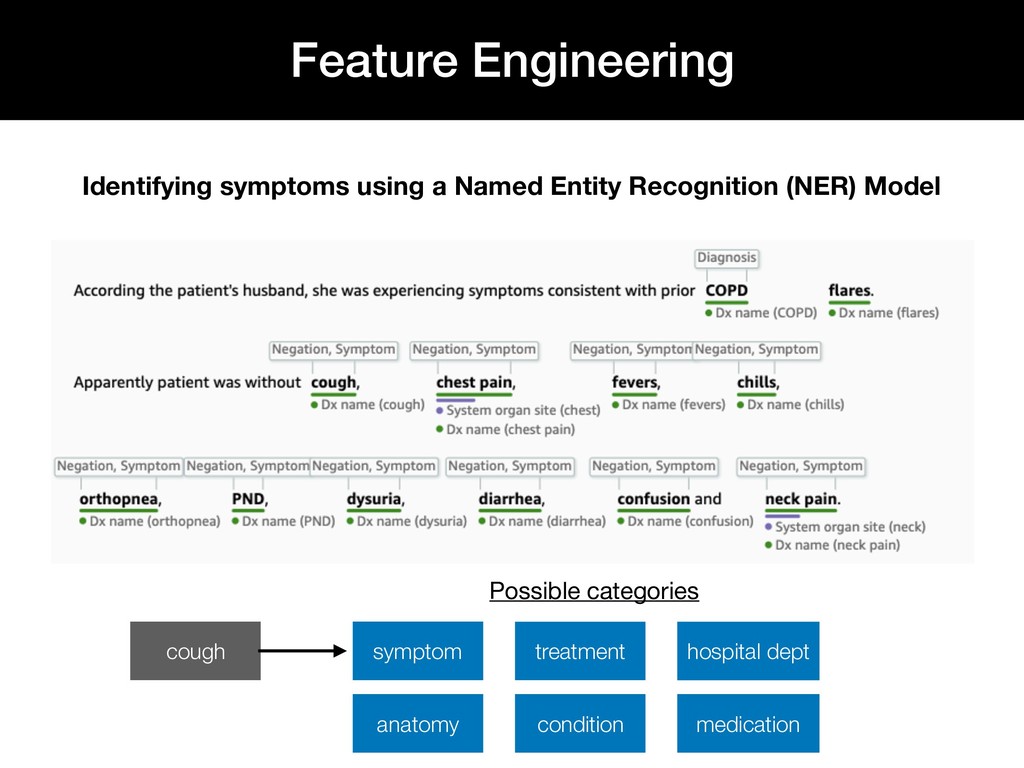
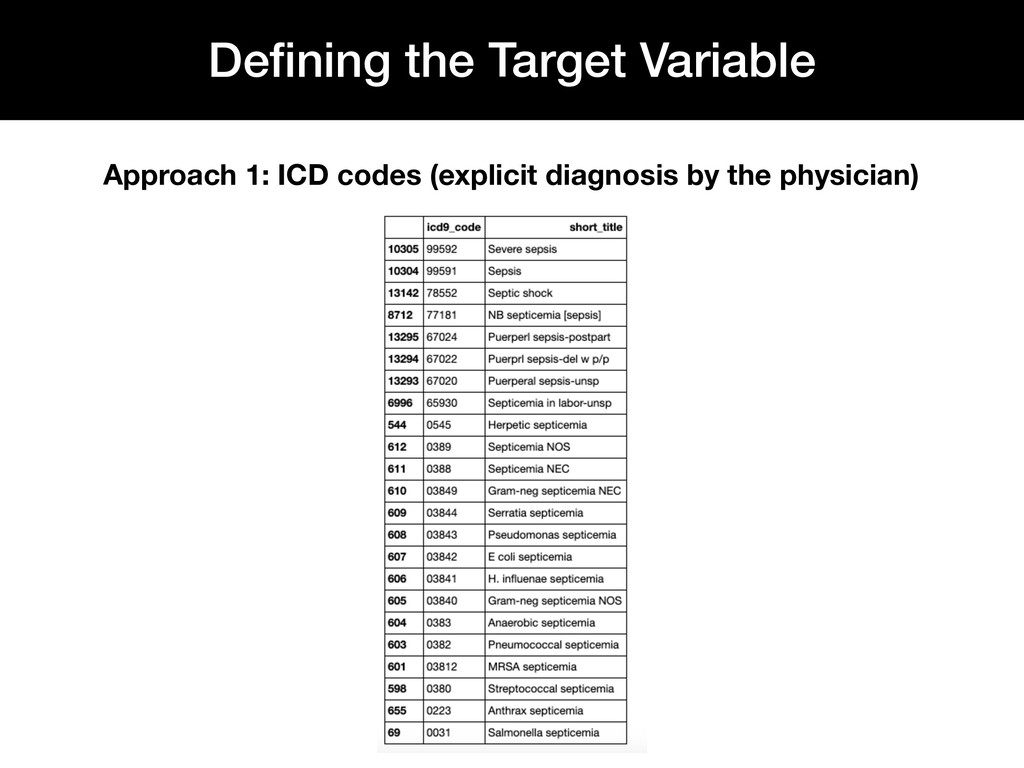
(ICD) • Classification system for clinical diagnosis • 13,000 ICD-9 codes, 68,000 ICD-10 codes • Reported by physician in patient record • Used for billing purposes Feature Engineering Categorizing diagnoses
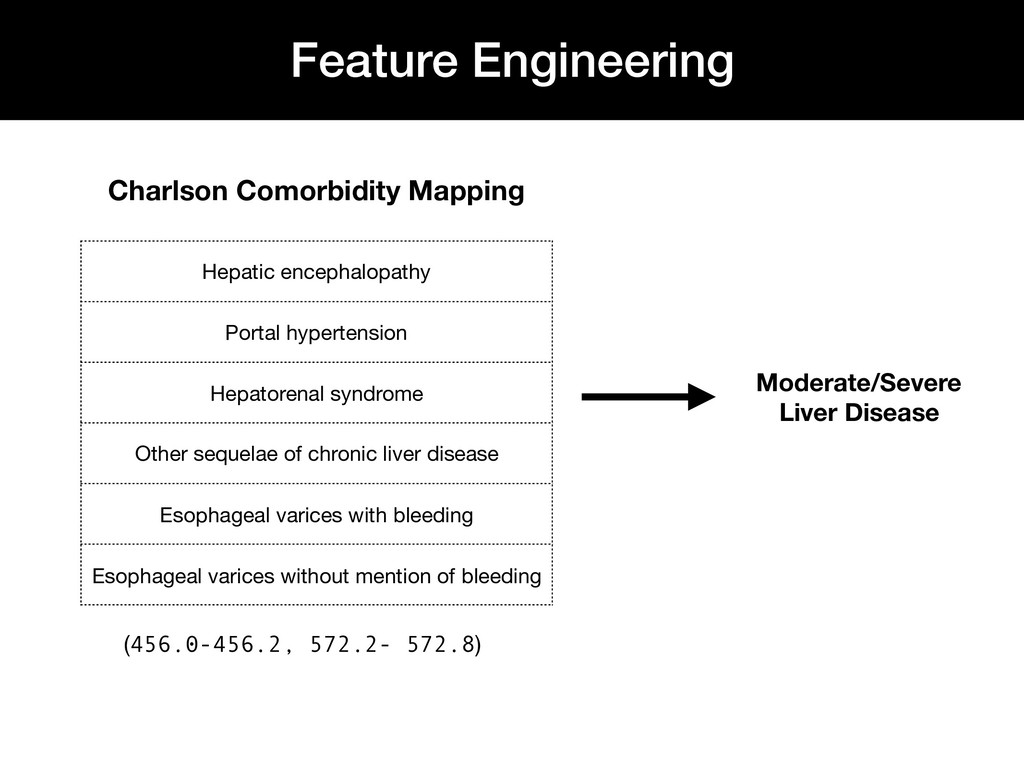
syndrome Other sequelae of chronic liver disease Esophageal varices with bleeding Esophageal varices without mention of bleeding Charlson Comorbidity Mapping (456.0-456.2, 572.2- 572.8)
