Bronchospasm Atelectasis Hypoxemia Morbidity increases directly with volume (as little as 20 cc) and inversely with pH Epithelial degeneration, alveolar edema, hemorrhage into airspaces ARDS Treatment (Supportive)
gastric pH better than ranitidine given several hours prior to surgery Famotidine • Most effective given in two doses, the evening prior and the morning of surgery PPIs • Neutralizes stomach acid, 15-30 mL given 1 hours prior Sodium citrate • 10 mg IV = prokinetic effects Metoclopramide
presents with worsening abdominal distension. CT scan shows large mass obstructing the duodenum. The stomach is distended. The GI service is consulted to place a duodenal stent endoscopically. What questions do you ask and what do you say?
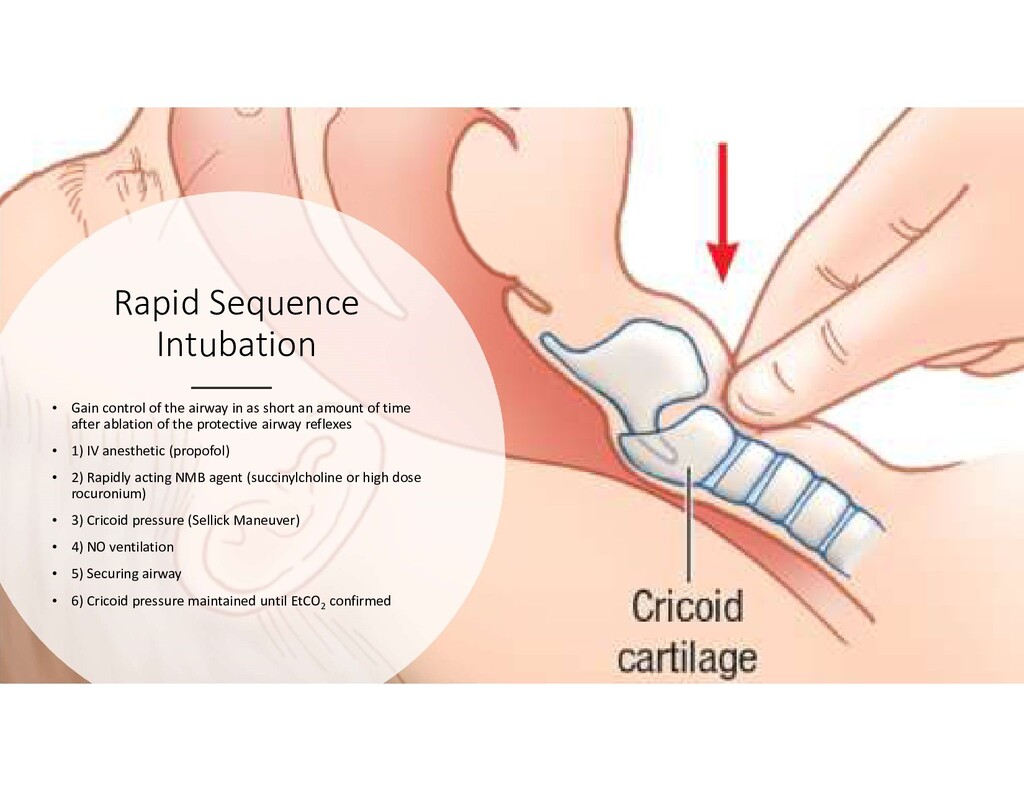
as short an amount of time after ablation of the protective airway reflexes • 1) IV anesthetic (propofol) • 2) Rapidly acting NMB agent (succinylcholine or high dose rocuronium) • 3) Cricoid pressure (Sellick Maneuver) • 4) NO ventilation • 5) Securing airway • 6) Cricoid pressure maintained until EtCO2 confirmed
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}