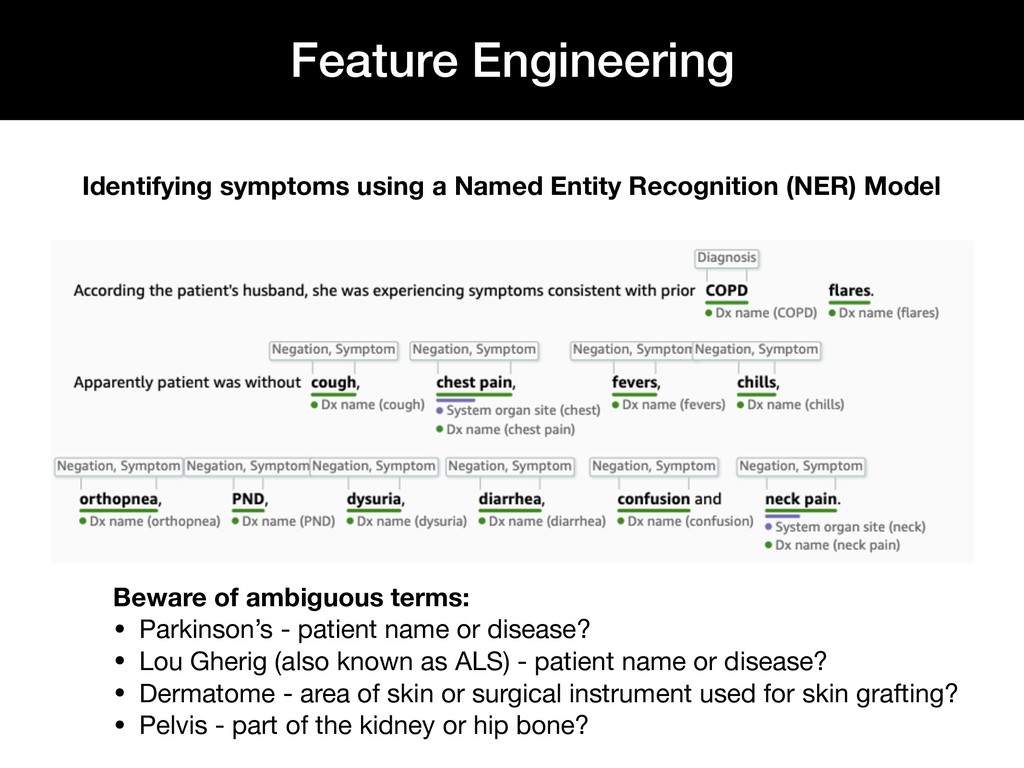
Engineering Beware of ambiguous terms: • Parkinson’s - patient name or disease? • Lou Gherig (also known as ALS) - patient name or disease? • Dermatome - area of skin or surgical instrument used for skin grafting? • Pelvis - part of the kidney or hip bone?
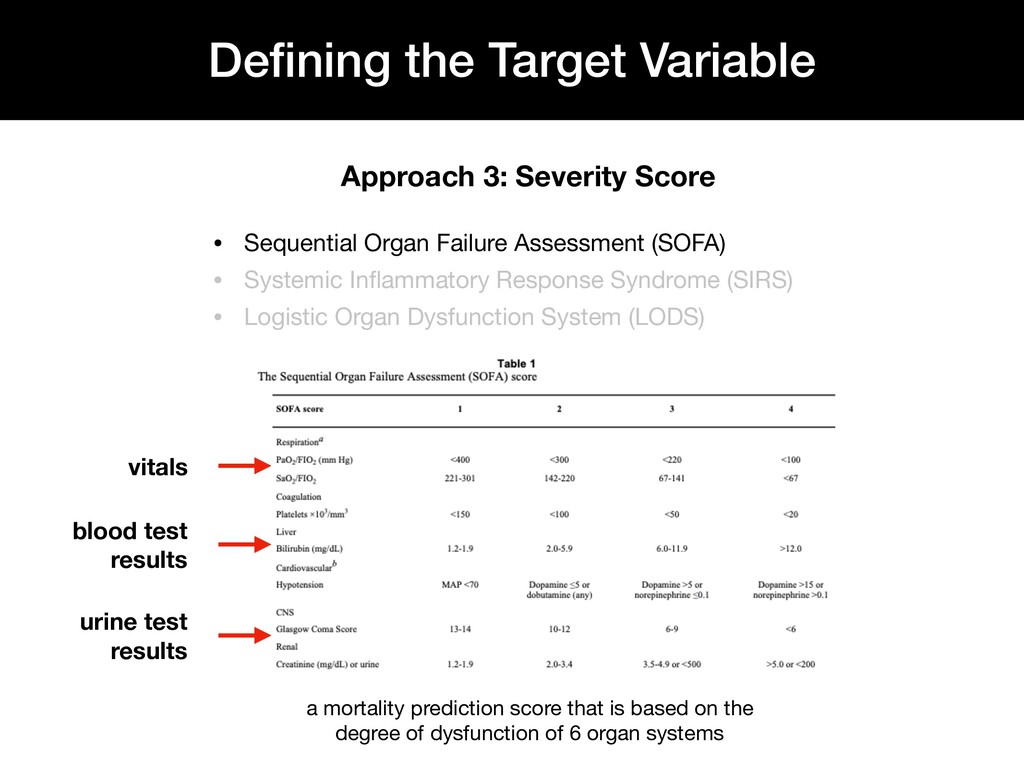
Organ Failure Assessment (SOFA) • Systemic Inflammatory Response Syndrome (SIRS) • Logistic Organ Dysfunction System (LODS) vitals blood test results urine test results a mortality prediction score that is based on the degree of dysfunction of 6 organ systems
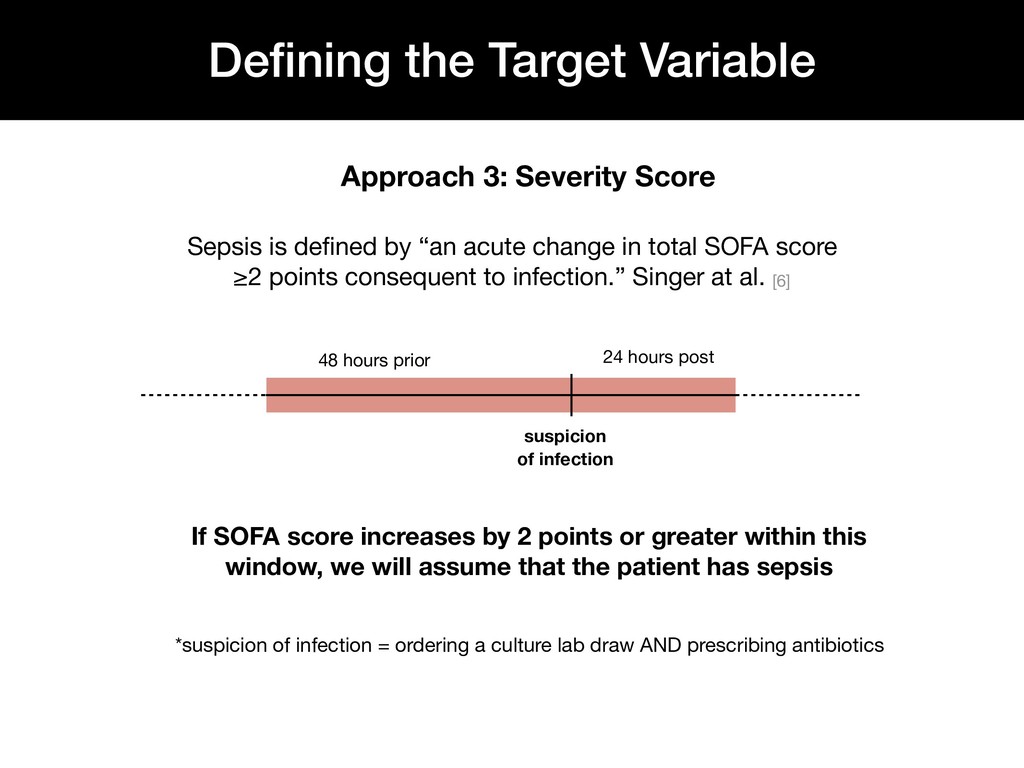
change in total SOFA score ≥2 points consequent to infection.” Singer at al. [6] *suspicion of infection = ordering a culture lab draw AND prescribing antibiotics suspicion of infection 48 hours prior 24 hours post If SOFA score increases by 2 points or greater within this window, we will assume that the patient has sepsis Approach 3: Severity Score
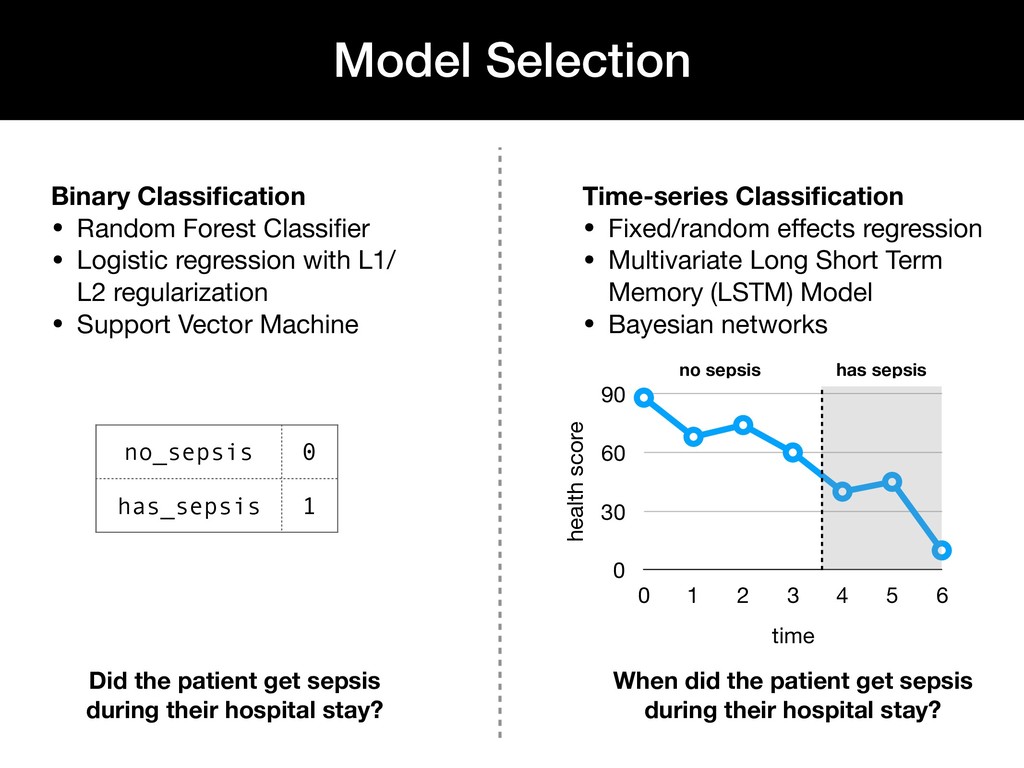
regression with L1/ L2 regularization • Support Vector Machine Time-series Classification • Fixed/random effects regression • Multivariate Long Short Term Memory (LSTM) Model • Bayesian networks no_sepsis 0 has_sepsis 1 health score 0 30 60 90 time 0 1 2 3 4 5 6 no sepsis has sepsis Did the patient get sepsis during their hospital stay? When did the patient get sepsis during their hospital stay?
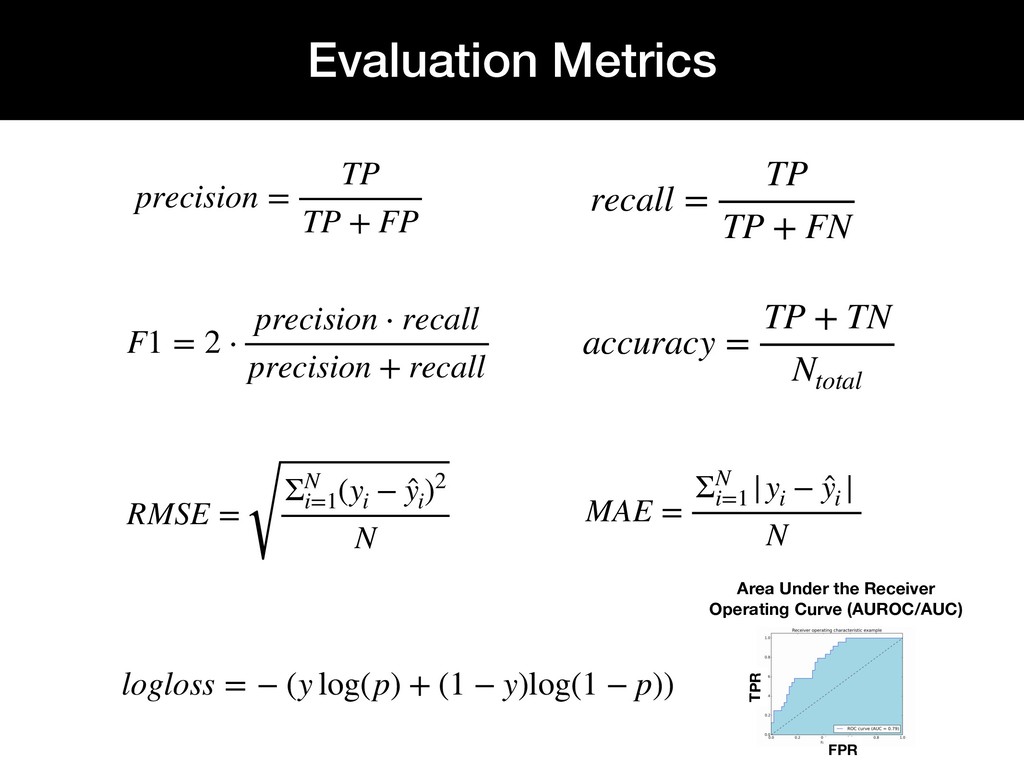
̂ y i )2 N Area Under the Receiver Operating Curve (AUROC/AUC) precisio n = TP TP + FP recall = TP TP + FN F1 = 2 ⋅ precisio n ⋅ recall precisio n + recall accu racy = TP + TN Nto tal lo glo ss = − (y log(p) + (1 − y)log(1 − p)) MAE = ΣN i= 1 |y i − ̂ y i | N FPR TPR
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}